
Abstract
Keywords
It is increasingly recognised that major public health issues related to behaviour and lifestyle, such as depression, violence, unemployment, unintended pregnancy and substance abuse have their origins in infancy and early childhood. Neuro-developmental science has made dramatic advances in assisting us to understand how early influences impact on brain development and resiliency to poor outcomes [1].
The initial postpartum months are especially significant for parents in developing a nurturing and responsive relationship with their infant. There is extensive evidence to show that the health and wellbeing of mothers and infants is adversely affected where a parent has mental illness [2]. Much of this work has been focused on postnatal depression, which has been estimated to affect 13–20% of women in studies carried out in industrialised nations [3]. Psychosocial risk factors that have been implicated include history of mental illness, lack of social support, recent life stresses, personality variables and feelings about pregnancy or parenthood [2,4].
Social and physical environmental adversity and measures of social capital have been found to be associated with maternal stress and pregnancy and infant health outcomes including prematurity, low-birth weight and infant mortality [5,6]. The detrimental and protective impact of these societal-level influences on postnatal depression is less well studied, with much of the emphasis to date being on individual-level psychosocial factors. Studies of these group-level influences will require the use of ecological, spatial, and multi-level study designs. The study reported here was used to inform the development of a mixed-method multi-level theory-building study.
The objective of this study was to determine the postnatal prevalence of maternal depressive symptomatology in South West Sydney, and to analyse the association with a range of potential socioeconomic, maternal and psychosocial risk factors.
Material and methods
The sample
The study population consisted of mothers of infants born in South West Sydney from January 2000 to June 2004 who received a first visit from a child and family nurse within 3 months of birth. A clinical assessment and questionnaire was completed for 29 405 mothers at their first home or clinic visit. Of those approached, 25 455 women completed an Edinburgh Postnatal Depression Scale (EPDS). Linked obstetric data was available for a subgroup of 6900 women from four local government areas.
Data source
The data for this study were drawn from two sources within the Mother and Infant Network (MINET) data system. These are the Obstetrics Package (OBSTET) and the Ingleburn Baby Information System (IBIS) database. The MINET was established in South West Sydney in November 1995 and has been reported in several previous publications [7–9]. The OBSTET data was used to assess associations with maternal age and parity. The IBIS database contains data collected by Child and Family Health Nurses for mothers of newborn infants at their first home or clinic visit after hospital discharge. This information is completed on a clinical record form and scanned into a Windows© based PC program. The 45 IBIS items are both clinical (e.g. weight) and parental self-report in nature including the EPDS.
The independent variables included in the reported study were: mother's country of birth (Australia or other), Aboriginal or Torres Strait Islander culture, age of mother, marital status, household size, blended family, number of children under five, accommodation (privately owned or not), financial situation (‘Would you say your financial situation is: very difficult – very good’, 10-point scale), car access, phone access, mother's rating of her health (five-point scale), mother's rating of her child's health (five-point scale), breastfeeding (which included both exclusive and partial breastfeeding), smoking, planned pregnancy, previous miscarriage, previous child death, previous stillbirth, previous child disability, previous termination of pregnancy, previous sudden infant death, suburb duration, regret about leaving the suburb (‘If for some reason you had to leave this suburb would you be sorry to go?’).
Outcome measure: Edinburgh Postnatal Depression Scale
The EPDS [10] is a brief 10-item self-report scale which is reliable, well validated and widely used internationally. It is widely accepted for use by child and family nurses and others (including GPs) in primary care settings. Validation studies have demonstrated 68–86% sensitivity and 78–96% specificity, and in an Australian sample 100% sensitivity and 89% specificity. Positive predictive value has been reported between 70–90%. The EPDS has been validated for a number of other languages and ethnic groups [11]. South Western Sydney studies have found that Vietnamese and Arabic translations of EPDS were acceptable to the women and appear to be suitable screening instruments for distress and depression [12]. For community screening purposes, Cox recommended a cut-off point greater than 9 [13]. Buist and others [14] maintain that using EPDS >12 reduces the chances of a false-positive diagnosis of likely depression. This study reports on screening cut-offs of both EPDS >9 and EPDS >12.
