
Abstract
Objectives:
Mental health service use among young people is increasing, and small groups within the population disproportionately account for the majority of mental health service use. The aims of this study were to identify population-based trajectories of mental health service use across childhood and adolescence and associated sociodemographic/other risk factors.
Methods:
Mental health trajectories between birth and 17 years of age were identified using zero-inflated Poisson latent-class growth mixture modelling, in a New South Wales cohort of 9510 children (born between 2002 and 2005) who had at least one primary diagnosis of a mental disorder recorded in ‘Emergency Department’, ‘Admitted Patients’ and/or ‘Mental Health Ambulatory’ data collections.
Results:
A two-trajectory solution provided the optimal fit to the data: One trajectory displayed high increasing service use (n = 1861, 19.6%) and accounting for more than 68% of the days treated for mental disorder among the entire cohort. The other trajectory (n = 7649, 80.4%) was distinguished by a consistently low level of service use. Membership in the high mental health service use trajectory was associated with parental mental disorder, child maltreatment exposure and diagnoses of psychosis spectrum and personality disorders.
Conclusion:
Less than one-fifth of children account for more than 68% of hospital and ambulatory services used up to age 17 years; these children are more likely to have parents with mental disorder and to have been exposed to child maltreatment, pointing towards multi-disciplinary supports as a basis for early intervention.
Mental disorders are diagnosed in approximately 14% of Australian children each year, yet only half of these children receive treatment, with around one in 16 young people receiving mental healthcare through a hospital, emergency department, or outpatient service (Lawrence et al., 2015). Longitudinal follow-up of 1037 individuals over 40 years in the Dunedin (New Zealand) study demonstrated that the top 20% of mental health service users in childhood accounted for a high proportion (~80%) of overall public expenditure on health and social services in adulthood (Caspi et al., 2016). Well-powered studies of the factors associated with high levels of hospital, emergency and specialist mental health service use for mental health care among children and adolescents are limited.
In Australia, mental health services are more heavily used by girls, increasing with age throughout childhood and adolescence (Productivity Commission, 2020; Watkeys et al., 2024). Despite the increased prevalence of mental disorders among young people in outer regional and remote areas, access to services in these regions is reduced (Productivity Commission, 2020), and this may be partially attributable to larger Indigenous populations in these regions, who experience disproportionally higher rates of psychological distress owing to the adverse impacts of colonisation (Australian Institute of Health and Welfare, 2014; Gee et al., 2020; Page et al., 2022). Other factors associated with higher rates of mental health service use include parental psychopathology, child maltreatment, perinatal risk factors and diagnosis (e.g. psychosis and borderline personality disorder) (Abdin et al., 2017; Nemeroff, 2016; Olino et al., 2010; Polari et al., 2018; Rajaleid et al., 2016; Sagué-Vilavella et al., 2022; Vella et al., 2019).
While a large number of studies have examined mental disorder symptom trajectories across adolescent and/or young adult development (Abdin et al., 2017; De Lijster et al., 2019; Fountain et al., 2012; Morgan et al., 2021; Paksarian et al., 2016; Polari et al., 2018; Rajaleid et al., 2016; Rivenbark et al., 2018; Veldman et al., 2015; Vella et al., 2019; Waizbard-Bartov et al., 2021; Zhang et al., 2022), only two studies have attempted to identify homogeneous groups of individuals according to patterns of mental health service use over time using latent class growth-mixture modelling (Musliner et al., 2016; O’Driscoll et al., 2021). These studies typically converge in identifying at least one subgroup, representing less than 20% of the population, who display an increasing or consistently severe clinical course over time (Abdin et al., 2017; Caspi et al., 2016; De Lijster et al., 2019; McCauley et al., 2020), with sex differences in the propensity for particular mental health trajectories (Musliner et al., 2016; Olino et al., 2010; Shore et al., 2018; Waizbard-Bartov et al., 2021). The identification of mental health service use trajectories and their associated risk factors in childhood can inform primary prevention efforts to curb the need for intensive mental healthcare.
This study aimed to describe patterns of mental health service use in childhood and adolescence, and associated sociodemographic/other risk and clinical factors, using longitudinal administrative data for a population cohort of Australian children followed from birth until approximately 17 years of age. The aims of the study were to (1) identify latent groups of children with homogeneous patterns of mental health service use from birth to age 17 years; (2) explore whether certain types of mental disorder diagnoses are associated with more persistent mental health service use trajectories; (3) identify factors associated with high service use trajectories, with consideration of the timing of exposure to said factors; and (4) explore sex differences in the diagnostic and other factors associated with the latent trajectories of mental health service use.
Method
Participants
Participants were 9510 children, representing 10.4% of the population of 91,597 children born between 2002 and 2005 from the New South Wales Child Development Study (NSW-CDS); the selected sample of children had at least one primary mental disorder diagnosis in administrative health records (described below) prior to their 18th birthday, and had linked data for both parents (82% of the overall cohort) (Green et al., 2024). For any siblings in the cohort, one sibling was selected at random for inclusion to ensure independent observations about sociodemographic and other risk factors. Record linkages were conducted by the NSW Centre for Health Record Linkage (CHeReL) under the ‘waiver of consent’ provision of the National Statement of Ethnical Conduct in Human Research, with approval from the NSW Population and Health Services and ACT Health Human Research Ethics Committees (HREC/18/CIPHS/49).
Modelled data – days treated for mental disorders
The number of days of mental health treatment was determined for each child – within four developmental periods spanning early childhood (0–5 years), middle childhood (6–11 years), early adolescence (12–14 years) and late adolescence (15–17 years) – by summing the days of care received across presentations and services recorded in the NSW or ACT Admitted Patient Data Collections (APDC; 3 January 2002 to 31 March 2021) and Emergency Department Data Collections (EDDC; 8 January 2002 to 31 March 2021), and the NSW Mental Health Ambulatory Data Collection (MH-AMB; 27 November 2002 to 31 December 2020) data sets. The APDC contained information on all hospital admissions including in Public Hospitals, Private Hospitals, Private Day Procedure Centres, Public Psychiatric Hospitals, and Multi-Purpose Services. The EDDC comprised records of attendances to Emergency Departments at public hospitals. The MH-AMB contained records of mental health day programmes, care provided by community workers to admitted patients and clients in staffed community residential settings, psychiatric outpatient and outreach services, and mental health prevention services (Australian Institute of Health and Welfare, 2018). Records were restricted to those with a primary diagnosis of a mental disorder, and each day of care was counted only once, regardless of the number of individual services/presentations on any given date.
