
Abstract
Most mental disorders exist on a severity dimension that extends from one or two characteristic symptoms, to having more symptoms but still being subthreshold, to being cases that meet or exceed the threshold established by the diagnostic criteria. Researchers are interested in the whole phenotype, while clinicians are more interested in people who match or exceed the DSM-IV diagnostic criterion. In DSM-IV, the position of the threshold on the severity continuum was a matter for expert judgment that people above the threshold would mostly warrant treatment, and people below would probably not warrant treatment.
The DSM-IV clinical significance criterion ‘the symptoms cause clinically significant distress and impairment…’ is part of the criteria for most common disorders, as a separate criterion (major depressive disorder (MDD), generalized anxiety disorder (GAD) etc.) or implicit in the description (alcohol/drug use, the phobias etc.). The clinical significance criterion does not contribute to the specific definition of any disorder, has no anchor points, is variably worded, and is not applied at all in some disorders. It has been effective at raising the threshold and therefore reducing the prevalence of some anxiety and depressive disorders [1].
In the present study we asked whether the DSM-IV diagnostic thresholds for the different anxiety and depressive disorders are set at comparable levels of severity. We estimated this by plotting the levels of disability and distress for each disorder against mean levels of disability or distress among the well people in the Australian National Survey of Mental Health and Well-being who reported no mental or physical disorder. We then explored the levels of disability and distress among cases when the clinical significance criteria were not operationalized.
Methods
We used data from the 1997 Australian National Survey of Mental health (n=10 641) [2]. Disability in the past 30 days was measured with the 12-item Short Form Mental Components Scale (SF-12 MCS) [3] and distress was measured from the Kessler-10 (K-10) [4]. Diagnosis of an anxiety or depressive disorder (social phobia, GAD, obsessive–compulsive disorder (OCD), post-traumatic stress disorder (PTSD), MDD and dysthymia) in the last 30 days was obtained using the Composite International Diagnostic Interview (CIDI) version 2.1 12 month version without the exclusion criteria being operationalized [5]. When people met criteria for more than one diagnosis we asked ‘which troubled you the most’ and identified this as their principal diagnosis. The few with more than one diagnosis who did not choose one of these six disorders as troubling them most, or who did not meet criteria for the disorder they chose, were allocated hierarchically to a principal diagnosis. We attributed the disability and distress scores to this diagnosis, thereby preventing people with comorbid, and therefore more severe, disorders being represented in the data more than once. We examined the levels of disability and distress again, after removing the clinical significance criteria.
The reference group was not the population sample as a whole but ‘well people’, the 5655/10 461 people in the survey who did not meet criteria for any of the 14 mental or 12 physical disorders covered by the survey. We hypothesized that the average disability and distress scores for well people would form a lower threshold of disability and distress for all people who met criteria for a mental disorder, that is, all should be more disabled or distressed than the average scores of well people.
Results
The prevalence of these six disorders was 7.2% (762/10 641) and this rose by one-quarter to 9.1% (970/10 641) when the clinical significance criteria were removed. The prevalence of five of the disorders rose by 17–24% but the prevalence of OCD rose by 219%, from 0.3% to 1.0% with the clinical significance criteria removed.
The results are displayed in Figures 1,2 and Tables 1,2, for disability (SF-12 MCS) and distress (K-10) scores, respectively. The two frequency bars associated with each diagnosis contain all the cases of that diagnosis, using the standard DSM-IV criteria (with clinical significance criterion; top bar) and after removing the clinical significance criterion (bottom bar). The per cent scale shows the proportion of people with each disorder above and below the mean for well people, and the shading is the distribution of disability and distress in standard deviations. The same data are in Tables 1,2, showing the increase in prevalence when the clinical significance criteria are removed.
