
Abstract
The suicide attempt rate of the County of Funen, Denmark, was estimated at 185 per 100 000 in 2003 [1]. The rate was fairly constant in the 15 years prior to 2003, whereas the Danish national suicide rate has been decreasing over the past two decades. The suicide rate was 16.6 per 100 000 in 2001 following a decrease of almost 60% since the beginning of the 1980s [2]. Previous self-harm is associated with suicide [3] and individuals with a history of self-harm or suicide attempt form a well-defined high-risk group for suicide. Owens and colleagues [4] systematically reviewed the literature on fatal and non-fatal repetition of self-harm. The probability of repeated self-harm was strongest within the first year after the episode (median: a minimum of 16% repeated within the first year, 21% within 4 years, and 23% within > 4 years). The probability of death by suicide was also strongest within the first year after the episode (median: a minimum of 1.8% committed suicide within the first year, 3% within 4 years, 3.4% within 9 years, and 6.7% within > 9 years). Owens and colleagues found wide variations in suicide rates among different studies [4].
A successful screening for suicide risk in the general population with no previous suicidal behaviour is difficult, because the population is large and indefinable. The prevention of suicide calls for a systematic screening for suicide risk after an episode of self-harm or attempted suicide with a view to informing somatic and psychiatric staff of risk factors, thus enabling the health-care system to offer treatment for suicidal individuals. In order to make the screening successful, it is vital to have knowledge about the characteristics of individuals who repeat the suicide attempt or commit suicide after an episode of self-harm or attempted suicide. The characteristics can be social, demographic, clinical, mental, etc. Some studies have analysed potential risk factors for suicide after an episode of self-harm and found that undetected self-harm or suicide attempt, method used, living alone or not having close relations, alcohol abuse and psychiatric and physical health problems were useful predictors for suicide [5, 6]. This study analysed the potential risk factors on three levels: repetition of suicide attempt, suicide and all deaths, and will include well-known as well as recently discovered risk factors. In this study, we analysed a large population of more than 2500 individuals who have made a suicide attempt.
This study was based on Danish register data, which provided us with an opportunity for precise censoring of individuals who immigrate or die. In so doing, we were able to make a correct estimation of the function of the distribution of repetition of suicide attempt (henceforth this will be called repetition), suicide and deaths. We analysed the risk of repetition, suicide and death following the index attempt (the first registered suicide attempt). We only analysed suicide attempts committed in the County of Funen, Denmark, by individuals living in that county. The risk of these individuals was compared to the risk of a matched control group, which was characterized by members being of the same age, gender and place of residence. Factors relating to the suicide attempt, socio-demographic factors and mental illness were analysed as potential risk factors (non-time dependent and time-dependent factors) for repetition, suicide and death.
Method
We analysed a total sample from The Register for Suicide Attempts [7] of individuals, with an index attempt during the period 1995–2000 inclusive. This resulted in a total of 2614 suicide-attempters. For every suicide-attempter, 15 individuals were identified from the Danish Civil Registration System (CRS), matched by gender, age and place of residence at the day of the suicide attempt [8]. (CRS administrates the personal identification number and personal data on every citizen in Denmark.) Non-attempters were given the date of the index attempt of the attempter to whom they were matched. The date was used as the index date from which survival on any of the outcomes was measured. The matching procedure ensures that, at the day of the suicide attempt, the matched control group was alive and living in the county. It was checked that no one in the matched control group had made a suicide attempt during their period of risk. As we used register data for this, it was not possible to check for suicide attempts that did not result in treatment in somatic or psychiatric departments. No individuals from The Register for Suicide Attempts appeared in the matched control group and no individuals from the matched control group were matched to more than one suicide-attempter. The procedure resulted in a total of 39 210 individuals used for comparison.
In The Register for Suicide Attempts, a suicide attempt is defined as: ‘An act with a non-fatal outcome, in which an individual deliberately initiates a non-habitual behaviour that, without intervention from others, will cause self-harm, or deliberately ingests a substance in excess of the prescribed or generally recognized therapeutic dosage, and which is aimed at realizing changes which the subject desires via the actual or expected physical consequences’.
This definition has been used since the birth of The Register. It is wide and covers almost all kinds of self-harm as long, as the self-harm is aimed at realizing changes. The changes are not necessarily death but can be something else.
