
Abstract
Early intervention programmes stress the importance of the intensive treatment of the first psychotic episode in order to optimize recovery, reduce the risk of relapse and prevent the worst outcomes of comorbidity, namely depression, substance abuse and vocational disruption [1–4]. Therefore the protocols of care in early intervention in psychosis emphasize the need to detect the first episode at its very onset, and encourage earlier effective help seeking, with the aim of reducing or preventing secondary morbidity and improving symptomatic and functional outcomes [5], [6]. Evidence is growing for the fact that most cognitive changes, particularly those more likely to last over time and affect social functioning negatively, take place early in the illness before the first hospitalization, and possibly before a frank episode of psychosis is detected [7–9]. Early detection of evolving symptoms is therefore advisable to prevent the worst outcomes of the disorder [10], [11].
In Italy, reform law 180 enforced in 1978 brought about a substantial change in the architecture of the mental health system [12], [13]. The setting up of a comprehensive and integrated system of community-based mental health services [14] resulted in an environment that should be particularly favourable for the detection and the early enrolment of psychotic-onset patients and of all those in need of treatment among the people at risk or showing prodromal signs of psychosis.
Since the gradual closure of all mental hospitals, as established by the aforementioned reform law, in Italy (60 million inhabitants) mental health care is provided by a network of public and private facilities organized into 211 departments of mental health (MHDs) and 23 university psychiatric clinics (UPCs). This network of mental health services includes 262 general hospital psychiatric units (GHPUs), 707 community mental health centres (CMHCs), 16 of them operating 24 h per day (24 h CMHCs), 612 day centres (DCs) and 309 day hospital units (DHUs) [15], [16]. At present Italian public facilities offer 4108 beds (mean size: 12.8±5.3 beds), with 0.78 beds per 10 000 inhabitants. Fifty-four private inpatient facilities (with a total of 4862 beds, mean size: 90±48.2 beds) are also operating, with 0.94 beds per 10 000 inhabitants: they are not allowed to admit patients compulsorily [14], [17].
This organization enhances the visibility of and accessibility to mental health services, and decreases the stigma associated with the diagnosis of mental disorders; it has been effective in increasing mental health service utilization by part of those in need for treatment. In the first 10 years of application first-contact rates have grown robustly for both schizophrenia and affective psychoses, as well as for non-psychotic disorders [18]. Hospitalization, however, remains the first contact with the mental health system for a large fraction of patients with psychoses, and their admission is often compulsory [19], [20].
Despite this profound reorganization of mental health care, implemented in Italy in the past 30 years, the area of early intervention in psychosis has not been very active compared to other European [21–23], and non-European countries [6], [24–27].
In Italy the only specific and comprehensive programme targeted at the early detection of and early interventions for subjects at onset, or showing prodromal signs of psychosis was set up in Milan in 1999 (Programma 2000), after 2 years of preliminary study and organization. The service has been very active since and at the time of writing (spring (April) 2008); >300 young patients have been evaluated.
The aim of the present paper was to review the structure and the organization of Programma 2000, providing details on the activities and results of this service that is entering its 10th year of activity.
Methods
Staff and organization
Following 2 years of extensive study of the existing international experiences – and their relevant structures and organization – Programma 2000 was established in 1999 by the Health Authority of a catchment area of inner Milan (Italy), the Niguarda Ca’ Granda General Hospital, which serves approximately 200 000 inhabitants.
The services offered to the people in need for psychiatric treatment in this catchment area are two GHPUs with 18 beds each (total = 36 beds), two CMHCs, two DCs, a residential facility with 20 places and a five-bed supported apartment.
Programma 2000 was set up in 1999 in a dedicated CMHC created for the purpose of treating young people aged 17–30 years at their first episode of psychosis, or showing prodromal signs of it [28], [29]. The service is located in a city park, to limit all the stigmatizing elements that could lower the appeal of the structure for its young users and their families; it has 10 rooms for assessment, therapy, and group or social interventions.
The team is led by a senior psychiatrist (AC), who is supported by a clinical psychologist (AM) in coordinating all the clinical and scientific activities of the project, and it now includes four psychiatrists on a rotational scheme (1 day per week), four part-time clinical psychologists, a part-time statistician, a vocational educator, a nurse, a variable number of psychologists in training (on average 7–8 at a time), and finally a secretary.
