
Abstract
Psychotic disorders, particularly schizophrenia, are typically prolonged and often result in considerable disability and economic burden [1–4]. It is recognized as the third leading cause of disability-adjusted life years lost according to the World Health Organization's World Health Report 2001. International studies on early detection and intervention of first episode psychosis suggest that provision of comprehensive integrated treatment can reduce treatment delay (duration of untreated psychosis) of the first psychotic episode and may improve the outcome [5–10]. In fact, over the last decade, early intervention of psychosis has grown to become a mainstream and well-funded approach to clinical practice [9]. Indeed, international consensus statements were established providing guidance on strategies for development of the early intervention service for psychosis [11].
Hong Kong has a population of just over 7 million. Local psychiatric services are provided mainly by the government-subsidized public health-care system. The organization governing the public health-care system is the Hospital Authority (HA). In view of the rapid expansion of the early intervention paradigm, a new service initiative, namely the Early Assessment Service for Young People with Early Psychosis (EASY), was developed by a psychiatric central coordinating committee of HA in 2001. The aim of EASY was to implement early detection and intensive phase-specific intervention of first episode psychosis [12,13] in Hong Kong. It is a territory-wide service providing two-year specific psychiatric care to patients aged between 15 and 25 with first episode psychosis. Initial evaluation of this service has shown that patients with shorter durations of untreated psychosis have better treatment adherence and earlier treatment response one year following first presentation [14]. The three year outcome evaluation comparing EASY with standard care services showed that patients receiving EASY service had lower hospitalization rates and better functional outcomes [15], indicating the effectiveness of this new service.
With scarcity of resources and competing demands, evidence indicating an intervention is effective is not enough to support the implementation of a service. In recent years, economic evaluation of service, whereby costs and outcomes are viewed simultaneously, has become increasingly important as an evidence of a programme's value among mental health services [16,17]. This is particularly important for policy planners given the early intervention model for psychosis has gradually become accepted as part of the mainstream clinical approach for service delivery internationally.
One of the first evaluations on the cost-effectiveness of the early intervention service compared with that of standard care originated from the Early Psychosis Prevention and Intervention Centre (EPPIC) in Australia [18]. They compared one year outcomes of 51 patients receiving early intervention service with 51 matched retrospective controls under the pre-treatment model. Cost measures were limited to health service, whereas outcome measures were focused on the quality of life and negative symptoms. They adopted cost-effective analysis using cost for unit improvement of clinical outcomes as the comparison variable. Early intervention service was found to cost less than standard care. Another study designed by a Swedish group looked at treatment costs and clinical outcomes at three years, comparing 61 first episode schizophrenia patients with both prospective and historical control counterparts [19]. They found that patients who received specialized service had significantly better functioning at three year follow up compared to those with standard care service; and it also cost significantly less in the first year for those receiving specialized service. Most recently, a study from a London group compared the cost-effectiveness of the early intervention service with the standard care [20]. This randomized control study followed 144 patients for 18 months. Outcome measures focused on quality of life and vocational recovery. Cost-effectiveness was assessed using a net benefit approach with bootstrapping regression model and a public sector perspective was adopted for cost calculations. It was shown in this study that the early intervention service had a higher likelihood of being cost-effective. Other studies found that there was a reduction of hospital costs after introducing early intervention services [21,22]. However, evidence on cost-effectiveness of early intervention service specific for psychosis are still limited and mostly restricted to the western community. Given this research gap, we aimed to examine the cost-effectiveness of the EASY service.
Methods
Treatment models
EASY
EASY is a specialized multi-disciplinary service programme, which was established in 2001 in Hong Kong to provide early detection and intervention services for young people aged 15 to 25 with first episode psychosis. The programme consists of public education facilitating early detection of the illness and comprehensive intervention targeting the specific needs of patients using case management approach. It is a publicly funded special service covering the whole territory. The service was divided into four units in 2001 and each unit was responsible for looking after patients of a specific geographical region. A full description of this programme is provided elsewhere [12,13]. The objectives were to reduce delays in initial treatment, to provide specific intervention to young people with early psychosis and their families, and to improve the overall outcomes of the patients. Each patient under this service would receive care for two years. For this study, patients were recruited from one of the four newly developed EASY service units; the Department of Psychiatry, Queen Mary Hospital (QMH).
Pre-EASY (standard care)
The comparator of the current study is the standard care model (described below as ‘pre-EASY’). It is a publicly funded general psychiatric service with inpatient and outpatient service and community support services covering the whole territory. This service was available to all patients who were eligible to receive publicly funded psychiatric care. It is a model prior to the inception of EASY (i.e. 1999–2000). Patients of standard care were recruited from the same unit as the EASY patients, namely the Department of Psychiatry of QMH, hence covering the same catchment area.