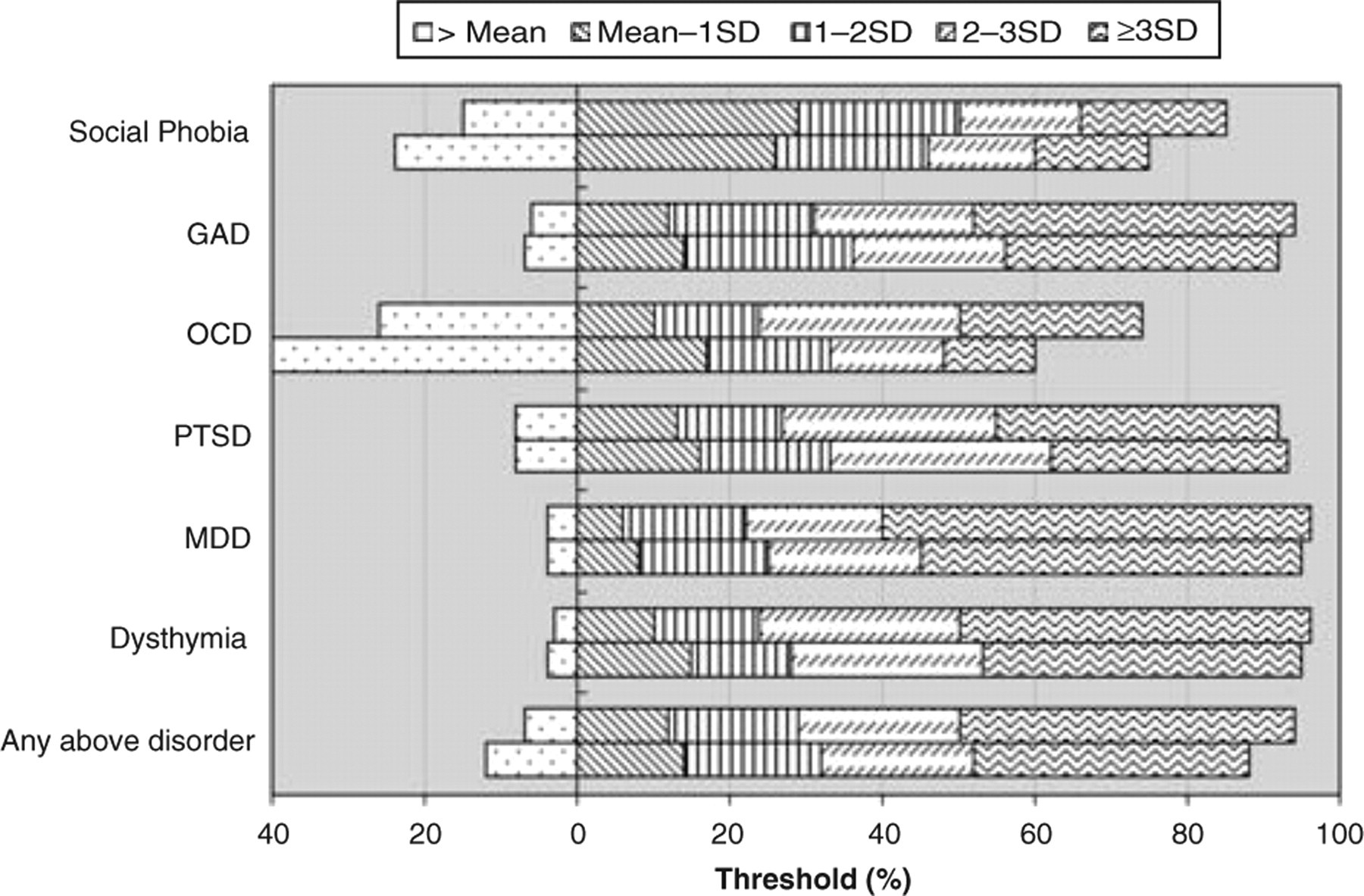
Main problem DSM-IV diagnosis (30day) stratified by Disability (12-item Short Form Mental Components Scale). The frequency bars show the number of people with each disorder who fall into the different severity categories of disability, as defined by the mean and standard deviation of well people for disability (mean = 54, SD = 7). The threshold value of 0 is the mean for well people score as less disabled than this. For each disorder the first bar represents people with the standard DSM-IV diagnosis and the second bar represents people with the diagnosis without the clinical significance criteria operationalized. GAD, generalized anxiety disorder; MDD, major depressive disorder; OCD, obsessive–compulsive disorder; PTSD, post-traumatic stress disorder.