Assistance is offered 9 h per day, 5 days per week, throughout the year. Criteria of enrolment are (i) age 17–30 years; and (ii) first contact with any mental health service of the catchment area for a first episode of psychosis (with duration of untreated psychosis (DUP) ≤ 24 months), or assessed as being at high risk of psychosis.
To facilitate enrolment, in 2002 the referral was extended to other catchment areas of Milan and its suburbs, whenever active participation in the programme was deemed feasible. The service also accepts self-referrals.
Assessment procedures
All patients referred for evaluation to Programma 2000 undergo a comprehensive, multidimensional evaluation, which includes the following standardized assessment instruments (the time interval for each administration is given in parentheses): (i) a sociodemographic form (only at baseline); (ii) the Early Recognition Inventory Retrospective Assessment of Symptoms (ERIraos) [30], a 17-item screening checklist intended to select subjects needing a more in-depth assessment (every 6 months); (iii) the Health of the Nation Outcome Scale (HoNOS) [31], which is used to assess psychopathology and disability; it includes 12 5-point items to evaluate clinical and social functioning in the previous 2 weeks (every 6 months); (iv) the 24-item Brief Psychiatric Rating Scale (BPRS) [32], [33], to assess general psychopathology (every 6 months); (v) the Cognitive Behavioural Assessment 2.0 (CBA) [34], a set of 10 self-report scales aimed at measuring personality traits, neurotic symptoms, somatization, anxiety, depression (every 6 months); (vi) the Camberwell Family Interview (CFI) [35], a semi-structured interview to assess the family's emotional climate (every year); (vii) the Disability Assessment Schedule (DAS) [36], 24 items to evaluate disabilities in social and role functioning (every year); (viii) the Global Assessment of Functioning (GAF) [37] (every year); (ix) the Satisfaction Profile [38] (every year); and (x) a comprehensive set of instruments to assess cognitive functioning (every year) [39]. Further details elsewhere [28], [29].
Criteria for inclusion
The first episode is diagnosed according to both ICD-10 and DSM-IV criteria for schizophrenia [40], [41]. Patients with affective psychosis are not enrolled; also a comorbid persistent substance-use dependent disorder is an exclusion criterion, while substance use/abuse without dependence is not.
Signs of incumbent distress are considered to screen out the patients at risk of psychosis: unusual content of thought, reduced attention and/or concentration, symptoms of anxiety, depression, suspicion, are considered for inclusion whenever they are associated with marked social withdrawal and/or severe impairment in social role functioning. Final inclusion, however, is made only when the ERIraos scores are ≥12, and when positive symptoms are present on the BPRS and/or HoNOS – even if in attenuated form – or, alternatively, when symptoms lead to a diagnosis of schizotypal personality. People with recognized risk factors for psychosis, such as a family history of psychosis, or use/abuse of psychotogenic substances (cannabis, amphetamine, cocaine), or documented pre-/perinatal complications in their obstetric records, are also included when they meet the main requirements, that is, ERIraos ≥ 12, and attenuated positive symptoms on the BPRS and/or HoNOS, or a diagnosis of schizotypal personality.
Exclusion criteria for high-risk patients are a staff-confirmed past or current diagnosis of psychosis in the spectrum of schizophrenia or affective disorders. Diagnoses of any anxiety disorder or of personality disorder, or of alcohol and/or substance abuse are not exclusion criteria when the main requirements are met.
Intervention package
All the patients enrolled in Programma 2000 receive an individual intervention package that takes into account the patient's wishes and needs: for each patient a thorough team discussion is made and a comprehensive and flexible intervention package is proposed, based on the assessment results.
Proposed interventions include individual informative and motivational sessions, medication (if necessary), cognitive behavioural therapy (CBT), individual and family psychoeducation and support, therapeutic group activities (e.g. anxiety management, social problem solving, assertive training, substance abuse prevention etc.), various social group activities (e.g. musical group, multimedia group, computer training sessions, language courses, empowerment group etc.), individual employment support, intensive and personalized school support, medication group support, and planning of recreational activities and so on.
All interventions are regularly discussed and reviewed with each patient on a regular basis, and modified if necessary [28], [29].
All these interventions are free of charge for the patients and are financed by a special grant of the Lombardy Regional Authority.
Statistical analyses
Data were analysed using SPSS for Windows, version 11 (SPSS, Chicago, IL, USA). All data were analysed using non-parametric statistics due to non-normality. As for duration of untreated illness (DUI) and DUP, because their distribution is highly skewed [42] we performed an additional transformation into reciprocal values (1/DUI; 1/DUP), as is advisable for measures of duration.