The survival distribution function estimates for repetition of suicide attempt, suicide and death was generated by the use of proc Lifetest from SAS on UNIX [9]. A test for homogeneity of survival functions across attempters and non-attempters was completed regarding death and death by suicide by use of a generalized Wilcoxon test. The effect of factors on survival was analysed using Cox's proportional hazards model. The procedure Phreg from SAS proved suitable for analysing the association [9]. The procedure yields an estimate of the hazard ratio and a test for the significance of the estimate. Hazard ratio can be interpreted as relative risk. Phreg is capable of analysing time-dependence covariates. In this study, factors that may change value during the follow-up period are analysed as time-dependence covariates [10]. Individuals were removed from the study if they died or immigrated during the follow-up period.
We found information on repetition during the follow-up period by merging population data with data from the Danish National Patient Register (DNPR) on an individual level using the unique Danish identification number [11]. Individuals with the code of contact cause EUN4 (code of contact cause for suicide/suicide attempt which includes self-mutilation and deliberate self-harm) in DNPR during the follow-up period were coded as repeaters. Practice has taught us that not all suicide attempts are correctly registered with a EUN4 code, and also that some events registered with EUN4 are more related to deliberate self-harm than to suicide attempt [7, 12]. Information on suicide and other reasons for death is found in the national Causes of Death Register [13].
Potential risk factors for repetition, suicide and death were created by merging data from various national registers on an individual level. The registers used were:
The Register for Suicide Attempts [7], which was established in 1989 and contains information on suicide attempts that resulted in a contact with the secondary health-care system in the County of Funen in Denmark. The Demographic Database [14], which contains demographic information on every citizen in Denmark. It has a longitudinal design where individuals can be followed continuously over time. The Danish National Patient Register [15], which contains information on every contact to the secondary health-care system in Denmark. The Causes of Death Register [13], which contains information on time, place and causes of death of individuals who died in Denmark. The Danish Psychiatric Central Register [16], which has been computerized since 1969 and covers all psychiatric inpatient facilities in Denmark. The Register of Medicinal Product Statistics [17], which contains information on prescription drugs prescribed for an individual. The database has information on all medical drugs bought on prescription after 1995. The Integrated Database for Labour Market Research [18], which links individuals with companies, providing longitudinal information on labour market conditions. The Centralized Civil Register [19], which was established in 1968 as a national civil register with the purpose of administrating the personal identification number system as well as general personal data.
Potential risk factors were categorized into the following domains: demographic characteristics, circumstances of the index attempt, occupation, level of education, substance abuse, treatment of mental illness, and factors related to social circumstances. Some factors were analysed as non-time-dependence covariates on the day of the index attempt, and others as time-dependence covariates, which can change value during the follow-up period. The results of the forward and backward selection were analysed in order to create a list of factors that make up the adjusted analysis. The factor ‘no link to parent’ was used to control for missing links to a parent and is therefore included in every analysis of factors relating to parents. Younger people were more likely to have a link to a parent because of the structure and age of the registers. No link to a parent is therefore highly correlated with age.
Results
The 41 824 participants were followed throughout 1995–2001. The gender distribution for attempters was 1076 (41.16%) males and 1538 (58.84%) females. The age distribution of the attempter participants ranged from 15 to 90 years with a median of 37 years. Gender and age distribution of the non-attempters were the same owing to the matching procedure. The primary methods applied in the suicide attempt act were: 2022 (77.35%) medical drugs, 51 (1.95%) other substance for poisoning, 80 (3.06%) hanging or drowning, 384 (14.69%) gas, cutting or stabbing, 27 (1.03%) jumping from high places or in front of traffic, and 50 (1.91%) used another method.
Attempters were compared to non-attempters in relation to death by suicide and all deaths. Table 1 is a summary of the analysis for attempters and non-attempters. The analysis for suicide and all deaths rejected the hypothesis that the survival function for attempters and non-attempters was generated from the same survival function distribution.
