
Abstract
The relevance of PTSD to Australian society has never been greater than it is now. At the time of writing this paper, Australia has ongoing military deployments in Afghanistan, Iraq, East Timor, the Solomon Islands, Egypt, the Middle East and the Sudan. The Australian and New Zealand public is still recovering from the devastation of bushfires, flooding, cyclones and earthquakes. The key findings of the most recent National Survey of Mental Health and Well-Being (NSMHWB) [1] confirm an increasing prevalence of this disorder, noting the 12 month prevalence of PTSD as 6.4%. This figure, according to the NSMHWB, makes PTSD now the most prevalent of all individual mental disorders. Hence psychiatrists, psychologists and allied mental health workers need to become more aware of effective treatment options for this growing problem.
The Toowong Private Hospital Combat Related Posttraumatic Stress Disorder PTSD Day Program has been operating since 1998 and has provided cognitive behavioural therapy (CBT) group-based treatment to over 600 servicemen. At the inception of the programme, there was a relative dearth of high quality evidence with respect to effective management of this chronic and severe disorder which conveys high rates of comorbidity and significant functional impairment. Twelve years on, this remains the case in terms of biological management, but there have been noticeable advances in the efficacy evidence base for individual and group psychological approaches with the publishing of randomized control trial data, meta-analyses and multiple national and international clinical practice guidelines for the treatment of PTSD.
An overview of efficacy research into the outcomes of psychological therapies for PTSD can be drawn from meta-analytic studies published since 1998 [2–6]. These comprehensive reviews of controlled studies consistently find that individual and group psychotherapeutic approaches demonstrate statistically significant benefits in PTSD.
The Sherman et al. meta-analysis [5] included 17 studies on a combined sample of 690 participants, the majority of whom received CBT or behavioural approaches. They found a moderate effect size (d = 0.52) from psychotherapy when measured immediately post treatment with no decay in treatment effect at the first follow up point (between 3 and 24 months post treatment, d = 0.53). Bradley et al. [6] (26 studies, 1535 subjects) found that the majority (54%) of patients treated with psychotherapy improved with a large effect size (d = 1.1).
The Bisson et al. [3] (38 trials), Benish et al. [2] (15 trials) and Mendes et al. [4] (23 trials) papers attempted to establish relative efficacy between the different psychotherapies in the treatment of PTSD. The Benish et al. and Mendes et al. analyses found equivalent benefits from treatments intended to be therapeutic for PTSD (CBT, EMDR, cognitive therapy and exposure therapy) which were superior to supportive techniques or waiting list/usual care. The Bisson et al. paper found superiority from trauma-focused CBT and EMDR treatments.
All of the above reviews address caution when generalizing efficacy data to the ‘average PTSD patient’. They allude to the use of inclusion and exclusion criteria, the failure to address polysymptomatic presentations, the heterogeneity of patient groups and the relatively low numbers in individual controlled trials.
One way to address problems of generalizability, small sample sizes and lack of longer term follow up data is to examine the outcomes of established treatment programmes. Whilst clearly lacking the more definitive answers that come from methodologically sound controlled trials, effectiveness or naturalistic research does provide data on the transferability of validated psychotherapeutic modalities from the controlled trial environment into routine clinical practice [7,8]. The growing interest in this type of research has been referred to by some authors as ‘a new era of more ecologically valid psychotherapy research’ [9]. Evidence has emerged, not surprisingly showing more modest effect sizes than those observed in controlled research environments [10,11] Specifically when reviewing combat related PTSD, literature cautions to temper expectations of treatments, given serious comorbidity and the fact that treatment often begins many years after the trauma [12].
Perusal of the literature on group treatment programmes in combat-related PTSD located seven papers evaluating pre- to post-treatment change from a single treatment. Five papers came from evaluations of US programmes. Fontana and Rosenheck [13] drew data from 785 Vietnam veterans and concluded that short stay specialized PTSD treatment programmes produced superior, more sustained and more cost effective improvements when compared with long stay inpatient units. In 1996, Johnson et al. published results of a four month intensive inpatient programme [14]. A total of 51 Vietnam veterans exhibited an increase in symptoms at 6, 12 and 18 month follow up points. In a 2004 follow up paper on the same veteran cohort, Johnson [12] described decreases in violence and substance abuse but ongoing high levels of symptomatology. There was a five-fold increase in mortality rate when compared with US normative data in this age range (17% versus 2.8%). Two further studies evaluating 12 [15] and 17 week [16] programmes found statistically significant improvements in PTSD symptoms (as measured by the Clinician Assessed PTSD Scale), with the 12 week programme showing sustained improvements in overall CAPS scores at 12 months.
The two remaining papers come from Australia and provide perhaps the best data in terms of sample sizes and longer term follow up [17,18]. Both papers come from the Australian Centre for Posttraumatic Mental Health and evaluate pooled outcome data from 9 and 19 accredited inpatient and outpatient, group CBT-based programmes around Australia. As an accredited programme, Toowong Private Hospital contributed to these pooled data sets on both occasions. The 2006 paper evaluated 24 month follow up data on 1508 Vietnam veterans finding an effect size of 0.7 for PTSD at 12 months (as measured by the Posttraumatic Stress Disorder Checklist) and 0.8 at 24 months. These encouraging outcomes provide more robust evidence that brief CBT-based courses produce sustained improvements in PTSD. In the Australian studies therapy was exclusively group-based and produced large effect sizes on par with the predominantly individual treatment data found in meta-analyses.