To evaluate the effects of treatment using the total score of the BPRS, a percent change score is frequently calculated by subtracting the pre-specified treatment outcome score from the baseline score, dividing this figure by the baseline score, and multiplying this value by 100, as in this formula: percent change = ((BPRS1–BPRS2)/BPRS1)×100. As in past studies, the cut-off to define responders on the BPRS was set at 20% [43].
As for measures of outcome, according to the Remission in Schizophrenia Working Group a patient was considered in remission at 1 year when he/she scored mild or better (BPRS ≤ 3) on all seven items of BPRS simultaneously, representing the core symptoms of psychosis: grandiosity, suspiciousness, unusual thought content, hallucinatory behaviour, conceptual disorganization, mannerism/posturing, blunted affect [44], [45].
Results
A total of 315 subjects have been referred to the service since its foundation (available data are from January 1999 to December 2007). Referrals were compatible with the enrolment criteria for 289 subjects: among these, 33 were evaluated and then referred back to the service that had asked for the evaluation because these patients were living in other regions of Italy. A total of 147 subjects were offered a dedicated protocol of care: 132 accepted and were enrolled in the programme, 15 refused. The rejected subjects (n = 109) were either not in their first episode, having a DUP > 24 months (n = 47), or were evaluated as not being at high risk of psychosis (n = 62). The rejected subjects and those who refused treatment received appropriate advice for future treatment.
In the past 2 years (2006/2007) the programme has received 60 referrals per year on average, with 20 subjects enrolled per year (on average 12 in the first-episode, and eight in the high-risk group).
Table 1 summarizes the main characteristics of the sample evaluated as being in need of treatment at the time of their first assessment (data available for 143 subjects out of 147): 72% of the sample were male with a lower age at entry than female subjects, in both the first-episode and the high-risk groups (although the difference was not statistically significant due to low statistical power).
