
Abstract
Children born at very low birth weight (VLBW; birth weight < 1500 g) and/or very preterm (gestational age < 32 weeks) are known to be at increased risk for a range of cognitive, academic, behavioural, and psychological problems [1–3]. Although there is an extensive body of research examining child and adolescent outcomes, follow up into adulthood is rare. Some studies have reported that VLBW adults are more likely to be hospitalized with a psychiatric disorder [4] and score higher on screening measures for psychopathology [5] compared with their normal birth weight (NBW; birth weight > 2499 g) peers. More specifically, research suggests an increased risk for mood disorders [6] and other internalizing symptoms [7]. However, this is not a universal finding as other studies have reported no differences in rates of psychopathology between VLBW and NBW adults [8,9]. Research in this area is characterized by methodological limitations such as reliance on screening measures to assess psychopathology [8,10], lack of a comparison control group [8], and cross-sectional or retrospective data collection methods [4,11].
The present study sought to determine the rates of psychiatric disorders in VLBW adults. We addressed the limitations of previous research by using a prospective, longitudinal study design that incorporated a NBW control group, and by combining screening measures with semi-structured clinical interviews for psychiatric assessment. It was hypothesized that VLBW adults would have higher levels of psychopathology on screening measures and higher rates of psychiatric diagnoses on assessment than NBW adults. As internalizing disorders have been reported to be more prevalent in VLBW women at age 20 [10], it was expected that VLBW adult women would have higher levels of psychopathology relative to VLBW men and NBW peers.
Methods
Participants
VLBW participants were consecutive survivors from two overlapping cohorts born at the Royal Women's Hospital in Melbourne, Australia. The first comprised 86 consecutive survivors of birth weight < 1000 g, born between 1 January 1977 and 31 March 1982. The second comprised 124 consecutive survivors of birth weight 1000–1500 g born between 1 October 1980 and 31 March 1982. A randomly selected comparison cohort was also recruited, comprising term, normal birth weight (NBW) infants with birth weights ≥ 2500 g, born between 1 October 1981 and 31 March 1982. These participants were randomly selected using hospital unit record numbers, whereby 1 in every 100 births was invited to be in the study, until 60 participants were successfully recruited. The cohorts had been assessed at ages 2, 5, 8, 14, 18–22 years, and most recently, aged 25–29 years. However, follow up was not identical for all cohorts at all ages and thus, only data from the birth and adult assessments will be described in the current study. In total, 117 of 210 (56%) VLBW participants and 32 of the 60 (53%) NBW controls were successfully followed up in the most recent data collection period.
Procedure
The study was approved by the Research and Ethics Committees of the Royal Women's Hospital. Participants were sent information on the study and invited to participate in the adult follow up assessment. After written informed consent was obtained, data collection took place in two phases. In the first phase, participants were invited to attend an appointment at the Royal Women's Hospital, Melbourne, during which they were asked to complete a psychiatric screening questionnaire (Symptoms Checklist (SCL-90-R)). In the second phase, participants who scored above the specified cut-off point on the screen were re-contacted and invited to attend a structured clinical interview (Structured Clinical Interview for DSM-IV-TR for Axis I Disorders, research non-patient version (SCID-I/NP)).
Perinatal and demographic data
Demographic (race, gender, family structure, maternal education and primary income earner's employment and occupation) and perinatal (birth weight and gestational age) data had been collected at birth. Social demographic data were collected at age 18 (highest grade completed in high school) and at the adult assessment (relationship status – single or other; relationship with parents - adequate or poor).
Psychiatric symptoms
The Symptoms Checklist (SCL-90-R) [12,13] was administered as a screening measure for psychopathology. The SCL-90-R assesses the following nine primary symptom dimensions: somatization, obsessive–compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation and psychoticism. Internal reliability for each measure has an alpha coefficient range of 0.66 to 0.90. Global and subscale scores were used in analyses to provide an overall estimate of psychopathology as well as an estimate of impairment within specific dimensions (such as anxiety). The Global Severity Index (GSI) is the mean score of all responses. The SCL-90 and SCL-90-R both have adequate validity (specificity and sensitivity) in predicting DSM-IV psychiatric disorders [14,15]. A clinical cut-off score was set as a T-score of 65 (1.5 standard deviations above the mean) on any of the 10 scales of the SCL-90-R. See Figure 1 for a flow chart of the recruitment and follow up process.
