
Abstract
Comorbidity between chronic physical conditions and mental disorders has emerged as a major clinical and public health issue over the past few decades. The increased attention on this issue is largely due to population surveys that have highlighted that this comorbidity is common and can lead to significant disability. This paper presents the first nationally representative Australian data on the prevalence and correlates of comorbidity between chronic physical conditions (diabetes, asthma, coronary heart disease, stroke, cancer, arthritis) and the two most common mental disorders, affective and anxiety disorders.
Comorbidity between chronic physical conditions and affective and anxiety disorders has been reported in large epidemiological surveys across the world. Some of the largest studies examining comorbidity come from the US and include the National Comorbidity Survey (NCS) [1], its replication (NCS-R) [2] and the National Epidemiological Survey on Alcohol and Related Conditions (NESARC) [3,4]. Studies using similar measures have also been conducted in other countries including Canada [5], the Netherlands [6], Germany [7], the UK [8]; New Zealand [9,10] and Australia [11,12]. The epidemiological literature on comorbidity has been consistent in finding high rates of affective and anxiety disorders in those with chronic physical conditions [10]. A recent review by Clarke [13] found evidence of a strong association between chronic physical conditions and affective and anxiety disorders, and their effects on outcome.
Yet there are no national Australian data examining the relationship between the major chronic physical conditions and affective and anxiety disorders. Such descriptive epidemiology is critical for providing an evidence base for the treatment and prevention response to these problems and to inform our hypotheses on biological and psychosocial causes of comorbidity. It is crucial that such epidemiological information be as up to date and accurate as possible.
This paper examines 12-month comorbidity using data from the 2007 NSMHWB. Twelve-month comorbidity is the focus of this paper as it reflects most strongly the impact of comorbidity on individuals and treatment systems. Twelve-month comorbidity has been associated with greater disability, higher service use and poorer treatment response compared to a single disorder alone [14]. Even so, the treatment provided to those with comorbidity is often inadequate [14–16]. Up-to-date findings on the prevalence, patterns, severity and treatment response to comorbidity are required to guide an informed response.
This paper aims to:
describe the prevalence and patterns of 12-month comorbidity of affective or anxiety disorders and physical conditions in the Australian population;
examine the relationship between 12-month comorbid disorders and disability and treatment.
Method
Sample
The 2007 NSMHWB was commissioned by the Department of Health and Ageing and conducted by the Australian Bureau of Statistics (ABS). All interviews were carried out between August and December 2007. Respondents were selected at random from a stratified, multistage area probability sample of private dwellings. The population was individuals aged 16–85 years who were usual residents of private dwellings across Australia. Household information was provided by any householder aged over 17 years, and from all eligible respondents an algorithm randomly selected a householder to complete a personal interview. At this point the youngest (16–24 years) and oldest (65–85 years) age groups had a higher probability of being selected, in order to ensure sufficient sample size [17]. Sampling procedures generated an initial sample of 17 352 dwellings. Following loss of ineligible dwellings, due to all household members being out of scope or vacant dwellings, the effective sample size was 14 805. Of these, 8841 respondents completed the interview, representing a 60% response rate. The achieved sample of 8841 represents an estimated population count of 16 015 000 Australian adults.
Measures
Information required for the assessment of ICD-10 disorders was collected using a modified version of the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI 3.0). A full description of the measures can be found in Slade
Affective disorders: depression, dysthymia, bipolar affective disorder;
Anxiety disorders: agoraphobia, social phobia, panic disorder, generalized anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder
The chronic physical conditions discussed in this section were six chronic physical conditions recognized as national health priority areas (NHPA). These are diabetes, asthma, coronary heart disease (CHD), stroke, cancer and arthritis [17]. Respondents were asked if they have, or have received treatment for one of these chronic physical conditions in the last 12 months. Disability was assessed using a measure of ‘days out of role’ [18,19]. Respondents were asked how many days in the previous 30 they were totally unable to perform and days that they had to cut down on their normal activities as a result of health problems. For this paper, service use was assessed in the 12 months prior to the interview. Using previously published methods [20], twelve age-by-sex categories were defined and the number of visits required to place an individual in the top 15% (to the nearest whole number) was calculated from the frequency distributions of GP consultations for each of the 12 categories adjusted by SUDAAN [21]. For the purposes of this study, men aged 18–29 years were considered high service users if they attended more than four times in a year, while men and women aged more than 70 years were classified as high service users if they saw the GP more than 12 times in a year. Using this cut-off, the top 15% in each age-by-sex category account for approximately 50% of all GP consultations per annum [20].