Subjects
A retrospective historical control design was adopted in the current study. A sample of 65 young people with first episode psychosis was randomly selected and recruited from the first 200 patients who presented to the EASY service of the Psychiatric Department of QMH in Hong Kong between 2001 and 2002. The selected EASY sample was individually matched (on age, gender and diagnosis) with 65 patients receiving pre-EASY service from the same hospital between 1999 and 2000. Comparisons were made between these two samples and a retrospective cost-effectiveness analysis was conducted for a period of 24 months, the duration for which patients received care from the EASY service.
Cost measurement
The economic evaluation in this study focused mainly on the direct service utilization cost defined as the actual dollar expenditure on the provision of the mental health service by the public sector. The direct costs associated with other non-government or non-mental-health services were not included. Indirect costs were not included. The service utilization data was obtained using the Clinical Data Analysis and Reporting System (CDARS), a territory-wide retrospective decision support system, which aims at providing value-added clinical information for management decision, clinical audit and research. Developed by the Information System Department of the HA, CDARS captures clinical data from all public mental health services in Hong Kong and provides the most accurate and reliable sources of information on inpatient, outpatient, medication and Accident and Emergency service utilization in Hong Kong. The cost-estimation strategy involved computing direct service utilization costs for each patient across the 24 month follow-up period and then aggregating within each group to compute costs per patient. A one-off start up lump sum payment to the EASY service was excluded as it did not reflect an ongoing running cost of the service.
The financial year of 2001–2002 was chosen as the time period from which the financial data were retrospectively collected and analysed. The unit cost provided by the HA Finance Department in 2001–2002 was used in cost estimation for both samples. Hence, the costs of the two intervention models were evaluated as if the two patient groups were treated concurrently with two different services. That is, the 2001–2002 costing formulae were applied to the 1999–2000 pre-EASY data. In this connection, no discounting was made for the analysis. ‘Contact’ and/or ‘service unit’ used was defined as face-to-face contact between a clinician and a patient and/or family members. Duration of contact was not included in this evaluation. Cost data collected were further categorized into four areas as follows:
Inpatient utilization
This was measured as number of bed days of each patient being admitted to the inpatient unit of QMH. The mean unit cost for each inpatient bed day was estimated based on a specialist costing formula provided by the Finance Department of Hospital Authority. The mean unit cost of each inpatient bed day in QMH in 2001–2002 was HK$2955 per day.
Specialized outpatient clinic
The number of outpatient contacts of each patient during the 24 month follow-up period was counted. Again, the unit cost was estimated on the basis of the psychiatric specialist costing method provided by the Finance Department of Hospital Authority. The average unit cost for each outpatient contact at the QMH psychiatric clinic was HK$704.
Medication utilization
The average cost of medication per patient was derived by adding all of the costs of prescribed medications of each group and dividing this by the total number of patients in the cohort.
Other professional service utilization
In addition to regular outpatient follow up, a number of other psychiatric services offered in various professional settings including those of social workers, clinical psychologists and community psychiatric nurses, as well as visits to emergency departments were also included in cost estimation. The unit cost of each service was obtained using the government's Controlling Officer's Report in 2001–2002 (http://www.budget.gov.hk/2002/eng/eframe4.htm) which provided the unit cost of each professional contact.
Based on the above direct service utilization estimate, the total cost of each group of patients was computed. The average cost per patient from each intervention model was then calculated by dividing the total cost with the total number of patients in each group.
Outcome measure
The total number of psychiatric inpatient admissions was used as a primary outcome of this study. Additionally, psychopathology of patients was selected as the secondary outcome measure and was measured with the Positive and Negative Syndrome Scale (PANSS) [23]. It is a 30-item, 7-point psychopathology rating instrument, which represents increasing levels of psychopathology from 1 (absent) to 7 (extreme). Of the 30 items, seven of them constitute a positive symptom scale, another seven items as a negative symptom scale and the remaining 16 items as a general psychopathology scale. The PANSS is scored by summation of ratings across items, such that the potential ranges are 7–49 for both the positive and negative symptom scales and 16–112 for the general psychopathology scale. PANSS scores of patients from the two groups were collected by the patients’ medical officers at baseline and at the end of the 24 month follow-up period. The items were scored according to standardized instructions based on clinical interviews. The samples of the Pre-EASY and EASY groups were selected from the same centre at two different periods, with the same clinicians working at the centre during both periods. PANSS scores of patients in the pre-EASY group were collected through clinical interviews as part of a different study on first episode psychosis carried out by the Department of Psychiatry of the University of Hong Kong. The same clinician then worked at the EASY service when it was started, and conducted the PANSS. The intra-class correlation coefficients were 0.83 for PANSS positive subscale and 0.73 for the PANSS negative subscale. The change in PANSS scores of each patient between the two time points was used as the effectiveness measure.
