
Abstract
Keywords
Comorbidity refers to having more than one physical or mental disorder at the same time. In this paper we examine the comorbidity between the mental disorder classes (anxiety, affective and substance use disorders) and comorbidity between physical disorders and mental disorders. Comorbidity is common and complex and this presents a significant challenge with respect to the most appropriate identification, prevention and management strategies [1, 2].
The complexity of comorbidity has been a focus of large epidemiological surveys across the world. Some of the largest studies focusing on comorbidity come from the USA and include the National Comorbidity Survey (NCS) [3], its replication (NCS-R) [4], and the National Epidemiological Survey on Alcohol and Related Conditions (NESARC) [5, 6]. Studies using similar measures have also been conducted in other countries including Canada [7], the Netherlands [8], Germany [9], the UK [10]; New Zealand [11, 12] and also Australia (1997 National Survey of Mental Health and Wellbeing; 1997 NSMHWB) [13, 14].
The epidemiological literature on comorbidity has been highly consistent in a number of important findings [15]. First, comorbidity between anxiety, affective and substance use disorders is very common, with around one-quarter to half of persons with any mental disorder meeting criteria for another disorder at some point in their lives [1, 16]. Second, the highest rates of comorbidity are observed between anxiety and affective disorders [16, 17]. Third, there are high rates of comorbidity between substance use disorders, affective and anxiety disorders [2, 18–20]. Last, there are high rates of mental disorders in those with chronic physical conditions [11]. The findings are complex and the descriptive epidemiology of comorbidity is critical for providing an evidence base for the treatment and prevention response to this problem and to inform our hypotheses on biological and psychosocial causes of comorbidity. It is crucial that such epidemiological information be as up to date and accurate as possible [6]. For example, recent international surveys [4, 12, 21, 22] deviated from the substance use disorder diagnostic criteria and skipped substance use dependence criteria if respondents did not endorse lifetime harmful use/abuse criteria [6, 23–25]. The 2007 NSMHWB survey instrument was modified so that it more closely followed the diagnostic criteria
This paper examines 12 month comorbidity using data from the 2007 NSMHWB. Twelve month comorbidity is the focus of this paper because it reflects most strongly the impact of comorbidity on individuals and treatment systems [12]. Twelve month comorbidity has been associated with greater disability and poorer treatment response [2]. Treatment seeking is greater among those with comorbid anxiety, affective and substance use disorders [2], and those with comorbid physical and mental disorders experience significant disability [26]. Even so, only a minority of those with comorbid disorders receive treatment [2], and the treatment provided to those with comorbidity is often inadequate [1, 2]. Up-to-date findings on the prevalence, patterns, severity and treatment response to comorbidity are required to guide an informed response.
The aims of this paper are to (i) describe the prevalence and patterns of 12 month mental disorder comorbidity in the Australian population; (ii) examine the relationship between 12 month comorbid mental disorders, severity and health service utilization; (iii) describe the prevalence and patterns of 12 month physical–mental disorder comorbidity in the Australian population; and (iv) examine the relationship between 12 month comorbid physical–mental disorders and severity.
Method
Sample
Slade et al. have described the survey methods and presented the basic findings of the survey [27]. The 2007 NSMHWB sample was based on a stratified, multistage probability sample of persons aged 16–85 years living in private dwellings in Australia, excluding very remote areas. The overall response rate was 60% and there were 8841 fully responding participants.
Measures
Information required for the assessment of ICD-10 disorders were collected using a modified version of the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI 3.0). A full description of the measures can be found in Slade et al. [27]. In order to capture the true extent of comorbidity the ‘without hierarchy’ diagnoses are used in this paper. The diagnoses covered in the 2007 NSMHWB were categorized into three classes of mental disorder: (i) affective disorders: depression, dysthymia, bipolar affective disorder; (ii) anxiety disorders: agoraphobia, social phobia, panic disorder, generalized anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder; and (iii) substance use disorders: harmful use and dependence derived separately for alcohol, cannabis, sedatives, stimulants and opioids.
The chronic physical conditions discussed in this section were six chronic physical conditions recognized as National Health Priority Areas (NHPA). These are diabetes, asthma, coronary heart disease, stroke, cancer, and arthritis [27]. In addition to diagnostic information, all individuals with 12 month mental disorders were classified into one of three severity categories: mild, moderate, or severe. Severity was defined according to an adapted algorithm originally developed by the World Mental Health Survey Initiative team. Severity is attributed to an individual, not to a mental disorder, and reflects the total impact of all 12 month mental disorders experienced by that individual, thus taking into account comorbidity. Disability was further assessed using a measure of ‘days out of role’. Respondents were asked how many days in the previous 30 they were totally unable to perform, and days that they had to cut down on their normal activities as a result of health problems. For this paper, service use was defined as at least one consultation specifically for mental health problems with any health professional in the 12 months prior to the interview.