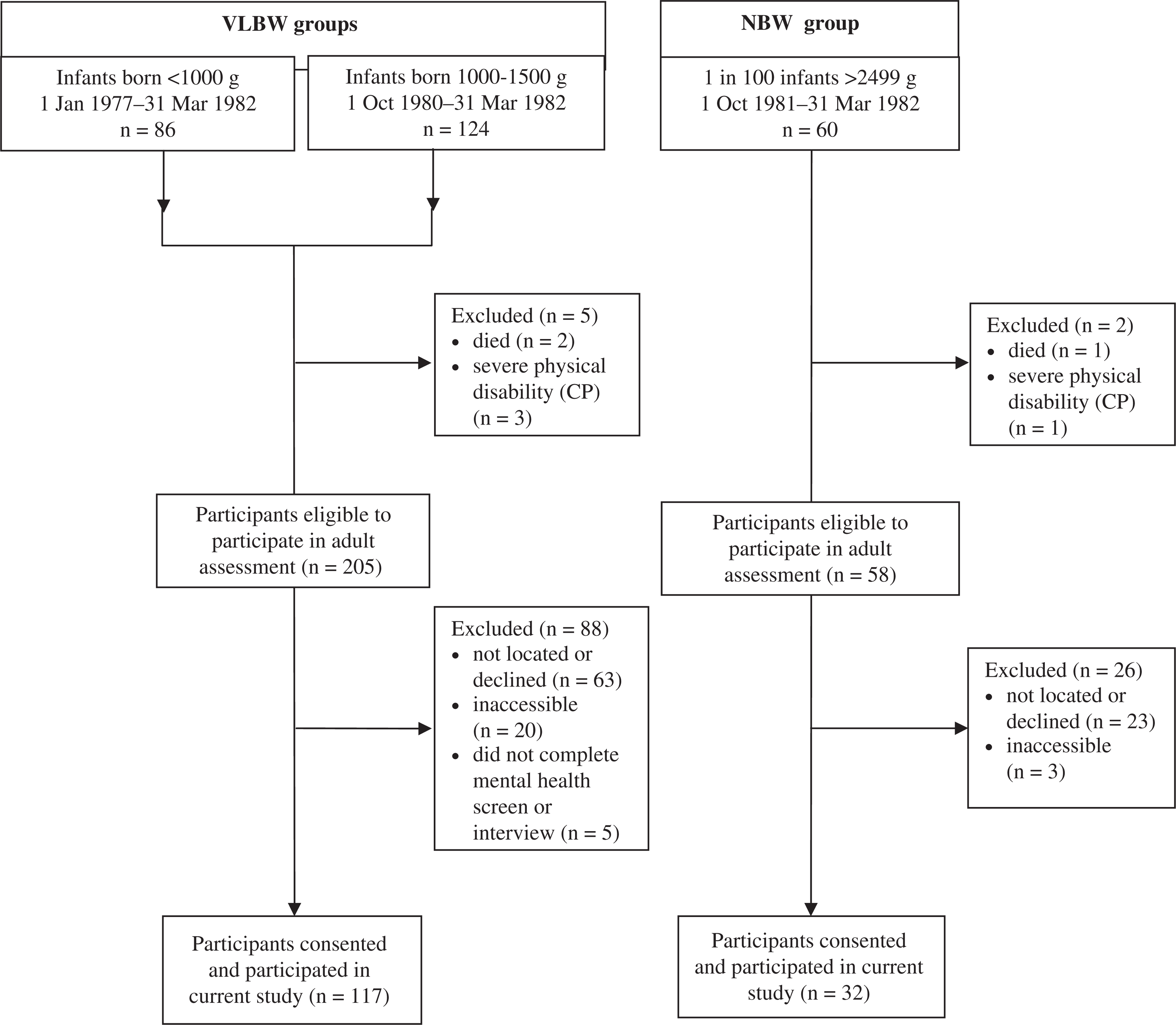
Flow diagram of participant recruitment at birth and retention at adult follow up, when participants were 24–29 years of age.
Psychiatric diagnosis
VLBW and NBW participants who scored in the clinical range on any of the 10 scales of the SCL-90-R were contacted and invited to attend an interview. The SCID-I/NP [16] was used to determine a formal clinical diagnosis for these participants. The SCID-I/NP is a semi-structured diagnostic interview, which takes 60–90 min in duration to complete over a single sitting. A qualified psychologist who had completed formal training in the SCID-I/NP interview technique, and blinded to participant group membership, administered all interviews.