Cost-effectiveness
Cost-effectiveness analysis was suggested to be one of the most appropriate methods for combining cost and outcome data [24], and was used as the form of economic evaluation in the current study. In this study we assessed cost-effectiveness by calculating incremental cost-effectiveness ratios (ICER), which measured the difference in average costs between the two groups divided by the difference in average effects. In the primary analysis we explored cost-effectiveness in terms of psychiatric inpatient admissions. In the secondary analyses we explored the cost per unit improvement in PANSS over the 24 month follow-up period. It was computed by dividing the total cost of treatment by the change in PANSS score between the baseline and 24 month follow up. Estimates of cost-effectiveness are inevitably associated with some degree of uncertainty, generated jointly from the estimates of effectiveness and costs [25]. To address the issue of uncertainty in the costs and effects associated with specific intervention, we used non-parametric bootstrapping to generate a distribution of mean costs and effects for the two treatments (1000 iterations generated by Microsoft Excel). On the basis of this bootstrap analysis, a scatter plot of simulated incremental cost and effect pairs on the incremental cost-effectiveness plan was constructed. The bootstrap distributions were also used to plot a cost-effectiveness acceptability curve. The curve showed the probability where the EASY model is cost-effective compared with the pre-EASY approach for a range of maximum monetary values that a decision maker might be willing to pay for a reduction of psychiatric inpatient episode [25]. For the secondary analysis, cost per point improvement in PANSS with sensitivity analysis was calculated.
Statistical analysis
All statistical analyses were performed using SPSS (version 16.0) for Windows. Chi-square tests were used for categorical data comparisons, and t-tests were used for continuous data comparisons. As stated above, bootstrapping analysis was used to study the cost-effectiveness in reducing hospitalization.
Results
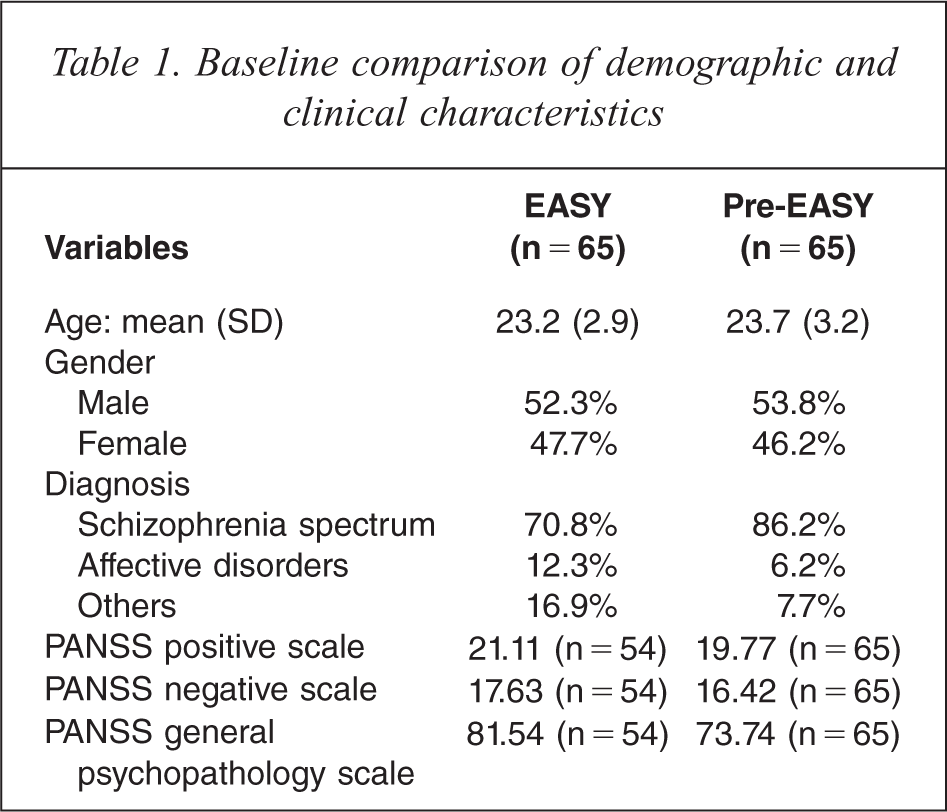
The demographic and clinical diagnosis of patients in each group are reported in Table 1; no significant difference was found in any of the variables (Table 1). The average cost of the pre-EASY standard care model was HK$152 740 per patient whereas the average cost of the EASY model was HK$112 830 per patient. Although the cost of the two models was not significantly different (t = − 1.365; df = 128; p = 0.175), the overall average per patient cost of the EASY service was 26.1% less than that of the pre-EASY service.