Summary of survival analysis for repeated suicide attempts and mortality for attempters and non-attempters
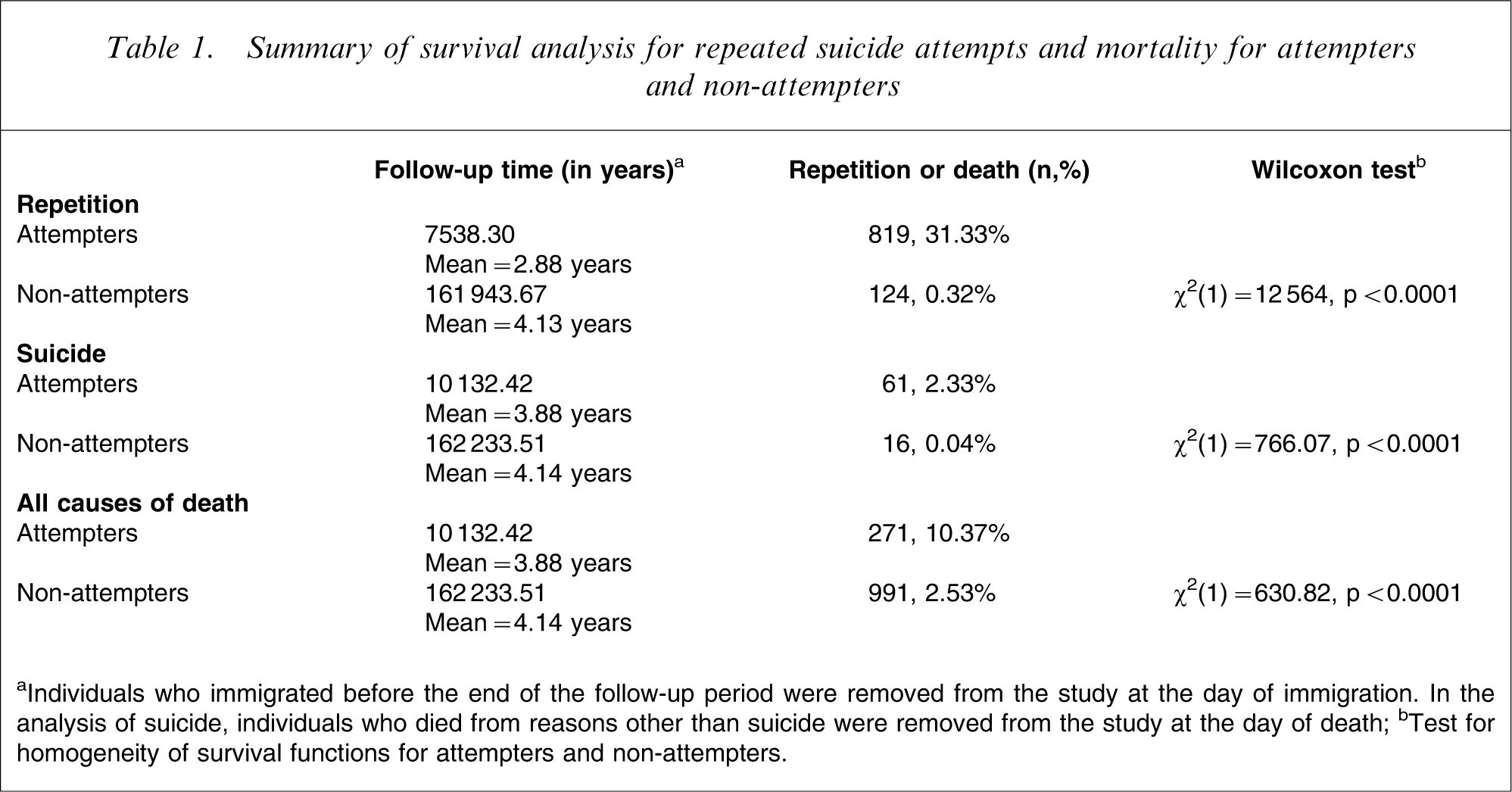
aIndividuals who immigrated before the end of the follow-up period were removed from the study at the day of immigration. In the analysis of suicide, individuals who died from reasons other than suicide were removed from the study at the day of death; bTest for homogeneity of survival functions for attempters and non-attempters.
The estimate of the function of the distribution of repetition, suicide and death for attempters and non-attempters is displayed in Figure 1. The probability of attempters repeating the suicide attempt within 2000 days (5.5 years) is approximately 37.34%. The probability of attempters repeating the suicide attempt is strongest immediately after the first registered suicide attempt, but after approximately 2 years it is reduced and remains constant for the rest of the follow-up period.