Given that research suggests comparability of in-person and telephone SCID-I/NP diagnoses [17], participants unable to attend a SCID-I/NP interview in person were invited to complete the interview over the phone. The inter-rater and test–retest reliability of the SCID-1/NP varies across different diagnoses and studies, and ranges from 0.53 (inter-rater) for dysthymic disorder [18] to 0.96 (inter-rater) for other substance abuse/dependence [19]. Acceptable validity has also been demonstrated over standard clinical interviews at intake episode [20,21]. The SCID-I/NP investigates 37 major disorders across five broad categories: depressive, anxiety, bipolar/psychotic, eating, and drug/alcohol disorders. Two estimates of depressive disorders were calculated for analyses. Both included current dysthymic disorder diagnoses. In addition, ‘current’ estimates included current minor depressive episode (mDE) and major depressive episodes (MDE) only, while the ‘inclusive’ estimates of internalizing disorder included both current and past mDE and MDE. Two (current and inclusive) ‘total number of diagnoses’ categories also reflect this distinction.
Statistical analysis
Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, Chicago, IL) version 18 for Windows. P values < 0.05 were regarded as statistically significant across all analyses as the study was considered to be hypothesis-generating rather than hypothesis-proving, and analyses primarily were focused on comparing the magnitude of birth weight group differences. Given the small relative sample size of the NBW control group, Cohen's d effect size calculation was used as an index of strength of association between independent and dependent variables; effect sizes of 0.2 were classed as small, 0.3–0.7 medium, and above 0.7 as large [22]. Independent samples t-tests were used to assess birth weight group differences (VLBW versus NBW) for subscale scores on the SCL-R-90 and chi-square for categorical variables. When data were non-normally distributed the Mann–Whitney U-test was used. Yates' continuity correction was not reported for 2 × 2 group χ2 analyses given that this statistic tends to overcorrect and was considered too conservative [23]. Analyses compared rates of participants who met criteria for a diagnosed disorder across the VLBW and NBW groups. Odds ratios (OR) and 95% confidence intervals (CI) were calculated for significant results, or relative risks (RR) where cells contained zero. Participants who were not elevated on either of the screening measures were treated as not having a diagnosed disorder.