Baseline comparison of demographic and clinical characteristics
When studying the cost of specific services (Table 2), EASY patients utilized significantly more psychiatric outpatient contacts and had higher medication expenditures. It was estimated that the average medication cost for an individual EASY patient was HK$7542, whereas it was HK$231 for each pre-EASY patient (t = 5.56, df = 128, p < 0.01). This was because more atypical antipsychotic medication was prescribed in the EASY service. Based on the clinical data, 60% of patients with the EASY service were prescribed atypical antipsychotics as opposed to only 9.2% with the pre-EASY group (χ2 = 44.84; df = 1; p < 0.01). Though the difference in the cost of inpatient service utilization between the two groups was not statistically significant, patients managed in the EASY service utilized 31.6% less inpatient psychiatric service.
Cost Analysis of EASY and pre-EASY service
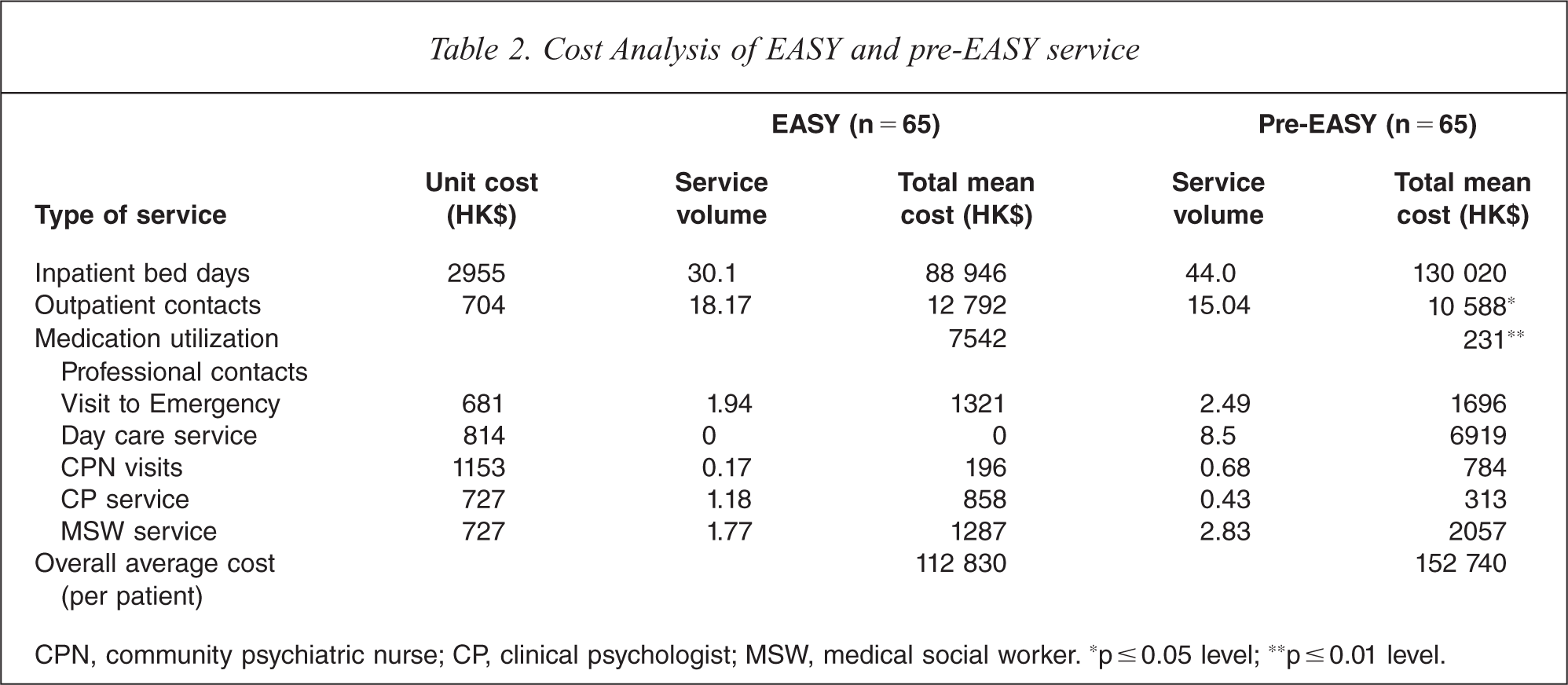
CPN, community psychiatric nurse; CP, clinical psychologist; MSW, medical social worker. *p ≤ 0.05 level; **p ≤ 0.01 level.
