
Abstract
Keywords
The high prevalence of depressive disorder patients and clinically significant depressive symptom ‘cases’ (i.e. patients with bothersome depressive symptoms that do not fulfil formal criteria for a depressive disorder) among the elderly [1] underlines the relevance of follow-up studies of these patients concerning morbidity, mortality and health care services utilization. Such studies have shown that community-living depressive disorder elderly patients and depressive symptom cases use more somatic in- and outpatient services including emergency medical services, primary care services and medications, but also that they use less psychiatric services including antidepressants [1–9]. Two studies showed higher consumption of somatic services to be particularly prominent and that elderly depressive disorder patients are more likely to be referred to services not suitable for treatment of depression [10,11]. In another two studies, community-living depressive disorder patients had only increased outpatient services utilization [12,13].
Literature on the comorbidity with depressive disorders shows that physical illness (e.g. cardiovascular and cerebrovascular diseases), cognitive disorders and functional impairment are main predictors of depressive disorders in the elderly [1].
Studies of mortality with depression are contradictory. Some studies report depressive symptom ‘cases’ and mild to moderate depression to be associated with no increased risk [14,15] while others report increased mortality [16–18]. Most studies, however, showed increased mortality in severe depression [14,17,19–21], especially chronic depression [22].
Follow-up studies show that depressive disorders among elderly in primary care have a poor prognosis [23] with under-utilization of psychiatric services [24–26]. Inconsistent with guidelines, elderly patients with and without depression commonly receive treatment with benzodiazepines [26,27,28] and it seems well documented that antidepressants are under-used [1,26].
A study of the need for psychiatric services among rural elderly Americans with depressive symptoms suggested that lack of awareness of available services and lack of routine contact with mental health service providers are important factors limiting the use of these services [29].