Results
Perinatal and demographic characteristics
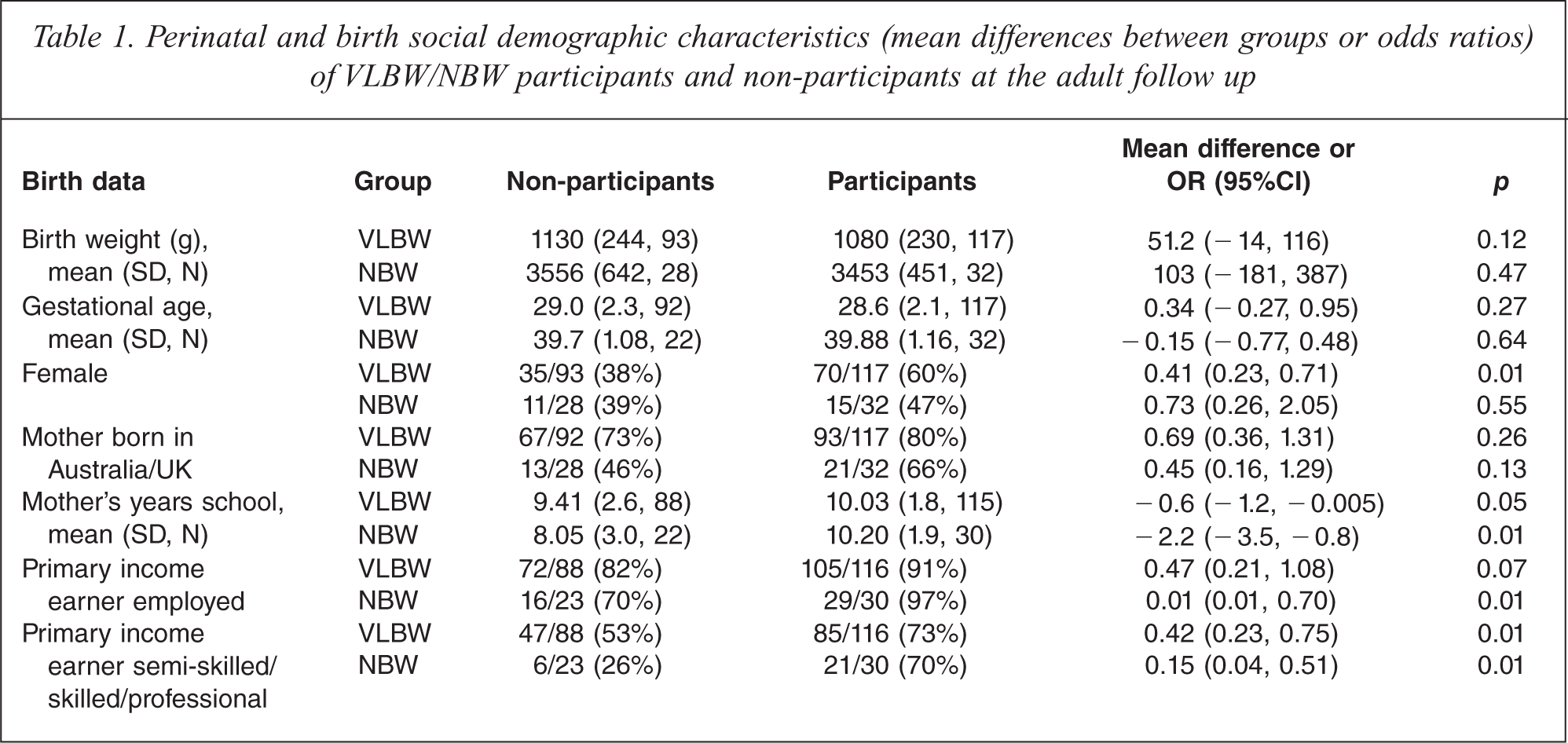
While there were no differences between VLBW participants and non-participants at this adult follow up for birth weight or gestational age, VLBW participants were significantly more likely to be female (Table 1). For both VLBW and NBW groups, participants were more likely than non-participants at adult follow up to have a mother who completed at least 11 years of education and to have been from a family where the primary income earner was employed. For current participants there were no significant differences between VLBW and NBW groups for gender (χ2 = 1.72, p = 0.19) or whether mothers were born in Australia (χ2 = 2.69, p = 0.10). There were also no group differences for indicators of socioeconomic status within the family at birth: primary income earner's employment status (χ2 = 1.19, p = 0.27), occupation (χ2 = 0.13, p = 0.72), and maternal education (χ2 = 1.24, p = 0.27). The majority of primary income earners within families of current participants, for both birth weight groups, identified as being in professional, skilled or semi-skilled work at the time of birth. Group differences were also tested for three social demographic variables collected at the adult assessment. While there were no birth weight group differences on how participants rated their current relationship with their parents, or on participants' current relationship status, VLBW participants had spent significantly fewer years in high school (VLBW mean = 11.53, SD = 0.9; NBW mean = 11.93, SD = 0.4, p < 0.001; note missing data VLBW n = 26; NBW n = 9).
Perinatal and birth social demographic characteristics (mean differences between groups or odds ratios) of VLBW/NBW participants and non-participants at the adult follow up
Psychopathology outcomes by birth weight groups
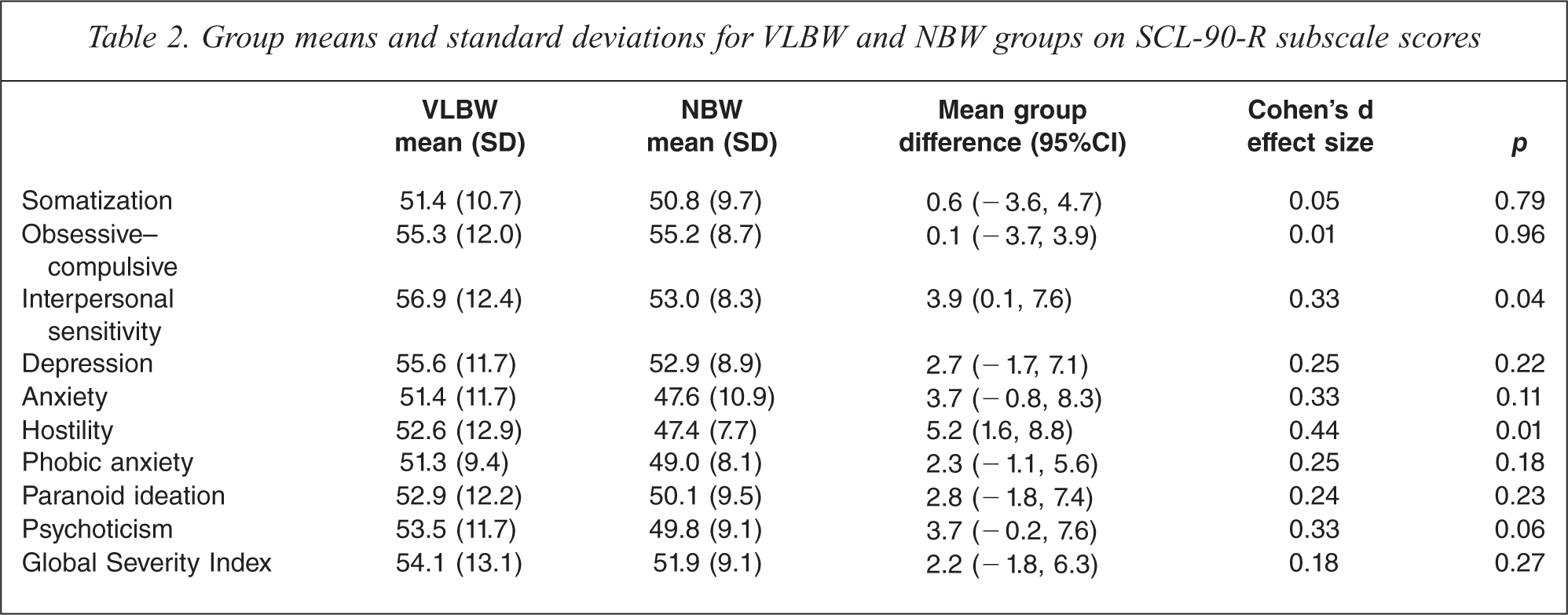
Table 2 presents the data for the NBW and VLBW groups across subscales of the SCL-90-R. The VLBW group scored significantly higher than controls on the interpersonal sensitivity and hostility scales, indicating greater psychopathology. Further, there were low to medium effect sizes for birth weight group differences, in the same direction, across the depression, anxiety, phobic anxiety, paranoid ideation, and psychoticism subscales and the Global Severity Index, though these differences did not reach statistical significance.