The recent NSMHWB PTSD prevalence data points toward a growing problem and underlines both the need for further research into effective treatments, and the increasing relevance of group treatment approaches. The TPH database had access to almost 500 veterans with PTSD treated under one established, essentially unchanged programme within the same milieu and with the same core staff between 1999 and 2008.
When conceptualizing this paper, the researchers had to decide how this data could add to the pre-existing literature on PTSD treatment and provide applicable information to clinicians. We hoped to match the magnitude of positive change seen in the pre-existing individual and group efficacy data. To demonstrate that principles learnt from studies on sanitized research populations are transferrable to routine practice, we hoped to add to pre-existing CBT group programme evaluation data by replicating a statistically significant positive outcome. Beyond this, however, we feel our research can show that the benefits seen in PTSD group treatment are not only sustained by individual veterans, but are also consistently reproducible cohort after cohort, year after year for a 10 year period. Hence group treatment for PTSD would be providing a statistically valid, sustainable and repeatable positive symptomatic change in clinical populations. Experts in the literature have questioned a blinkered tendency to judge PTSD treatment success on symptom reduction alone and point towards a greater emphasis on global functioning [19]. For this reason we have also examined some quality of life and global functioning data across 12 months.
Method
Participants
A total of 496 veterans participated in a group-based PTSD programme from 1999 to 2008. All veterans were formally diagnosed with chronic PTSD by their referring psychiatrists. The mean Clinician-Administered PTSD Scale (CAPS) score at assessment was 77.49 (SD = 18.35), indicating significant PTSD symptomatology. Self-report data at intake indicated 72.3% of veterans presented with depressive symptoms (Hospital Anxiety and Depression Scale (HADS) depression), 90.9% with anxiety symptoms (HADS anxiety) and 65.9% with significant alcohol abuse (Alcohol Use Disorders Identification Test (AUDIT)). The majority of veterans (75%) were unable to work in a full-time capacity because of severity of symptoms.
All veterans were male apart from one. Veterans’ ages ranged from 25 years to 74 years, with a mean age of 53 years, median age of 55 years and mode age of 57 years. Nearly 80% had served in the army, 18% in the navy and 2% in the air force. The majority of veterans served in the Vietnam conflict (68%), with the remainder serving in combat zones prior to Vietnam (e.g. Korea, Malaya) and various peacekeeping operations post Vietnam (e.g. East Timor, Somalia, Rwanda, Iraq, Afghanistan). Most veterans were married or in a long-term relationship (79%).
Measures
Participants completed a variety of mental health self-report questionnaires contained within the Australian Centre for Posttraumatic Mental Health (ACPMH) outcome measures protocol. The questionnaires targeted symptoms of PTSD, marital satisfaction, alcohol use, anger, depression, anxiety and quality of life. The questionnaires were administered on four occasions: intake, discharge, 3 months post treatment and 9 months post treatment. All particpants who attended assessment occasions were administered all questionnaires.
A brief description of each questionnaire is described below.
The Clinician-Administered PTSD Scale
The Clinician-Administered PTSD Scale was developed by the US National Centre for PTSD in Boston [20]. This 30 item clinician-administered assessment tool contains criteria testing the intensity and frequency of all 17 DSM-IV PTSD symptoms. The CAPS has shown good sensitivity (0.84), is highly specific (0.95), and has excellent test–retest and inter-rater reliability [21].
The Posttraumatic Stress Disorder Checklist
The Posttraumatic Stress Disorder Checklist (PCL) [22] is a 17 item self-report questionnaire measuring specific PTSD symptoms contained within three subscales. The use of this self-report scale on male combat veterans has been well validated [23]. The PCL has excellent test–retest reliability (0.96) [22] and exhibits a strong correlation with other measures of PTSD [24].
Abbreviated Dyadic Adjustment Scale
The Abbreviated Dyadic Adjustment Scale (ADAS) is a 7 item self-report measure of marital satisfaction [25]. The mean score for marital satisfaction was determined at 22.5 (SD = 5.4).
The Alcohol Use Disorders Identification Test
The Alcohol Use Disorders Identification Test (AUDIT) is a 10 item self-rated screening tool, developed by the World Health Organization in 1989 to assess hazardous and harmful alcohol use [26]. Saunders et al. demonstrated that a cut-off score of 8 on the AUDIT would reliably diagnose persons with hazardous or harmful alcohol use [26].
Dimensions of Anger Reaction
The Dimensions of Anger Reaction (DAR) is a short 7 item self-report measure of anger [27]. Scores range from 0 to 56, with higher scores indicating strong anger reactions.
The Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) is a 14 item self-report instrument measuring symptoms of anxiety and depression [28]. Dagan et al. (2000) described robust psychometric properties with this instrument [29].
Brief World Health Organization Quality of Life Instrument
The Brief World Health Organization Quality of Life Instrument (WHOQOL-Bref) is a 26 item self-report questionnaire measuring quality of life over four domains (physical, psychological, social, environment). It has shown good to excellent reliability and performs well on tests of validity [30].
Procedure
This programme employs a predominantly cognitive behavioural approach. The CBT is group-based and utilizes a comprehensive manual, homework tasks, video presentations, and numerous field trips. Additionally, veterans receive individual sessions on a weekly basis with an allied health clinician, have access to individual psychiatric input, and receive approximately 20% of sessions with their partners.