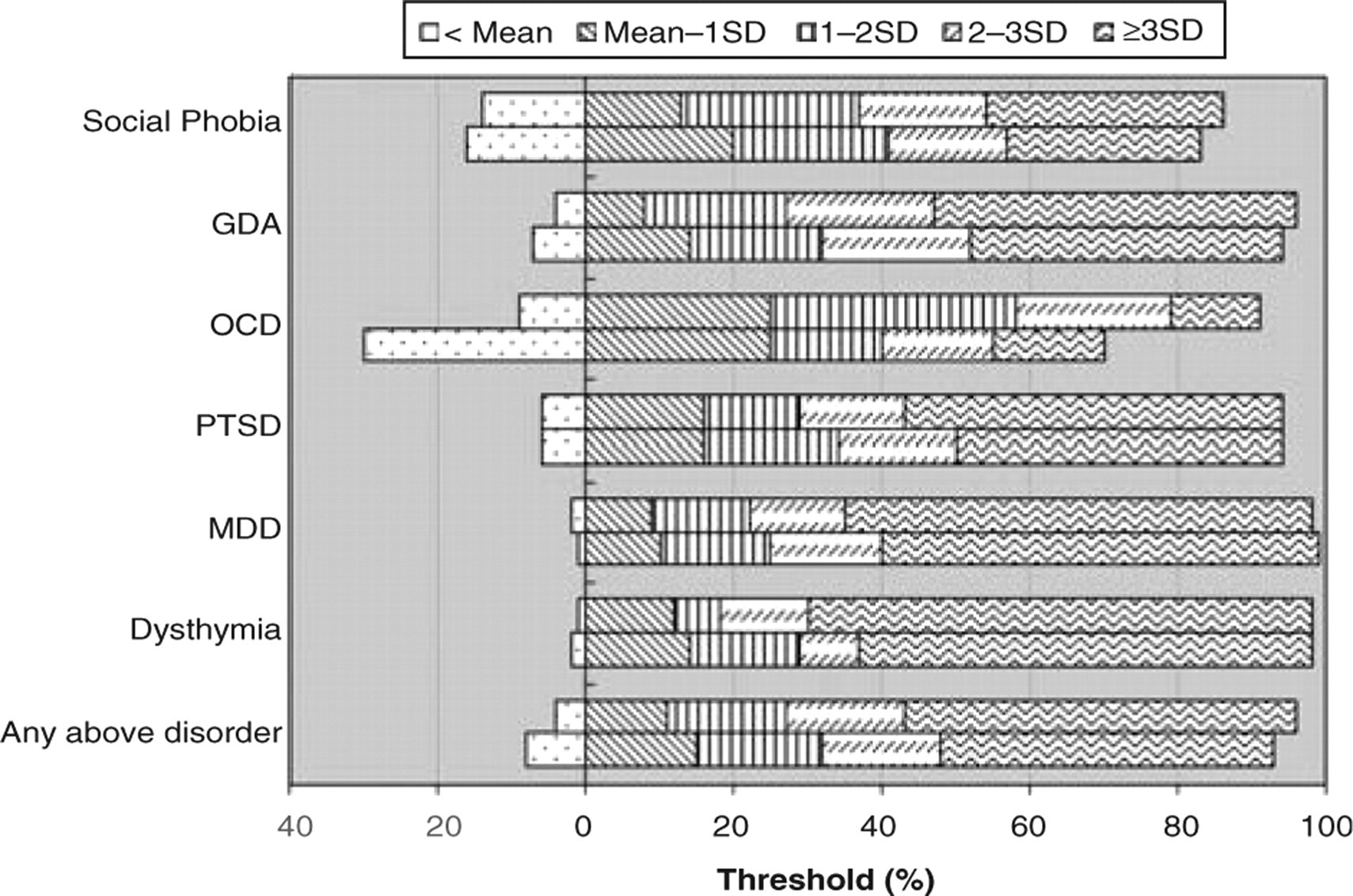
Main problem DSM-IV diagnosis (30 day) stratified by psychological distress (Kessler-10). The frequency bars show the number of people with each disorder who fall into the different severity categories of distress, as defined by the mean and standard deviation of well people for distress (mean = 13, SD = 3). The threshold value of 0 is the mean for well people score as less distressed than this. For each disorder the first bar indicates the standard DSM-IV diagnosis and the second bar shows people with the diagnosis without the clinical significance criteria operationalized. GAD, generalized anxiety disorder; MDD, major depressive disorder; OCD, obsessive–compulsive disorder; PTSD, post-traumatic stress disorder.
