
Abstract
There is a high prevalence of depressive disorders in children and adolescents up to 18 years of age [1,2] and these disorders have a significant negative impact on social and occupational functioning [2,3]. Of particular concern is the link between depression and completed suicide in young people [4–8]. In the last few years, research has indicated that not only are those with untreated depression at risk of suicide, but that young people up to the age of 25 who are treated with antidepressant medication are more likely to experience an increase in suicidal ideation and suicide attempts [9–11].
This research has led to controversy about what constitutes optimal treatment for depressive disorders, particularly with regard to the role of medication [12–15]. There is a relative paucity of large, representative and well-conducted trials in young people [12,16,17], particularly those that include participants with severe, complex disorders and suicide risk. In this context, guideline recommendations that aid clinicians to make evidence-based treatment decisions that maximize the chance of recovery and minimize the risk of suicidal behaviour, are essential. A number of guidelines for the treatment of depression in young people exist [18–21], most recently an Australian guideline [22]. Key recommendations are relatively consistent across these guidelines, encouraging practitioners to engage in a model of care that sequences interventions from those that are low intensity for mild presentations to more intensive psychotherapy and medication (fluoxetine first line) interventions for more severe presentations, and to ensure close monitoring of emergent suicidality.
However, despite the existence and dissemination of guidelines, it is widely recognized that the incorporation of evidence-based recommendations into everyday clinical practice is far from universal among clinicians [23]. For example, a study of antidepressant use in young people in Australia between 2003 and 2005 showed sertraline was more commonly used [24]; American research indicates that monitoring of symptoms and adverse events after prescription of an antidepressant is vastly below what is recommended [25]; and UK research shows less than 100% compliance with guideline recommendations [26]. The uptake of evidence into everyday clinical practice is best supported by interventions that are specific to the setting, and tailored to address specific barriers to the use of guidelines both at an individual, local and systemic level [23,27–29]. While there are some examples of this approach in mental health [30], little has been done in the area of youth depression. Therefore, we sought to examine potential barriers to the use of evidence-based guidelines for youth depression in a tertiary specialist mental health service.
Materials and methods
Study design
This was a qualitative study using a social constructionist perspective (that assumes individuals and groups participate in the construction of their perceived reality in an ongoing dynamic process) [31,32], to undertake focus groups. The local ethics review committee approved the study (Melbourne Health Research and Ethics Committee; reference number 2008.18).
Setting
The research took place at Orygen Youth Health (OYH). OYH is the public youth mental health service for young people aged 15–24 living in the north-western metropolitan area of Melbourne, Australia. For the purposes of this paper we will refer to OYH as a tertiary service in that we receive referrals from primary services (e.g. general practitioners) and secondary services (e.g. paediatricians), although we accept any referrals, including direct referrals from young people themselves, their caregivers, or places such as education settings. Once accepted by the service, clients are allocated to specialized treatment teams. Focus groups were held with six clinical programme teams and with a group of psychiatrists who work across these teams (indicated as MEDICAL in the results section). The clinical programmes included the Personal Assessment and Crisis Evaluation (PACE) team for young people considered to be at incipient risk of developing a psychotic disorder, the Early Psychosis Prevention and Intervention Clinic (EPPIC) for young people experiencing a first episode of psychosis, the Youth Mood Clinic (YMC) for moderately and severely depressed young people, the Helping Young People Early (HYPE) clinic for emerging borderline personality disorder, the Intensive Mobile Youth Outreach Service (IMYOS) for YMC and HYPE clients who need outreach assistance, and the Youth Access Team (YAT) who provide three main functions: triage by telephone for all referrals, assessment and allocation to the most appropriate clinic, and a 24 hour acute service for OYH clients in crisis. The majority of these clinics have some clinic-specific guidance about management of young people in their clinic; however, with the exception of the YMC, this is not specific to treating depression. The YMC clinic guidance is broadly consistent with guideline recommendations in that they propose cognitive behavioural therapy (CBT) as a first line treatment and selective serotonin reuptake inhibitor (SSRI) fluoxetine as the first line medication. There is no specific guidance within the organization about using externally produced guidelines.