The fifteen modules covered incorporated psycho-education, cognitive therapy, relaxation and distraction techniques, together with imaginal and in vivo exposure. Specific topics include psycho-education on PTSD prevalence, symptoms, aetiology, and management. Additional education is provided on post trauma reactions, survivor guilt, addictive behaviours, medications, and physical wellbeing. Veterans are taught skills to manage anxiety, depression, anger, and sleep difficulties. They have sessions on basic problem solving and goal setting, and receive communication and social skills training.
The programme does not employ group sessions dedicated to strict trauma-focused work, given the heterogeneity of identified traumatic situations, concerns over therapeutic alliance and trust, and the potential for symptom exacerbation and increased drop-out rates.
The programme incorporated an initial 6 week intensive phase where veterans attended 8.30 a.m. to 4.00 p.m. 4 days per week for 6 weeks (total 24 days). The intensive phase was followed by fortnightly 2 day sessions over a 6 week period (total 6 days). Veterans then attended 1 day follow-up sessions at 3 months and 9 months post-intensive phase (total 2 days). From 2000 to 2008, 64 groups completed the programme.
Health professional involvement includes two consultant psychiatrists, two clinical psychologists, two social workers and two registered nurses. A physiotherapist/physical trainer is employed, together with numerous guest speakers (drawn from ex-course participants, veteran advocacy groups and ex-service organizations).
Results
Preliminary data analysis
Sample size at intake
The sample size for veterans completing the PCL, HADS anxiety, HADS depression and AUDIT questionnaires at intake was n = 496. The sample size for veterans completing the full suite of questionnaires at intake (i.e. including DAR, ADAS and WHOQOL-Bref introduced in 2002) was reduced to n = 298.
PCL missing data (completers and non-completers)
Of the 496 veterans who commenced the programme, approximately 24% did not attend the final follow up session (9 months data point) and therefore did not complete the programme or questionnaires at that point. Hence, no data was available to examine non-completer outcome. Completers were defined as participants who completed both the PCL at intake and 9 months post treatment. Non-completers were defined as participants completing the PCL at intake, but not at 9 months post treatment.
There was no statistically significant difference between completers and non-completers with respect to intake PCL scores (p = 0.298). When utilizing a conservative ‘last observation carried forward’ (LOCF) type technique (by carrying forward the non-completers’ intake PCL score to the 9 months data point), we continued to demonstrate an effect size score in the moderate range (d = 0.5, down from 0.7). Investigation of skewness of data within the two groups indicated mild negative skew for both populations (completers: −0.654, non-completers: −1.057), with neither group falling in the ‘severe range’ (>−0.2), as defined by Hildebrand [31].
No statistically significant differences were noted between completers and non-completers with respect to symptom measures at intake; HADS depression (p = 0.259), HADS anxiety (p = 0.8), AUDIT (p = 0.97) and DAR (p = 0.296). No significant difference was noted on marital status (p = 0.492) between the two groups. A statistically significant difference with respect to age (p < 0.001) was noted with the non-completer group having a younger mean age.
Dependent variables
Outcome measures were grouped into two separate components. The first group combined measures which reflected symptom change, where improvement was noted by a decrease in test scores (PCL, HADS Anxiety, HADS Depression, DAR). The second group combined measures which reflected quality of life issues where an increase in test scores indicated improvement (WHOQOL-Bref Physical, WHOQOL-Bref Psychological, WHOQOL-Bref Social, ADAS). Both groups were subjected to separate repeated measures MANOVA analyses. Multivariate analysis was chosen to reduce the likelihood of Type I error expected with a number of repeated analyses of variance.
Because the AUDIT was considered relatively insensitive to change over short time frames, treatment of this variable was confined to intake and 9 months post treatment scores only. A paired samples t test was employed to test for statistical significance.
All data was analysed with SPSS version 17 (Chicago, IL).
Treatment significance and effect sizes
Effect sizes
Change scores were determined by outcome differences on a variety of clinical symptom measures from intake to 9 months post treatment. Strength or impact of group treatment was determined by effect sizes (Cohen's d), calculated by dividing the changed score by the pooled standard deviation. In clinical terms, Cohen (1975) indicated 0.5 as a moderate change and 0.8 as a large change [32].
As noted in Table 1, most effect size results were in the moderate strength range (0.4–0.7). A small effect size was associated with a measures of marital satisfaction (ADAS: d = 0.2).