Baseline characteristics of patients enrolled in Programma2000 since its beginning (1999)
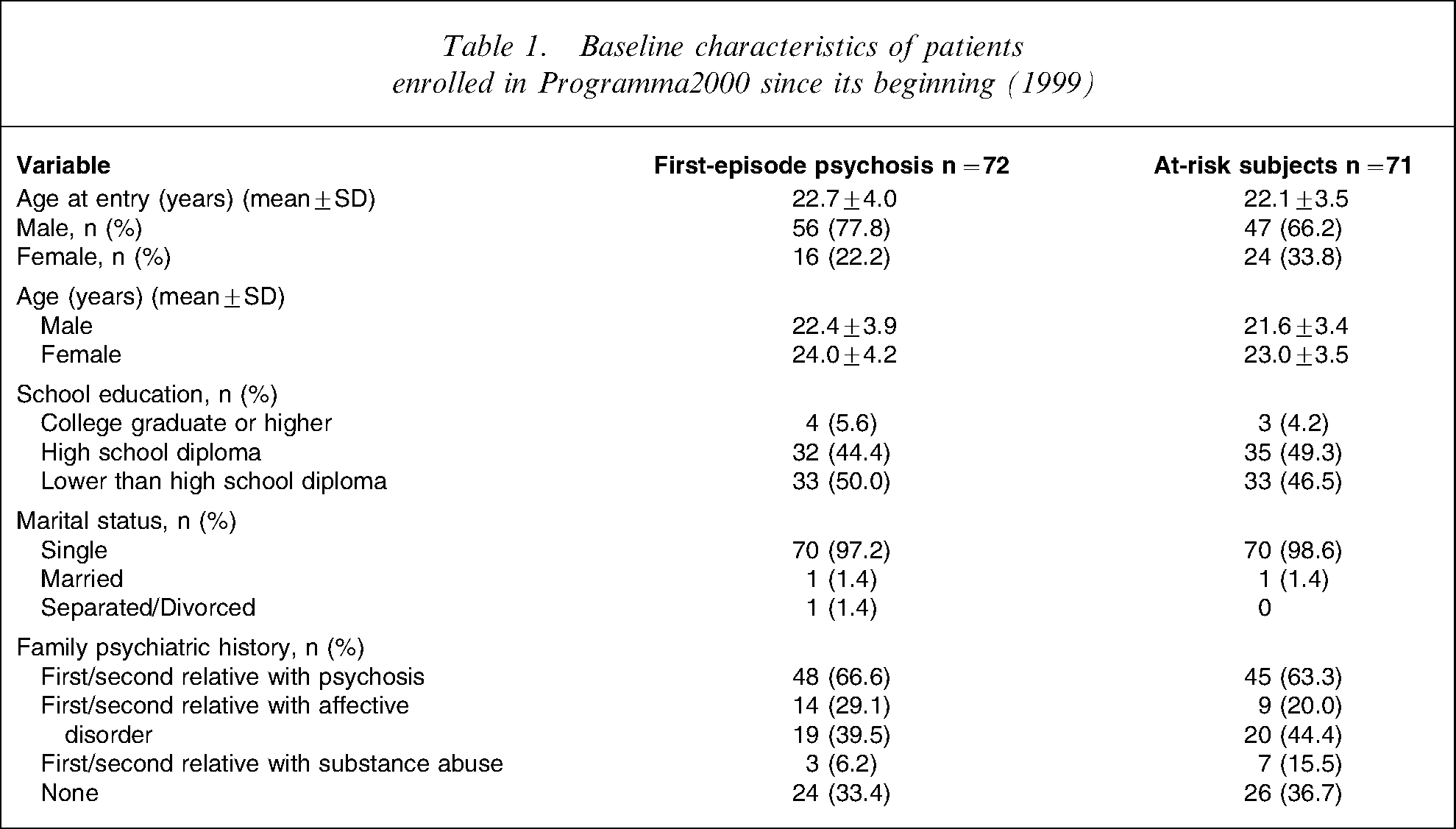
Family history for mental disorders was high in both groups: approximately two-thirds of patients had a first or second relative diagnosed with a mental disorder, namely alcohol and/or substance abuse (6% among those with first-episode psychosis, and 15% among at-risk subjects), schizophrenia-like psychosis (29% among those with first-episode psychosis, and 20% among at-risk subjects), or affective disorders (around 40% in both samples).
Symptom profile at entry
Approximately 40% of the referrals (50% among those with first-episode psychosis) were already in treatment for psychological problems when referred to the service (Table 2).
Clinical characteristics of patients enrolled in Programma2000 since its beginning (1999)
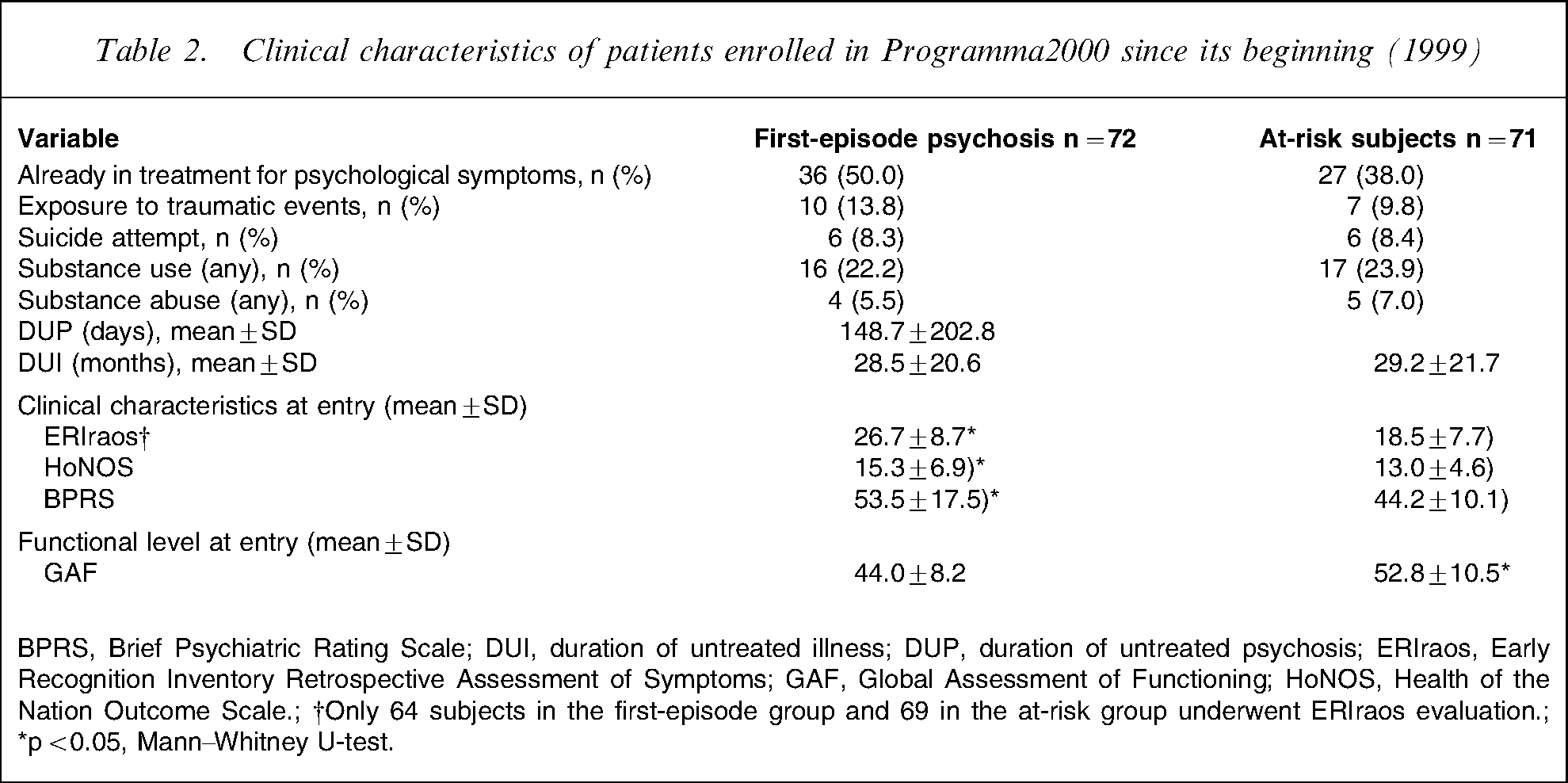
BPRS, Brief Psychiatric Rating Scale; DUI, duration of untreated illness; DUP, duration of untreated psychosis; ERIraos, Early Recognition Inventory Retrospective Assessment of Symptoms; GAF, Global Assessment of Functioning; HoNOS, Health of the Nation Outcome Scale.; †Only 64 subjects in the first-episode group and 69 in the at-risk group underwent ERIraos evaluation.; ∗p < 0.05, Mann–Whitney U-test.
A total of 44 referrals (67.6%) among those with first-episode psychosis and eight (12.9%) among those at high risk had already been hospitalized before being addressed to the Programma 2000 service (odds ratio (OR) = 12.3, 95% confidence intervals (CI) = 5.1–29.6).
Substance use was widespread in the sample: approximately 22% of patients admitted using psychoactive substances, cannabis mostly (90% of subjects reporting substance use), with a limited group also reporting having experienced ecstasy and cocaine (n = 7 per group). Criteria for substance abuse were observed in four subjects (5.5%) in the first-episode psychosis group, and in five (7.0%) in the high-risk group. In the sample substance abuse was statistically associated with a history of suicide attempt (OR = 12.6, 95%CI = 2.8–56.2).