Analysis
Weighted means, frequencies and cross-tabulations were computed. Adjusted odds ratios (ORs) derived from multiple logistic regressions indicated associations between physical and affective or anxiety disorders controlling for sociodemographic variables. Standard errors and 95% confidence intervals were estimated using Stata [22] which adjusts for characteristics of complex survey design [23,24]. In this data set, age was standardized in order to remove the effects of the different age structures of the different groups which could otherwise lead to misleading results.
Results
Prevalence of mental disorder–physical condition comorbidity
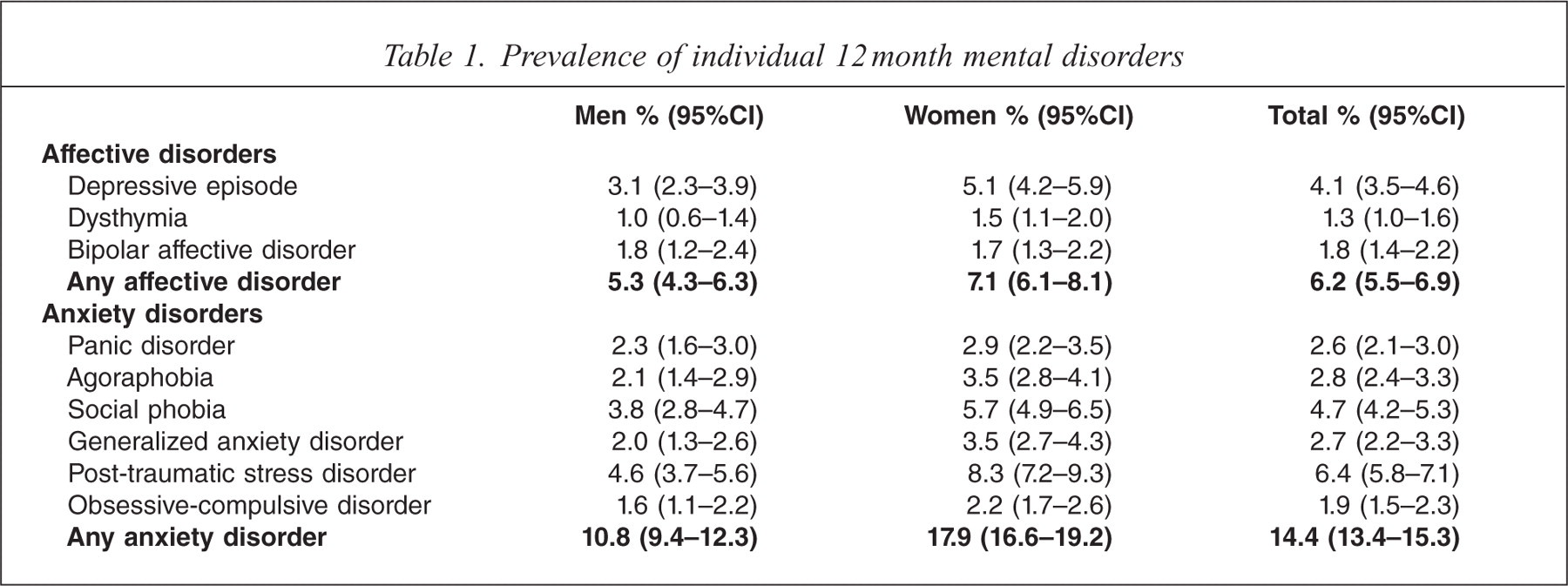
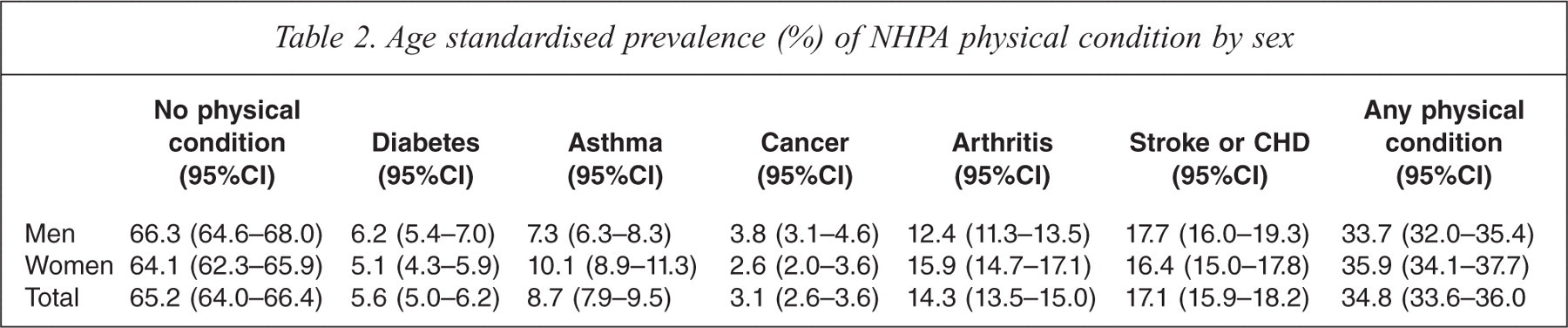
The prevalence rates for individual mental disorders assessed are presented in Table 1. The overall prevalence rate for anxiety disorders was 14.4% (95%CI = 13.4%–15.3%) and for affective disorders was 6.2% (95%CI = 5.5%–6.9%). Depressive disorders were the most common affective disorder with a prevalence of rate of 4.1% (95%CI = 3.5%–4.6%). Just over one third (34.8%, 95%CI = 33.6%–36.0%) of the sample reported having at least one chronic physical condition (diabetes, asthma, coronary heart disease, stroke, cancer, arthritis). The rate for males was 33.7% (95%CI = 32.0%–35.4%) and females were slightly higher at 35.9% (95%CI = 34.1%–37.7%). The rates for individual physical disorders are presented in Table 2.