Univariate test results for symptom change and quality of life components; means, standard deviations at each assessment point; effect sizes (Cohen's d)
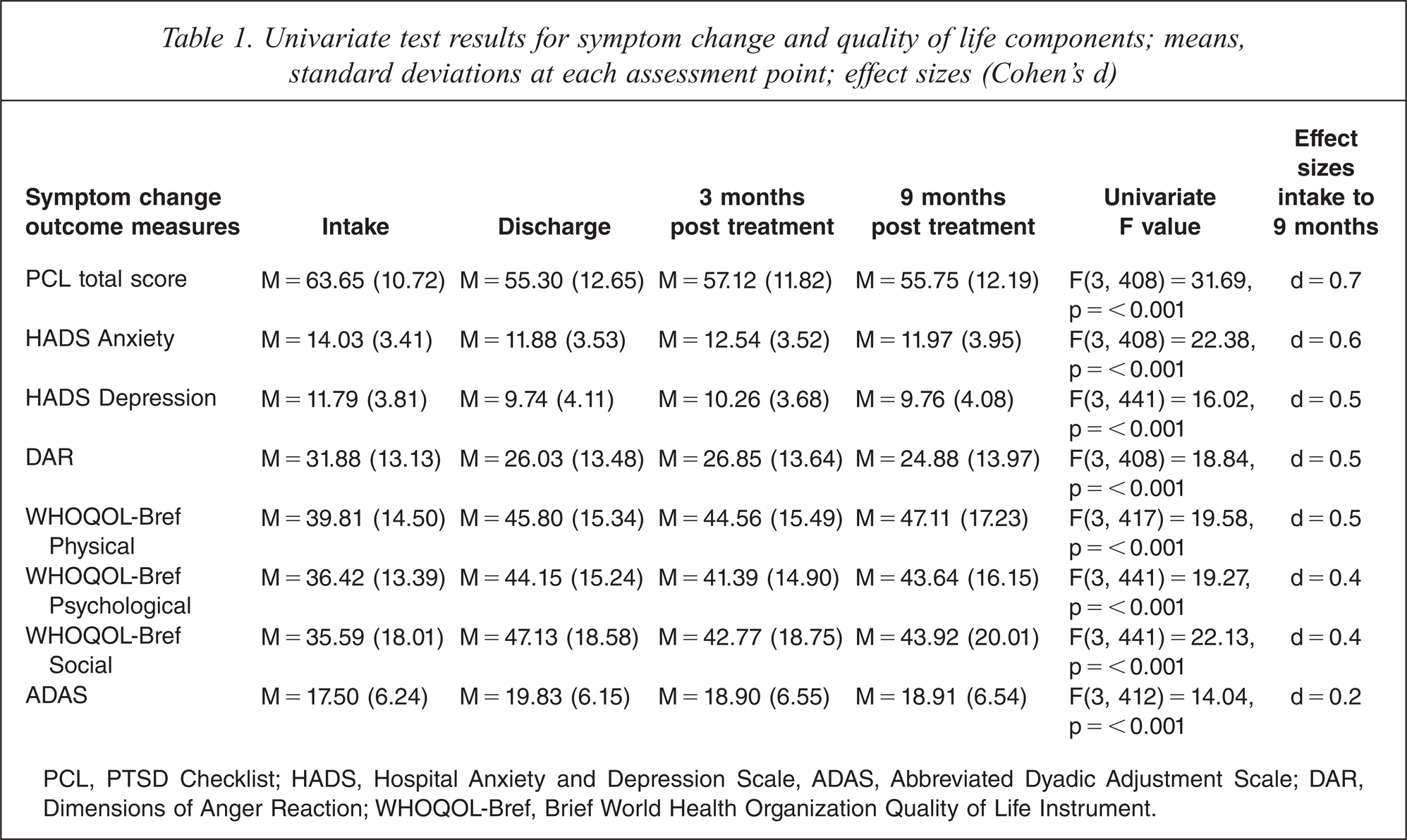
PCL, PTSD Checklist; HADS, Hospital Anxiety and Depression Scale, ADAS, Abbreviated Dyadic Adjustment Scale; DAR, Dimensions of Anger Reaction; WHOQOL-Bref, Brief World Health Organization Quality of Life Instrument.
Statistical significance
MANOVA with repeated measures was conducted across the four assessment points (intake, discharge, 3 months post treatment, 9 months post treatment), to include outcome measures associated with symptom change (combined scores: PCL, HADS Anxiety, HADS Depression, DAR). The overall MANOVA result was highly significant: F(3, 595) = 46.35, p < 0.001. Univariate test results for each of the dependent variables are outlined in Table 1. The results indicated statistical differences at a highly significant level for each of the four measures (p < 0.001). Post hoc pairwise comparisons for the combined symptom change variables indicated maximal changes occurring at the discharge assessment point, with no statistically significant differences between assessment points after that time (see Figure 1). There was a statistically significant difference, however, on one of the measures (HADS Anxiety) between the discharge and 3 months assessment points (p = 0.049), indicating mild return of anxiety symptoms during this period. However, there was no statistically significant difference between discharge and 9 months post treatment scores.