Outcomes
Table 3 gives the outcomes for the two groups on psychiatric inpatient admissions and PANSS subscales scores. The average mean psychiatric inpatient admission of the EASY group was significantly less than that of the pre-EASY group (0.78 versus 1.58; t = −3.46; df = 128; p < 0.01). For psychiatric symptoms, the EASY group consistently had superior subscales scores at the 24 month follow up. A statistically significant difference was found in PANSS negative subscale scores between the groups (t = −3.19; df = 86; p = 0.002).
Outcomes of the two groups at 24-month follow-up
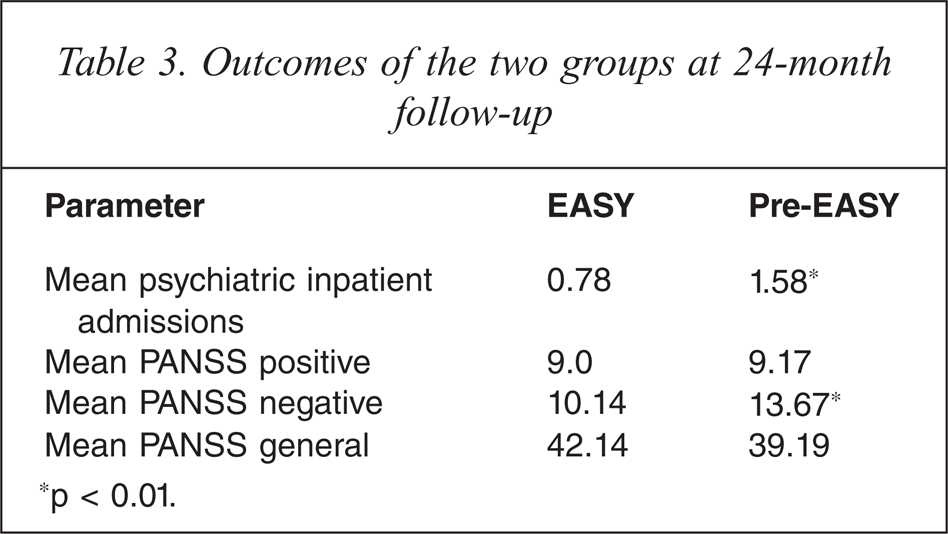
*p < 0.01.
Cost-effectiveness
The incremental cost-effectiveness ratio for psychiatric inpatient admissions over the 24 month follow-up period was HK$49 888 per unit reduction in psychiatric inpatient admissions. To address the issue of uncertainty in cost-effectiveness estimation, an incremental cost-effectiveness plane was constructed to illustrate the bootstrapping incremental cost and incremental effect (Figure 1). Since the majority of the ICER pairs fell in the south-east quadrant of the incremental cost-effectiveness plane, indicating that EASY was less costly and more effective than the pre-EASY group, EASY was considered to be dominant. Figure 2 shows the cost-effectiveness acceptability curve associated with the reduction of psychiatric inpatient admissions. The curve indicates the probability of EASY model being more cost-effective than the pre-EASY service for a range of potential maximum amounts (ceiling ratio) that decision makers are willing to pay for a unit reduction in psychiatric inpatient admissions. The curve shows that the EASY model is superior to the pre-EASY service over the full range of values of the ceiling ratio plotted. The curve shows that there is at least a 94.4% probability that the EASY model is more cost-effective than the standard pre-EASY model in reducing psychiatric inpatient admissions (ranging from 94.4% to 99.8%).