In an 8-year controlled follow-up study of inpatients with depressive disorder and frail rural community-living patients with depressive disorder or dysthymia [30] diagnosed according to ICD-10 [31], we saw significantly increased rates of recurrent depression, consumption of antidepressants, use of psychiatric in- and outpatient admissions, hospital days and outpatient home visits, but no increased use of somatic services or mortality [32].
The overall objective of the present 13-year follow-up study was to evaluate whether there were differences in morbidity, mortality and use of health care services as a function of depression, frailty and urban/rural living.
Materials and methods
Materials
This study included individuals 70 years of age or older (70+ years) on the date of entry in the index study in 1996, i.e. groups I and II [30] (Figure 1). In 1996 the subgroups I and II were extracted from the local social welfare register system. Frail elderly people are defined as community-living elderly people to whom municipality visiting nurses have assigned municipality home help in their private home, or residence in a public nursing home on mental and/or physical indications.
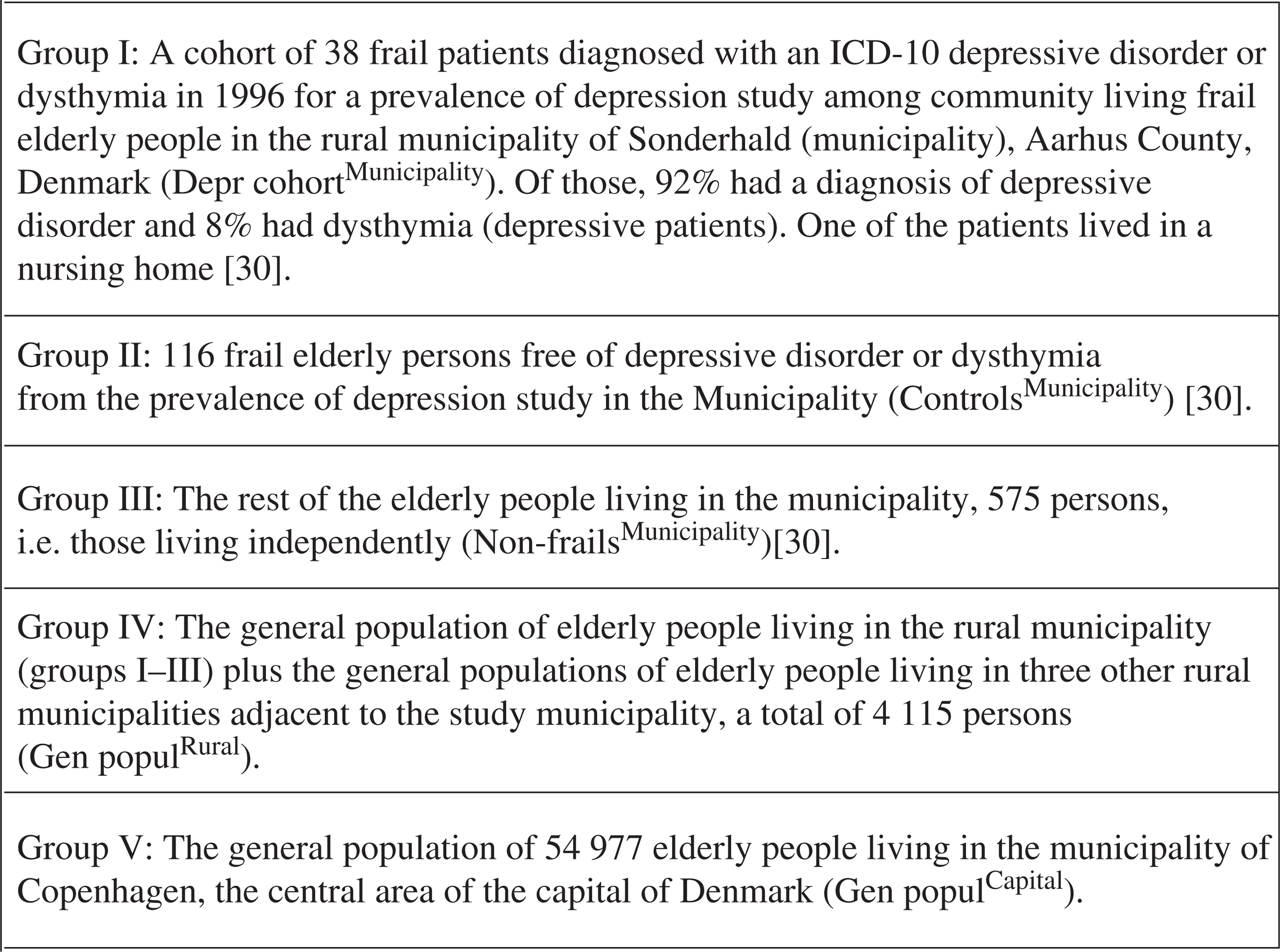
Definitions of the five groups of 70 years of age or older (elderly) participants of the study
The study also included two register-identified 70+ years general populations of rural (group IV) and urban populations (group V), respectively. These data, and data on group III (Figure 1), were extracted from the Danish Civil Registration System [33].
The study was approved by the Danish Data Protection Agency and the scientific ethic committee.
Methods
Overall study methodology
We compared morbidity, mortality and use of health services among five subgroups, i.e. (i) the specified clinical groups I, II and III, and (ii) the register [33] identified general elderly rural and capital living populations, groups IV and V (Figure 1). The general elderly rural and capital populations are studied with the purpose to widen the epidemiological perspective of the subject of morbidity, mortality and services utilization among elderly people living in different sociodemographic areas.
Periods of investigation
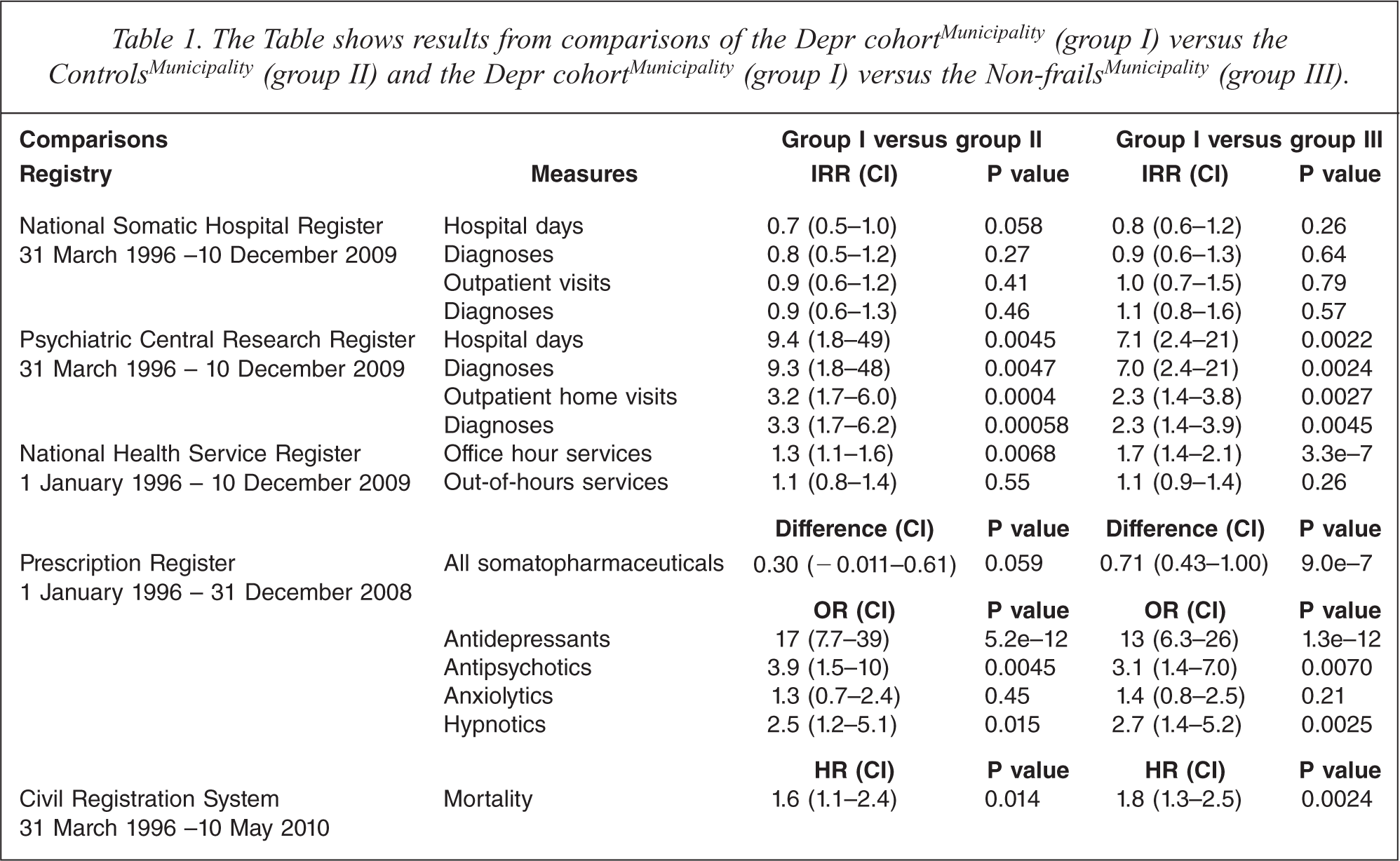
The study included data on health characteristics from 31 March 1996 and follow-up periods. Specification of the periods of investigation appear from Table 1, column one.