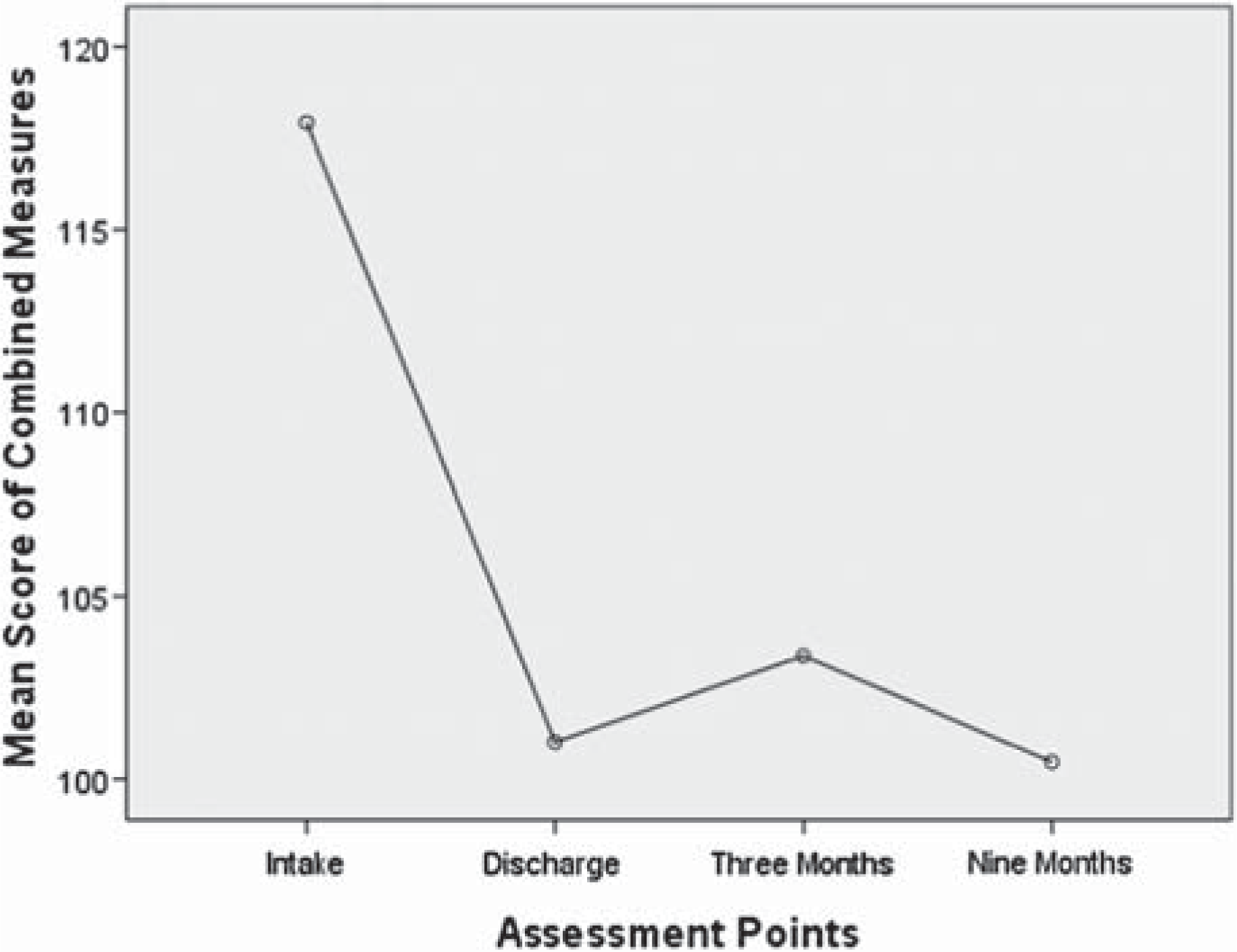
Symptom change (PCL, HADS Anxiety, HADS Depression, DAR).
MANOVA with repeated measures was also conducted across the four assessment points for quality of life outcome measures (combined scores: WHOQOL-Bref Physical, WHOQOL-Bref Psychological, WHOQOL-Bref Social, ADAS). The overall MANOVA result was statistically significant: F (3, 601) = 42.243, p < 0.001. Univariate test results for each of the dependent variables are outlined in Table 1. The results indicated statistically significant differences for each of the four measures (p < 0.001). Post hoc pairwise comparisons indicated a statistically significant difference between intake and discharge scores (p < 0.001). Mean scores are represented in Figure 2. There was a statistically significant difference between the discharge and 3 months assessment points (p = 0.002), indicating a decrease in overall quality of life during this time. This was largely accounted for by a statistically significant difference on the WHOQOL-Bref Social questionnaire items (p = 0.016). However, there was no statistically significant difference between discharge and 9 months post treatment scores on overall quality of life when the outcome measures were combined (p = 0.271). Post hoc analysis also revealed a statistically significant difference between ADAS intake and discharge scores (p < 0.001), indicating improved marital/ relationship satisfaction at discharge when compared to pre-treatment levels. However, there was no statistically significant difference between intake and 9 months post treatment scores (p = 0.084), indicating no sustainable improvement in this area from pre-treatment functioning.