Statistical analysis
The data was analysed with the population group stratified by socio-demographic factors and other maternal characteristics. Associations of the various ‘risk factors’ with EPDS were initially evaluated by t-test and Chi square tests. Univariate and multivariate logistic regression was subsequently used to model both EPDS >9 and EPDS >12 in relation to the identified significant ‘risk factors’. Univariate and multivariate results of the logistic regression are reported. All data management and analysis used SPSS version 11.5.
Results
The socio-demographic factors and maternal characteristics of the 25 455 mothers and their infants are outlined in Table 1. Of the 6900 women for whom maternal age data was available (by linkage to obstetric data) 92% were aged between 20–39 years of age, 6% were less than 20 years of age and 2% 40 years of age or greater.
Characteristics of subjects: 25 455 cases
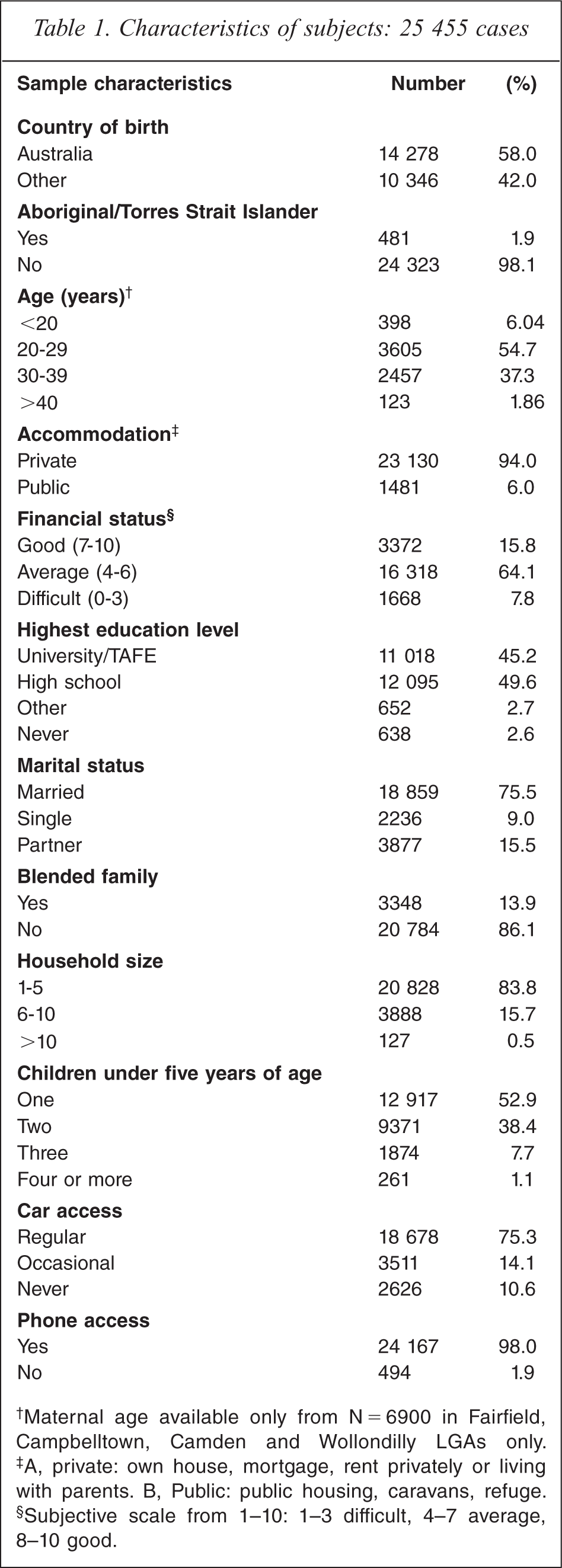
Maternal age available only from N 5 6900 in Fairfield, Campbelltown, Camden and Wollondilly LGAs only.
A, private: own house, mortgage, rent privately or living with parents. B, Public: public housing, caravans, refuge.
Subjective scale from 1–10: 1–3 difficult, 4–7 average, 8–10 good.