Group means and standard deviations for VLBW and NBW groups on SCL-90-R subscale scores
Birth weight group proportions of clinical elevation on the SCL-90R are shown in Table 3. There were a number of significant group differences across the psychopathology subscales: compared with NBW peers, VLBW participants were significantly more likely to be in the clinical range on the interpersonal sensitivity, depression, hostility, paranoid ideation and global severity index scales of the SCL-90-R. A significantly higher percentage of VLBW participants were elevated on at least one of the SCL-90-R scales, compared with NBW participants (43% versus 22%; Table 3). Further, the average number of elevated SCL-90-R scales was significantly greater in the VLBW group, Mann–Whitney U-test, z = − 2.19, p = 0.03. VLBW birth weight distributions for each of the screening subscales were also examined for those scales showing significant birth weight group differences for binary outcomes but non-significant differences when comparing mean scores (depression, paranoid ideation, Global Severity Index); there was no relationship between birth weight and scores on these three scales, and no evidence of extreme score clusters. Gender effects were also tested. There were no differences between how men and women scored on any subscales of the SCL-90-R for either of the birth weight groups.
Percentages, odds ratios (OR) and χ2 analyses for birth weight group comparisons on binary rates of clinical elevation on SCL-90-R scales
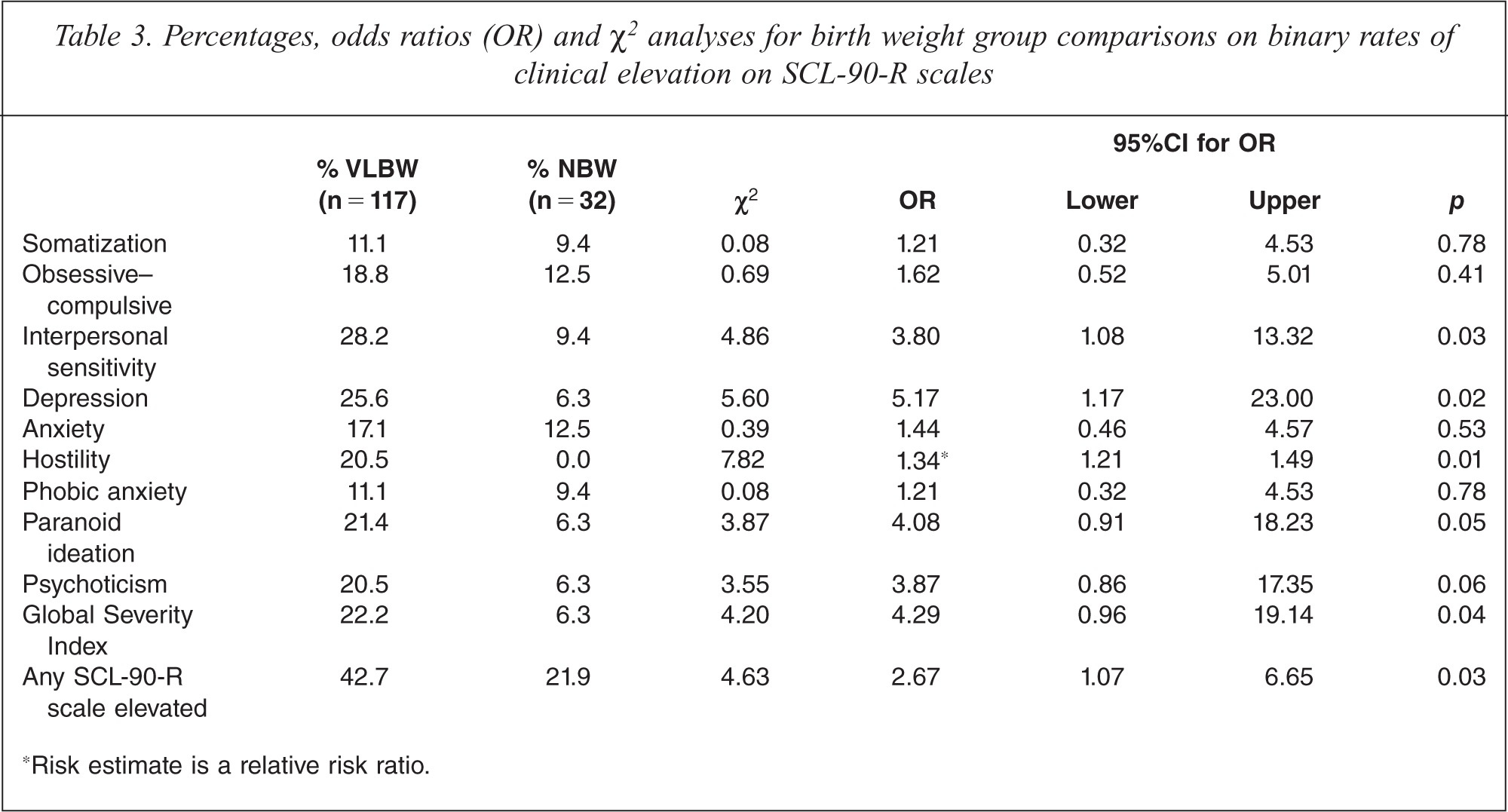
Risk estimate is a relative risk ratio.
Formal psychiatric diagnoses on clinical interview
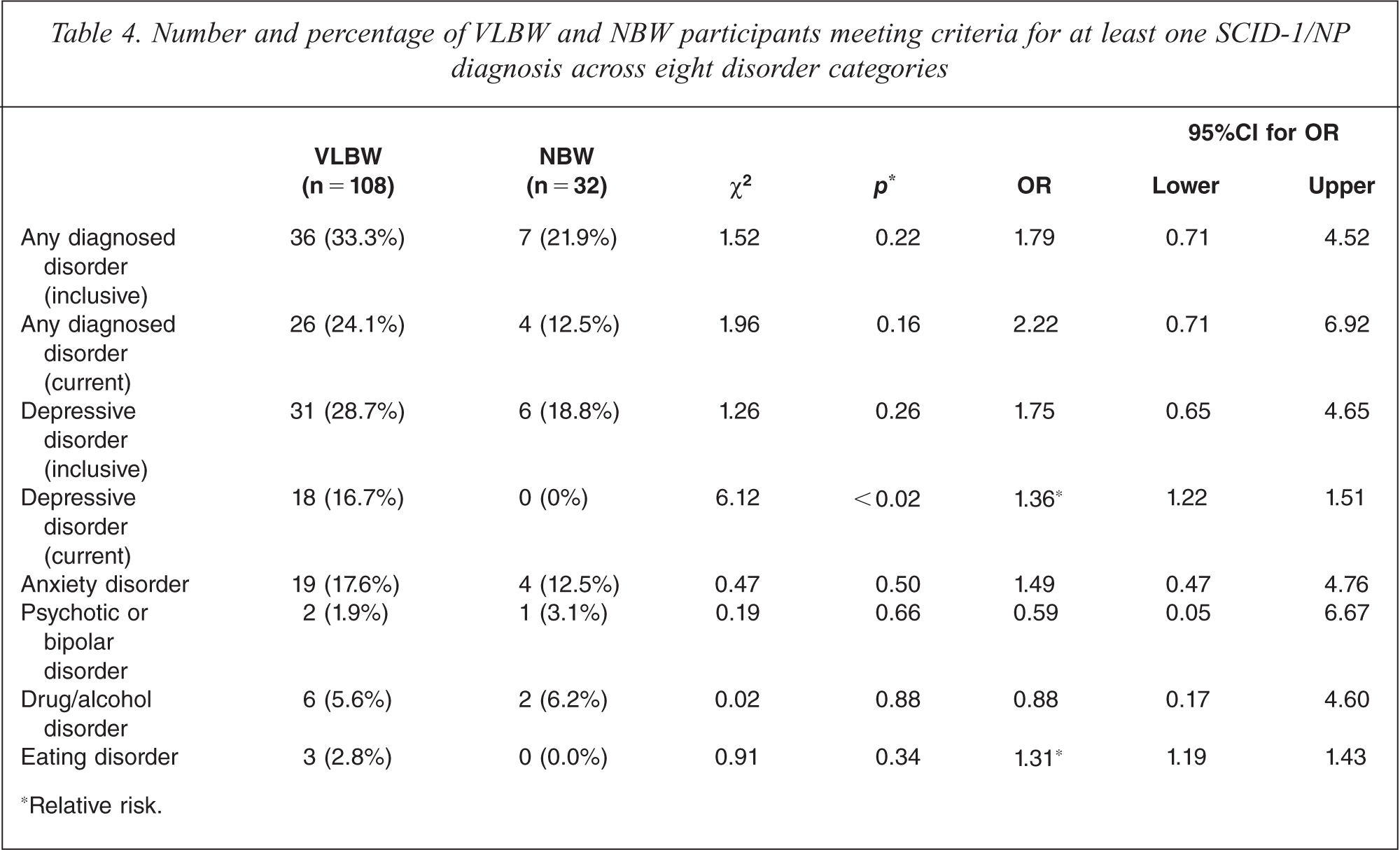