Sociodemographic factors
Demographic factors
Each participant’s month of birth was determined using their NSW Registry of Births Marriages and Deaths (RBDM) Birth Registration (2002–2005) record. The participant’s sex assigned at birth was determined via consensus across available records, and Aboriginal and/or Torres Strait Islander (Indigenous) background was indicated in either the child or their parent’s linked records. Measures of socio-economic status and geographical remoteness at birth, were derived according to the Australian Bureau of Statistics (ABS) (2006) Statistical Index for Areas (SEIFA) (ABS, 2008) and Remoteness Areas (derived from the Accessibility/ Remoteness Index of Australia; ARIA) (ABS, 2006), respectively, using postcode available in RBDM or Perinatal Data Collection (PDC) records. A SEIFA quintile variable was derived ranging from 1 (lowest SEIFA quintile) to 5 (highest SEIFA quintile; reference category), based on the ABS SEIFA deciles for the Index of Relative Socio-economic Disadvantage; geographic remoteness at birth was categorised as (1) major cities (reference category), (2) inner regional areas, (3) and outer regional, remote, or very remote areas.
Perinatal factors
Binary indicators of several perinatal factors were obtained from the NSW Ministry of Health or ACT Health Directorate’s PDC (2002–2005), including ‘maternal smoking during pregnancy’, and ‘obstetric complications’ (including hypertension, diabetes mellitus, pre-eclampsia, and/or gestational diabetes), and ‘multiparity’ (two or more prior pregnancies). Three categories of ‘maternal age’ at the child’s birth included: young maternal age (⩽21 years), advanced maternal age (>35 years), and maternal age 22–35 years (reference category).
Child maltreatment
Child maltreatment was indicated by at least one substantiated ‘risk of significant harm’ (ROSH) report, in which child protection caseworkers independently verified the veracity of a report of child maltreatment which could be made by various sources (e.g. other government department, the general public) to the NSW Department of Communities and Justice (ChildStory records, 2000–2020). A series of binary indicators of maltreatment were determined during early childhood (0–5 years), middle childhood (6–11 years), early adolescence (12–14 years), and/or later adolescence (15–17 years).
Mental disorder diagnoses
Mental disorder diagnoses were indicated in any primary or secondary diagnosis by an International Classification of Disease 10th Edition Australian Modification (ICD-10-AM) F-code (F00-F99) or any code for self-harm or suicidal ideation (X64-X80, R45.591, T14.91, or Y87.0) recorded in APDC, EDDC, MH-AMB. Eight, non-mutually exclusive, binary indicators of mental disorders included: ‘thought disorders’, ‘internalising disorders’, ‘non-psychotic depressive disorders’, ‘anxiety disorders’, ‘externalising disorders’, ‘cluster B personality disorders’, ‘neurodevelopmental disorders’, and ‘suicidal ideation and self-harm’. The Controlled Drugs Data Collection (CoDDaC; 2000–2020) subsystem was also used to identify children treated for hyperkinetic (attention deficit) disorders (included among neurodevelopmental disorders) and substance use disorders (included among externalising disorders). Full details of the childhood mental disorder variables generated are available in Supplementary Table 1. A series of 10 binary indicators (five per individual parent) were derived for parental mental disorders recorded during the prenatal period and each of the developmental periods as described above for child maltreatment.
Statistical analysis
Analyses were performed in RStudio v.1.3.1093 using R v.4.0.3 base software. To derive latent growth trajectories, latent class growth mixture modelling of the number of days of mental healthcare was performed using the crimCV package, which utilises zero-inflation Poisson models with cubic spline polynomials, in combination with leave-one-out cross validation (Nielsen et al., 2014). This approach considered 1–4 class solutions, with each model fitting repeated with 20 different initial values to increase the likelihood of converging on the true global solution. The optimal model was selected based on the Cross-Validation Error (CVE), Bayesian Information Criterion (BIC), and parsimony. Associations between sociodemographic factors and childhood mental disorders were explored via a series of log binomial regression analyses. Childhood mental disorders were assessed via a series of univariable models (one for each disorder) while sociodemographic factors were assessed via a series of multivariable models–one each for demographic factors, perinatal factors, maternal mental disorders, paternal mental disorders, and child maltreatment. All adjusted models accounted for sex. These analyses were repeated stratified by sex. Effect sizes were reported as risk ratios (RRs, and 95% confidence intervals [CIs]); RRs between 1.00 and 1.49 (or 1.00–0.67) were considered small, 1.50–2.49 (or 0.66–0.40) as medium, and 2.50 and over (or < 0.40) as large (Rosenthal, 1996). Where 95% confidence intervals did not include zero, they were considered statistically significant. Effects were taken to be significantly stronger/weaker than one another if their 95% confidence intervals did not overlap. All figures were plotted using ggplot2 (Wickham, 2016).
Results
There was a slightly higher proportion of girls in the study sample (n = 5050; 53.1%) than the population cohort (n = 44,216; 48.3%) from which the sample was drawn, and a higher proportion of children of Indigenous background (n = 1789 [18.8%]), compared with 7970 [8.7%] of the population cohort. However, the average age of the children at the end of the follow-up period (31st March 2021) was comparable across the study sample (mean age = 17.52 years) and population cohort (mean age = 17.48 years).
Latent trajectories
The model fit statistics for the latent class growth mixture model of the number of days treated for mental disorders are displayed in Table 1. Based on the CVE, the two-trajectory solution was the optimal model and was therefore selected for further analysis. While the BIC performed better for the 3- and 4-class solution, this solution increased the CVE and was less parsimonious. As seen in Figure 1 (and presented in Supplementary Table 2), most of the cohort exhibited a low service use trajectory (n = 7649, 80.4%), with the average number of days treated for mental disorders increasing only marginally between early childhood (0–5 years) and late adolescence (15–17 years) accounting for only 31.2% (68,495 days of care) of the overall mental health service use of the cohort. The remainder of the children demonstrated a high service use trajectory (n = 1861, 19.6%), with the average number of days treated for mental disorder increasing from approximately 2.65 in early childhood to over 41.37 in late adolescence, and accounting for 68.8% (151,282 days) of the cohort’s total days of mental health care. Children with high-use attended services slightly earlier (M = 11. 23, SD = 4. 31) relative to those with the low-use (M = 11.80, SD = 4.66) trajectory (t = 5.048, p = 4.73 × 10-7). There was no difference in the mortality rate (n = 27, 0.3%) between the latent trajectories (Fisher’s p = 0.635).