The mean EPDS score was 5.40 (95% CI 5.34–5.45) and the mean age of infant at the time of administration of the EPDS was 2.16 weeks. At the first visit, 12.2% of mothers had an EPDS score >9 and 6.8% had an EPDS score >12.
Predictors for EPDS >9
When the factors were considered individually in the logistic regression model (Table 2), those significantly associated with EDS >9 at time of the first visit were Other country of birth (OR 1.73, 95%CI: 1.6–1.9), Public accommodation (OR 1.3, 95%CI: 1.2–1.5), Difficult financial situation (OR 3.5, 95%CI: 3.0–4.1), Single/married status (OR 1.5, 95%CI 1.3–1.7), No car access (OR 1.7, 95%CI 1.5–1.9), One year or less suburb duration (OR 1.4 95%CI: 1.3–1.5), No regret leaving the suburb (OR 1.8, 95%CI: 1.6–2.1), Unplanned pregnancy (OR 1.3, 95%CI: 1.2–1.4), Not breastfeeding (OR 1.2, 95%CI: 1.1–1.3), Poor rating of own health (OR 13.0, 95%CI: 8.2–20.8), and Poor rating of child's health (OR 4.4, 95%CI: 1.6–12.4).
Factors associated with Edinburgh Depression Scale >9
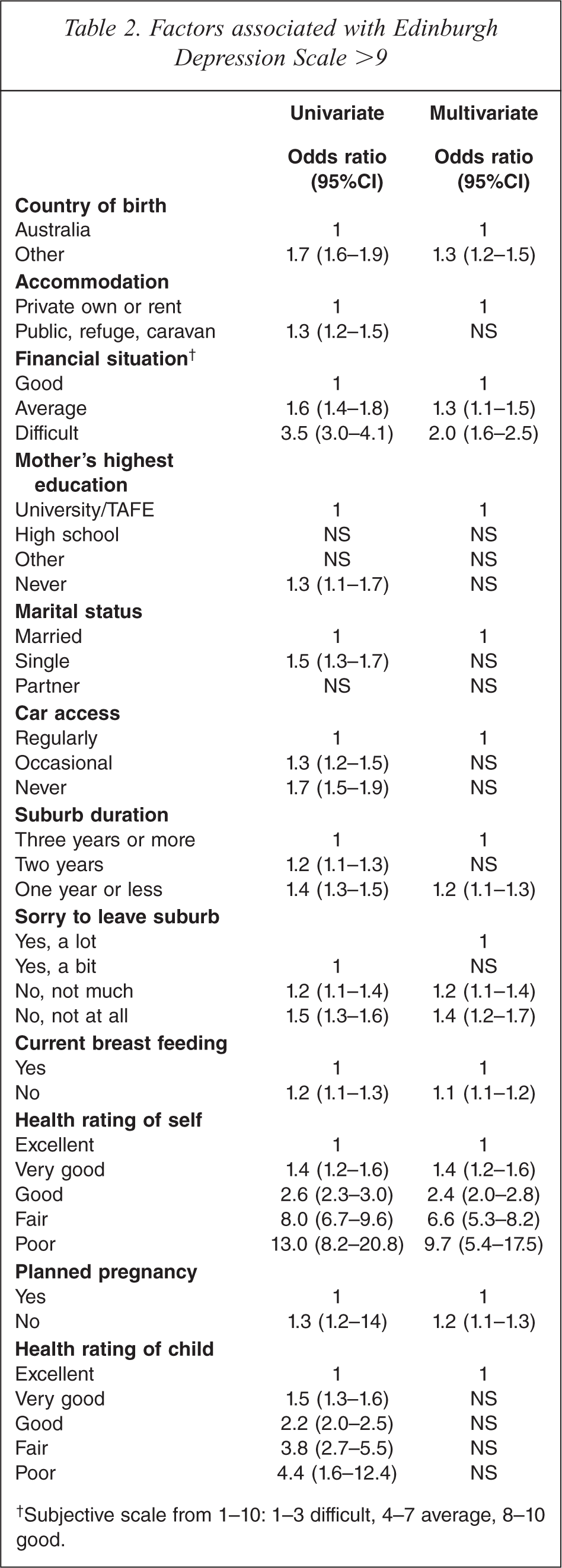
Subjective scale from 1–10: 1–3 difficult, 4–7 average, 8–10 good.