The Table shows results from comparisons of the Depr cohortMunicipality (group I) versus the ControlsMunicipality (group II) and the Depr cohortMunicipality (group I) versus the Non-frailsMunicipality (group III).
Data
Data were collected from the Danish national disease and health registers that provide prospectively registered data. The registers are: (i) the Danish National Somatic Hospital Register [34], (ii) the Danish Psychiatric Central Register [35], (iii) the Danish National Health Service Register [36], (iv) the Danish Prescription Registry [37], (v) the Centralised Civil Registration System [38] and (vi) the Danish Register of Causes of Death [39].
Variables
The variables measured during follow-up were: (i) hospital days, (ii) outpatient visits, (iii) psychiatric and somatic disease diagnoses, (iv) GP services, (v) medications, (vi) causes and manners of death and (vii) survival time. Note that the National Health Service Register only provided type and quantity of GP services, not diagnoses.
Statistics
Comparison groups
First, the three clinical groups I, II and III from the municipality (Figure 1) are compared with each other. Next, the register identified four rural municipalities (group IV) are compared with the central urban area municipality population of Copenhagen (group V).
Follow-up period
Each individual's period in the study (‘risk time’) was calculated as the time in years from study entry and until death or end of registration. Period length varies between registries as noted in Table 1. The logarithm of the risk time was included as a covariate in all analyses to account for differences in follow-up time except for survival analyses where the dates define the entry and exit time.
Confounders
The subjects’ gender and age on 31 January 1996 were included as covariates in all analyses. Age was centralized by subtraction of the grand mean calculated from the groups to be compared.
Analyses/models
The following quantities (individually aggregated over the entire study period) were analysed using negative binomial generalized linear models (GLMs) with logarithmic link function [40]: number of hospital days, number of outpatient treatments and number of diagnoses (separate analyses for somatic and psychiatric hospital admissions), and the number of GP services (office hours and out-of-hours, respectively). Negative binomial regressions were chosen to account for over dispersion, i.e. extra variation that implies a pure fit of the usual Poisson distribution.
We used the parameterization with constant dispersion (opposed to the parameterization where the dispersion is a function of the expected mean) as this resulted in the best fit. The result from comparing one group with another is shown as an incidence rate ratio (IRR) with a corresponding 95% confidence interval (CI). Survival curves and estimated hazard rate ratios (HR) were obtained from Cox regressions. Natural versus unnatural manner of death (only available until 31 December 2006) was analysed using a binomial GLM with a logarithmic link function [40]. In every case, two-sided likelihood ratio tests (one degree-of-freedom chi-square) were used to test the null hypothesis that the ratio equals one.
Analysis/model for the prescription data
Separate analyses were made for the following groups of Anatomical Therapeutic Chemical (ATC) codes: antidepressants (N06A), antipsychotics (N05A), anxiolytics (N05B), hypnotics (N05C), and somatopharmaceuticals (all other codes). Contrary to the other analyses, data from the prescription registry included a yearly aggregated number of sold defined daily dosages (DDD) for each ATC code. The logarithm of the proportion of a year that the individual was alive was included as a covariate to the models. Records missing ATC (and therefore DDD) do not contribute to the yearly counts but are potential confounders, as the pattern of missing differs between the groups and the number of missing ATC to some degree correlates to the aggregated measure of drug use (results not shown). In addition to the adjustment for gender and age, we therefore included a dichotomous factor giving a change in intercept for those having at least one record missing ATC (in that year) plus a slope parameter for the number of missing ATCs (individually aggregation per year). Moreover, potential change in medication use over years was accounted for by a four degree polynomial in years since 1996. Somatopharmaceuticals were analysed using generalized estimation equations (GEEs) with a gamma distribution, logarithmic link function, and exchangeable correlation structure [41]. Coefficients (or contrast) measuring the difference in DDDs (logarithmic scale) between groups were estimated with 95%CI and Wald's tests (one degree-of-freedom chi-square) were used to test the null hypothesis that the coefficient equals zero. Psychopharmaceutical usage (yes/no) of each of the four medications was analysed by use of binomial GEEs with logit link function [41] and the same covariates and confounders as for somatopharmaceuticals. Results are given as odds ratios (OR) with 95%CI and the null hypothesis, OR = 1, was tested by a Wald's test.