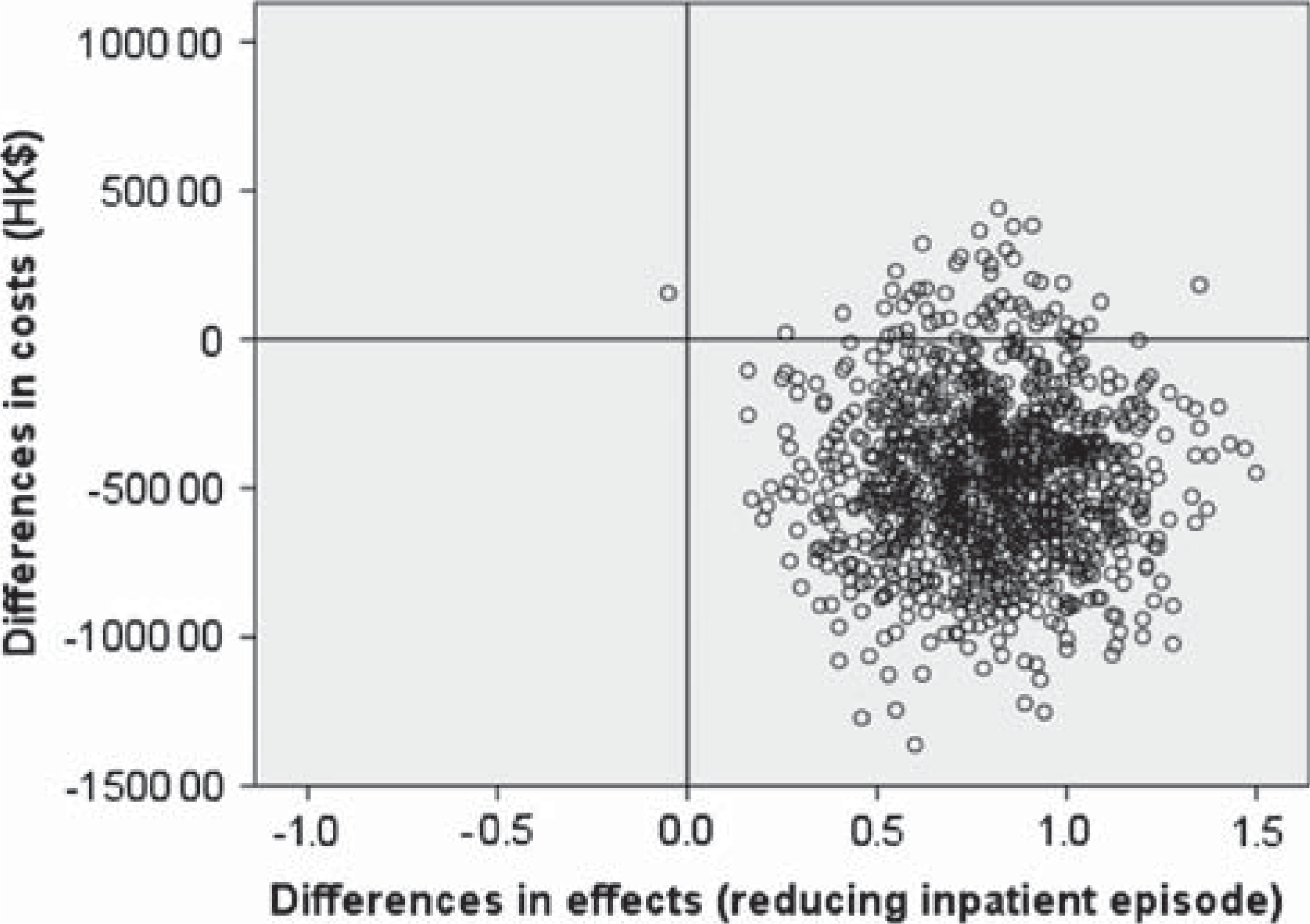
Scatter plot showing the bootstrapping mean differences in incremental costs and incremental effects (reducing inpatient episodes) of EASY versus pre-EASY groups.