Analysis
Data were provided by the Australian Bureau of Statistics in the form of point prevalence and standard errors [27]. Prevalence estimates were derived using a complex estimation procedure to account for the stratified multistage survey design and to adjust for oversampling and non-response. Differences were considered statistically significant if the 95% confidence intervals (CIs) did not overlap [27]. This is a conservative test of statistically significant differences because it essentially requires two point estimates to be separated by four standard errors.
Results
Prevalence of mental disorder comorbidity
The proportion of the population with no disorder was 80% (95%CI = 79.0–81.1%), one disorder class was 14.9% (95%CI = 13.9–15.8%), two disorder classes was 4.4% (95%CI = 3.9–4.9%), and three disorder classes was 0.7% (95%CI = 0.5–0.9%). Overall, one in four people (25.4%) with a 12 month mental disorder were comorbid. Specifically, of those with at least one 12 month mental disorder, 74.6% (95%CI = 69.7–79.5%) met criteria for one disorder, 21.9% (95%CI = 19.3–24.5%) met criteria for two disorder classes and 3.5% (95%CI = 2.3–4.7%) met criteria for all three classes of mental disorder (anxiety, affective and substance use disorder).
Percentage with a comorbid 12 month mental disorder vs 12 month mental disorder class
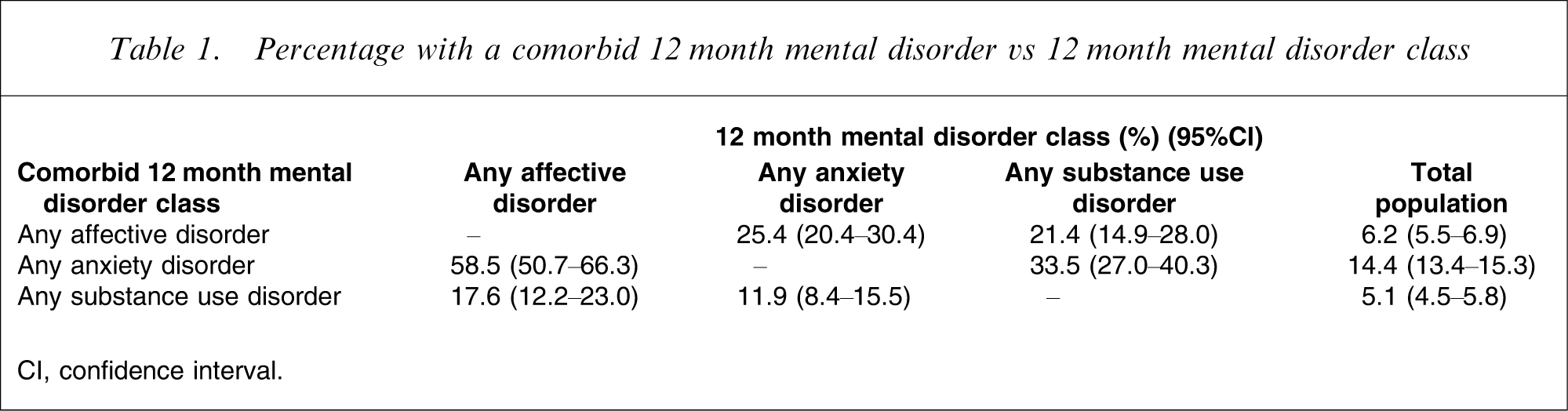
CI, confidence interval.
The patterns of comorbidity for women and men are shown in Figure 1. Affective and anxiety disorder comorbidity was the most common comorbidity for both sexes (female 3.9%, 95%CI = 3.2–4.6%; male 2.0%, 95%CI = 1.4–2.5%) although female subjects were more likely to experience this comorbidity than male. The next most common comorbidity for both sexes was a substance use disorder in combination with an anxiety disorder (female 0.8%, 95%CI = 0.4–1.1%; male 1.3%, 95%CI = 0.8–1.7%). The third most common comorbidity for both sexes was a substance use disorder in combination with an affective disorder (female 0.2%, 95%CI = 0.0–0.4%; male 0.6%, 95%CI = 0.2–1.0%). Female and male subjects were equally likely to have all three mental disorder classes (female 0.6%, 95%CI = 0.3–08%; male 0.8%, 95%CI = 0.4–1.3%).