Participants
All clinicians (psychiatrists approximately 29%, nurses approximately 14%, allied health professionals including psychologists approximately 32%, occupational therapists approximately 14%, and social workers approximately 12%) from OYH who gave informed consent were eligible for inclusion in the study. Therefore, the term ‘clinician’ when used in the results refers to any of these professionals unless specified. Each clinical team consists of a slightly different mix of clinicians with IMYOS, PACE, HYPE, YMC and PACE made up of allied health professionals, while YAT has approximately 50% nurses and 50% allied health professionals and EPPIC has approximately 15% nurses and 85% allied health professionals. Clinicians had between 0.5 and 18 years experience in youth mental health.
Participants were recruited between January and August 2010. The project was presented at staff and clinical review meetings, after which all clinicians were invited to participate. A time for the focus group was arranged with each team separately.
Data collection
Two of the authors (M.S. and S.H.) facilitated the focus groups using a semi-structured focus group schedule. The schedule was designed to ‘lead’ the participants as little as possible, and the dialogue between the facilitator and participants was treated as equally relevant to the data. Participants were given a written copy of the four key recommendations of the NICE guidelines for the treatment of depression in children and adolescents (see Figure 1). These recommendations were chosen as exemplars of the recommendations made in similar guidelines internationally and in the absence of published Australian guidelines. Subsequent to this study, Australian guidelines have been published, with recommendations entirely consistent with those presented to the focus groups (CBT/IPT as first line treatment for moderate to severe depression with fluoxetine considered if the psychological treatment is not effective, although no guidance is given about how long psychological therapy should be trialled before fluoxetine is considered; close monitoring is recommended with similar guidance as to the timing). Participants were asked to comment on barriers (‘things that make it difficult to do’) to following these recommendations. The focus groups were audio recorded and transcribed using an orthographic (verbatim) style, and field notes were taken during each focus group by M.S. or S.H. Each focus group was attended by between 8 and 12 clinicians with attendance varying between 75% and 85% of clinicians working on the day of the focus group. Each focus group lasted between 23 and 48 min (mean time = 36.4 min).
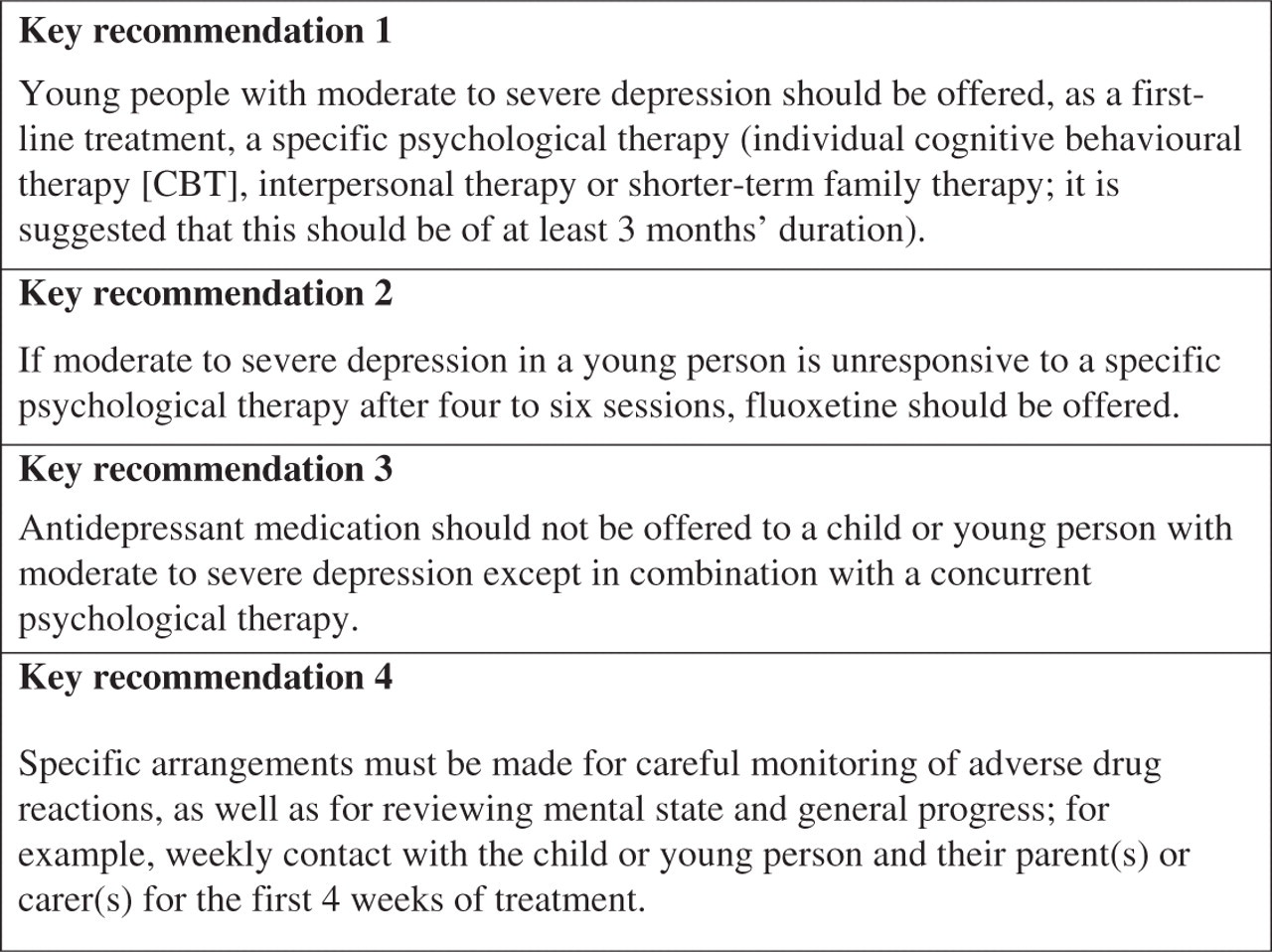
Key recommendations from the NICE guideline.