Summary of model fit matrices for 1, 2, 3, and 4 latent class growth mixture models for number of days of mental healthcare received in childhood and adolescence (n = 9, 510).
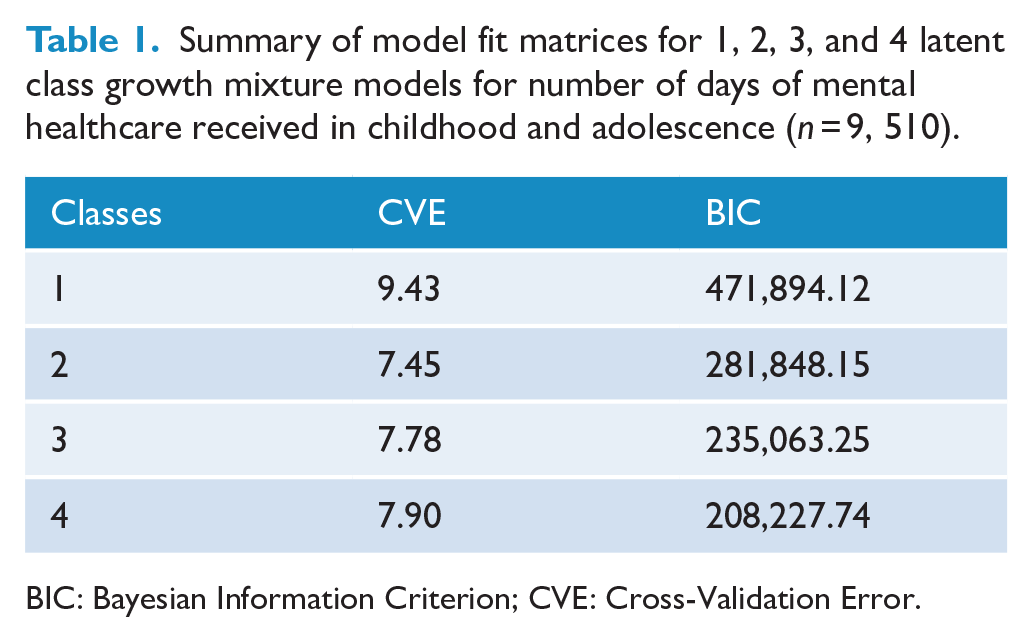
BIC: Bayesian Information Criterion; CVE: Cross-Validation Error.
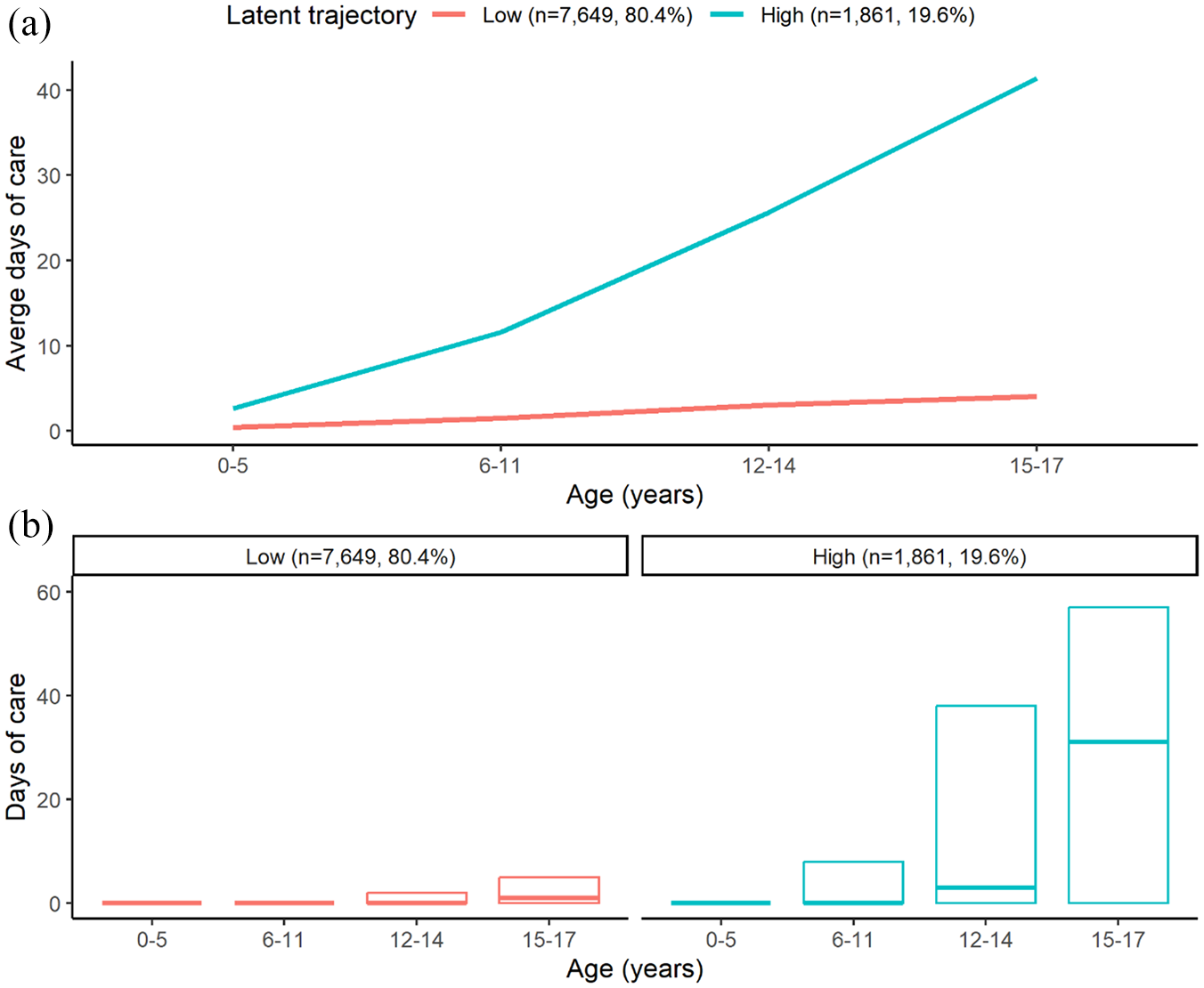
(A) Average and (B) median and interquartile range of number of days of mental healthcare received during childhood and adolescence by children in each latent trajectory.