The estimate of the function of the distribution of repetition, suicide and death for attempters and non-attempters.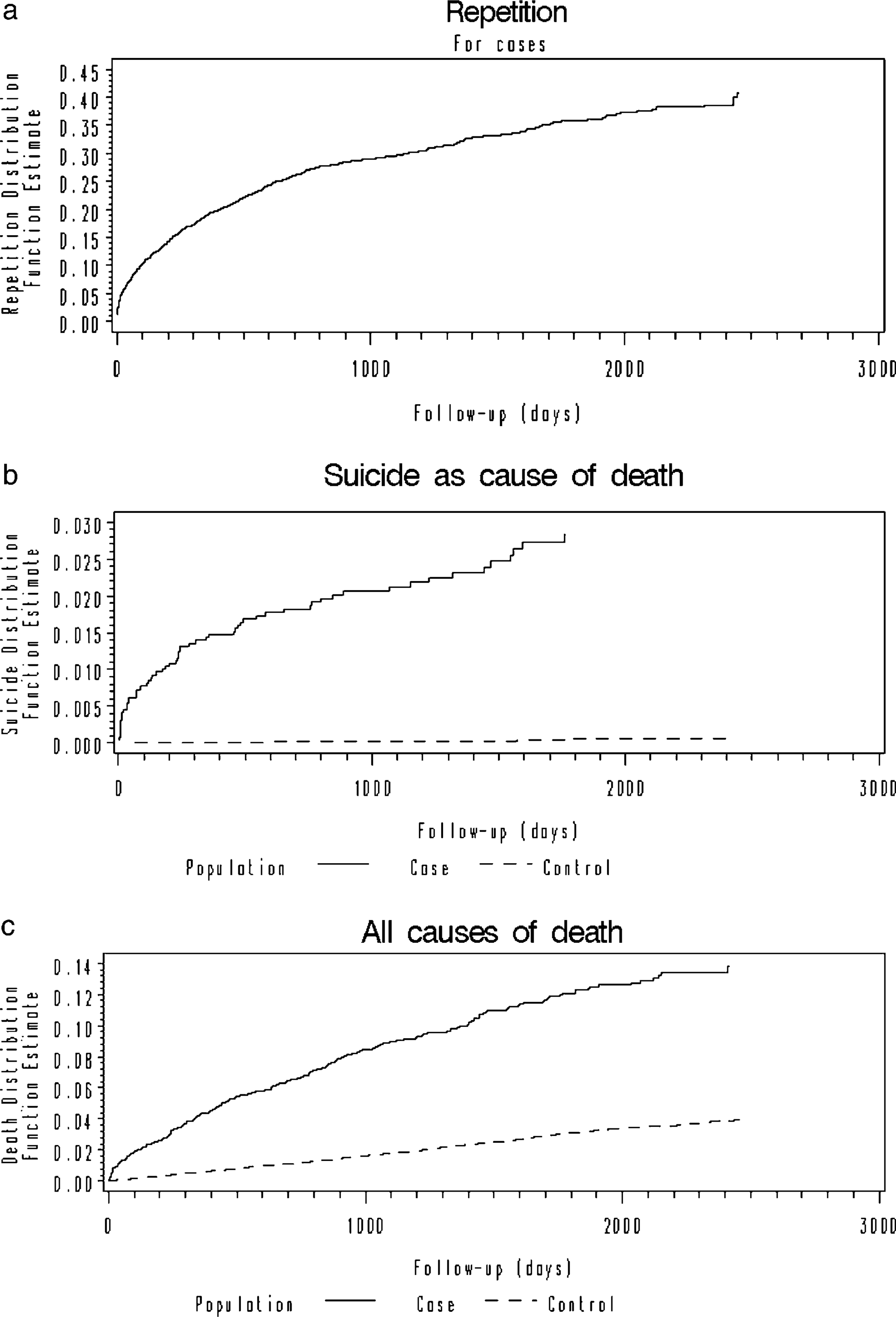
The probability of death by suicide within 1750 days (4.75 years) is approximately 60 times stronger for attempters than non-attempters, and the probability of death within 2000 days (5.5 years) is approximately four times stronger for attempters than non-attempters. When excluding suicides from the analysis, attempters are approximately three times more likely to die than are non-attempters within the follow-up period. Suicide is also more likely to occur shortly after the suicide attempt, which places the period immediately after the index attempt as the highest risk period for repetition and suicide. Death occurs more constantly across the follow-up period for attempters than for non-attempters.