Prevalence of individual 12 month mental disorders
Age standardised prevalence (%) of NHPA physical condition by sex
The prevalence of 12-month mental disorders in people with chronic physical conditions is presented in Table 3. Mental disorders were more common among people with chronic physical conditions than among people without chronic physical conditions (21.9%, 95%CI = 19.4%–24.4% compared to 13.5%, 95%CI = 12.4%–14.6%). Specifically, affective disorders were more common among people with physical conditions than among people without chronic physical conditions (affective OR 1.5; 95%CI = 1.1–1.9). Further, anxiety disorders were more common among people with physical conditions than among people without chronic physical conditions (anxiety OR 1.8; 95%CI = 1.4–2.4).
Age standardized prevalence of 12-month affective and anxiety disorders amongst those with chronic physical conditions
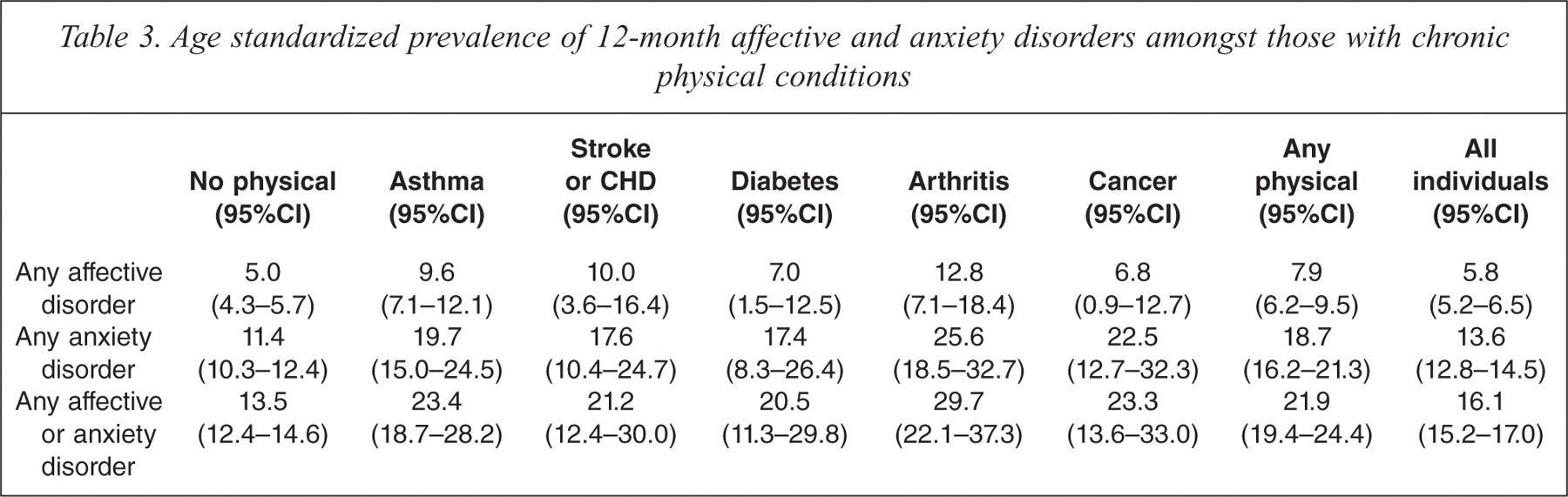
A higher proportion of women with a chronic physical condition had an affective or anxiety disorder compared to men (women 27.7%, 95%CI = 23.8%–31.7% compared to men 14.5%, 95%CI = 10.9%–18.1%).