Diagnostic comparison between latent trajectories
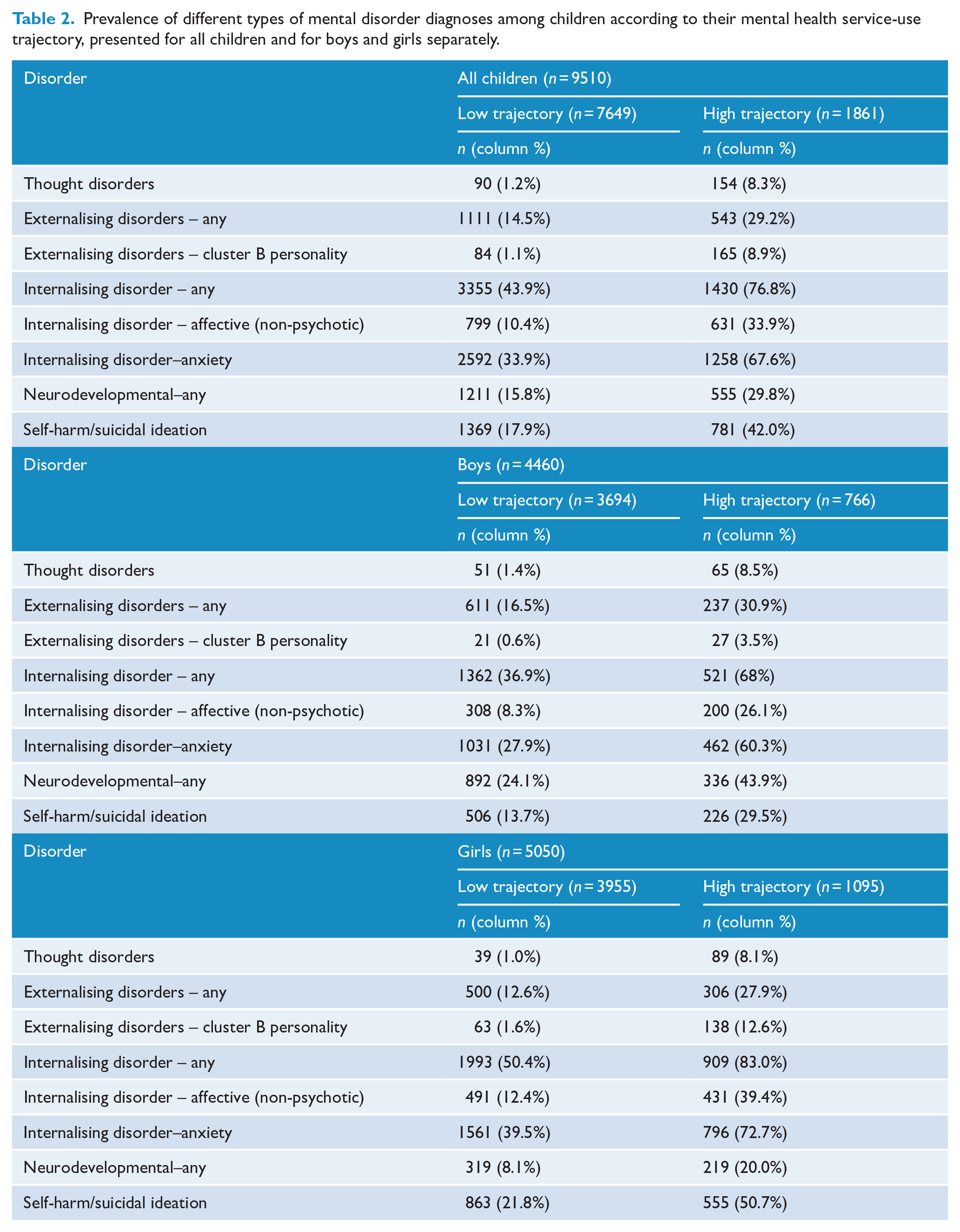
The incidences of different mental disorders among all children in each latent trajectory, and for boys and girls separately, are displayed in Table 2 with unadjusted RRs depicted in Figure 2. All types of mental disorder were more common among children in the high service use trajectories (relative to the low trajectory) but the strength of effects varied across diagnostic groups and trajectories (see Figure 2). For example, cluster B personality and thought disorders were most strongly associated with the high-use trajectory, followed by internalising disorders in general, and in terms of anxiety and non-psychotic affective disorders, respectively. Diagnoses of externalising disorders, neurodevelopmental disorders, and self-harm/suicidal ideation were also all more likely to be diagnosed in the high-use (relative to the low-use) trajectory, but with smaller effect sizes. Findings were similar when boys and girls were examined separately, with a trend towards associations being stronger in girls (see Figure 2B and Supplementary Table 3). Anxiety disorders were the most common first diagnosis (of those examined) for both trajectories, particularly for children in the high-use trajectory class (see Supplementary Table 4).
Prevalence of different types of mental disorder diagnoses among children according to their mental health service-use trajectory, presented for all children and for boys and girls separately.