Data analysis
Due to the lack of research in this area our primary aim was to obtain a descriptive account of the barriers to implementing the key recommendations from the NICE guideline. We used thematic analysis with initial coding undertaken by two authors (S.H. and M.S.). The main themes that arose were barriers that exist at (i) the individual clinician level, (ii) the clinical level in terms of the presentation of young people, and (iii) the systemic or service level. Barriers identified in the data were therefore classified according to these themes in subsequent coding.
Results
Recommendation 1
“Young people with moderate to severe depression should be offered, as a first-line treatment, a specific psychological therapy (individual cognitive behavioural therapy [CBT], interpersonal therapy or shorter-term family therapy; it is suggested that this should be of at least 3 months duration).”
Individual clinician
Across all clinics, except EPPIC (who primarily treat psychosis and stated a preference to see psychosis resolved before diagnosing and treating depression), clinicians expressed a belief that medication was necessary earlier for severe and complex presentations: ‘[if they are] severe, I think they should be offered medication first’ (YMC). If therapy could not be initiated, for whatever reasons, there was an implied belief that it would be unethical to withhold medication: “One often feels more compelled to prescribe because, just because of the long delay. So if a patient was coming into Orygen, it could easily be a 6 to 8 week delay before you start any sort of psychological intervention for depression. That's unethical to just hold a patient for that long without an intervention” (MEDICAL).
Clinical presentation
Clinicians from several clinics stated that the guidelines were not suited to tertiary services, highlighting the lack of evidence specific to the severe and complex presentations of young people who often had comorbid diagnoses, suicide risk, significantly impaired functioning, few supports or social networks, unstable or unsafe accommodation, and extreme financial hardship. Clinicians highlighted that such young people are often too unwell to do therapy: ‘if ultra severe, then I would suggest there's not much point going into therapy just yet’ (YMC). Clinicians also stated that young people themselves, especially those with severe and complex presentations, were sometimes reluctant to engage in therapy.
Service level
Clinicians described one barrier related to the wider system of care. The primary issue was that young people were often already on medication ‘Australia doesn't have a tiered system like the UK – some young people come straight to a tertiary service’ (HYPE).