The prevalence of affective or anxiety disorders in those with specific chronic physical conditions compared to those without specific chronic physical conditions differed for men and women, but there was no such sex difference in those without any chronic physical condition. Women with diabetes had a higher prevalence of affective and anxiety disorders than corresponding men, but there was no such sex difference in those without any chronic physical condition. The rates of affective and anxiety disorders were consistently elevated across all of the physical health conditions examined (Table 3).
The prevalence of 12-month chronic physical conditions in people with mental disorders is presented in Table 4. Of those with a 12-month anxiety or affective disorder 45.6% (95%CI = 41.9%–49.2%) had at least one chronic physical condition. For women, 48.1% (95%CI = 43.2%–53.0%) of those with a 12-month mental disorder had a physical condition compared to 33.1% (95%CI = 31.2%–35.1%) of women without a mental disorder. For men, 38.5% (95%CI = 30.8%–46.3%) of those with a mental disorder had a physical condition compared to 32.8% (95%CI = 30.9%–34.6%) of men without a mental disorder. Specifically, physical disorders were more common in those with an affective disorder than among people without an affective disorder (affective OR 1.6; 95%CI 1.2–2.0). Further, physical disorders were more common in those with an anxiety disorder than among people without an anxiety disorder (anxiety OR 2.0; 95%CI 1.5–2.5). The rates of asthma, stroke and arthritis were the most markedly elevated in individuals with affective and anxiety disorders.