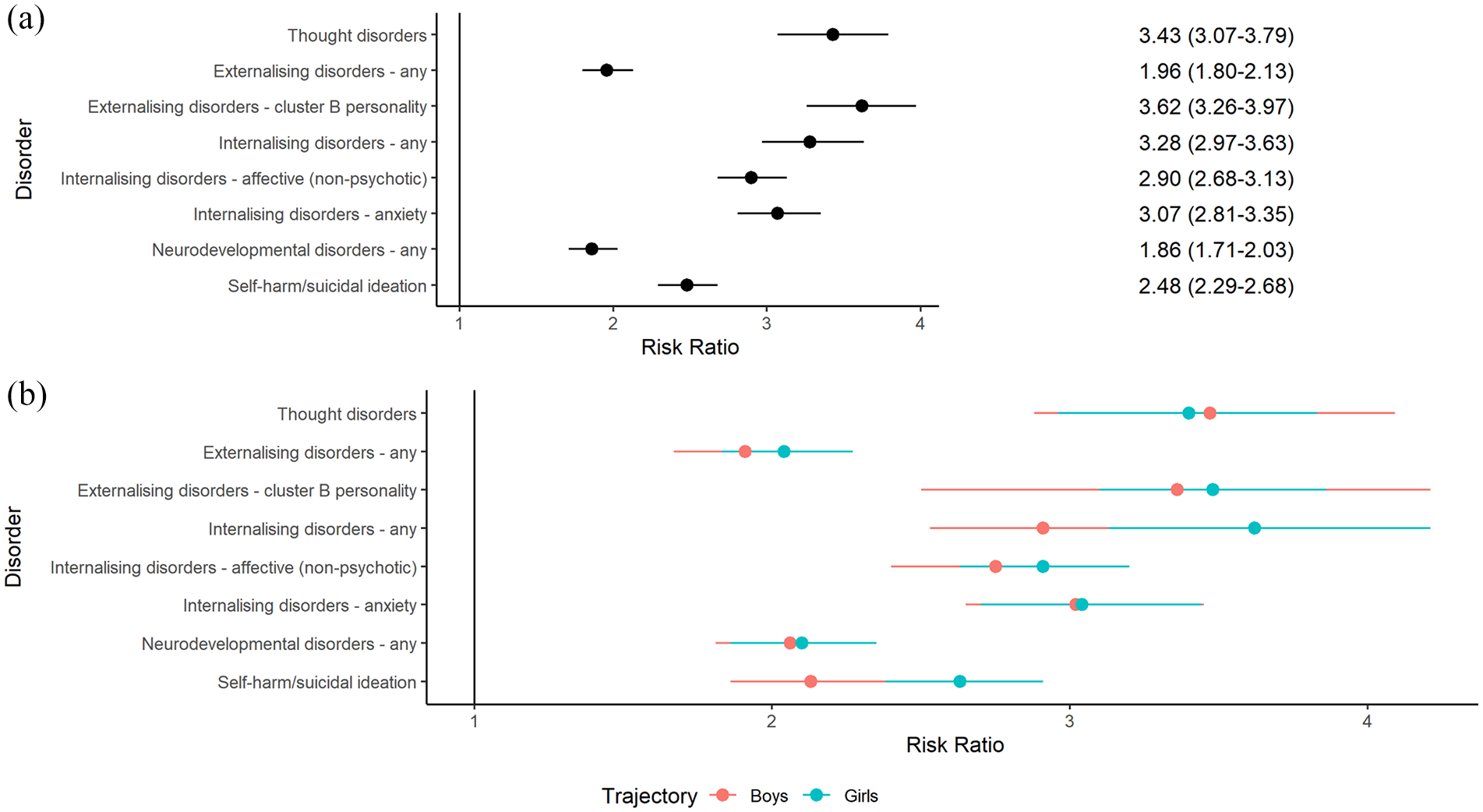
Unadjusted relative risk ratios for membership in the high mental health service use trajectory according to different types of mental disorder diagnoses for (A) all children and (B) boys and girls separately.
Sociodemographic and other risk factors and latent trajectories
The descriptive statistics for sociodemographic and other risk factors across the mental health service use trajectories are displayed in Table 3, with corresponding adjusted RRs displayed in Figure 3. Girls were 27% more likely to be classified as high service users, relative to boys. Advanced maternal age and smoking during pregnancy were weakly associated with increased risk of being classified in the high-use trajectory. Maternal mental illness, regardless of the child’s developmental periods, was associated with the high-use trajectory development in the unadjusted models; but only maternal mental illness that occurred in early childhood (0–5 years) remained significant in the adjusted model. In contrast, paternal mental illness throughout childhood (but not in the prenatal period), was associated with the children’s high service use in unadjusted models; but only parental mental illness recorded during the child’s later adolescence (15–17 years) remained significant in the adjusted model. Finally, child maltreatment reported in adolescence was moderately associated with membership in the high-use trajectory (albeit slightly attenuated in adjusted models); while child maltreatment in early-middle childhood was weakly associated with the high-use trajectory, but only in unadjusted models.
Descriptive statistics for sociodemographic/other risk factors in low and high mental health service-use trajectories (n = 9510).
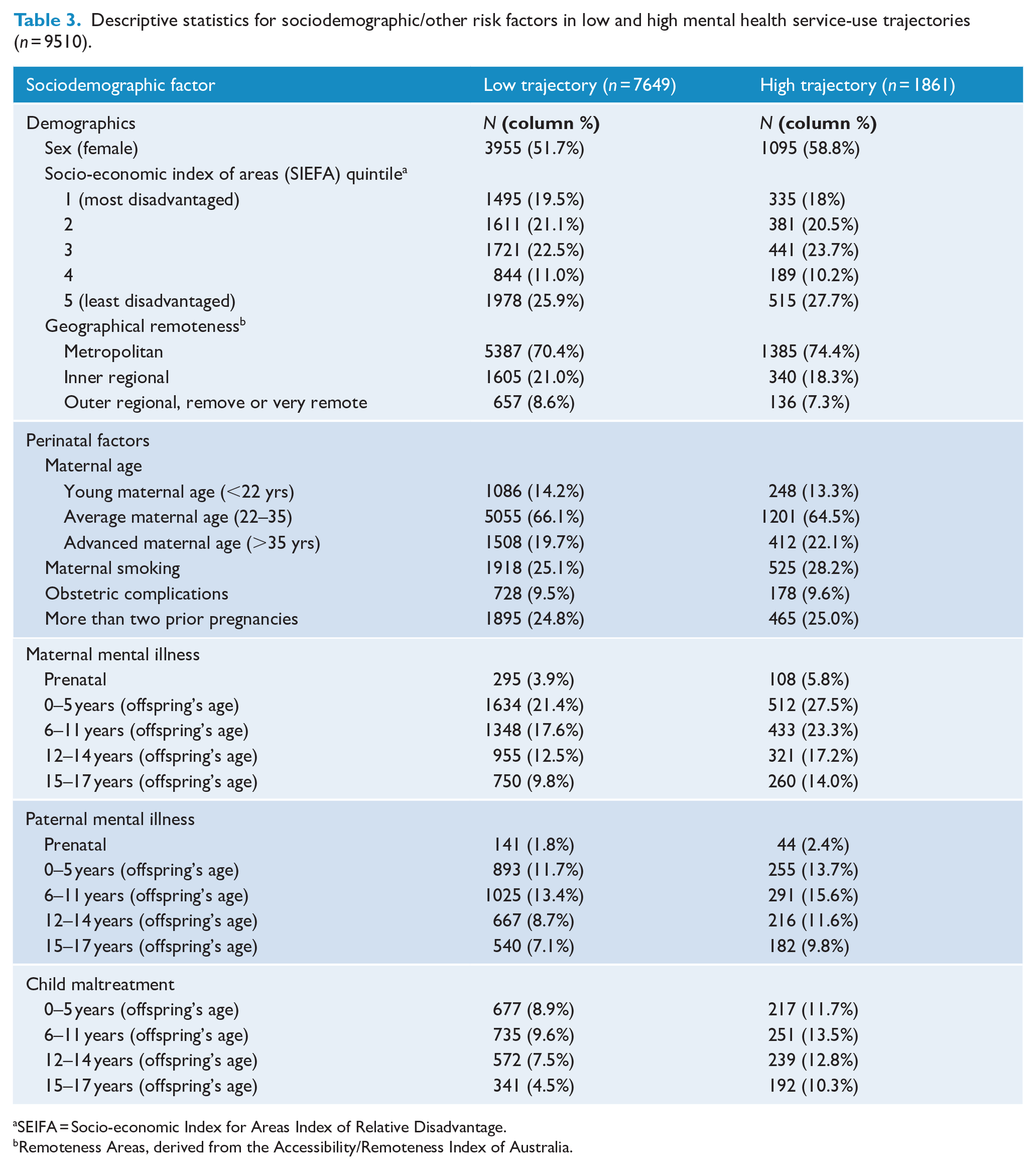
SEIFA = Socio-economic Index for Areas Index of Relative Disadvantage.