Main problem DSM-IV diagnosis (30 day) vs level of impairment (SF-12 MCS score)
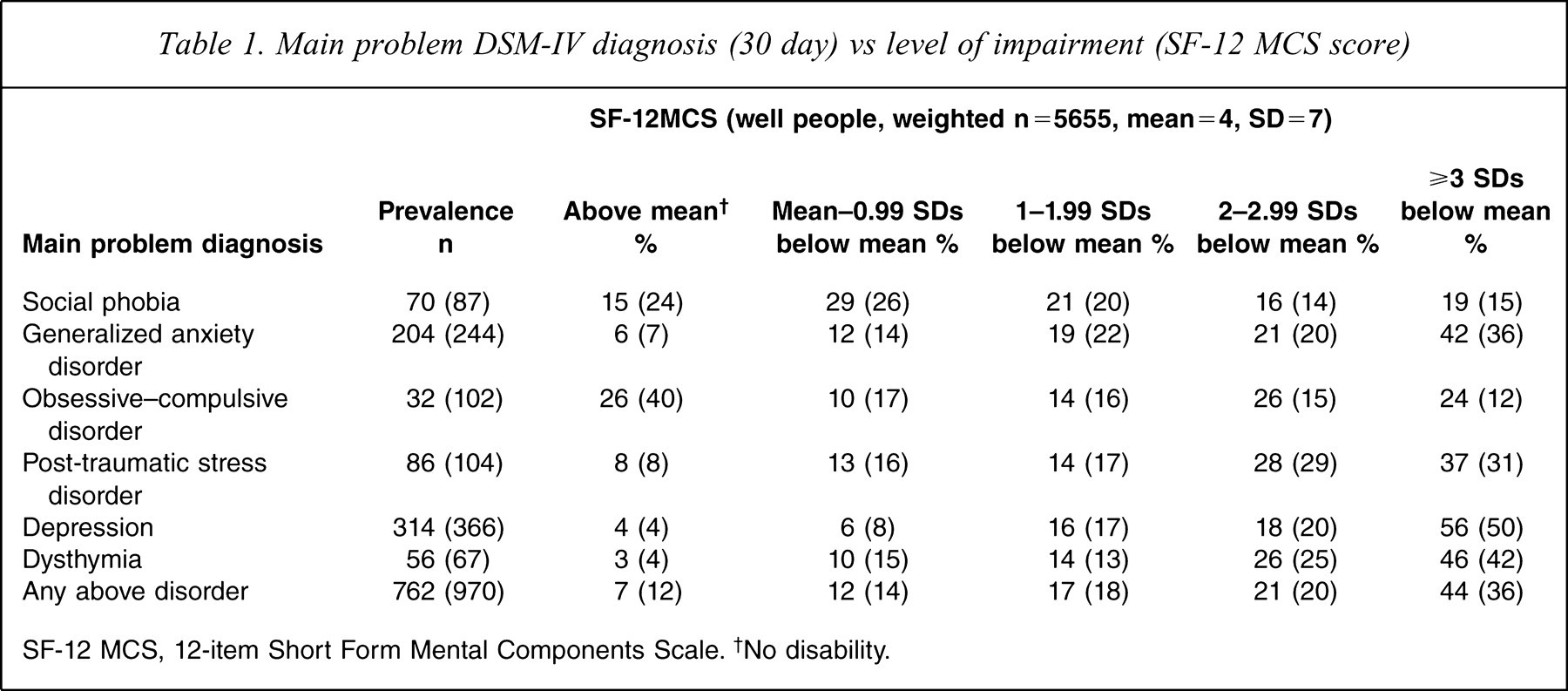
SF-12 MCS, 12-item Short Form Mental Components Scale. †No disability.