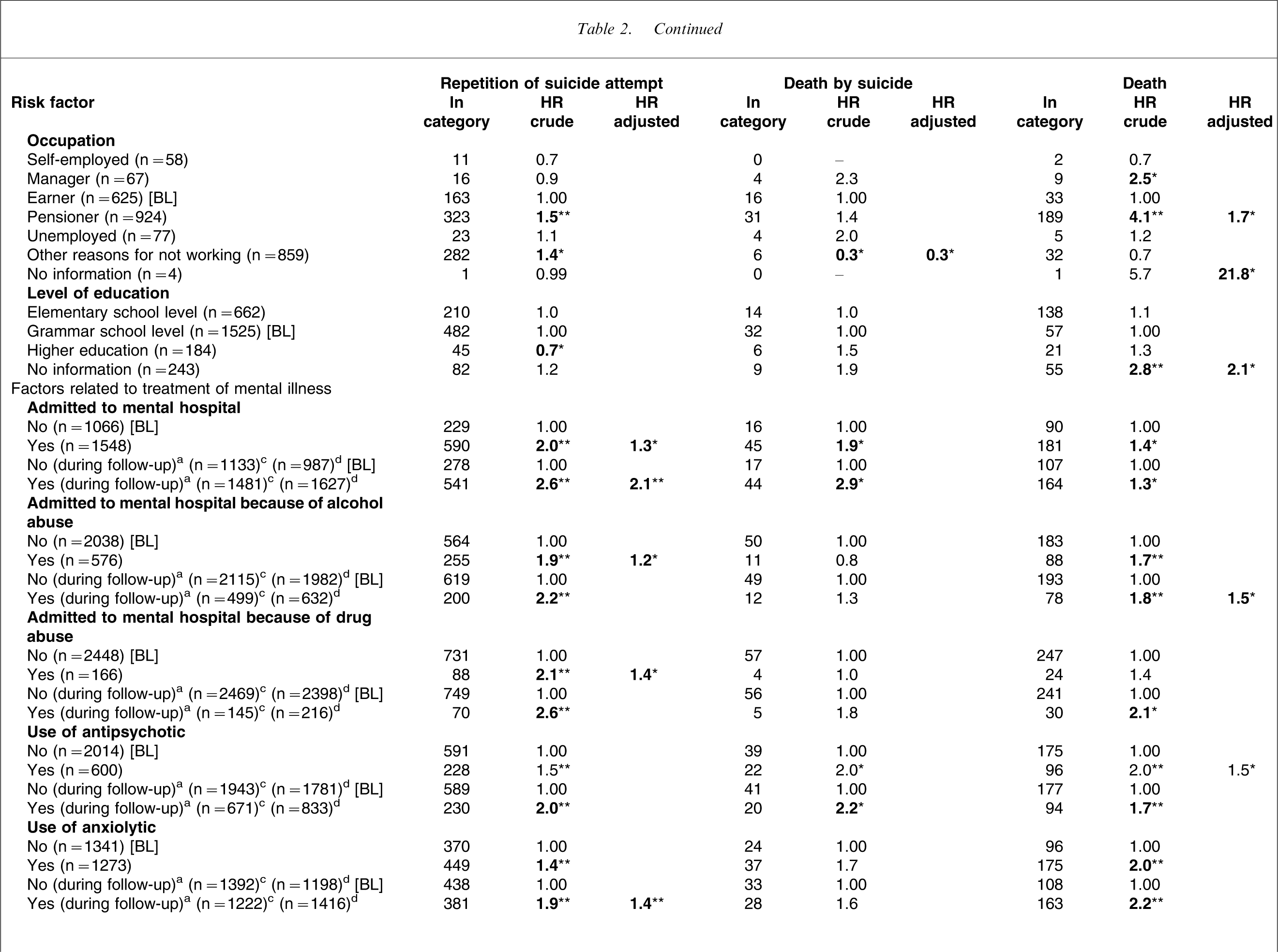
Repetition was positively associated with gas, cutting or stabbing, being male, young or middle-aged, living alone, certain types of occupation, low level of education, admission to a psychiatric department (before and during the follow-up period), psychopharmacological drugs (before and during the follow-up period; Table 2). In the adjusted analysis, only method, age and psychiatric morbidity were significant risk factors for repetition (Table 2).