Remoteness Areas, derived from the Accessibility/Remoteness Index of Australia.
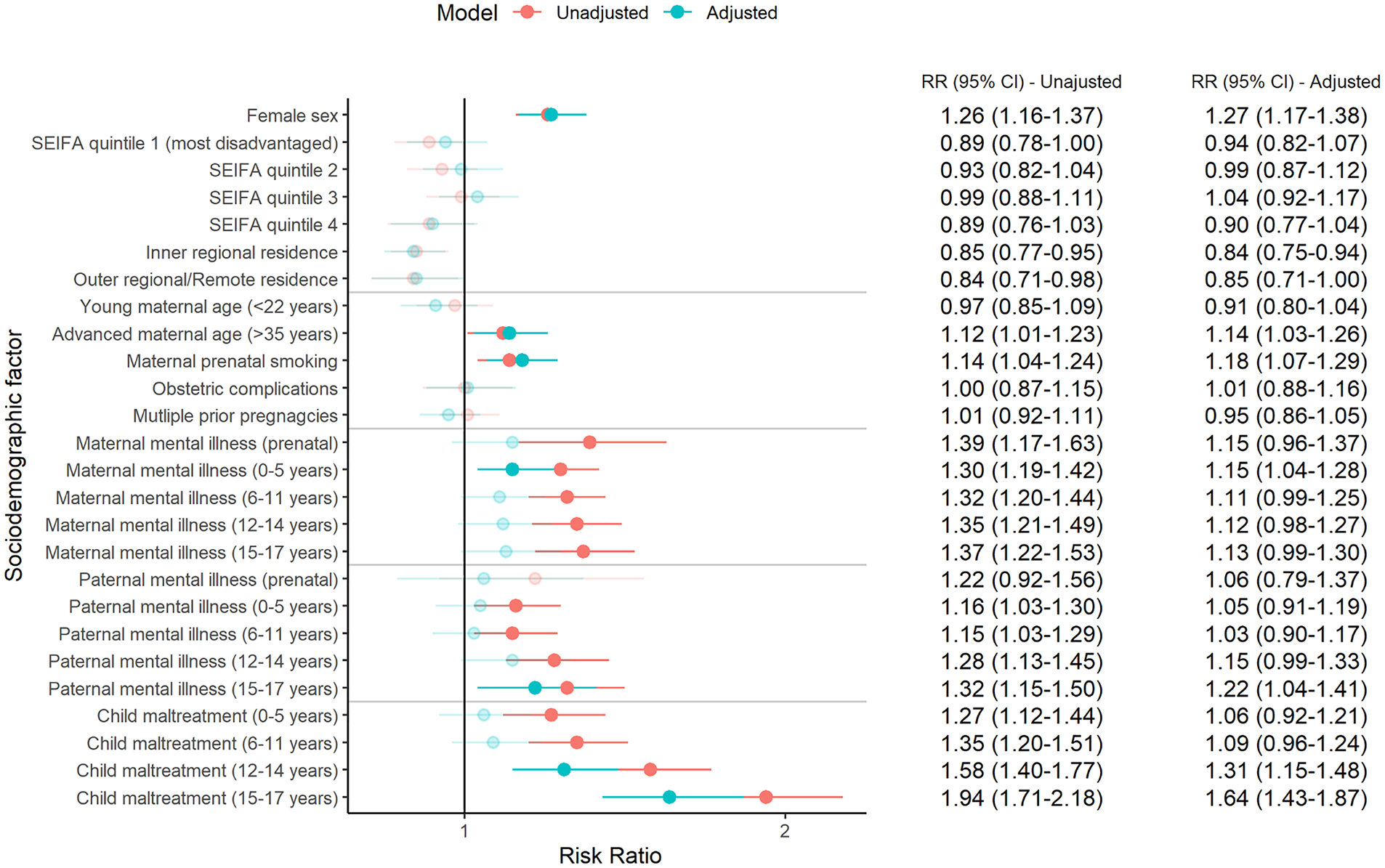
Adjusted relative risk ratios for membership in the high service use trajectory according to sociodemographic/other risk factors.
Associations between sociodemographic/other risk factors and mental health service use trajectories are displayed for boys and girls separately in Figure 4 (see Supplementary Tables 5–8 for descriptive statistics and unadjusted RRs). Among boys, maternal prenatal smoking, maternal mental illness in early-middle childhood, paternal mental illness in early childhood and early adolescence, and child maltreatment in middle childhood and early adolescence were associated with increased risk of membership to the high-use trajectory in adjusted models. In contrast, girls exposed to advanced maternal age, prenatal maternal smoking, maternal mental illness prenatally and in late adolescence, paternal mental illness in late adolescence, and child maltreatment during adolescence were more likely to be members of the high-use trajectory.