There were also barriers at the local system level in that medication was often commenced at YAT before young people were seen by the specialist clinics. Another barrier was the lack of availability of doctors, with limited access to doctors influencing the timing of medication prescription: “So if you choose one week not to commence medication but you can't get an appointment with your doctor to see that client for another month, are you going to be able to hold off on the decision? Probably not” (EPPIC).
A lack of psychologists both within and outside the service, and a lack of clinicians trained specifically in CBT or IPT was seen as a barrier by medical staff and clinicians in YAT, EPPIC and IMYOS. Clinicians from all clinics were unclear about what ‘therapy’ meant in the guideline and were concerned that the ‘guideline (recommendation) doesn't acknowledge the importance of case management or engagement’ (YMC).
Large caseloads were an issue, particularly in EPPIC, where case managers might only see a client every 2 or 3 weeks. In this situation, 6 weeks of therapy can take many months to deliver, with some clinicians stating it was ‘unreasonable’ not to commence medication.
Recommendation 2
“If moderate to severe depression in a young person is unresponsive to a specific psychological therapy after four to six sessions, fluoxetine should be offered.”
Individual clinician
Most clinicians acknowledged fluoxetine should be first-line medication, but clinicians in several clinics (YAT, PACE, EPPIC, MEDICAL) expressed a belief that, depending on the presenting issues of the client, guideline recommendations need not be adhered to:
“Rather than prescriptively being told to use fluoxetine, we try to manage symptoms. So if they are having problems with sleep, we look for medication that's going to help with that” (YAT).
Medications other than fluoxetine were offered by doctors due to a belief that fluoxetine made anxiety symptoms worse. As for recommendation 1, clinicians expressed a view that medication should be started earlier for severe and complex presentations. On the other hand clinicians in several clinics stated ‘four weeks of therapy is not enough to give therapy a go for somebody who has severe [depression]’ (PACE).
Clinical presentation
Engaging young people in medication treatment was at times endorsed as a barrier: ‘I've got a patient who isn't keen on medication’ (YMC). Clinicians from the majority of clinics saw patient choice as an important factor in treatment decision-making. Engaging the young person's family was also stated to be a barrier, with clinicians preferring that the family be involved: ‘obviously you need the support of the family’ (YAT). Medical staff highlighted the potential of negative media about antidepressants to influence young people's and carers' views about medication.
The relevance of guidelines was again cited as a barrier by several clinics; the (NICE) guidelines were relevant only for those up to the age of 18.
Service level
Similar system level barriers were highlighted as for recommendation 1 with clinicians stating there was little choice about the timing or type of medication if young people were already on medication. Other barriers included within-clinic procedures that did not include a standard 4 to 6 week review. YMC clinicians, on the other hand, stated ‘if anything is not working after 4 to 6 weeks, then the treatment should be reviewed and changed.’ Finally, orientation of new registrars to the service was cited as a potential barrier with clinicians stating they noticed more prescriptions of medication other than fluoxetine when new registrars began.
Recommendation 3
“Antidepressant medication should not be offered to a child or young person with moderate to severe depression except in combination with a concurrent psychological therapy.”
Individual clinician
A belief that it was better for young people to have some treatment (i.e. medication in the context of some case management) than no treatment at all was a barrier described by clinicians in three clinics (YMC, IMYOS and HYPE). One of the medical staff suggested that ‘if it is a very early stage, you want to just make sure they are taking medication and getting some response’, highlighting the concern clinicians have to see treatment responsiveness.
Clinical presentation
Similar to barriers for recommendation 1, difficulty engaging a young person in therapy was seen as a barrier: ‘there's a group with depression as part of intellectual disability or autism who are essentially harder to engage in therapy’ (YMC). These are different examples of the type of complex and severe presentations seen in public mental health services, and clinicians consistently highlighted how difficult young people with these types of presentations were to engage in therapy.