When factors were analysed in a multivariate logistic regression model (Table 2), the factors that were independently associated with EDS >10 at first visit were Other country of birth (OR 1.5, 95%CI: 1.4–1.7), Difficult financial situation (OR 2.2, 95%CI: 1.8–2.7), One year suburb duration (OR 1.2, 95%CI: 1.1–1.3), No regret leaving the suburb (OR 1.4, 95%CI: 1.2–1.7), Unplanned pregnancy (OR 1.2, 95%CI: 1.1–1.3), Not breastfeeding (OR1.1, 95%CI: 1.02–1.2) and Poor rating of own health (OR 9.7, 95%CI: 5.4–17.5).
In the logistic regression models the following were not significant associated with EDS >9: Aboriginal or Torres Strait Islander, Maternal age, Blended family, Household size, Number of children under five, Phone access, Previous miscarriage, Previous child disability, Previous termination, Previous SIDS, Previous death of child, Previous still birth, and Current smoker.
Predictors for EPDS >12
When the factors were considered individually in the logistic regression mode (Table 3), those significantly associated with EDS >12 at time of the first visit were Other country of birth (OR 1.9, 95%CI: 1.7–2.1), Public accommodation (OR 1.6, 95%CI: 1.3–1.9), Difficult financial situation (OR 4.5, 95%CI: 3.6–5.6), Single married status (OR 1.7, 95%CI 1.5–2.0), No car access (OR 1.9, 95%CI 1.7–2.3), No phone access (OR 1.9, 95%CI: 1.4–2.5), One year or less suburb duration (OR 1.4, 95%CI: 1.3–1.5), No regret leaving the suburb (OR 2.2, 95%CI: 1.8–2.6), Unplanned pregnancy (OR 1.5, 95%CI: 1.3–1.6), Not breastfeeding (OR 1.3, 95%CI: 1.2–1.4), Poor rating of own health (OR 16.2, 95%CI: 9.9–26.5), and Poor rating of child's health (OR 6.3, 95%CI: 2.1–19.4).
Factors associated with Edinburgh Depression Scale >12
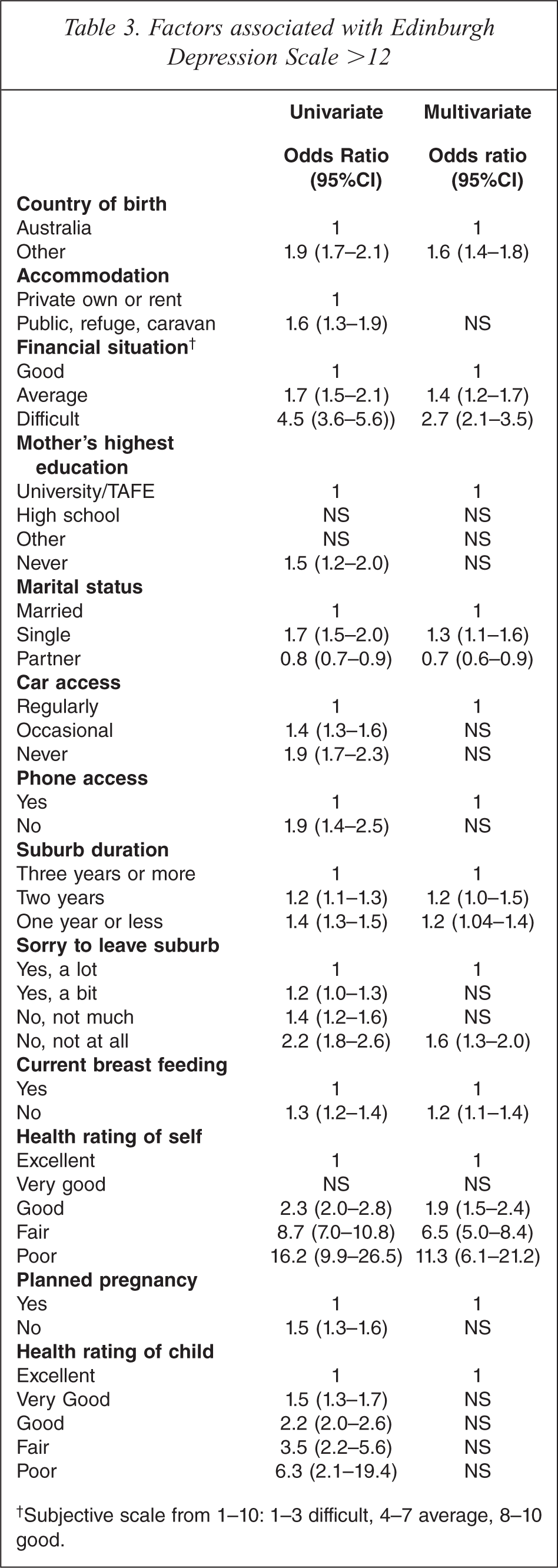
Subjective scale from 1–10: 1–3 difficult, 4–7 average, 8–10 good.