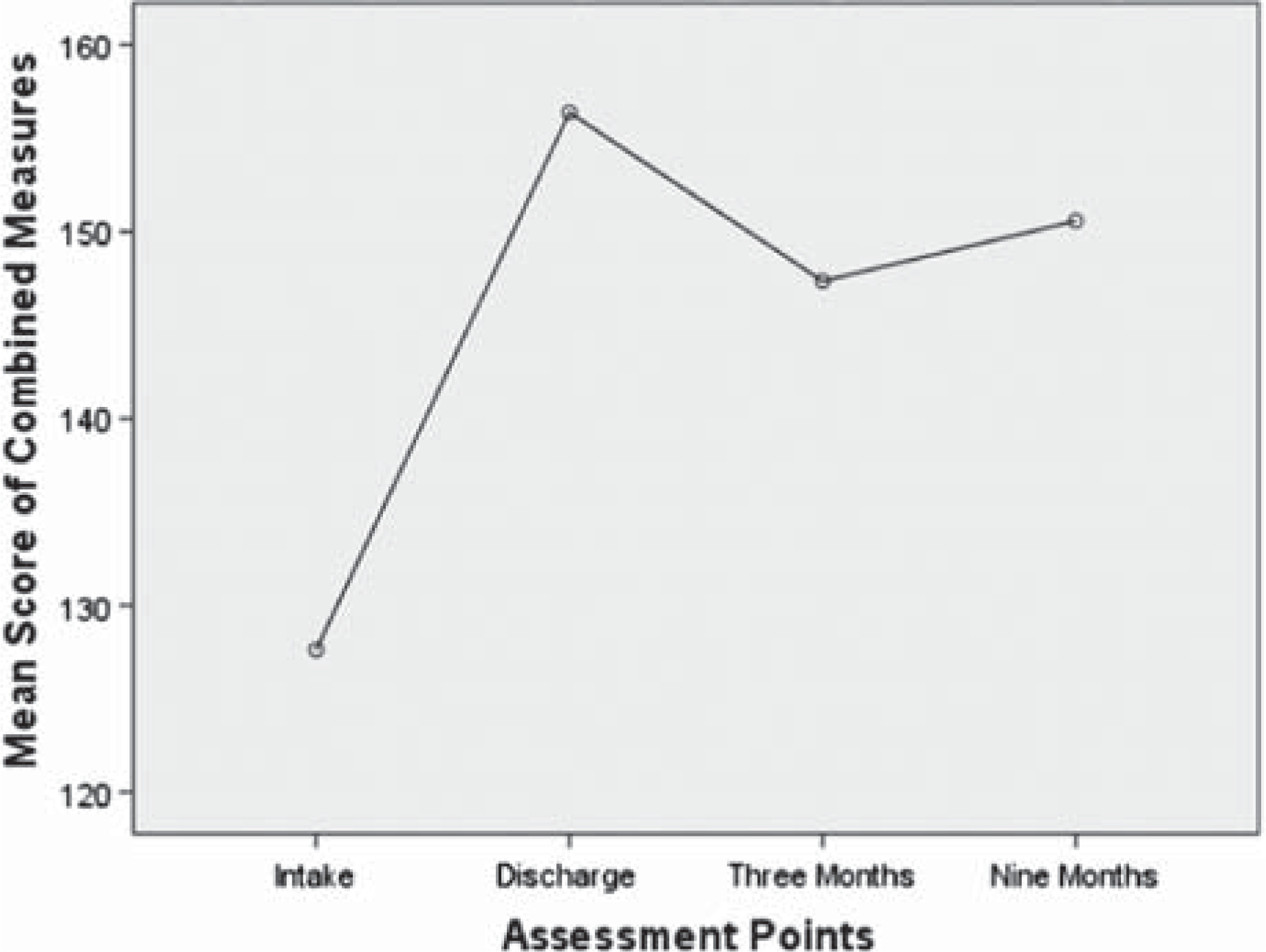
Quality of life (WHOQOL-Bref Physical, Psychological, Social, ADAS).
A paired samples t test was conducted between intake and 9 months post treatment AUDIT scores. The results indicated a highly significant difference between the two assessment points (t (375) = 6.319, p < 0.001), indicating veterans were consuming less alcohol at the conclusion of the programme. The effect size, however, was calculated as small (d = 0.24).
Clinical and reliable improvement in PTSD symptoms
Investigation was made to determine the number of participants who responded clinically during the course of the programme with respect to PTSD symptoms from intake to 9 months post treatment (n = 496). PTSD symptom outcomes were classified into three distinct entities based upon reliable and clinically significant changes on the PCL (clinically significant remitters, significant responders, non-responders).
PCL reliable change index scores were determined through our own dataset and references from other studies. Weathers et al. [22] determined the internal consistency coefficient (Cronbach's alpha) for the PCL on a sample of 123 male Vietnam veterans was in the order of 0.97. For this study, reliable change cut-off scores for the total PCL were established at − 5 (improvement) and + 5 (deterioration). These scores were also cited in a paper by Monson et al. [33]. Clinically significant change on the PCL was determined if the score fell below 50.
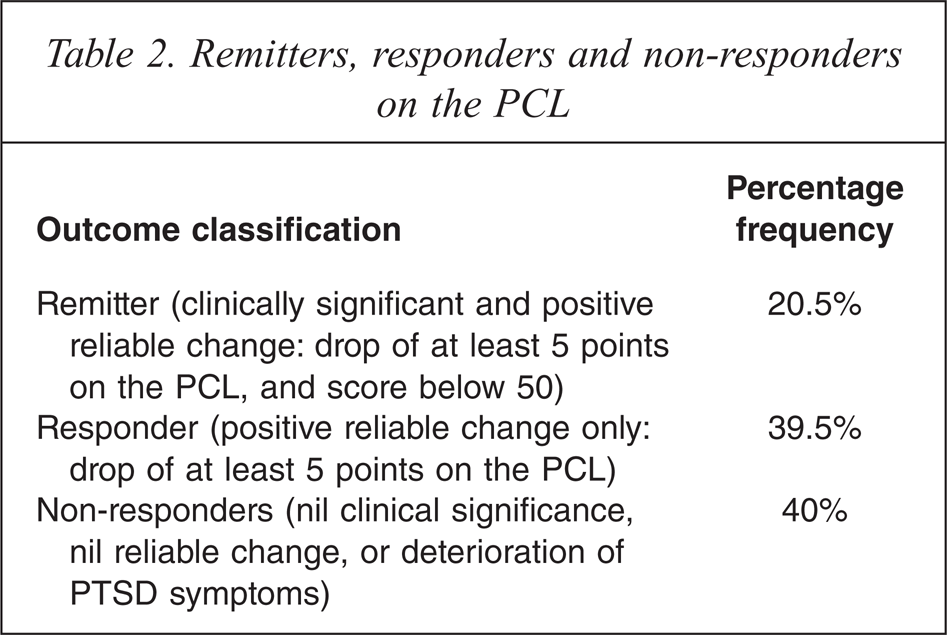
Remitters were defined as participants who demonstrated both clinically significant and positive reliable changes from intake to 9 months post treatment on the PCL. Responders were defined as participants who demonstrated positive reliable PCL changes only, and non-responders defined as achieving neither of these outcomes.