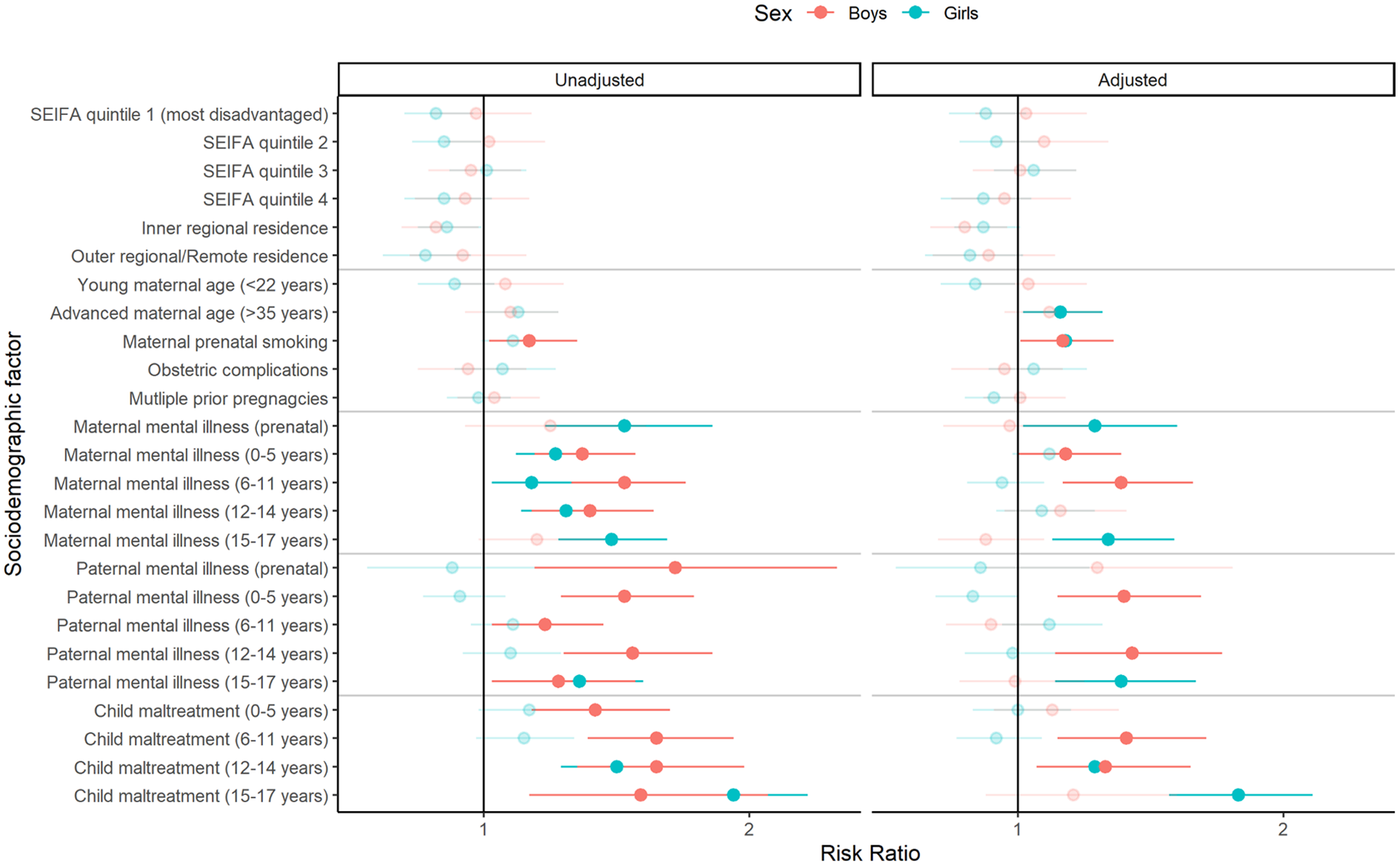
Adjusted risk ratios for membership in the high service use trajectory according to sociodemographic/other factors, for boys and girls separately.
Discussion
Two distinct trajectories of mental health service use were identified among 9510 children between birth and 17 years of age: a low-use trajectory accounted for 80.4 of children and a high trajectory, in which mental health service use increased markedly with age, accounted for 19.6% of children. Children in the high-use trajectory accounted for more than 68.8% of the total days of mental health treatment for the entire sample, were more likely to be female, and to have all mental disorder diagnoses (especially thought disorder and cluster B personality disorders), relative to children in the low-use trajectory. Maternal smoking during pregnancy, advanced maternal age, parental mental disorders, and child maltreatment were also each associated with membership in the high-use trajectory.
These findings are broadly consistent with previous evidence of a small subgroup of the adolescent population (typically less than 20%) who show a more pervasive or worsening trajectory of mental health symptoms (or service use) over time (Abdin et al., 2017; De Lijster et al., 2019; McCauley et al., 2020; Musliner et al., 2016; O’Driscoll et al., 2021; Olino et al., 2010; Waizbard-Bartov et al., 2021). The identification of individuals likely to develop chronic or declining mental ill-health is important to be able to meet their needs, but is also critical from a public health perspective, as these individuals typically account for a disproportionate amount of wider social service use in adulthood (Caspi et al., 2016; Rivenbark et al., 2018) consistent with this study. Despite multiple methodological differences in sampling, data ascertainment, length of follow-up, and type of outcome, the present study identified similar trajectories of low and increasing mental health use throughout childhood and adolescence.
Child maltreatment in adolescence was strongly associated with membership in the high-use trajectory, when mental health service use also peaked. This may be attributable to the cumulative impact of trauma across childhood and adolescence since few maltreated children experience trauma limited to a single developmental period (Russotti et al., 2021; Warmingham et al., 2019). Alternatively, adolescence may be a critical period during which traumatic incidents significantly impact mental health (Fuhrmann et al., 2015). This interpretation is consistent with recent evidence of developmentally sensitive periods, during which specific types of adversity, occurring within different developmental periods, may modulate brain development in regions relevant to processing threatening stimuli (Zhu et al., 2023). While we cannot rule out reverse causality (i.e. NSW health services may have been the first to notify child protection services about a child presenting with mental health problems between 12 and 17 years of age), considerable evidence suggests a causal association between child maltreatment and mental disorders (Grummitt et al., 2024; Schaefer et al., 2018) across all major diagnostic groups, and maltreatment may occur for prolonged periods of time before a report is eventually made (Cashmore et al., 2017).