Hazards ratio (HR) for risk factors for repetition of suicide attempt, suicide and death. Crude and adjustedb model
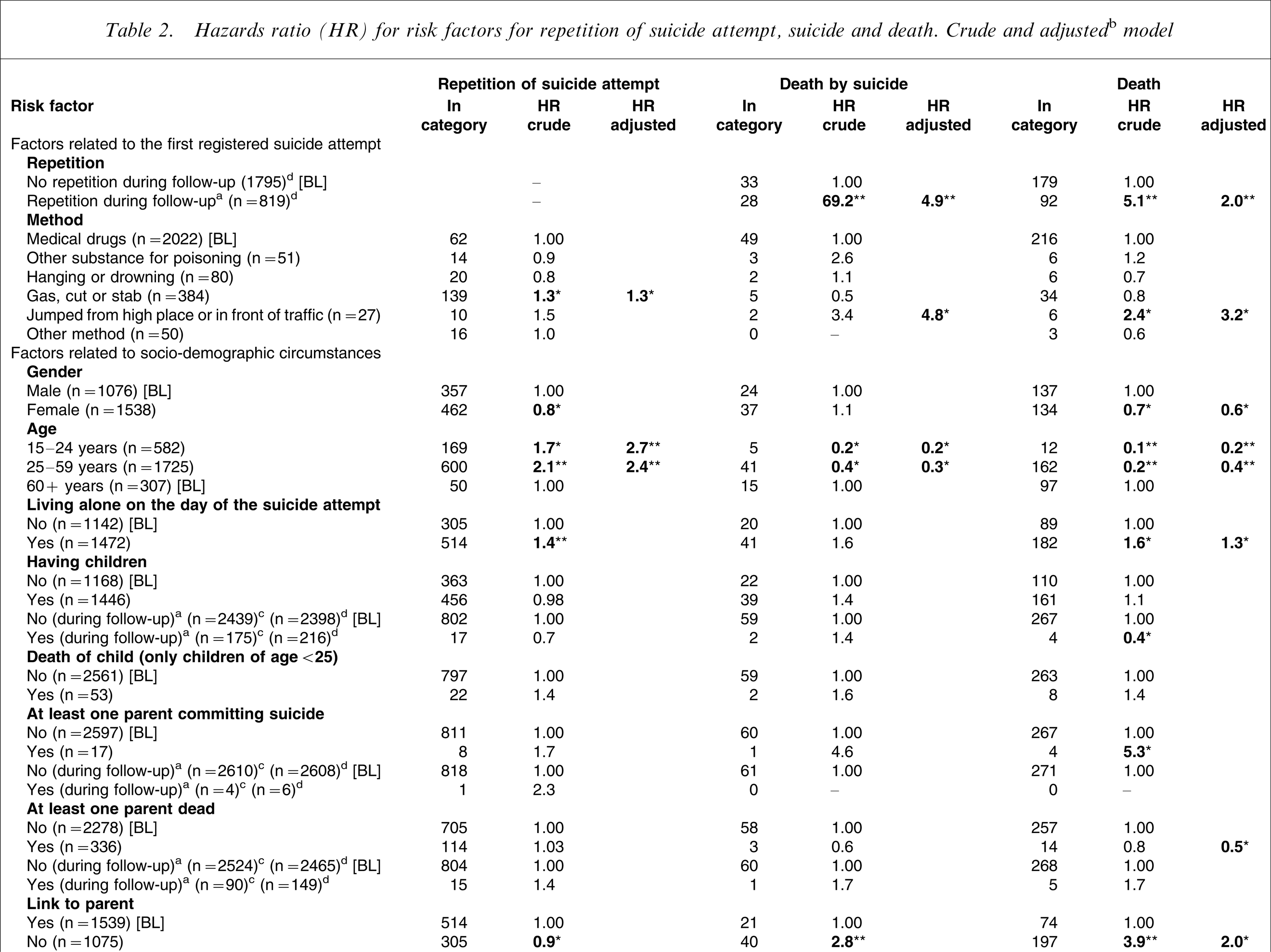
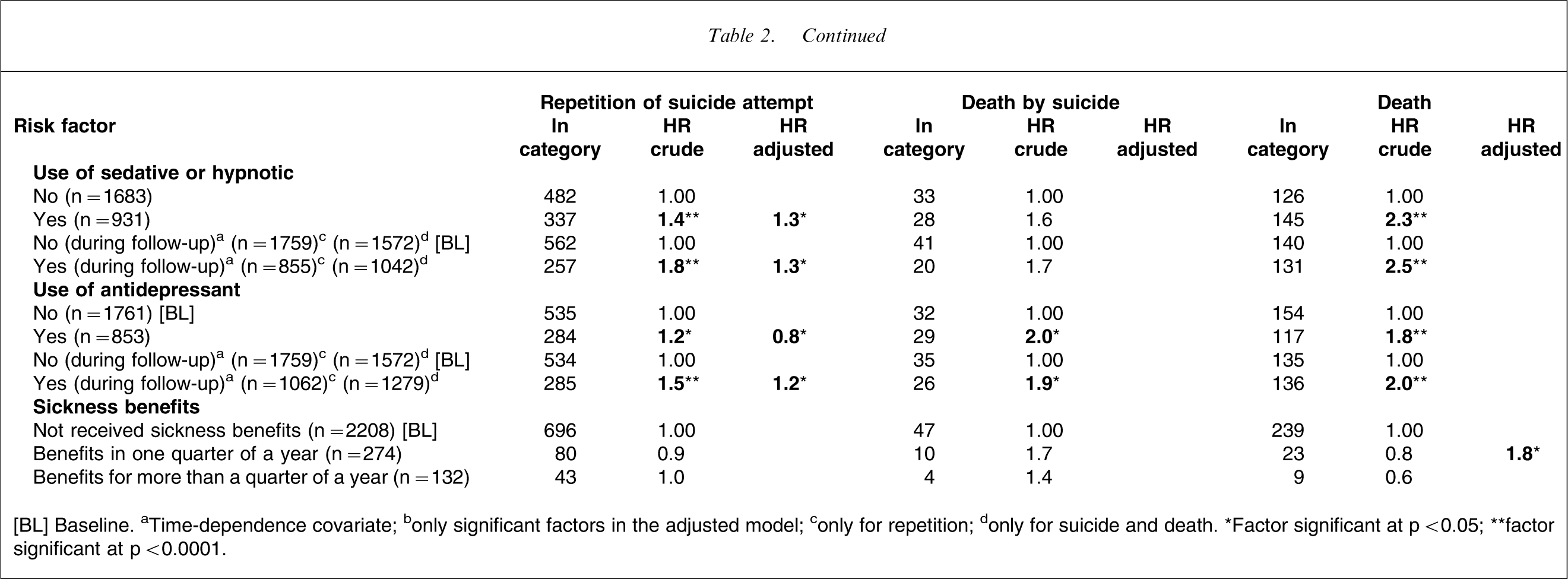
[BL] Baseline. aTime-dependence covariate; bonly significant factors in the adjusted model; conly for repetition; donly for suicide and death. ∗Factor significant at p < 0.05; ∗∗factor significant at p < 0.0001.
Suicide was positively associated with repetition, being 60 years of age or older, admission to a psychiatric department (before and during follow-up), antipsychotic drugs (before and during follow-up), antidepressant drugs (before and during follow-up). Other psychopharmacological drugs were weakly associated with suicide (Table 2). In the adjusted analysis, only repetition, method, age and occupation were significant risk factors for suicide following a suicide attempt (Table 2).
Death was positively associated with repetition, jumping from high places or in front of traffic, being male, 60 years of age or older, living alone, parent having committed suicide, being a manager or retirement pensioner, admission to a psychiatric department (before and during follow-up), admission to a psychiatric department because of alcohol abuse (before and during follow-up), admission to a psychiatric department during the follow-up period because of drug abuse, all kinds of psychopharmacological drugs (before and during follow-up; Table 2). In the adjusted analysis, significant factors were repetition, method, age, being male, living alone, being a retirement pensioner, alcohol abuse (during the follow-up period), antipsychotic drugs, sickness benefits, and death of parents (Table 2).
Discussion
In this study, we analysed a population of 2614 individuals who had made a suicide attempt and a large control group. The size of the population made way for a good estimation of risk. A comparison of risk for attempters with the risk for the general population was not made. Instead, a comparison was made with a matched control group, which was characterized by members having the same age and gender distribution. The merging of longitudinal