Age standardized prevalence (%) of physical condition in people with affective or anxiety disorder
Association between physical-mental disorder comorbidity, disability and service use
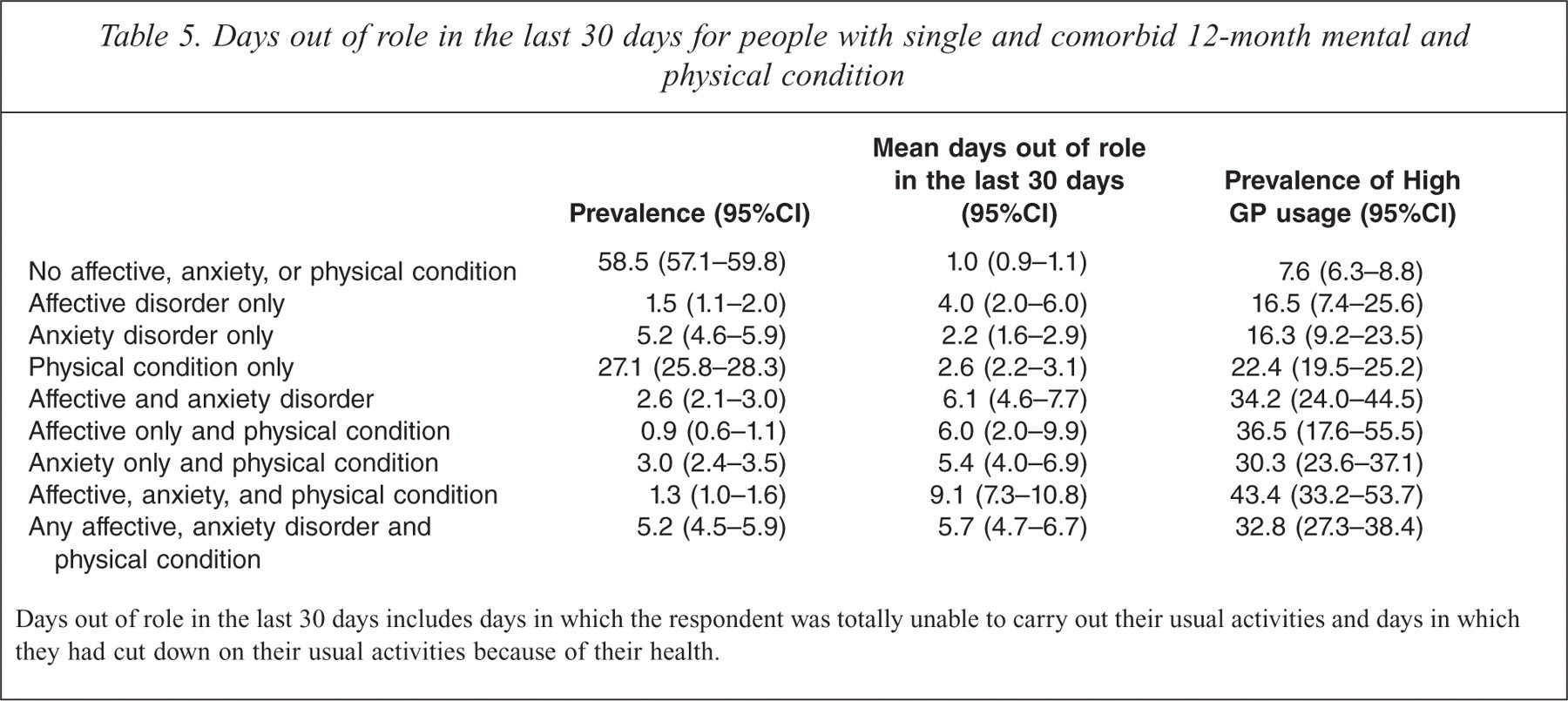
There was a clear association between physical-mental disorder comorbidity and days out of role in the last 30 days and high GP service use; this data is presented in Table 5. People without an affective or anxiety disorder or chronic physical condition had, on average, one day out of role in the past 30 days (95%CI = 1.3–1.6). People with an affective or anxiety disorder in the absence of chronic physical conditions had 6.1 (95%CI = 4.6–7.7) days out of role. People with chronic physical conditions in the absence of affective or anxiety disorders had 2.6 (95%CI = 2.2–3.1) days out of role and people with both an affective or anxiety disorder and a chronic physical condition had 5.7 (95%CI = 4.7–6.7) days out of role. The prevalence of high GP service usage was 7.6% (95%CI = 6.3–8.8) in those with no affective, anxiety or physical condition. In contrast, the prevalence of high GP service usage was 36.5% (95%CI = 17.6–55.5) in those with affective disorders and physical conditions, 30.3% (95%CI = 23.6–37.1) in those with anxiety disorders and physical conditions and 43.4% (95%CI = 33.2–53.7) in those with anxiety, affective and physical conditions.