Multiple testing
All analyses were carried out using Stata 11 (StataCorp 2009). A significance level of 5% was chosen but as a number of tests have been carried out the thresholds for significance should be adjusted for multiple testing [42]. We consider each pair of groups compared and each registry a separate family of tests. Thus to keep the family-wise error rate near 5% we (maybe somewhat conservatively) used a Bonferroni threshold (Bt) for four tests on somatic registrations (Bt = 0.0125), four on psychiatric disorders (Bt = 0.0125), two for health service utilization (Bt = 0.025), five concerning medications (Bt = 0.01) and one for mortality (Bt = 0.05). That is, only P values below the corresponding Bt are considered significant. The comparison of natural/unnatural death was considered explorative only. P values and CIs are shown unadjusted.
Results
Median ages with standard deviations in parentheses and age ranges for the groups I, II, III, IV and V (Figure 1) were: 79.7 (6.3); 69.0–93.4, 81.3 (6.8); 69.1–101.1, 76.4 (6.8); 70.0–98.2, 77.7 (5.9); 70.0–101.1 and 79.3 (6.2); 70.0–106.7.
The total risk time measured in person years was 197 for the Depr cohortMunicipality (group I), 717 for the ControlsMunicipality (group II), 4,547 for the Non-frailsMunicipality (group III), 29,579 for the Gen populRural (group IV) and 362,941 for the Gen populCapital (group V). Total number of participants (n) in the five groups and percentages of women (%) were on 31 March 1996: group I n = 38 (74%), group II n = 116 (64%), group III n = 575 (49%), Group IV n = 4,115 (55%) and Group IV n = 54,977 (68%). All patients in the