(a) Prevalence (%) of single and comorbid affective, anxiety and substance use disorders among Australian male subjects in the previous 12 months. (b) Prevalence (%) of single and comorbid affective, anxiety and substance use disorders among Australian female subjects in the previous 12 months.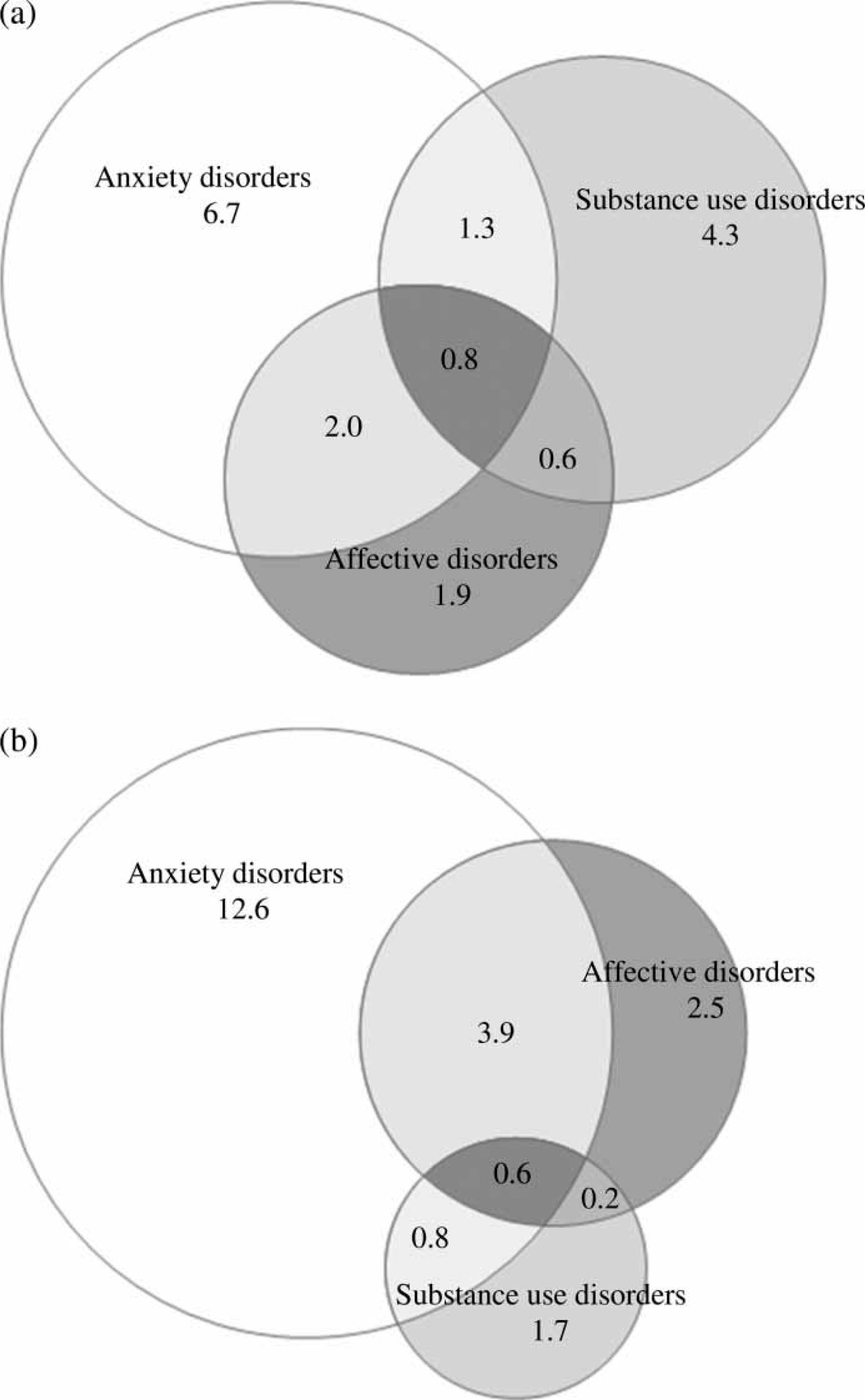
Association between mental disorder comorbidity and severity of impairment
Severity of 12 month comorbid mental disorders
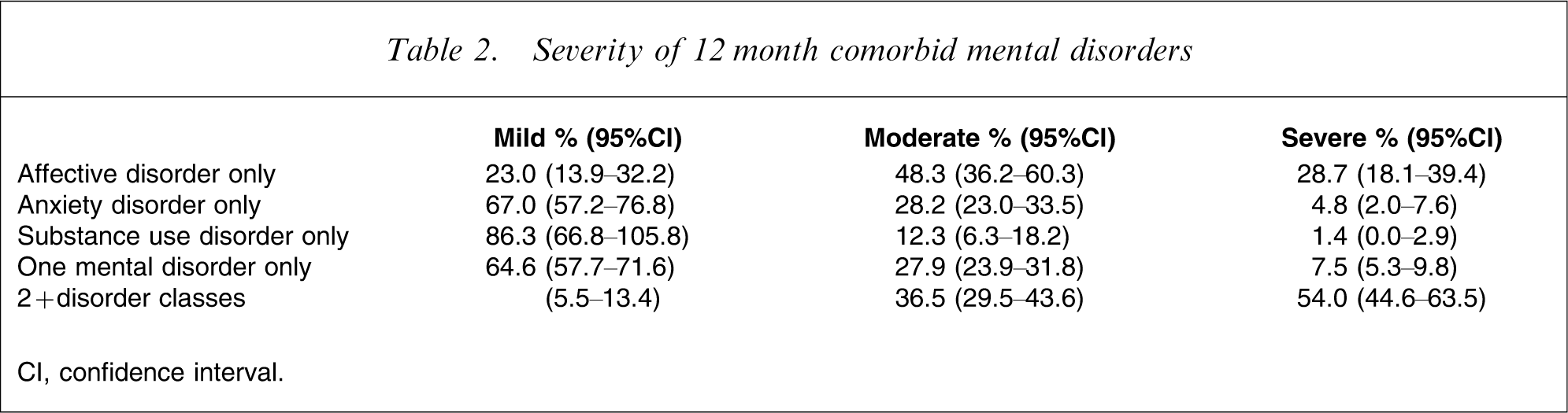
CI, confidence interval.
Association between mental disorder comorbidity and days out of role in last 30 days
Days out of role in the last 30 days for people with single and comorbid 12 month mental disorders
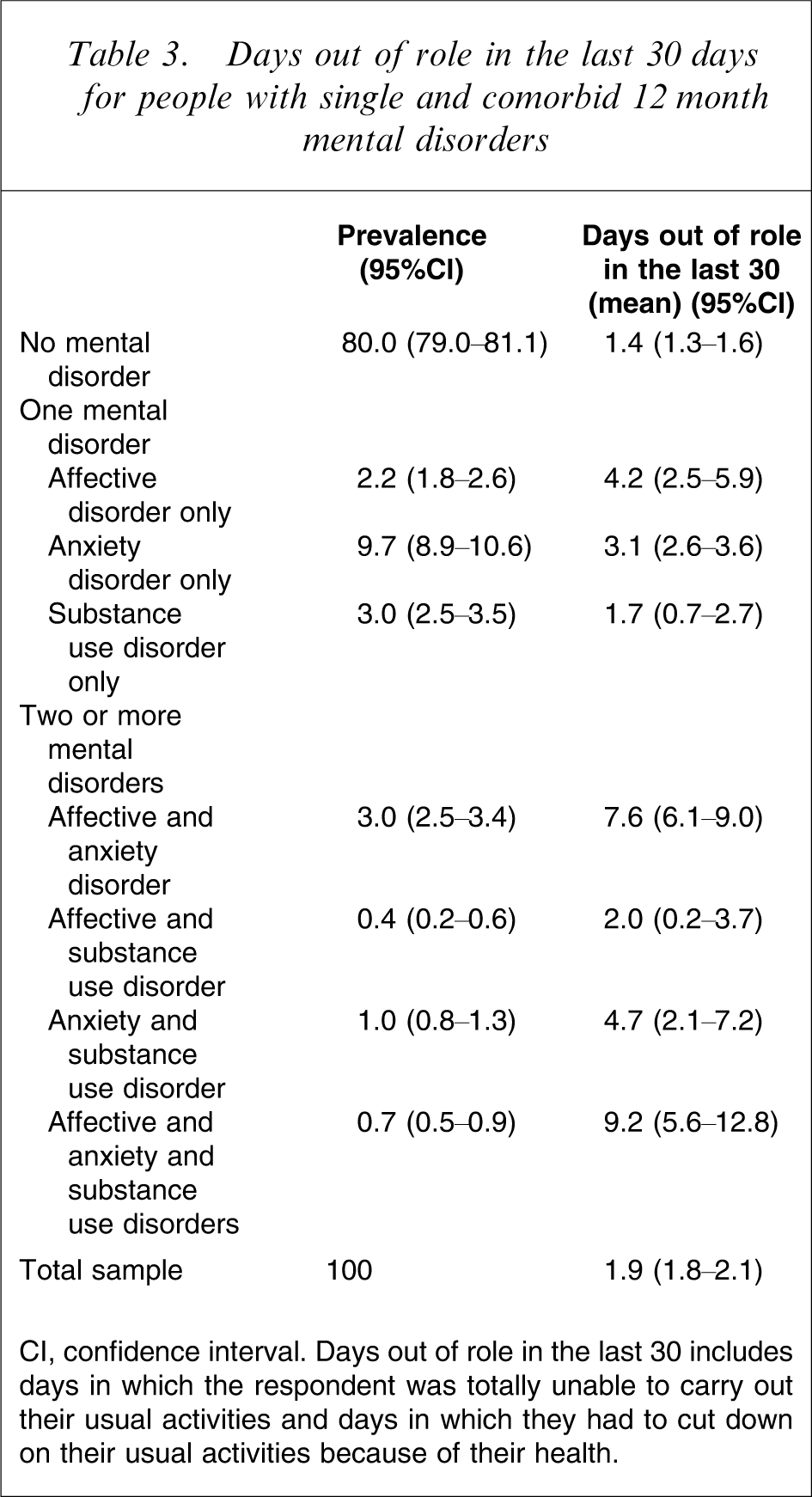
CI, confidence interval. Days out of role in the last 30 includes days in which the respondent was totally unable to carry out their usual activities and days in which they had to cut down on their usual activities because of their health.
Association between mental disorder comorbidity and service use
Two-thirds (65.4%, 95%CI = 33.4–97.5%) of people with mental disorders from all three classes in the 12 months prior to interview used services within that period. People with all three classes of mental disorder used more services (65.4%) than those with anxiety