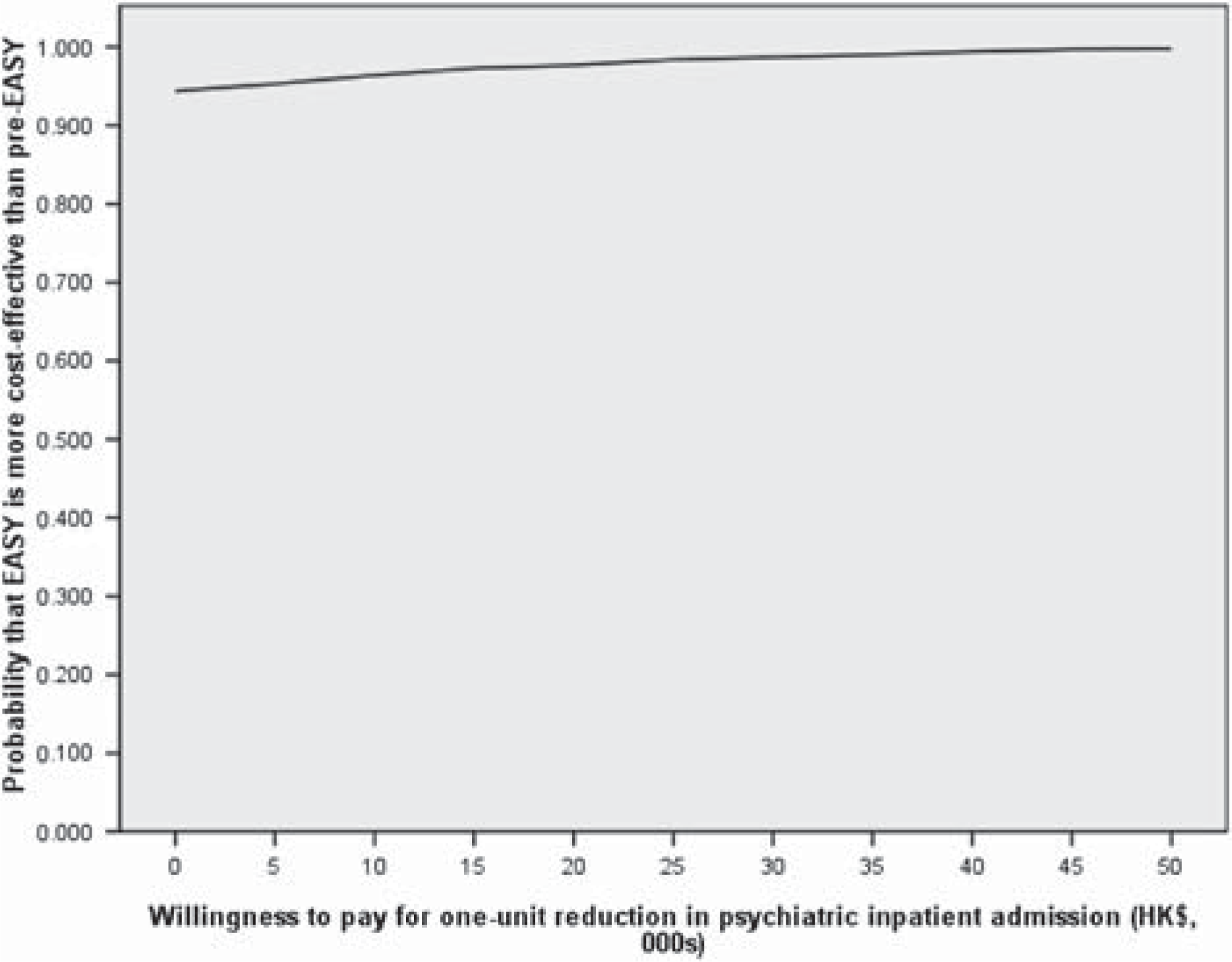
Cost-effectiveness acceptability curve showing probability that EASY is more cost-effective than pre-EASY at reducing inpatient admission over a range of values for the maximum acceptable ceiling ratio.
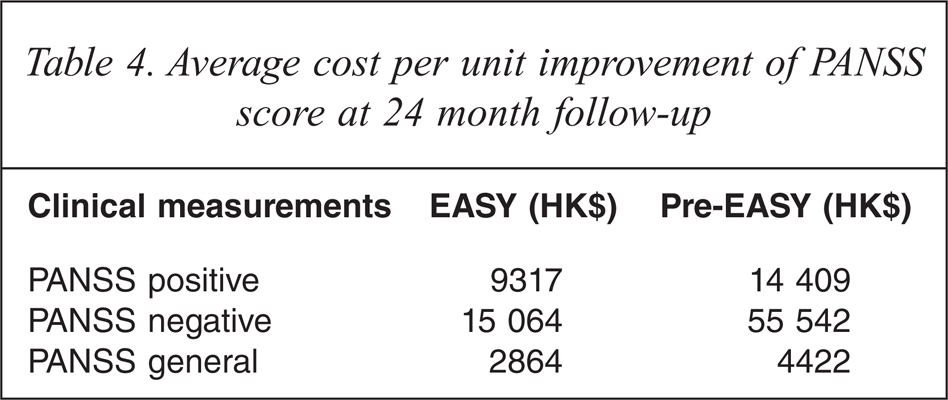
It is also evident that cost per point improvement in PANSS was considerably less for EASY patients than that for the pre-EASY patient sample. Per one point improvement on the PANSS positive scale, the EASY model of treatment offered a 35% savings as compared to the pre-EASY model. The savings of the EASY model per one point improvement on the PANSS negative and general psychopathology scales were 73% and 35% respectively (Table 4).