Eight NBW and 50 VLBW participants were eligible for the SCID-1/NP interview. Of these, all of the NBW and 41 of the VLBW participants successfully completed the clinical interview. Participants who were eligible for an interview but who did not complete the formal interview process were excluded from analyses. However, for five of the nine eligible participants who were not interviewed, ongoing phone contact was maintained for up to 3.5 years. Of these, four participants self-reported significant stressful life events (social or medical) or mental health problems that made it difficult for them to complete the interview. Data from the SCID-1/NP clinical assessment interviews are presented in Table 4. The percentages in the table represent the proportion of participants who met criteria for a diagnosed disorder, from the total number of participants who completed all assessments. Approximately one third of VLBW participants met criteria for a past or present (inclusive definition) psychiatric diagnosis compared with 22% of their NBW peers. Further, 24% of VLBW participants met criteria for a current psychiatric diagnosis compared with 12% of NBW participants. There was only one significant group difference between the VLBW and NBW groups on rates of specific disorders; for current depressive disorder. Group medians for the number of past or present (inclusive) SCID-1/NP diagnoses were also compared. Though VLBW participants had almost twice as many diagnoses (median = 0.78, n = 41) compared with NBW controls (median = 0.47, n = 8), this difference failed to reach significance, Mann-Whitney U-test, z = −1.20, p = 0.23.
Number and percentage of VLBW and NBW participants meeting criteria for at least one SCID-1/NP diagnosis across eight disorder categories
Relative risk.
Discussion
The VLBW adults had more abnormalities compared with NBW controls on several subscales of the Symptom Checklist (SCL-90-R). Further, structured clinical interviews revealed VLBW adults were more likely to be diagnosed with a current depressive psychiatric disorder, which included current diagnoses of major