disorders only (27.3%, 95%CI = 22.1–32.4%), and substance use disorders only (11.8%, 95%CI = 5.8–17.7%). As demonstrated in Figure 2, however, service use was predominantly driven by people with affective disorders, either alone (48.8%, 95%CI = 36.6–61.0%) or in combination with other comorbid classes of mental disorder: affective and anxiety only (68.7%, 95%CI = 54.5–82.9%); affective and substance use disorder only (27.8%, 95%CI = 8.9–46.8%); anxiety and substance use disorder only (30.0%, 95%CI = 14.3–45.6%).
Percentage of the Australian population with single and comorbid mental disorder classes who used health services for mental health problems.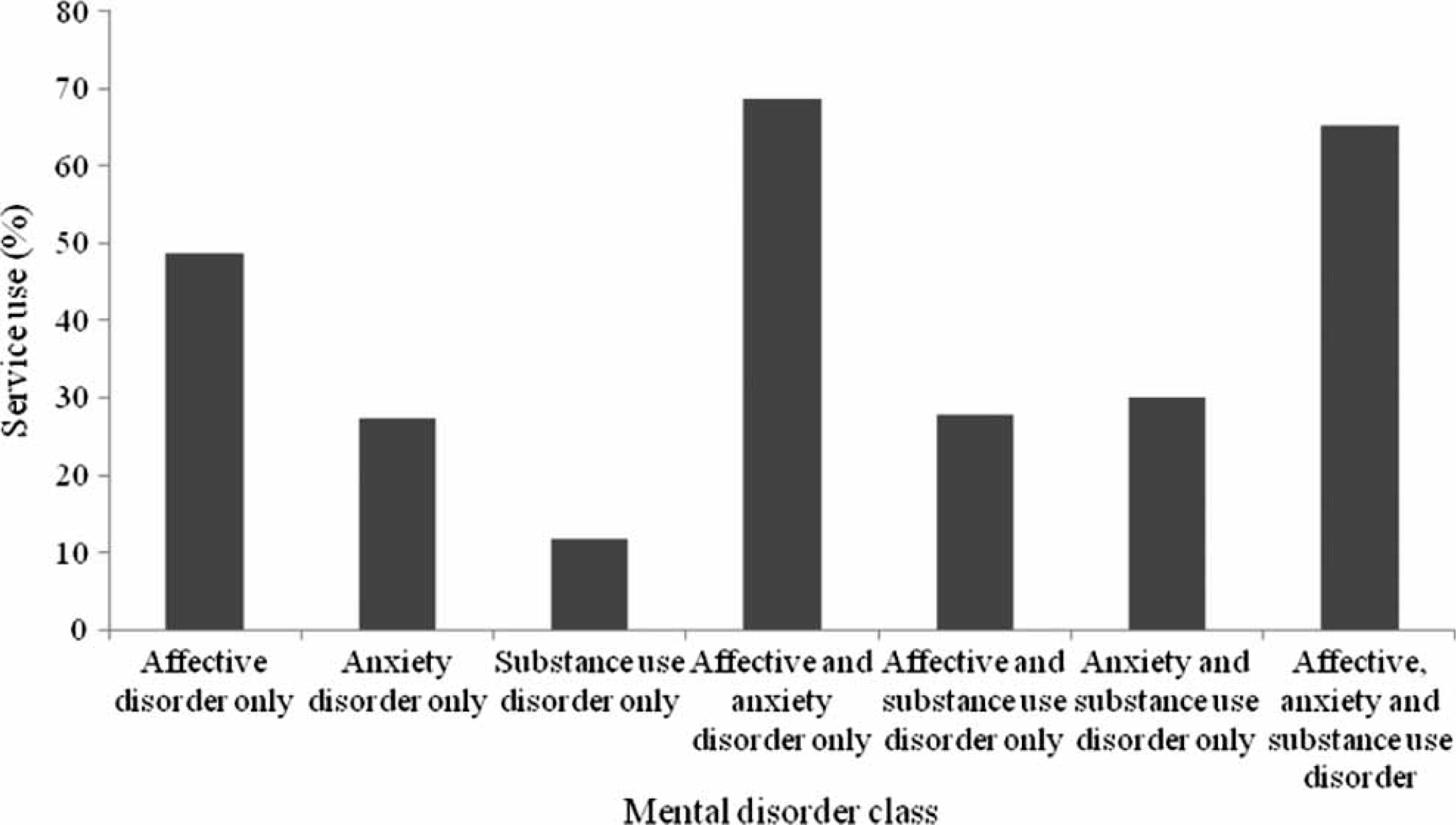
Prevalence of mental disorder–physical disorder comorbidity
Just less than one-third (32.2%, 95%CI = 30.9–33.4%) of the population reported having at least one NHPA chronic physical condition (diabetes, asthma, coronary heart disease, stroke, cancer, arthritis). The rate for male subject was 30% (95%CI = 28.2–31.9%) and female subjects were slightly higher at 34.3% (95%CI = 32.5–36.1%).
Of those with 12 month mental disorder 34% had at least one NHPA chronic physical condition. For female subjects, 38.3% of those with a 12 month mental disorder had a chronic physical condition compared to 33.2% of female subjects without a mental disorder. For men, 28.5% of those with a mental disorder had a chronic physical condition compared to 30.3% of men without a mental disorder.