Main problem DSM-IV diagnosis (30 day) vs level of psychological distress (K-10)
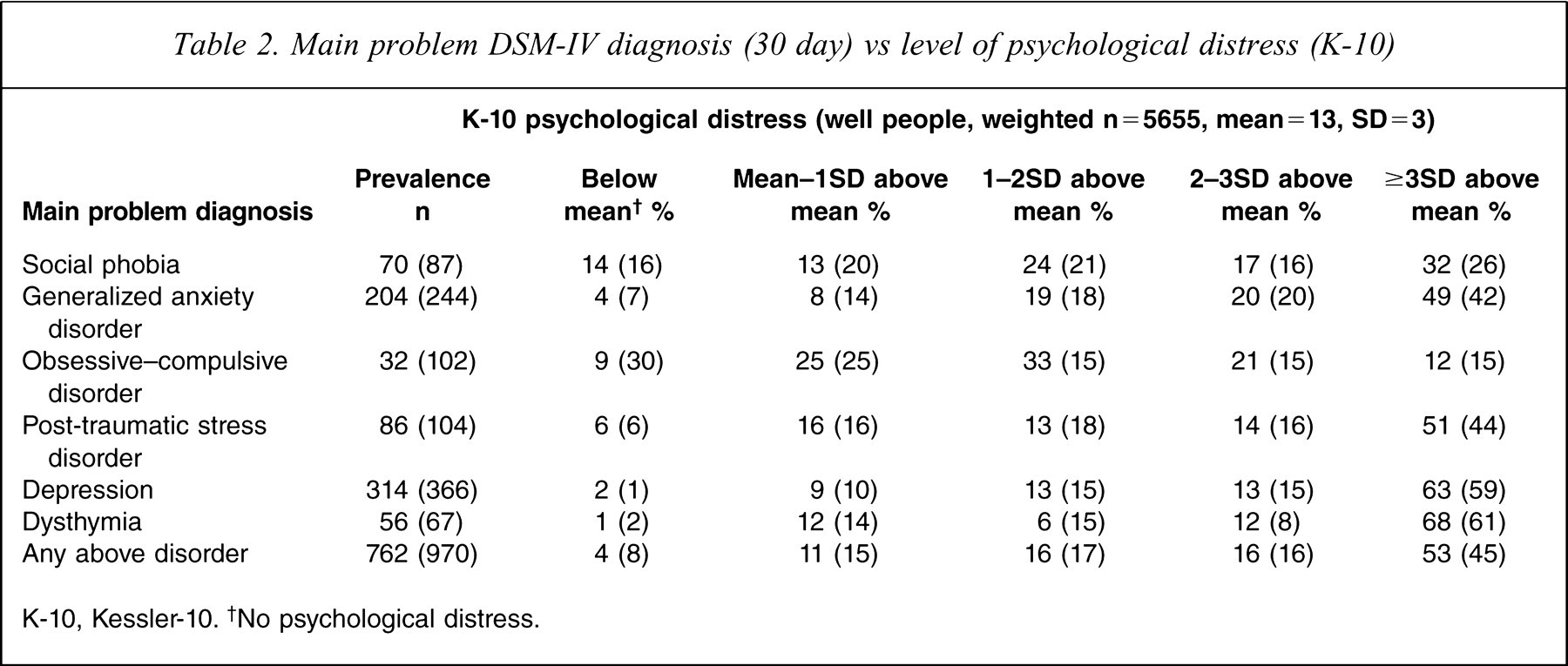
K-10, Kessler-10. †No psychological distress.
Using the standard DSM-IV diagnosis criteria (without the exclusion criteria), fewer than one-tenth of people who met criteria for having dysthymia, MDD, GAD or PTSD as their main problem had disability or distress scores lower than the average for well people. That is, >90% had distress and disability scores in the mild, moderate or severe ranges. People with the remaining two diagnoses, social phobia and OCD, seemed less distressed or disabled in comparison to people with the other disorders. In social phobia, as operationalized by the CIDI-2.1, 15% were less disabled and 14% were less distressed than the average for well people, that is, were neither distressed or disabled by their disorder. In OCD 26% were below the well person mean for disability and 9% below the well person mean for distress. We then looked at the other end of the distribution, how many cases scored more that two standard deviations above the mean for well people, that is, were severe. In dysthymia, MDD, GAD and PTSD the proportion ranges were 63–74% for disability and 65–80% for distress. In social phobia the proportions scoring in the severe range were 35% for disability and 49% for distress. In OCD the proportions in the severe range were 50% for disability and 33% for distress. We conclude that the diagnostic criteria that presently define social phobia and OCD define disorders that are milder than the criteria that define the thresholds for dysthymia, MDD, GAD or PTSD.