Days out of role in the last 30 days for people with single and comorbid 12-month mental and physical condition
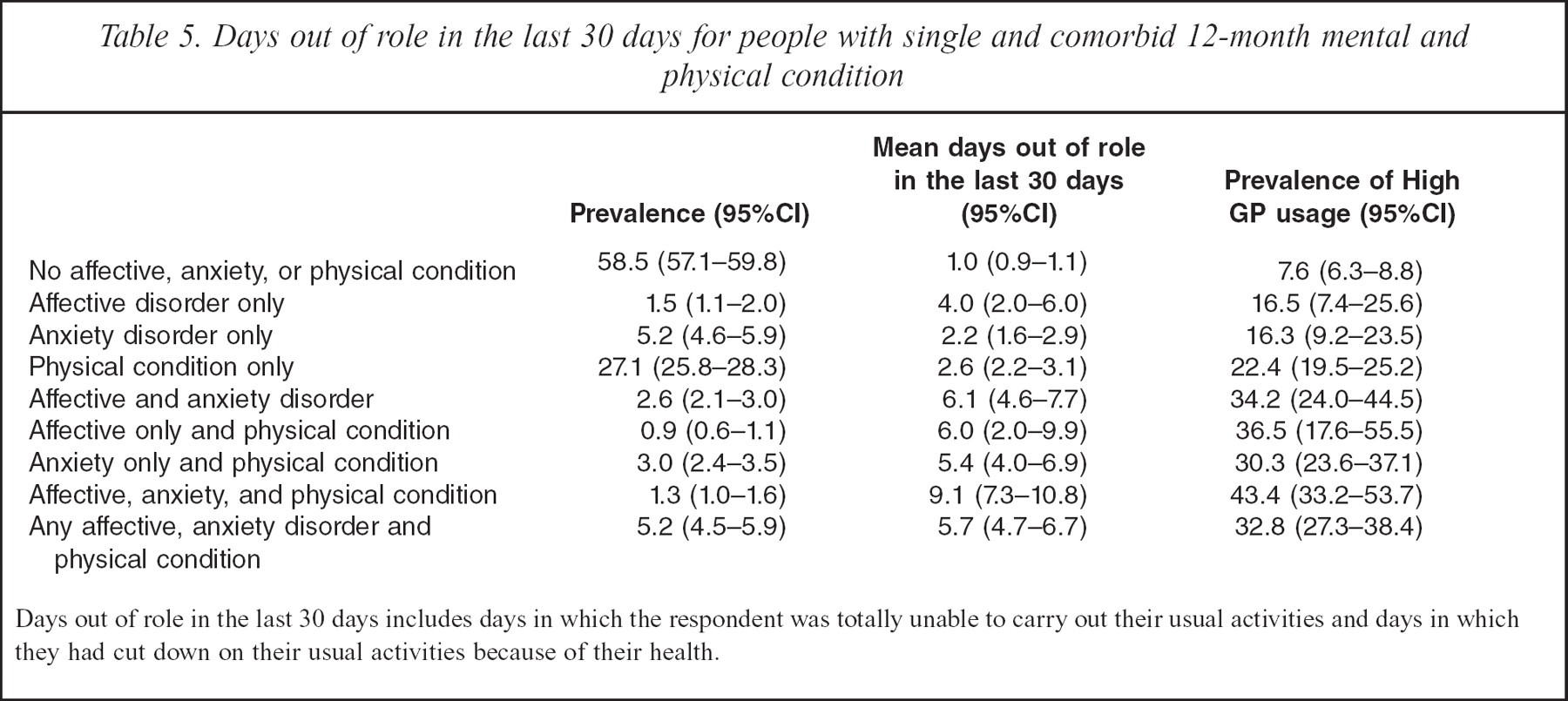
Days out of role in the last 30 days includes days in which the respondent was totally unable to carry out their usual activities and days in which they had cut down on their usual activities because of their health.
Discussion
The 12-month physical–mental disorder comorbidity patterns in the 2007 NSMHWB consistently show high rates of affective and anxiety disorders in those with chronic physical conditions. Such comorbidity was associated with increased disability, with some evidence that the effect was additive. Physical–mental disorder comorbidity was also associated with high GP service usage. Interestingly, the rates of affective and anxiety disorders were consistently elevated across all of the physical health conditions examined. In those with anxiety and affective disorders, asthma, stroke and arthritis were the most markedly elevated physical conditions. The results do not imply causality, but rather they indicate the significance of the population disease burden of individuals with both mental disorders and physical conditions. Indeed, the findings of this paper are consistent with reports showing that anxiety disorders and depressive disorders have independent relationships with a wide range of chronic physical conditions [25].
This paper clearly shows comorbidity is the rule rather than the exception. The first and most important implication of this study is the improved recognition of the impact of anxiety and affective disorders in those with physical conditions. This improved recognition needs to occur at three levels: individual, clinical and system, if we are to address the burden associated with this comorbidity.
There have been three core components of campaigns to improve individual and community responses to depression and to a lesser extent anxiety disorders: the availability of effective interventions, better coordination of care services, and public campaigns to de-stigmatize and educate the public about recognition and treatment [26]. These campaigns may be well extended into those with physical conditions.