Results from comparisons of the measured variables among the
The results from comparing measures of the
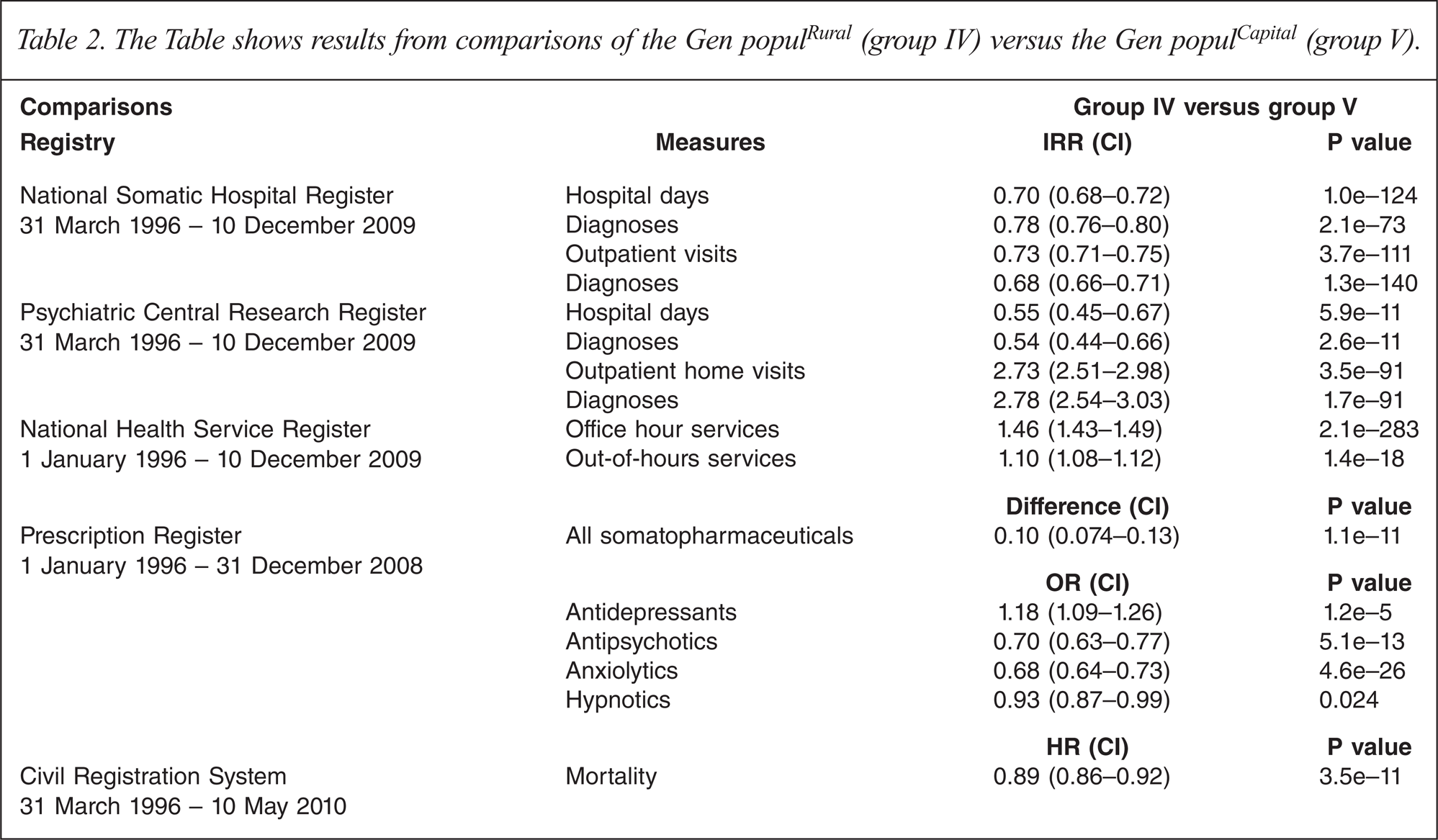
Table 2 shows the results from comparisons of the Gen populRural (group IV) versus the Gen populCapital (group V).
The Table shows results from comparisons of the Gen populRural (group IV) versus the Gen populCapital (group V).
The proportion of individuals that died during the entire study period in groups I, II, III, IV and V were: 100%, 88%, 86%, 87% and 91%. In the five groups the range of natural death was 94.7% to 97.1% with no statistically significant differences between the groups. The hazard rate ratios comparing mortality between groups can be seen in Tables 1 and 2. Survival curves are shown for groups I, II and III in Figure 2 and for groups IV and V in Figure 3.
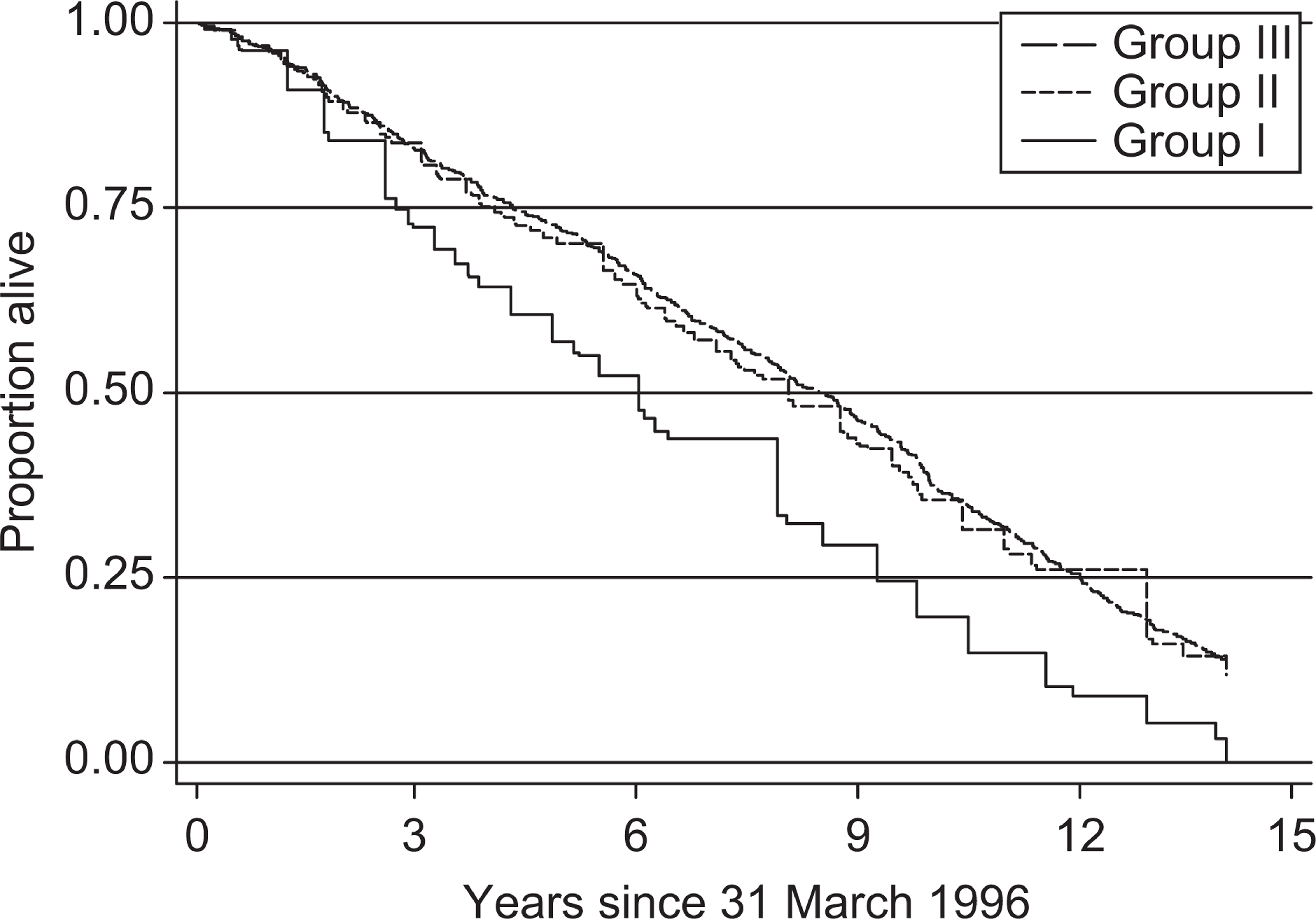
Survival curves for the cohort of frail depressed patients (Group I, Depr cohortMunicipality) (n = 38), the controls (Group II, ControlsMunicipality) (n = 116) and the non-frails (Group III, Non-frails Municipality) (n = 575), all living in the municipality of Sonderhald, adjusted for age and gender. Hazard rate ratios are shown in Table 1.