Service level
Clinic-based care was stated to be a barrier as young people can find it difficult attend sessions. It was suggested by several clinics that a young person who was only interested in medication would probably be linked in with a GP (via a referral either back to the GP who referred the young person or to a GP known to the service to be ‘youth friendly’ and with a particular interest in mental health disorders), although YMC clinicians stated that they would be ‘chasing them for a few months.’
As for recommendation 1, clinicians highlighted the lack of clarity about the term ‘therapy’, stating that they ‘do psychological interventions but it's not therapy’ (YAT). Many of the clinicians stated that they use ‘psychologically informed case management’ and were uncertain whether this is what is referred to in the guidelines. It is unclear exactly what clinicians are delivering in this case.
Similar to barriers cited for recommendation 1 and 2, some clinics highlighted the lack of psychologists and the fact that young people may have already been prescribed mediation by a GP without the commencement of psychological treatment.
Recommendation 4
“Specific arrangements must be made for careful monitoring of adverse drug reactions, as well as for reviewing mental state and general progress; for example, weekly contact with the child or young person and their parent(s) or carer(s) for the first 4 weeks of treatment.”
Individual clinician
While clinicians across all clinics were confident about their ability to undertake a mental state examination and monitor risk, non-medical clinicians stated they felt ‘professionally incompetent’, asking and discussing physical symptoms (PACE) and were unsure about what side effects to monitor (PACE and EPPIC). Clinicians stated they tended to ask general questions about ‘any side effects’ rather than about specific side effects (EPPIC). While non-medical clinicians would not be expected to monitor side effects of medication, it is the case that they are in regular contact with their clients and therefore in a position to be able to screen for and report to the medical staff any side effects noted, in what is a team-based approach to care.
In terms of using standardized tools for undertaking monitoring of symptoms and adverse effects, only the YMC clinic had implemented the PH9 [33], a self-report depression severity measure, to monitor symptoms (at entry and review); however, clinicians stated that ‘pulling out an instrument … could be a bit counter-productive and a bit impersonal.’ Clinicians stated they tended to rely on spontaneous report: [we] ‘encourage people to get in contact with us by phone, particularly if there's an emergent suicidal reaction’ (HYPE). Clinicians in several clinics were keen on a system whereby young people were encouraged to be involved in self-monitoring and contact them if they were experiencing side effects, with clinicians in one clinic highlighting the heavy load of mandatory outcome measures as a barrier to using further standardized tools.
Clinical presentation
The majority of clinics stated that severity and complexity of presentation was a barrier to any form of monitoring in young people who were difficult to engage, did not attend and were difficult to contact.
Service level
Communication between clinicians was stated to be a barrier with, for example, clinicians in the YMC clinic citing delays in the transfer of clients from YAT to a case manager as a barrier whereby there may be a ‘variable amount of time … before they see the OCM … people probably go for a few weeks without anyone checking them.’
Clinicians in several clinics stated that a lack of availability of clinicians, particularly medical staff, was a barrier to routine monitoring as the young person's own doctor may not be available or that ‘its difficult to fit people within that [guideline recommended] timeframe. There's just no appointments free’ (HYPE). In terms of other resources, a lack of simple but thorough information on medication and their side effects was stated to be a barrier. This is in the context of existing OYH resources about medication, as well as a range of other information including online resources, that clinicians did not think was entirely appropriate for their use.
Discussion
Principal findings
The results of our study show that the key barrier to implementing guideline recommendations was clinician belief that the guideline recommendations were not relevant to many of the young people who present to a tertiary level mental health service. Clinicians stated that because young people presenting to the service often had severe and complex depression, including high suicide risk, medication was often required earlier than guidelines recommended, that fluoxetine may not be the medication of choice depending on the mix of symptoms, and that it was difficult to deliver psychological therapy. Patient preference was cited as a barrier to delivering guideline recommended care. Furthermore, clinicians agreed that the importance of delivering support and case management to address client's needs was neglected in guideline recommendations.
Service level barriers included a lack of psychologists to deliver psychological interventions, as well as a lack of medical staff to provide regular review and guideline recommended monitoring. Monitoring of side effects was a passive process that relied on spontaneous report from the client, or general enquiry about side effects due to a perceived lack of expertise and a lack of time. In terms of the wider system, young people were often already on medication with little information about their treatment history when they presented to the tertiary service, making sequencing interventions according to guideline recommendations impossible.