In clinical practice the complex decisions around differential diagnosis will remain, especially in complex cases. It may be, however, that with improved identification simple effective first line interventions for mental disorders can begin early in those with physical disorders without stigmatizing the patient. This has the potential to alleviate the disease burden for the individual, as well as their carers [27]. To achieve this, however, is not just a clinical issue, our current health services are organized in silos relating to specialty, and require either more resources for the general practice gatekeepers to coordinate care, or a reconsideration of the silo organization. Indeed there is some evidence to suggest that bringing mental health services to general practice is an effective way to deal not only with mental disorders such as anxiety and depression but also with comorbidity [28–30]. Regardless, the complexity associated with comorbidity has not been mastered anywhere, let alone in primary care and remains an ongoing challenge.
The treatment response for comorbid physical, affective and anxiety disorders is also critical. While research in this area is growing, it remains in its infancy [13]. One area where attention has focused is the relationship between depression and heart disease [31,32]. Depression is a risk factor for developing heart disease and a predictor of worse outcome after cardiac events. There are a number of plausible pathways through behavioural, immune, haematological, and endocrine mechanisms [33], and these may well be present in stress- and anxiety-related disorders and may impact on other physical conditions. In terms of specific treatment responses to comorbid physical and mental disorders the evidence is growing. A recent Cochrane review into the treatment of depression in those with stoke found some evidence of the benefit of pharmacotherapy in terms of a complete remission of depression and a reduction in scores on depression rating scales, but there was also evidence of an associated increase in adverse events [34]. In the current study, rates of antidepressant use and anxiolytic, hypnotic or sedative medication use were 6.8% and 4.7% respectively in the total sample [30]. Having a chronic physical condition was positively associated with both antidepressant use and anxiolytic, hypnotic or sedative medication use. Amongst those with a chronic physical condition this rate was 9.9% and 7.3% respectively [30]. Still, to date, most depression and anxiety treatment guidelines do not address the issue of comorbidity with physical conditions. A recent exception to this has been the UK National Institute for Health and Clinical Excellence (NICE) guidelines on the management of depression in those with comorbid physical conditions [35]. Unfortunately, equivalent Australian guidelines have not been developed despite the high prevalence and high service use of these groups.
Physical disorders were also found to be more common in those with an affective or anxiety disorder than among people without an affective or anxiety disorder, with the relationship strongest in those with anxiety disorders. Recent longitudinal research on the relationship between depression, anxiety disorders and physical function has shown that anxiety disorders contribute the most in the relationship to lower levels of physical function when compared to depression [36], a finding mirrored in our cross sectional research. The longitudinal research also shows that those with the lowest physical function carry the greatest risk of onset of both depression and anxiety disorders [36]. While the current study is cross sectional, it does reinforce the high prevalence of physical disorders in those with anxiety and affective disorders and the potential for a focus on prevention of the development of affective and anxiety disorders in those with physical disorders. The prevention of lower levels of physical function among those with physical disorders may be a potential mechanism to help to prevent the onset of depression and anxiety disorders in this group. While Australian policy efforts have focused on mental disorder comorbidity, comorbidity with physical conditions also clearly warrants attention.
Limitations
The assessment of mental disorders in the context of physical conditions can be problematic – the diagnostic criteria for many mental disorders exclude symptoms that are attributable to physical conditions [37]. Major depressive disorder, for example, is characterized by fatigue and low levels of energy, a symptom that is common in chronic illness. In the present analysis we presented rates of mental disorders without these exclusionary criteria applied so we could assess comorbidity rates. A non-clinical population survey, however, will have limitations in its ability to disentangle symptoms of physical and mental disorders.
A further potential source of error in the current study is the 60% response rate. The impact of this lower than expected response rate was examined in a purposive sample of fully non-responding households in two metropolitan areas [17]. The study indicated that the impact of non-response was small at the aggregate level. Due to the small, non-random nature of the non-response follow up sample the results were not incorporated into the survey estimation strategy. In relation to the present study there may be some underestimation of the prevalence of affective and anxiety disorders for men and young people. This is limited, however, and these data remain the most comprehensive data available on the prevalence of mental disorders in the Australian general population.
Conclusions
Comorbidity between anxiety and affective disorders and physical conditions is a major health issue for Australia. A significant proportion of those with chronic physical conditions will have a mental disorder and the impact on disability is additive [25]. While comorbidity patterns are complex it is clear that we require a sustained effort to deliver the most effective prevention and treatment response to this important health issue.
Acknowledgements
The authors would like to thank the NSMHWB Reference Group for their input into the survey's design.