Parental mental disorders diagnosed in various developmental periods of the offspring were associated with high service use among children, consistent with existing evidence (Musliner et al., 2016; Olino et al., 2010); this may reflect genetic and/or environmental contributions (or both) that cannot be determined with the available data. The lack of effects for maternal mental illness in the prenatal period (in the adjusted model) conflicts with previous evidence of long-term negative impacts of maternal mental illness during pregnancy on the mental health of offspring (Van den Bergh et al., 2020). However, prenatally recorded maternal mental illness did significantly increase the risk of high mental health service use among girls (but not boys). Further gender differences were evident in the developmental periods during which high mental health service use among children appeared to be related to maternal and paternal mental disorder diagnoses. Replication of this finding is warranted to verify these findings and substantiate their clinical implications.
In terms of other prenatal factors, only maternal smoking during pregnancy and advanced maternal age remained significantly associated with high service use after controlling for other factors, consistent with multiple previous studies (Gaysina et al., 2013; Green et al., 2022; Moylan et al., 2015), although it is noted that there has been some failure to replicate these associations (Obel et al., 2016; Quinn et al., 2017), suggesting the influence of other forms of disadvantage that occur in tandem with maternal smoking (Quinn et al., 2017). The relationship between advanced maternal age and offspring mental illness is similarly well-established, for which mechanisms remain unclear (Tearne, 2015).
Girls were more likely than boys to be classified in the high-use trajectory, consistent with previous evidence showing that females are more likely to present for mental health problems (Altemus et al., 2014; Mackenzie et al., 2012; Maselko, 2017), and with a prior latent trajectory analysis of depression and anxiety disorders (Olino et al., 2010). Conversely, higher service use is associated with first-episode psychosis (Abdin et al., 2017), and a greater extent of total difficulties in childhood (Vella et al., 2019). Sex differences in mental health service use trajectories may thus reflect diagnostic patterns. Further research is needed to establish whether males may develop later onset mental health difficulties not reflected in this study due to the limited age range of the cohort.
There are several limitations worth considering. First, all information on service use was drawn from NSW and ACT inpatient, public ambulatory, and emergency department services. As other sources of mental health support provided outside of these services (e.g. psychologists, private psychiatrists, counsellors, and general practitioners) were not captured, the full extent of treatment for mental health problems would be underestimated in this study. The quality of diagnoses in these various record sets was also likely to vary according to heterogeneity in assessment and diagnostic practices across the various contexts from which these data were derived. Similarly, some children may have been incorrectly coded as not maltreated if instances of maltreatment were either not reported, or insufficiently investigated to determine the veracity of a maltreatment report. Self-reported measures of maltreatment could overcome such limitations but are themselves subject to recall and response biases. Second, individuals may have been incorrectly classified as not having a mental disorder, and/or the extent of services used for mental health treatment may have been underestimated if they had emigrated interstate or abroad. Third, we were unable to examine mental health service use in gender diverse groups (e.g. trans, non-binary, and intersex young people) as gender identity and sex assigned at birth were not differentiated in the linked administrative data. However, the advantages of this study include the considerable sample size, reduced selection or recall bias, availability of parent data, length of follow-up, focus on the service use as the unit of study (rather than symptoms), and the ability to examine all periods of child and adolescent development.
In summary, a minority (19.6%) of the 9510 children with mental disorders diagnosed in administrative health records demonstrated patterns of high contact with mental health services (public and ambulatory) over the course of childhood and adolescence. These children made up less than one-fifth of the sample but accounted for 68.8% of the overall number of days of mental healthcare rendered to the cohort. The potential economic value of identifying this high-use group for early intervention is significant (Caspi et al., 2016). A range of factors, including female sex, maternal smoking during pregnancy, parental mental disorder, and child maltreatment, were all associated with membership in the high mental health service use trajectories; as were certain psychiatric conditions, particularly cluster B personality and psychotic disorders. Further research is warranted to assess the predictive utility of these and other risk factors for the prospective identification of children likely to use mental health services heavily in adolescence. The provision of targeted, multi-disciplinary interventions would provide a cost-effect means of substantially reducing the personal and public health burden associated with high mental health service use in young people.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251324805 – Supplemental material for Latent trajectories of mental health service use in an Australian state population cohort of children
Supplemental material, sj-docx-1-anp-10.1177_00048674251324805 for Latent trajectories of mental health service use in an Australian state population cohort of children by Oliver J Watkeys, Stacy Tzoumakis, Kimberlie Dean, Kristin R Laurens, Felicity Harris, Kirstie O’Hare, Vaughan J Carr and Melissa J Green in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This research used population data owned by the NSW Department of Education; Australian Curriculum, Assessment and Reporting Authority (ACARA), managed by the NSW Education Standards Authority; NSW Department of Communities and Justice; NSW Ministry of Health; ACT Health; NSW Registry of Births, Deaths and Marriages; the Australian Coordinating Registry (on behalf of Australian Registries of Births, Deaths and Marriages, Australian Coroners and the National Coronial Information System); Australian Bureau of Statistics; Australian Institute of Health and Welfare; Department of Social Services; NSW Bureau of Crime Statistics and Research, and; NSW Police Force. This research used data from the Australian Early Development Census (AEDC). The AEDC was funded by the Australian Government Department of Education. The findings and views reported are those of the authors and should not be attributed to these Departments, or the NSW and Australian Government. Record linkages were conducted by the NSW Centre for Health Record Linkage (CHeReL).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted by the University of New South Wales with financial support from the National Health and Medical Research Council (NHMRC) Project Grant (APP1148055), and Investigator Grant (APP1175408 awarded to K.D.); Australian Research Council (ARC) Discovery Project (DP230101990) and Discovery Early Career Researcher Award (DE210100113 awarded to S.T.); Department of Health and Aged Care Medical Research Future Fund Million Minds Mental Health Grant (APP2006436); Toyota Manual Handling Australia, and; a Postdoctoral Fellowship from Suicide Prevention Australia (awarded to O.W.).
Data Availability
Data used in this project has been provided by government or other agencies for the research purposes of the NSW Child Development Study and is unable to be shared with third parties or deposited into data repositories. Researchers wishing to access these data need to apply in writing to relevant data custodians.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.