Strengths and weakness of the study
This study had a high rate of participation and a large sample size, which increases generalizability significantly. However, we did not have 100% participation, and focus group methodology cannot ensure that all possible views are captured. It is interesting that while clinicians included in this study are from different clinics, treating different populations, and have different philosophies and staff mix, there was relatively high reported concordance with regard to barriers to implementing guideline recommendations. This is no doubt reflective of common organizational issues and approaches that aim to meet the needs of a population with severe and complex needs.
The findings may not be broadly applicable to services other than public mental health service for youths aged 15 to 25. However, it is likely that other public mental health services such as child and adolescent mental health services, which have a similar mix of professionals and see a similar group of clients in terms of presenting issues albeit of a younger age, may experience similar barriers to implementing guideline recommendations. We did not ask clinicians to specify their profession or years of experience as they made comments and so cannot identify this, though we have presented data about profession and years of experience in youth mental health over all. No doubt these factors have an impact on their knowledge of and attitudes to guideline recommendations.
Attitudes reported in this study may not be reflective of behaviour, and therefore an audit is currently underway to assess compliance with guideline recommendations. It is interesting to speculate that on the basis of our findings regarding attitudes to guidelines that practice may be broadly in line with guideline recommendations but that significant improvements may be necessary in some areas.
Strengths and weaknesses in relation to other studies, discussing important differences in results
There are few studies that specifically explore barriers to implementing guideline recommendations for the treatment of youth depression. One study conducted in the UK to explore psychiatrists attitudes to evidence-based guidelines indicated positive attitudes to guidelines; however, the barriers and enablers to using guideline recommendations were not examined [34]. A study in the USA surveyed medical directors about their use of practice system tools, showing these were facilitators of evidence-based practice; however, again it did not explore other factors that influence the uptake of evidence into practice [35]. In a study similar to this, child and adolescent mental health professionals in the USA participated in focus groups exploring barriers to evidence-based practice for youth mental health generally. While only 51% of clinicians participated (N = 19), the consistency of findings with the current study is striking, including barriers related to concerns about the applicability of evidence to the population being treated, a desire for greater emphasis on the therapeutic relationship, and the need for flexibility in implementing recommendations [36].
Implications
There are several potential responses to the current findings. First, services could develop resources for clinicians that clearly communicate the key guideline recommendations, but include considerations for individualizing recommendations relevant to the client population and system configuration [37]. Evidence shows that guidelines that take into account local circumstances [38,39] and are simple and easy to use [40] are more likely to be followed. Local services may also invest further effort towards addressing patient preference and related engagement of young people in evidence-based treatments. Considering patient preference from the outset is one way to encourage adherence to a treatment decision [41]. Finally, given the risk of treatment emergent suicidality, and research that indicates that spontaneous report of side effects does not sufficiently identify all those at risk of suicide [42], services should invest in systems that allow regular collection of standardized information about adverse effects, which may include clients having a role in self-monitoring.
The implications of our findings also point to the need for service reform where the system of care does not easily facilitate a stepped or sequenced model of care as advocated in the guidelines. Most mental health services are configured to treat those with the most severe mental health problems (approximately 3% of population) [43,44]. Additionally, mental health services predominantly remain configured to provide care for young people only up to the age of 18. Young people in early adulthood [18–25] find it difficult to access appropriate mental health care. There is a need to invest in collaborative care models that ensure integration between existing primary and secondary care and enhanced specialist early intervention mental health services for young people across the age spectrum up to the age of 25 [45]. This requires greater government investment in service reforms that ensure accessible and responsive clinical service systems for youth.
Future research
Guidelines are based on evidence from trials that typically exclude participants with comorbid conditions and suicide risk [16]. There is a clear imperative to develop the evidence base to ensure that effective treatments for young people with severe and complex disorders that include comorbid conditions, suicide risk and psychosocial difficulties, are investigated and disseminated.
Acknowledgement
The authors would like to thank all the clinicians from the service who participated.