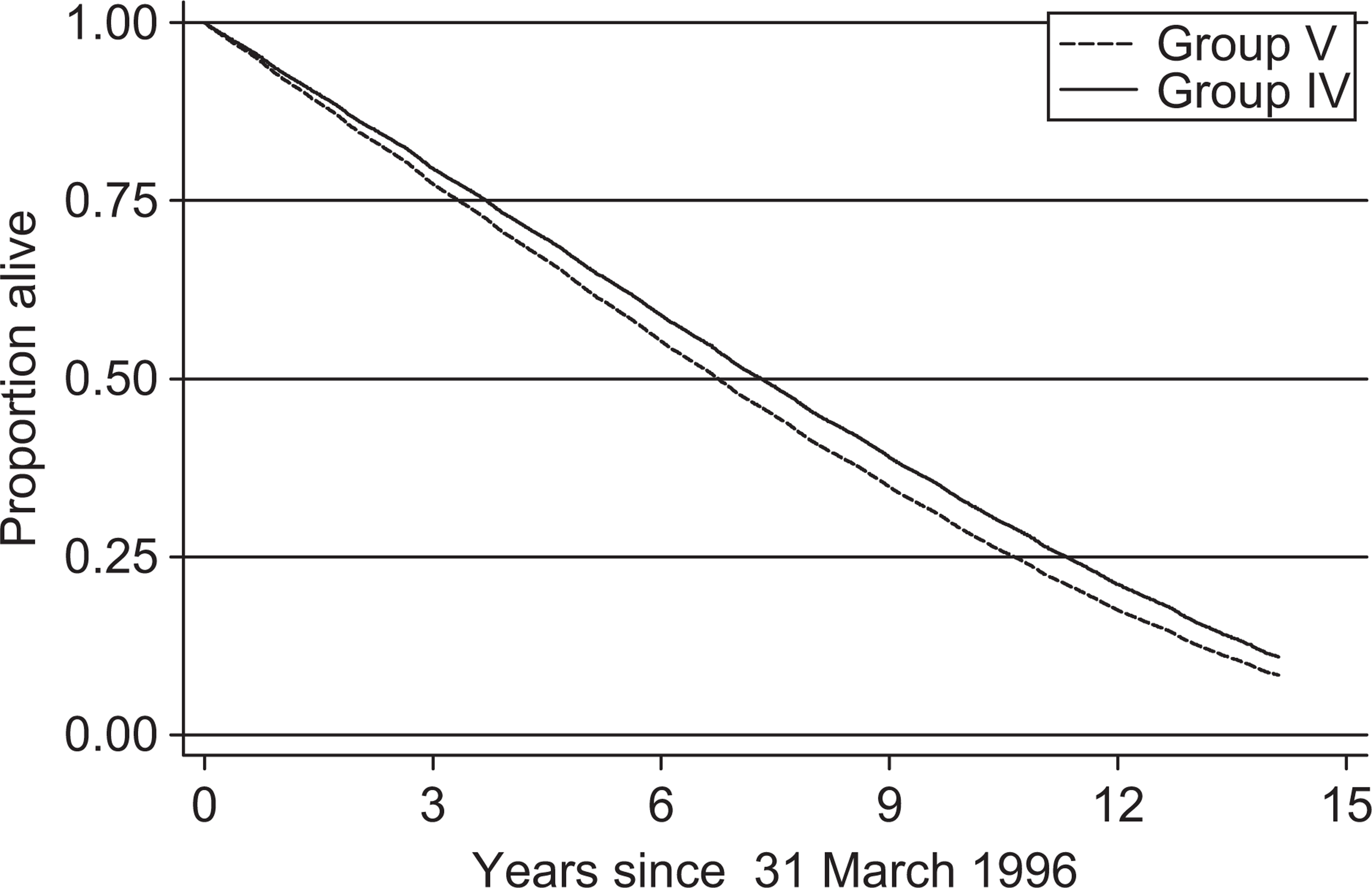
Survival curves for the general elderly rural populations (Group IV,
Discussion
The overall objective of the study was in a register-based design to evaluate whether there were differences in morbidity, mortality and use of health care services as a function of depression, frailty and urban/rural living.