Age-standardized prevalence of 12 month mental disorders among those with NHPA chronic physical conditions vs sex
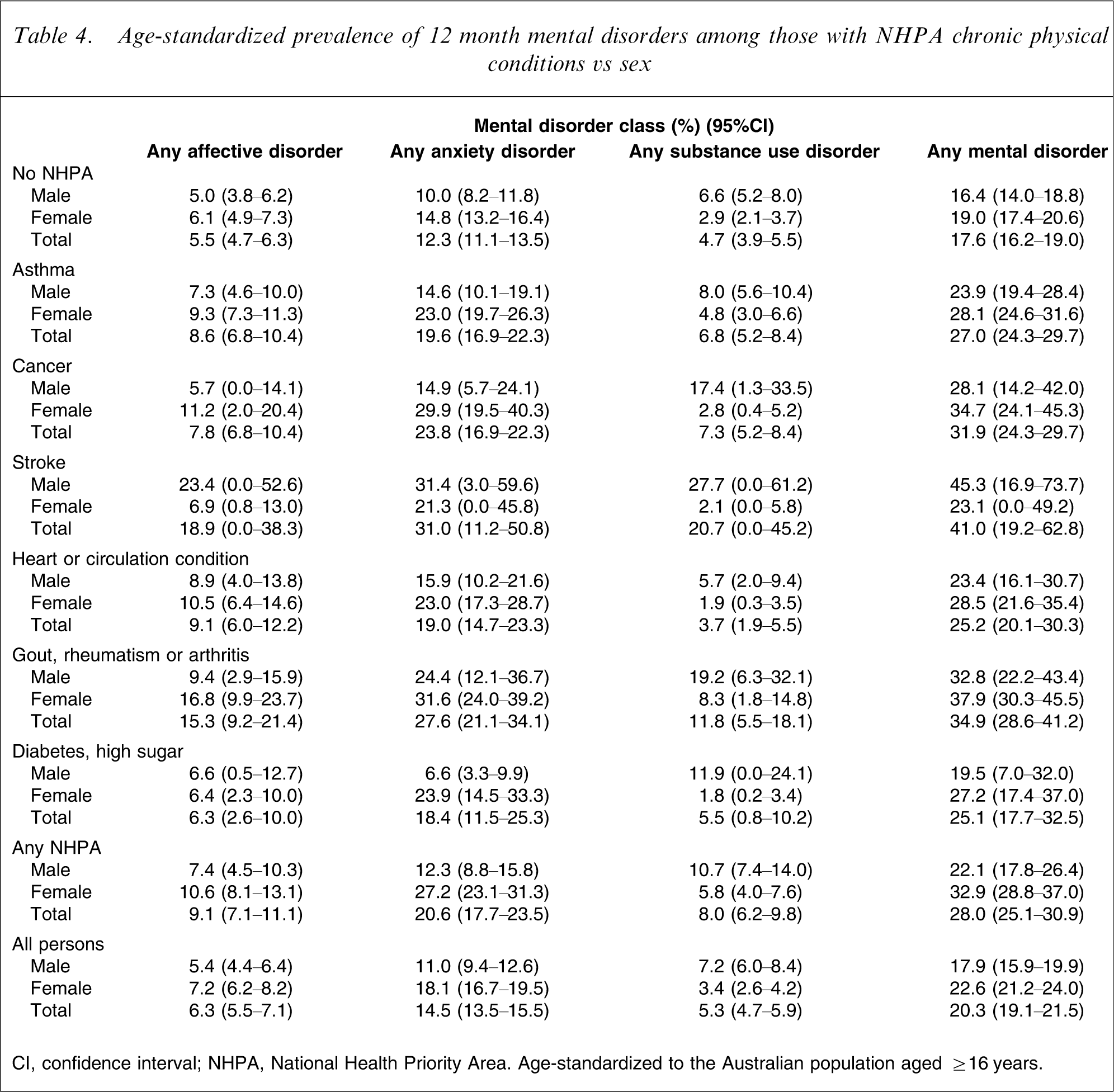
CI, confidence interval; NHPA, National Health Priority Area. Age-standardized to the Australian population aged ≥16 years.
The prevalence of mental disorders in those with specific chronic physical conditions compared to those without specific chronic physical conditions differed for male and female subjects. In particular, men with stroke had nearly twice the prevalence of any mental disorder as corresponding women, but there was no such sex difference in those without any chronic physical condition (Table 4). Female subjects with diabetes had a higher prevalence of any mental disorder than corresponding male subjects, but there was no such sex difference in those without any chronic physical condition.
Association between physical–mental disorder comorbidity and days out of role in the last 30 days
There was a clear association between physical–mental disorders comorbidity and days out of role in the last 30 days. People without a mental disorder or chronic physical condition had, on average, 1 