As noted in Table 2, nearly 21% of participants achieved both clinically significant and positive reliable changes on the PCL during the course of the programme. A further 39% achieved positive reliable changes only. When aggregated, a total of 60% of veterans demonstrated improvement on PTSD symptoms over the course of the programme. Conversely, 40% of participants failed to achieve a reliable positive clinical change in PTSD symptoms.
Remitters, responders and non-responders on the PCL
Repeatability of change with respect to PTSD symptoms
A mixed two-factor ANOVA was completed to investigate whether clinical changes in PTSD symptoms (PCL) could be sustained reliably over time, regardless of group membership and year of treatment. This analysis included PCL score changes from intake to 9 months post treatment for all groups within specific years, and across years from 2000 to 2008.
The results revealed a significant main effect for the PCL change scores, indicating reliable statistically significant changes in PCL scores between these two assessment points for each group over time: F(1, 334) = 164.56, p = <0.001. There was no interaction between the year of the treatment group and PCL change scores, indicating that the change in scores over the time points was not influenced by group membership.
The ANOVA indicated a significant main effect for group membership, indicating variability in PCL change scores across groups: F(8, 334) = 1.99, p = 0.047. However, post hoc pairwise comparisons of mean change scores indicated no statistically significant differences between treatment groups from year to year. This indicated that, overall, groups were fairly similar in outcome, and that reliable improvements in scores occurred over time.
A multi-level model to account for nested data was not considered because a previous study which incorporated much of this data [18] found little evidence to suggest that cohort effects played a significant role in observed symptom improvements.
Discussion
Analysis of the effectiveness of our CBT-based 6 week (24 sessions) closed, day patient group programme for combat-related PTSD contributes to the evidence base on PTSD management in several ways [31]. Primarily we were able to show that our programme was effective at reducing PTSD symptoms in a significant and sustained way. This added to the increasing literature presence of effective treatments for PTSD being employed in routine clinical practice. Secondly, by using a 9 year dataset we feel we have extended current research by providing a longitudinal perspective and showing that significant and sustained improvements are consistently reproducible year after year. In addition, the paper provides the reader with clinically applicable information on observed points of maximal symptom change, clinically relevant (as opposed to statistically significant) symptom change, and our conclusions regarding group therapy in the global treatment of PTSD.
Our data indicated a drop-out rate of 24% over the 12 month study period. This rate was comparable to that seen in published efficacy (up to 30% in active treatment arms) [3] and effectiveness (32% over 24 months) [18] research. We were not able to elucidate any statistically significant differences between 12 month completers and non-completers in terms of intake symptom severity. The only significant difference noted between the two groups was related to age, with the non-completer group showing a younger mean age. This finding suggests greater difficulties maintaining younger veterans in treatment. A LOCF type analysis of PCL data continued to realize a moderate Cohen's d effect size of 0.5.
Veterans exhibited a statistically significant reduction at 12 months in all PTSD symptom clusters and on all measures of comorbid symptoms. When presented as a Cohen's d figure (0.68), the PTSD symptom scores demonstrated a moderate to large effect size which was comparable to that seen in pre-existing efficacy and effectiveness literature on group therapy outcomes in PTSD [19]. The magnitude of positive change seen in measures of depression, anxiety and anger achieved a moderate effect size, whilst small effect size changes were seen in measures of alcohol use. The AUDIT results were comparable to other studies of Australian veterans [18]. In our cohort, results may have been influenced by the regular triage of veterans noted at assessment as having ongoing alcohol abuse or dependence issues, into alcohol programmes to be completed prior to beginning a PTSD course.
In an attempt to add further weight to our results we divided our 9 year dataset into calendar year cohorts. We were able to show repeatable statistically significant improvements year by year, with an average effect size of 0.68.
In addition to symptomatic evaluation, we examined 12 month outcomes on the WHOQOL-Bref finding statistically significant improvements on three subscales with a moderate ES. No significant improvement was found on measures of marital satisfaction (ADAS) at 9 months post treatment. It was hypothesized that the chronicity and comorbidity associated with service-related PTSD and its observed negative impact on domestic relationships accounted for this result. With sessions on communication and assertiveness, many veterans reported beginning the process of conflict resolution but tended to become more aware of problems in the relationships (and hence less satisfied).