Main results
During follow up the clinically established Depr cohortMunicipality (group I) had significantly larger use of psychiatric hospital days, outpatient home visits, antidepressants, antipsychotics and GP office hours services compared with the ControlsMunicipality (group II) (Table 1). Further, it had more psychiatric diagnoses including larger morbidity. However, there was no increased use of somatic hospital services or more somatic diagnoses. Versus the Gen populRural (group IV), the Gen populCapital (group V) had significantly larger use of somatic hospital services including more somatic diagnoses, psychiatric hospital days including more psychiatric inpatient diagnoses, antipsychotics and anxiolytics, but less psychiatric outpatient diagnoses and less use of psychiatric outpatient home visits, antidepressants, GP services and all somatopharmaceuticals (Table 2).
Similar to the 8 year follow up [32] we observed no significant differences in use of somatic hospital services (Table 1) and number of somatic diagnoses between the Depr cohortMunicipality (group I) and the ControlsMunicipality (group II) in this 13 year follow up and the same results apply to the Depr cohortMunicipality (group I) versus the Non-frailsMunicipality (group III). The results are contrary to other studies showing increased use of somatic services by depressed patients [2–13]. This is seemingly a result of a well-functioning old age psychiatry, intensively as well as extensively focusing on both mental and physical health.
In identical comparison combinations, i.e. the Depr cohortMunicipality versus the ControlsMunicipality and the Non-frailsMunicipality the number of psychiatric diagnoses and use of psychiatric hospital days, outpatient home visits, antidepressants, antipsychotics and GP office hours services (but not out of hours services) were significantly increased. This is in disagreement with other studies showing under-utilization of psychiatric services [1–13,23–26]. One study found limited use of available mental health services among rural elderly Americans with depressive symptoms [29], but the results of the present study indicate that this does not seem to be the case among Danish equals. Seemingly, the reason is the same as mentioned in the last three lines of the above section.
Like in other studies of depressive elderly patients [26–28], hypnotics were more used by the Depr cohortMunicipality versus ControlsMunicipality though not significantly when adjusted for multiple testing.
The risk of death (hazard rate) was significantly higher for the Depr cohortMunicipality both versus the ControlsMunicipality and versus the Non-frailsMunicipality (Table 1). This is in agreement with studies of severe depression [14,17,19–21] and some studies of depressive symptom cases and mild to moderate depression [16–18] but in disagreement with others [14,15].
However, this end point follow-up study of the Depr cohortMunicipality did not come up with new information concerning the measured health characteristics except that the hazard rate for risk of death was much increased (Table 1). This was not the case in the 8-year follow-up after adjustment for multiple testing [32]. Although there were no significant differences in cardiovascular, cerebrovascular and respiratory disorders between the Depr cohortMunicipality and the ControlsMunicipality at baseline [32], the increased mortality rate may be due to comorbid somatic disease [1] even if the Depr cohortMunicipality did not use more somatic hospital days compared with the ControlsMunicipality and the Non-frailsMunicipality. However, the Depr cohortMunicipality did use more GP office hours services and all somatopharmaceuticals (Table 1) versus both ControlsMunicipality and Non-frailsMunicipality (1), which suggests that the Depr cohortMunicipality may have had more somatic disorders/diseases during the follow up and that the GPs mainly treat these patients themselves. However, some of the excess mortality may be caused by the depressive disorder itself.
The much increased use of psychiatric hospital services, especially outpatient home visits, in the present study by the Depr cohortMunicipality versus both the ControlsMunicipality and the Non-frailsMunicipality (Table 1) may be, as we do not know the GP referring pattern prior to this study, a result of the interventions in the municipality (Figure 1) in connection with the study of prevalence of depression among frail elderly rural community-living individuals in 1996 (see Figure 1, group I) [30]. The interventions in continuation of the study targeted both GPs and nursing staff and included lessons on old age psychiatry and presentations and discussions of the results of the study. All participants of the study diagnosed with an ICD-10 depressive disorder or dysthymia were discussed between the patient's GP and the principal investigator (the first author), who worked out a treatment plan to be carried out by the GPs [30].
Overall, the results of the study indicate poor late-life psychiatric outcome of the Depr cohortMunicipality. Somatic morbidity, less use of somatic hospital services and the depressive disorder or dysthymia of the members of the cohort seem to explain increased mortality. However, the study does not allow us to point out the relative importance of each element due to the naturalistic design.