When factors were analysed in a multivariate logistic regression model (Table 3), the factors that were independently associated with EDS >12 at first visit were Other country of birth (OR 1.6, 95%CI: 1.4–1.8), Difficult financial situation (OR 2.7, 95%CI: 2.1–3.5), Partner/married status (OR 0.7, 95%CI: 0.6–0.9), No regret leaving the suburb (OR 1.6, 95%CI: 1.3–2.0), Not breastfeeding (OR 1.2, 95%CI: 1.1–1.4), and Poor rating of own health (OR 11.3, 95%CI: 6.1–21.2).
In the logistic regression models the following were not significantly associated with EDS >12: Aboriginal or Torres Strait Islander, Maternal age, Accommodation, Blended family, Household size, Number of children under five, Phone access, Previous child disability, Previous termination, Previous SIDS, Previous death of child, Previous still birth, and Current smoker.
Discussion
The size (25 455) of this population study of the women 2 weeks postnatally, who completed the EPDS, is significant. A recent Australian national study reported on 12 361 postnatal women who completed a postnatal EPDS [15]. Ferguson et al. [16] approached 14 893 women and interviewed 9316. Other large studies have included samples less than 3000 women [17]. The prevalence of EPDS score greater than 9 (12.2%) and greater than 12 (6.8%) is similar to that found in other studies [18], including the New South Wales study by Johnstone and others [19] in which the EPDS was administered at 8 weeks post partum. The mean infant age at screening of 2.16 weeks is younger than most other studies and consequently the findings may not be comparable.
The strong association of depressive symptoms with the mother being born in a country other than Australia is consistent with previous Australian studies. Williams and Carmichael [20] found in a Melbourne study that 35% of multi-ethnic, low socioeconomic status mothers with infants had significant depression. This was greatest among recent immigrants. The finding has important implication for the delivery of maternal and child health services in South Western Sydney where a high proportion of migrants and refugees settle. The ethnic diversity in South West Sydney is not uniform, with some migrant groups settling predominantly in certain suburbs and local government areas. The degree of ethnic diversity in a community may moderate the association of country of birth with depressive symptoms. For example, communities with more homogenous ethnic mix might have lower rates of depressive symptoms if common culture and language affords a protective benefit.
Our finding of an association of perceived financial difficulties with postnatal depressive symptoms has also been found in previous studies. O'Hara and Swain [18] found in their meta-analysis of 59 studies that of the socio-demographic factors analysed, only income was significant. Our findings are also consistent with the New South Wales study by Johnstone and others [19], who found that receiving a pension/benefit was independently associated with postpartum depression. There is marked variation in the distribution of financial hardship in South West Sydney with the region having some of the poorest suburbs in Australia. There are physical and social-environmental features of those poor suburbs, such as housing condition, traffic congestion and crime that may be important correlates of depressive symptoms. Similarly, there may be features of more affluent communities that confer protection. Given that postnatal depression is implicated as a negative determinant of child psychosocial development [21,22], the findings here would be consistent with a theoretical model where poverty and related stress impact on child (and family) psychosocial development in the early weeks of an infant's life.