day out role in the past 30 days (95%CI = 1.3–1.6). People with mental disorders in the absence of chronic physical conditions had 3.2 days (95%CI = 2.6–3.7) out of role. People with chronic physical conditions in the absence of mental disorders had 2.5 days (95%CI = 2.2–2.8) out of role and people with both a mental disorder and a chronic physical condition had 5.5 days (95%CI = 4.6–6.4) out of role.
Discussion
The 12 month comorbidity patterns in the past year in the 2007 NSMHWB were generally similar to those reported in other large epidemiological surveys and the 1997 NSMHWB. This was despite the use of different classification systems [18], DSM-III-R in the NCS [4], DSM-IV in NESARC [6] as against ICD-10 in the present study. The findings of all these studies are, first, consistent in showing that comorbidity between anxiety, affective and substance use disorders is common. Second, the highest rates of comorbidity were observed between anxiety and affective disorders. Third, there were high rates of comorbidity between substance use disorders and affective and anxiety disorders. Last, there were high rates of mental disorders in those with chronic physical conditions [26]. The associations with disability of these comorbid disorders were also similar in the different surveys. All studies found that comorbidity was more associated with increased disability and increased health service use.
Nearly one in four people with any mental disorder class met criteria for another mental disorder class. Individuals who had a substance use disorder in the 2007 NSMHWB had high rates of other mental disorders. Among those with a substance use disorder, one in five met criteria for an anxiety disorder and one in three met criteria for an affective disorder.
A limitation of the current paper was that we did not have information available on individual disorder comorbidity. The classes of affective disorder, anxiety disorder and substance use disorder contain individual disorders that are likely to vary in the degree of association or comorbidity with other disorders [12]. While future work on this survey will examine these individual comorbidities, it is also the case that the associations of individuals disorders are consistent despite heterogeneity with the findings of mental disorder classes observed in this paper. The overwhelming pattern is that most individual disorders have significant comorbidities with other individual disorders, the strongest associations occur across anxiety and affective disorders, followed by comorbidity between substance use disorders and anxiety and affective disorders [12].