and minor depression and dysthymic disorder. VLBW participants scored higher than their NBW peers on the interpersonal sensitivity and hostility subscales and were more likely to be elevated on hostility, interpersonal sensitivity, depression, paranoid ideation and the Global Severity Index of the SCL-90-R. With the exception of the Global Severity Index, this set of SCL-90R scales measure problems related to social and emotional functioning; how individuals feel about themselves and how they relate to others in the social world. For example, items in the interpersonal sensitivity scale ask whether individuals ‘[feel] inferior’, ‘easily hurt’ or ‘[feel that] others do not understand [them]’.
The current study findings provide evidence that while the increased risk for psychopathology persists into adulthood in the VLBW population, the severity of psychopathology may reduce over the transition from childhood to adulthood. Previous research exploring child and adolescent VLBW outcomes suggests a strong birth weight effect, where preterm or VLBW children and adolescents have significantly higher rates of behaviour problems [3,24,25] and mood and anxiety disorders [26] than NBW or term controls. While the current study found that VLBW participants were more likely to be elevated on 5 of 10 psychopathology subscales, in the clinical range on one or more screening subscale, and more likely to be elevated on a greater number of scales than NBW peers, the magnitude of these effects tended to be small to moderate. Further, while there was a consistent pattern whereby the VLBW group had higher mean scores across all of the psychopathology subscales, these birth weight group differences did not reach significance for the majority (8 out of 10) of the scales. Finally, the proportion diagnosed with a psychiatric disorder in the VLBW group did not differ significantly from NBW peers.