The association between the length of time that a mother had lived in a suburb and depressive symptoms was strongest for those mothers who had lived in the suburb one year or less. The short time spent in a suburb will impact on the social support systems available to women. Cutrona and Troutman [23] argued that the availability of social support may mitigate against the development or the severity of postpartum depression. The question about regret at leaving the suburb is used in the NSW Health Survey as one measure of social capital and was the only such question included in the routine postnatal IBIS health assessment. The finding that women who had no regret at leaving the suburb were more likely to have depressive symptoms also supports the importance of local social support systems. There may, however, be other interpretations. Maternal responses to the question may have been influenced by their physical or mental health. It is possible that a depressed maternal mood may have resulted in mothers being more likely to report a negative assessment of their ‘connectedness’ to the local suburb. Alternatively, the finding may indicate that maternal depressive symptoms are associated with the group-level constructs of social cohesion and social capital. These two suburb-related findings suggest that there are important neighbourhood factors that are associated with maternal perinatal distress and depressive symptoms. As discussed above it is also possible that group-level factors mediate the findings of country of birth and financial hardship. There is extensive research on the association of neighbourhood factors with low birth weight, and child health and development outcomes. A recent large Swedish study found an association between neighbourhood socioeconomic environment and postnatal psychosis [24].
The study used a secondary data source, with the variables available for study limited to those included in the IBIS questionnaire. Consequently we are unable to report on important variables that might have been included if the survey had been specifically designed for the study of postnatal depression. Significantly, there was limited information on personality traits, psychopathological factors, life events and lifestyle behaviours. Selection bias may have occurred from refusal and non-response in the study population and depressed women may be less inclined to consent to participate. The EPDS response rate of 87% at the first visit is high, and sufficient for the purposes of this study. Recall, interviewer or responder biases may have been present in the survey data. A particular problem of self-reporting surveys is that they are influenced by the mental status of the subject. Depressed women are more likely to have a negative view of their circumstances. This must be taken into account when considering the association found in this study of high EPDS with subjective variables such as ‘No reluctance to leave the suburb’, and ‘Difficult financial situation’.
The study has important public health policy implications. It confirms the importance of poverty (‘difficult financial circumstances’) as an independent risk factor for depressive symptoms. The finding of an association with country of birth and several suburb-related variables raises questions about the mechanism by which ethnic diversity and ‘place’ impact on postpartum maternal, infant and family health. The proposition that financial stress is independently implicated as a determinant of maternal depression is consistent with previous studies [18,19], and has implication for macro public policy and intervention-related service delivery.
The case for universal routine screening for perinatal depression and associated psychosocial risk factors in Australia has recently been argued [4,14]. These studies have identified a number of socio-demographic risk factors that may assist in identifying women who are currently distressed, depressed or ‘at risk’. Current psychosocial screening methods could be modified to include women who are born in another country, new to their current suburb, not reluctant to leave their current suburb, or who have difficult financial circumstances. Intervention strategies need to be considered for all childbearing women in need and particularly for these specific subgroups.
Antenatal psychosocial assessment and EPDS screening has been recently implemented in many of the hospitals in South Western Sydney. Record linkage difficulties encountered in this study have been remedied and will in future allow analysis of both antenatal and postnatal screening data on large cohorts of pregnant women. This will enable longitudinal analysis of depression to determine the incidence of new cases in the perinatal period. It will also enable future studies to analyse antenatal psychological risk factors on large population cohorts.
The findings from this study would be consistent with a theoretical model that proposed group-level socioeconomic deprivation, neighbourhood environment, social capital and ethnic diversity as having contextual effects on postnatal depressive symptomatology and other perinatal outcomes. These and other neighbourhood and community group-level factors may be important and should be studied further.
Acknowledgements
The authors would like to acknowledge the contribution of all the child and family nurses of the former South West Sydney Area Health Service, and the staff of the Simpson Centre, for their efforts in the collection and maintenance of the IBIS database.