We then removed the clinical significance criteria and the number of cases identified as meeting criteria rose by one-quarter. In dysthymia, MDD, GAD or PTSD the proportion of cases below the mean for well people altered very little (range=0–3%). For social phobia, however, 24% of the cases scored below the well person mean for disability, although there was little change for distress, with 16% of cases scoring below the mean. In OCD the effect was larger, with 40% of cases scoring below the well person mean for disability and 30% scoring below the mean for distress. In social phobia the proportions scoring in the severe range were reduced to 29% for disability and 42% for distress. In OCD the proportions in the severe range were 27% for disability and 30% for distress. We conclude that, after removal of the generic clinical significance criteria, the specific criteria defining social phobia and OCD define disorders that are much milder than the criteria that define the thresholds for dysthymia, MDD, GAD or PTSD.
Discussion
Most mental disorders exist on a continuum of severity that ranges from vestigial to very severe [6]. The diagnostic criteria in DSM-IV identify the place on the continuum where the diagnosis can be made. We used epidemiological data to estimate the current prevalence of six disorders with and without the clinical significance criteria. As expected, the prevalence of all but OCD rose by approximately one-fifth, but the prevalence of OCD rose threefold. We concluded that the specific OCD criteria are weak.
We plotted the distribution of severity of six disorders against the distribution of distress and disability among well people who did not meet criteria for any of the 14 mental or 12 physical disorders covered by the data. Few cases of dysthymia, MDD, GAD or PTSD involved disability or distress scores below the means for well people, whether or not the clinical significance criteria were operationalized. In contrast people with social phobia or with OCD more often scored below the means and there was a relative paucity of subjects who scored in the severer ranges. We conclude that the specific criteria defining social phobia and OCD identify disorders that are lower than the criteria that define the thresholds for dysthymia, MDD, GAD or PTSD, and may need revision.
These results are from one survey. It used a diagnostic interview to determine people who had met criteria in the past 12 months and concluded that people who were still troubled by such symptoms were likely to have 1 month cases. As such, the decision is likely to be more conservative than in surveys that determine that the person has met criteria sometime in their lifetime and use the recency question to identify 1 month cases. The measures of distress (the K-10) and of disability (the SF-12 MCS) are established measures with good psychometric properties. It is unlikely that an interaction between diagnosis and the questions in the measures would lead to an underestimate of either disability or distress in persons with social phobia or OCD. Nevertheless it will be important to replicate these findings from addition data sets and, if possible, using different diagnostic measures and measures of distress and disability.
We hypothesized that people who met criteria for a mental disorder should seldom have less disability (impairment) or distress than well people because of the implicit assumption contained in the DSM-IV clinical significance criterion that ‘the symptoms cause clinically significant distress and impairment.’ This is part of the criteria for most common mental disorders. It is clear that this is not always so for either social phobia or OCD. That OCD as currently defined should often be mild is a surprise, but that social phobia is often mild is consistent with the claim that classifications of mental disorder were redefining normality, in this case shyness, that was made by the media when the title of social anxiety disorder was introduced in DSM-IV. In both these disorders, if the diagnosis-specific criteria were strengthened and the clinical significance criteria were removed, the thresholds could be made appropriate and consistent with the other four disorders included in this study.
ICD-10 and ICD-11 measure disability or activity limitation separately to the symptoms that determine membership of a diagnostic class. Perhaps DSM-V should explore the possibility of doing likewise, using a measure of disability that is independent of the details of each diagnosis. The problem with distress is more difficult to resolve. Although self-reported distress is intrinsic to the six disorders studied here, it may not be intrinsic to the externalizing or cognitive disorders. Perhaps we should confine our attention to using disability (activity limitation) as an independent measure of the severity or intensity of a disorder.
Footnotes
Acknowledgements