There were higher rates of mental disorders in those with chronic physical conditions compared with those who did not have a chronic physical condition (28% vs 17.6%). The relationship between stroke and mental disorders (affective, anxiety and substance use disorders) that were observed for male subjects in the present study should be considered with caution because they are only associations and do not imply causality. The relationship is complex and the findings not consistent across epidemiological studies [11]. Although there is some debate that mild–moderate alcohol consumption has been linked to a decreased risk for stroke and other cardiovascular disease, excessive use is clearly associated with an increased risk for intracranial haemorrhage and cardiovascular diseases [28]. Affective disorders in those with stroke may impede rehabilitation by impairing physical and cognitive function [29]. Depression and anxiety disorders are also an important consequence of stroke that impacts on recovery but is often undetected or inadequately treated [29].
Untangling comorbidity
Hypotheses about the nature and causal relationships between comorbid disorders cannot be fully examined in cross-sectional epidemiological studies such as the 2007 NSMHWB. Although associations between mental disorder groups and between mental disorders and physical disorders can be described, no conclusions on causality are possible. Untangling the potential causes is crucial to developing effective responses. Cerda et al. have examined this issue within the longitudinal literature and suggest that the causal relationships can operate in both directions between mental and substance use disorders [30], for example conduct disorder and depression both increase the likelihood of developing substance use disorders; the development of substance use disorders among those with depressive and conduct disorders worsens their course; and persons who develop substance use disorders can develop depressive and anxiety disorders [15].
Large scale epidemiological follow-up studies are needed to examine the causal relationship in comorbidity and should be a future focus. The recent 3 year follow up of incident disorders in the NESARC cohort and their relationship to baseline disorders provides a clear example and important information on the relationship between disorders [31]. They found that the presence of some mental disorders at baseline did predict incident disorders during the 3 year follow up (after controlling for demographic variables). Alcohol abuse and dependence were strong predictors of each other, as were drug abuse and drug dependence. By contrast, alcohol and drug use disorders at baseline did not predict an increased incidence of mood disorders. Mood and/or anxiety disorders at baseline (specifically bipolar and panic disorders) did predict an increased risk of drug and alcohol abuse at follow up [31].
Responding to comorbidity
Prevention is a crucial component in the breadth of interventions that should be considered in the area of comorbidity. For example, if we can identify persons with symptoms of anxiety and affective disorders we can potentially intervene to reduce their use of alcohol and other drugs before abuse and dependence develop. Such interventions may have the potential to reduce a substantial percentage of lifetime substance use disorders and an even greater percentage of current disorders [32].
The findings also have a number of implications for the treatment response to comorbidity. A major research focus in the area of comorbidity has been the treatment of comorbid disorders, especially comorbid substance use and serious mental illness [15, 33]. Systematic reviews of studies of substance use and comorbid anxiety and affective disorders [32, 34, 35] suggested that these interventions can be effective but there are still very few well-designed and adequately powered clinical trials [33]. Regardless, specialist mental health services need to better recognize and treat comorbid substance use disorders. This is especially the case with anxiety and affective disorders, because substantial minorities of persons with these disorders who seek treatment in mental health services will have substance use disorders [33]. Specialist drug and alcohol services also need to better recognize the most prevalent disorders that are most amenable to treatment, namely, the anxiety and affective disorders [2, 14, 36]. Australia has developed innovative responses to comorbidity but clearly the improved delivery of care to these groups requires sustained effort [36].
While Australia has focused effort on mental disorder comorbidity, comorbidity with physical disorders also warrants attention, although the evidence for the most appropriate treatment response to these comorbidities is also limited. A recent Cochrane review into the treatment of depression in those with stroke found some evidence of benefit of pharmacotherapy in terms of a complete remission of depression and a reduction in scores on depression rating scales, but there was also evidence of an associated increase in adverse events [29]. Nevertheless, examining such high rates of physical/mental comorbidity will be the focus of future papers.
Conclusions
Comorbidity is a major health issue for Australia. Mental disorder comorbidity is high for both men and women and comorbidity is associated with greater disability and increased service use. A significant proportion of those with chronic physical conditions will have a mental disorder and again the impact on disability is additive [26]. Although comorbidity patterns are complex, it is clear that we require a sustained effort to deliver the most effective prevention and treatment response to this important health issue.
Footnotes
Acknowledgements
The NSMHWB was funded by the Australian Government Department of Health and Ageing, and conducted by the Australian Bureau of Statistics. The authors would like to thank the NSMHWB Reference Group for their input into the survey's design.