Concerning age ranges of groups I and II (see results, first section) two persons from group I and one from group II were between 69 and 70 years old. This is most likely due to mistakes made during the inclusion process in the prevalence of depression study in 1996 [30].
The frail ControlsMunicipality (group II)'s significantly larger use of all somatopharmaceuticals and GP office hour services versus the Non-frailsMunicipality (group III) (see Results, fourth section) suggests that the frail ControlsMunicipality have more somatic disorders. The fact that the ControlsMunicipality did not have significantly larger use of somatic hospital services suggests that the GPs of the municipality mainly treat their somatic disorders themselves.
The significantly increased mortality in the follow-up period among the register identified populations, Gen populCapital (group V) versus the Gen populRural (group IV) is conspicuous (Table 2). However, if we assume there were no differences in the general health and need of health services between the two populations, the interpretation of the results of the comparisons would be that the Gen populCapital had significant excess use of somatic hospital services including psychiatric hospital days versus the Gen populRural, but used much less psychiatric outpatient home visits and less GP office hours services and out-of-hours services (Table 2). However, the clinical relevance of 10% less use of out-of-hours services is unclear. The Gen populCapital's significantly more somatic and psychiatric inpatient diagnoses (Table 2) during the follow-up does not necessarily reflect poorer general health but may be a consequence of more admissions due to the same disorder(s). However, note that the Gen populCapital had much less psychiatric outpatient home visits and diagnoses versus the Gen populRural (Table 2).
Rather than just larger use of somatic hospital services and psychiatric hospital days, and less use of psychiatric outpatient home visits and especially GP office hours services by the Gen populCapital (Table 2), part of the explanation of the differences in use of the mentioned health services may be insufficient capacity or skills of the central capital municipality home health care services to take over inpatients for post-hospital home-care after discharge. Likewise, there may have been insufficient capacity of the psychiatric outpatient home visit service and GP services. Improved overall health care, i.e. improved access to suitable services, e.g. central capital municipality home health care services and psychiatric outpatient home visits and GP services, may improve the health care of the age group and reduce the need for somatic hospital services and psychiatric hospital days. Alternatively, the general health of the Gen populCapital may be significantly poorer than that of their rural living equals as indicated by the increased mortality; however, the results of the present study do not give an answer to this important question. Searches did not come up with similar studies and so the findings seem to be novel.
The Gen populCapital's significant lower use of somatopharmaceuticals and GP services compared with their rural equals may reflect insufficient treatment of somatic diseases, which may in turn contribute to the increased mortality. However, the clinical significance of 10% less use of all somatopharmaceuticals is unclear. The Gen populCapital's more use of antipsychotics and anxiolytics may be indicated but it still used more psychiatric hospital services except psychiatric outpatient visits. The Gen populCapital's more use of anxiolytics may support the results of other studies showing that elderly people commonly receive inexpedient treatment with anxiolytics [1,27,28]. Compared with rural equals the Gen populCapital used fewer antidepressants (Table 2), which may lead to increased use of psychiatric as well as somatic services. The latter because depression in the elderly often presents with somatic symptoms [43,44]. The Gen populCapital's lower use of antidepressants may even suggest that antidepressants are under-used [1,26–28]. The latter may be due to GP's difficulties with depression diagnostics among elderly patients [1,30,43].
Strengths of the study
The data from the national health registers are prospectively collected and updated within the time-frame of periods; further, the high number of person years regarding the general elderly populations is a strength of the study made possible by the use of the unique Danish health registers. Finally, it was possible to do a follow up of the municipality-living frail depressive patients from index diagnosis till they all had died.
Limitations of the study
The main limitation of the study was the limited number of person years contributed by the municipality-living depressive patients and controls. Data may also be missing in the registries. Overall register data are collected from daily clinical practice, i.e. they have not been collected by means of standardized research criteria.
Summary of results and conclusion
In this study, frail rural community-living depressed elderly patients used more of GP services, psychiatric hospital services, antidepressants and antipsychotics and had increased mortality, indicating poor late-life psychiatric outcome. The results point to the need for a more effective follow-up regime for this patient category, e.g. life-long follow-up by old age psychiatry district service and/or arranged collaborative care models with primary care involving regular follow ups, primarily to effectively observe for recurrence of depressive disorder and to ensure antidepressant medication compliance.
The register-established general population sample of the central capital municipality of Copenhagen showed increased use of somatic hospital in- and outpatient services and inpatient psychiatric services and higher mortality compared with rural equals. This may be due to a composite of poorer general health, insufficient access to outpatient psychiatric home visits, GP services, municipality care services and possibly to some extent due to lower rate of treatment with antidepressants. The results may indicate less sufficient old age psychiatry care in the elderly Gen populCapital in some areas. Thus, the perspectives for future research may be intensified focus on studies of treatment and evaluation of extent and quality of the care for elderly urban populations.
Footnotes
Acknowledgements
We are grateful to Gurli Perto and Søren Skadhede for skilled assistance and valuable discussions concerning the databases.