There are clinically applicable messages to be derived from the time of change data presented in the paper. For all measured parameters the period of maximal symptom change occurred between the intake and discharge points (over the intensive treatment phase). For PTSD, anger symptoms and two (psychological and physical) of three subscales of the WHOQOL-Bref, statistically significant differences existed between intake symptoms scores and all subsequent follow up points (discharge, 3 and 9 months post treatment). No statistically significant differences were noted between the discharge, 3 and 9 month post treatment time frames indicating stability in symptom reduction. Data for depression and anxiety symptom scores (HADS) and the WHOQOL-Bref social subscale also improved significantly from the intake to discharge point, but worsened at the 3 month follow up before stabilizing (i.e. no difference noted between the 3 and 9 month follow up points). Hence, given this large sample size, clinicians could reasonably assume that if there are no observable improvements in PTSD, depression, anxiety and anger symptoms after 3 months of CBT-based group therapy, further improvements over the ensuing 9 months are unlikely. This was also the case for quality of life scores.
Using reliable change data for the PCL-M tool, we found that 6 in 10 participants exhibit a clinically meaningful positive response in symptoms at the 12 month point and 2 in 10 will no longer meet criteria for PTSD. However, 4 in 10 will exhibit no detectable positive clinical change. The Bradley et al. [6] meta-analysis which included a section on clinically meaningful improvement arrived at a figure of 54% of those completing treatment having achieved a clinically meaningful improvement. The 2006 Australian paper [18] divided their 24 month sample into tertiles and found that the bottom tertile deteriorated, the middle tertile exhibited a small improvement and one third of veterans demonstrated an improvement of over 30% in PTSD scores. Unfortunately this paper was not able to add to the little that is known regarding moderators and mediators of group therapy outcome [19].
In a comprehensive literature review on the use of psychotherapeutic modalities in PTSD, the International Society for Traumatic Stress Studies concludes that at present there is not sufficient evidence to warrant the recommendation of either individual or group therapy in preference to the other, or the use of one type of group therapy over another [19]. Our findings would support this statement in that our cumulative effect size of 0.68 approximates efficacy data effect sizes for individual psychological therapy [6]. Given the increasing prevalence of this condition, the ability of group therapy to address greater numbers of sufferers argues for an increased focus on this treatment modality. We estimate that approximately 90% of our study cohort were already involved in treatment from a psychiatrist and/or psychologist at intake. With few exceptions group participants suspended their individual treatment during participation in the intensive phase (3 months from intake to discharge) of the programme. The period of maximal symptom change occurred over this period, leading the researchers to hypothesize that the observed symptomatic gains were primarily due to group treatment and independent of individual therapy. This finding suggests that group therapy could be utilized as an adjunct, as well as an alternative to individual therapy. It is our feeling, however, that group therapy works best in the former situation and may potentiate subsequent individual therapy. This may account for the increasing benefits over follow up in the Creamer et al. study [18]. This, however, would need to be more critically examined.
There are potential cost and access gains to be had from stand alone group therapy. However, when considering our recommendation for adjunctive group therapy, clinicians would need to weigh the potential clinical benefits against the additional cost.
Limitations
Interpretation of our data requires caution as definitive cause and effect conclusions are precluded by the uncontrolled study design.
This study lacked specific information on psychotropic medication use, the type and extent of external individual psychotherapy being employed outside the programme and proximal life events. This information would have enhanced the study.
Our study involved male veterans with a relatively homogeneous trauma type. As such, generalization of our results to female or civilian cohorts with PTSD requires caution.
Future directions
The literature identifies one study directly comparing individual and group therapy [34]. That paper was unable to separate the two modalities in terms of outcome. Hence the question of relative efficacy of individual versus group approaches remains unanswered. A further question raised by our research would involve measuring the added benefit of group therapy when used as an adjunct to individual psychotherapy in PTSD.
Research on whether our encouraging group therapy results on male veteran populations are generalizable to male and female civilian PTSD cohorts with more heterogeneous trauma would be meaningful to clinicians. The researchers are currently examining this question and are conservatively optimistic given that the literature consistently refers to veteran populations having worse PTSD treatment outcomes [3,19] when compared to civilian cohorts.
Observations of our naturalistic cohort suggest the need for more research investigating therapeutic and milieu aspects which would improve engagement with younger veterans. Further we are considering a greater emphasis on communication and domestic relationships to address our finding of non-sustained marital satisfaction scores in our participants and would welcome research in this area.
A greater focus on locating the effective therapeutic elements of a group therapy modality in PTSD would be beneficial. There is limited knowledge on positive and negative prognostic indicators for group therapy. This is particularly relevant in light of the lack of positive clinical response in 40% of our participants and the lower mean age of our non-completer group.
Conclusions
This paper adds to effectiveness research literature on group psychotherapy for PTSD. It shows that CBT concepts established by efficacy research can be taken into routine clinical settings and produce equivalent outcomes. Our results replicate the magnitude of symptom change seen with group therapy in previous research and provide longitudinal data showing that these significant and sustained outcomes are consistently reproducible. Importantly, quality of life measures also showed significant and sustained improvements in our study. With regard to our group CBT programme, our data suggests that the greatest symptomatic gains occur within the first 3 months of therapy and that 60% of patients’ symptoms will respond (in a clinically significant way). We would hope that clinicians can use this information and give consideration to the role of group therapy in the treatment of their patients.
Footnotes
Acknowledgements
We thank David Crompton for establishing the TPH Veterans PTSD group programme and encouraging outcomes research. We thank the ACPMH for collaboration in the collection and processing of data, and Sara Olsen for her advice on statistical matters. We also acknowledge Gordon Smith for his 12 year tenure as coordinator of the programme and finally, and most importantly, all Australian current and ex-service personnel.