administrative databases on an individual level provided us with an excellent opportunity for a proper censoring procedure [20]. A wide range of factors were analysed, which allowed for an estimation of predictors for repetition or mortality. It also allowed for the adjusting of effects of other factors, which was done in the adjusted analysis.
The creation of the covariate was limited by the information on the longitudinal administrative databases. Therefore, it was not possible to analyse information such as: did he/she leave a suicide note, what was the provoking factor, did he/she avoid discovery, the degree of hopelessness or impulsiveness, and other important factors. Still, we found predictors that helped us characterize individuals who repeated their suicide attempt or who committed suicide after a suicide attempt. The Register for Suicide Attempts only contains information on suicide attempts in the County of Funen, Denmark, committed by people living in that county. Consequently, the analysis only included people living in that catchment area. The catchment area contains approximately 8.5% of the Danish population and is in many ways representative of the entire nation.
The attempter population was a well-defined high-risk group for repetition, suicide and premature death. The risk was significantly higher for attempters than for non-attempters. Other studies have found similar results [4, 5]. Suicidal behaviour is positively associated with mental illness [21, 22], and mortality is high for individuals who suffer from mental illness [23]. This can explain the high mortality for suicide-attempters. Mortality may also be high for suicide-attempters as they can be more impulsive and take more risks [24, 25]. This may result in death by accidents more often [26]. The risk of repetition and suicide is highest in the period immediately after the index attempt. The suicidal behaviour of an individual is therefore more likely to be clustered in time [4, 27]. The risk of suicidal behaviour is often associated with crisis, negative and stressful life events, and is therefore more likely to be non-constant over time.