Average cost per unit improvement of PANSS score at 24 month follow-up
Sensitivity analyses were also performed on these results [26]. It was found that the results obtained using the PANSS as the outcome measure were robust to variations in both cost and outcome parameters. A 15% increase in the costs of EASY, combined with a 15% decrease in the costs of the pre-EASY group, left the EASY model less costly per one point improvement in the positive (12.5% cheaper), negative (63.3% cheaper) and general PANSS (12.4% cheaper) respectively.
Discussion
This study found that the early intervention service for first episode psychosis in Hong Kong (EASY) reduced psychiatric inpatient admissions and improved the clinical outcome, particularly negative symptoms, of young patients with first episode psychosis combined with a lower total service cost. The increase in outpatient care and medication costs associated with the EASY service was substantially offset by the reduction in the costs of inpatient care. This pattern of cost-effective enhancement of early intervention for young people with early psychosis has been reported in other studies from different regions [18,19,27]. Although direct service utilization costs between the two groups using point estimates did not reveal significant differences, exploration of the uncertainty surrounding the estimates of costs and effects suggests that EASY is a dominant option. There is at least 94.4% probability that EASY is a more cost-effective model than the standard pre-EASY service for reducing psychiatric inpatient admissions, irrespective of the amount a decision maker may be willing to pay for such reduction.
Clinically, patients with the EASY service had significant improvement in negative symptoms at 24 month follow up and saved 73% per one point improvement compared to their counterpart. This economic benefit of the EASY service persists with the sensitivity analysis indicating that the EASY service is likely to be more cost-effective in improving clinical symptoms compared to standard care. In fact, this pattern of intervention outcome of specialized early intervention services has been shown in other studies [28]. The economic evaluation of early intervention service in Australia has shown similar findings. The new service is 91% cheaper for one point improvement in negative symptoms compared with standard care [18].
The economic appraisal of this study focused mainly on the direct cost of public mental health utilization. All the service utilization information was collected from the computerized central registration to avoid recall bias. However, the cost of other health-care services, particularly primary health care, was not captured. This is mainly because the private sector is the main provider for primary health care in Hong Kong and the variation of costing makes it difficult to estimate the cost with reasonable accuracy. Other hidden, indirect and societal costs such as services provided by other community sectors that might have influenced the cost estimate were not included. We did not account for the differential timing of costs associated with two periods of the study with one year difference. These factors may influence the accuracy of costing. This is one of the main limitations of the study.
A second limitation of this study is that the design involved historical rather than concurrent controls and it was not a randomized design. However, there were relatively few changes in the overall mental health service system between the two linked periods. Additionally, a randomized control trial is relatively difficult to conduct in this particular setting as the EASY service was started as a territory-wide service with extensive public education about psychosis. In fact, various methodologies were used in the studies of cost-effectiveness of the early intervention service in other regions. The Australian group used matched historical control group design for the study of long-term cost-effectiveness of the early intervention service [29] and prospective historical control group for short-term (one year) comparison [18]. The evaluation of the Swedish early intervention service used both historical control and concurrent control groups [19]. In England, both historical control [21] and randomized controlled methodology [20] have been used.
Thirdly, the primary outcome of this study used was hospitalization, which is also a cost and makes it less straight-forward to interpret the result of cost-effectiveness study. Therefore clinical outcomes were used as a secondary outcome. Ideally, a wider perspective of outcomes, such as quality of life and functioning should be included. In fact, various studies have demonstrated that specialized early intervention services were more effective in improving functional outcomes and reducing family burden [8,28,30–32]. The inclusion of these outcomes in the evaluation of cost-effectiveness of the services could provide a more comprehensive economic evaluation. Another limitation of this study is the relatively small sample size and the difficulties in completing 24 month assessments for all patients. Finally, the follow up period of the current study is the inital 24 months of the establishment of EASY service model in Hong Kong. The outcomes may reflect a transitional state of the service development. It has been demonstrated recently that the early intervention service is more cost-effective than standard care at 8 year follow up [29].
Nevertheless, this study provides initial evidence that early detection and intervention programmes provided by the EASY model, with a shift in the pattern of care from higher cost inpatient care to lower cost community-based outpatient services, offer an economically viable approach to treating young people with first episode psychosis during the first two years in Hong Kong. This forms an important initial reference for policy makers for mental health services, particularly from an Asian perspective. However, further studies with a longer follow-up period, inclusion of other aspects of outcome and cost evaluations, and larger sample groups are needed to verify these initial findings.
Footnotes
Acknowledgements
This work was supported by a research grant from the Research Grants Council, Hong Kong (FEP grant) and the Early Assessment Service for Young People with First-episode Psychosis Programme (EASY) in Hong Kong. The authors alone are responsible for the content and writing of the paper.