No gender effect was evident, which is inconsistent with previous research where gender effects have been reported across different ages. For example, Hack et al. reported that VLBW women were rated higher than either NBW controls or VLBW men on a range of internalizing scales, while parents of VLBW men reported significantly more ‘thought problems’ for their sons than parents of NBW adults [10]. Patton and colleagues also found differential rates of mood disorder for preterm female and male adolescents [39]; and Dahl and colleagues found that parents reported more social and attention problems in VLBW boys and more internalizing behaviour in VLBW girls [40]. However, the current study findings are consistent with much of the previous VLBW outcome research, which suggests that VLBW children/adolescents are at risk of mood disorders [27], more likely to be socially immature, rejected by peers [28] and to experience isolation [29] and peer victimization [30]. Research has also shown that VLBW young adults tend to be slower in beginning romantic partnerships and sexual activity, delay leaving the family home-of-origin for longer, and are more likely to have social problems than their NBW peers [31]. Studies have also reported subtle birth weight effects in terms of education, psychological well-being and personality, where VLBW adults tend to be more risk avoidant, less satisfied with their physical appearance, less likely to be in higher education and more likely to be unemployed than their NBW peers [9,31–33]. This was consistent with the current study finding that VLBW adults had fewer years of schooling in high school. While it was beyond the scope of the current study to assess Axis II (personality) disorders or social functioning, these are important areas that should be addressed in future research.
It is possible that the nature of VLBW vulnerability is influenced by the very specific social and environmental context of preterm/VBLW birth, in addition to possible alteration to developing, internal biological systems, such as the hypothalamic–pituitary–adrenocortex (HPA)-axis [34,35]. VLBW survivors begin life with an immature biological system and are more susceptible to medical complications. Although intensive medical care is necessary for VLBW infants' immediate survival, the NICU environment is not ideal for creating a secure, positive attachment relationship between VLBW infant and parents. Preterm infants are also forced to participate in the social world before they are developmentally ready. It is possible that this early environmental context plays a role in determining the nature of the vulnerability associated with VLBW birth. In addition, numerous factors, such as other perinatal risk, socioeconomic position, family structure, parenting practices and home environment, have been identified as important in determining long-term outcomes for VLBW children [36–38]. It is likely that many of these factors remain important in terms of predicting adult psychiatric outcomes. It will be important for future research to explore longitudinal predictors of adult psychiatric outcomes in VLBW survivors, in order to identify and support those individuals most at risk of poor psychological outcomes.
The relatively low follow up rate in our prospective, longitudinal study was the primary limitation of the current study. However, this study is one of the first to follow VLBW survivors from birth and over such a long period. At every follow up assessment, including the final adult assessment with psychiatric interview, participants were required to attend an appointment at the Royal Women's Hospital in Melbourne. For participants who were interstate or overseas, this was usually not possible. In comparison with mailed questionnaire-based studies, this is likely to have contributed to participant attrition. However, the most common reason for non-participation was the inability to locate adult participants, given that many participants and their families had moved house without updating their contact details with the study, and were not locatable using Australian electoral rolls. This is expected, given the mobility of this age group.
The power of the current study was also limited by the comparatively small NBW group size, though findings indicated small birth weight group (VLBW versus NBW) differences on the majority of psychopathology subtests and for many of the psychiatric disorder categories. The study findings may also have been influenced by a natural bias from participant attrition over time. In both VLBW and NBW groups, participants differed from non-participants in that they were more likely to have come from a higher socioeconomic status family background. Therefore, it may be that the rates of psychopathology reported in this study for the VLBW group are an underestimation of the true morbidity in the overall cohort. It is also possible that the NBW rates of psychiatric disorder were somewhat artificially lowered by an under-representation of participants with higher social risk. Further, given that clinical interviews were only offered to participants who were elevated on the SCL-90-R screening questionnaire, it is possible that there may have been some false negatives, reducing the number of participants identified with a psychiatric disorder.
In summary, technological advances over the last few decades have resulted in an unprecedented survival rate of babies born very small and/or preterm. However, research continues to show that these individuals may have ongoing challenges during their development and into adulthood. Although research has become increasingly comprehensive in the assessment of developmental outcomes in the last decade, long-term psychiatric follow up remains rare. Improved understanding of mental health outcomes for VBLW adults is important in order to provide the most accurate picture of life-long morbidity and to allow the subsequent development of targeted, cost-efficient intervention programmes to prevent and treat long-term psychopathology. However, current understanding of both the trajectory and mechanisms associated with psychopathology is lacking. Future research needs to utilize longitudinal study designs in order to delineate factors influencing developmental pathways and to achieve the goal of minimizing long-term impairment associated with socioemotional impairment and psychiatric disorder.