Elderly individuals are more likely to die from natural causes, but also by suicide [28], whereas this study shows that younger individuals are more likely to repeat their attempt. Corcoran and colleagues [27] found that males aged 30–39 years were more likely to repeat an attempt within 1 year compared to other males. They found no difference in the age-specific repetition risk for females. Repetition of suicide attempt and mortality after suicide attempt in this study are very positively associated with factors that relate to treatment of mental illness. Mental illness is therefore among the best predictors for repetition and suicide. Cooper and colleagues and others found identical results [5, 6]. Hospitalization in a psychiatric department and the use of psychopharmacological drugs during the follow-up period are both categorized as treatment for mental illness and are therefore, paradoxically, to be found as risk factors. The factors may be indicative of severe mental illness and therefore figure as risk factors. The method used in the index attempt can, to some degree, predict repetition, suicide and death, especially gas, cutting, stabbing, jumping from a high place or in front of traffic. The method used may reflect the intention, and therefore the more violent the method used the higher the wish to die. This can increase the probability of repetition or suicide, if the suicide wish was not met in the first attempt.
It is difficult to predict suicide after an episode of attempted suicide. After controlling for other factors only three factors: age, method and repetition can predict suicide. Repetition is probably the best predictor for suicide after an attempt. Nordentoft et al. found similar results [26], but Owens et al. did not find the same connection [6]. Owens and colleagues adjusted previous self-poisoning for other factors, and it became a significant protective factor for suicide. They accounted for the finding by means of the fact that previous self-poisoning was strongly related to having seen a psychiatrist, and adjusting for this might explain the discrepancy. We, too, adjust repetition for psychiatric treatment, but it still figures as a significant risk factor. The finding of Owens and colleagues [6] may be owing to the small number of suicides during the follow-up period and to methodical and study design problems. They neither analysed the first registered self-poisoning nor the factors as time-dependent covariates. We conclude that individuals who use violent methods or repeat near-fatal suicide attempts form a high risk group for suicide. Clinicians can use this information to spot individuals who are at high risk of committing suicide.
In the crude analysis, living alone at the day of the index attempt is a risk factor for repetition and death, and it is on the verge of being a significant risk factor for suicide. Others found similar results [5, 26]. Individuals living alone may lack social support when going through a crisis, but living alone can also cover up mental illness or be the result of a break-up of a relationship. Living alone is only a risk factor for death in the adjusted analysis. This indicates that living alone has some correlation with other factors in the analysis of subsequent suicidal behaviour. Being a pensioner is associated with repetition and death. The reasons for being a pensioner include old age, or mental or somatic illness. After adjusting for other factors, being a pensioner became insignificant for repetition, which correlates with other factors.
This and other studies demonstrate that mortality (including suicide) is very high for individuals who have survived an episode of attempted suicide. The studies also show that the risk of repetition is highest in the period just after the suicide attempt, and that repetition is positively associated with subsequent suicide. This knowledge is vital in the work of preventing repetition and suicide, and it is therefore important that individuals who attempt suicide are given treatment immediately after the episode. Some factors are associated with subsequent suicidal behaviour, especially mental illness, method used and age. This information is very useful when trying to predict subsequent suicidal behaviour. In order to be given the right treatment, an individual who had a suicide attempt should always be seen by a psychiatrist to be screened for mental illnesses. Individuals who are living alone are at risk for subsequent suicidal behaviour. They may lack social support, and it is therefore central that the staff in somatic care encourage the suicidal person to include significant others in the treatment. The staff in somatic or psychiatric care should be well informed about the high-risk behaviour that can be brought about by an episode of deliberate self-harm or attempted suicide. Furthermore, departments that are in contact with suicidal individuals must have action plans to ensure that all such individuals who are discharged receive proper treatment as soon as possible.
Research in this field should focus on predictors for suicide after an episode of self-harm or attempted suicide. The information can help clinicians determine the risk of subsequent suicidal behaviour. Large cohort studies, with a careful selection of important potential risk factors analysed by Cox's proportional hazards model with time-dependent covariates, will be helpful. Today, it is possible, within a limited time frame, to analyse for many factors in a large population with the aid of computer power and software solutions.