The most frequent symptoms at referral were anxiety (81.1% of the sample, no differences by group), depressed mood (75.5% of the sample, marginally more frequent in the high-risk group), social withdrawal and deterioration in role functioning (75.0% of the sample, no differences by group). Psychomotor agitation was more frequent among patients with first-episode psychosis (34.7%) than among those in the at-risk group (16.9%): OR = 2.6, 95%CI = 1.2–5.7.
The patients with first-episode psychosis were, on average and as expected, more severe than those in the high-risk group. In general they were statistically more likely to score higher on the HoNOS and the BPRS, and lower on the GAF (corresponding to a more impaired functioning) than the high-risk patients.
The DUI was not related to the mental health status (HoNOS or BPRS) or to the level of functioning (GAF) in the patients at high risk of psychosis, nor was the DUP in those with a first episode of psychosis (Spearmann's ρ, p > 0.05). In first-episode patients only, however, transformed DUI (1/DUI) was related to BPRS (Spearmann's ρ, p < 0.05) and, marginally, to HoNOS at assessment (Spearmann's ρ, p = 0.06), but not to GAF: the longer the DUI, the more severe were the symptoms. Transformed DUP (1/DUP) was not related to any of these measures.
Provision of treatment
The patients in their first psychotic episode were more likely to receive antipsychotic drugs, atypical mostly, and less likely to receive antidepressants than the high-risk patients (Table 3). They were also more likely to be prescribed mood stabilizers other than lithium, and more likely to receive hypnotics for sleep disorders.
Pattern of care provided to the patients receiving treatment under Programma 2000 since its beginning (1999): 1 year follow up
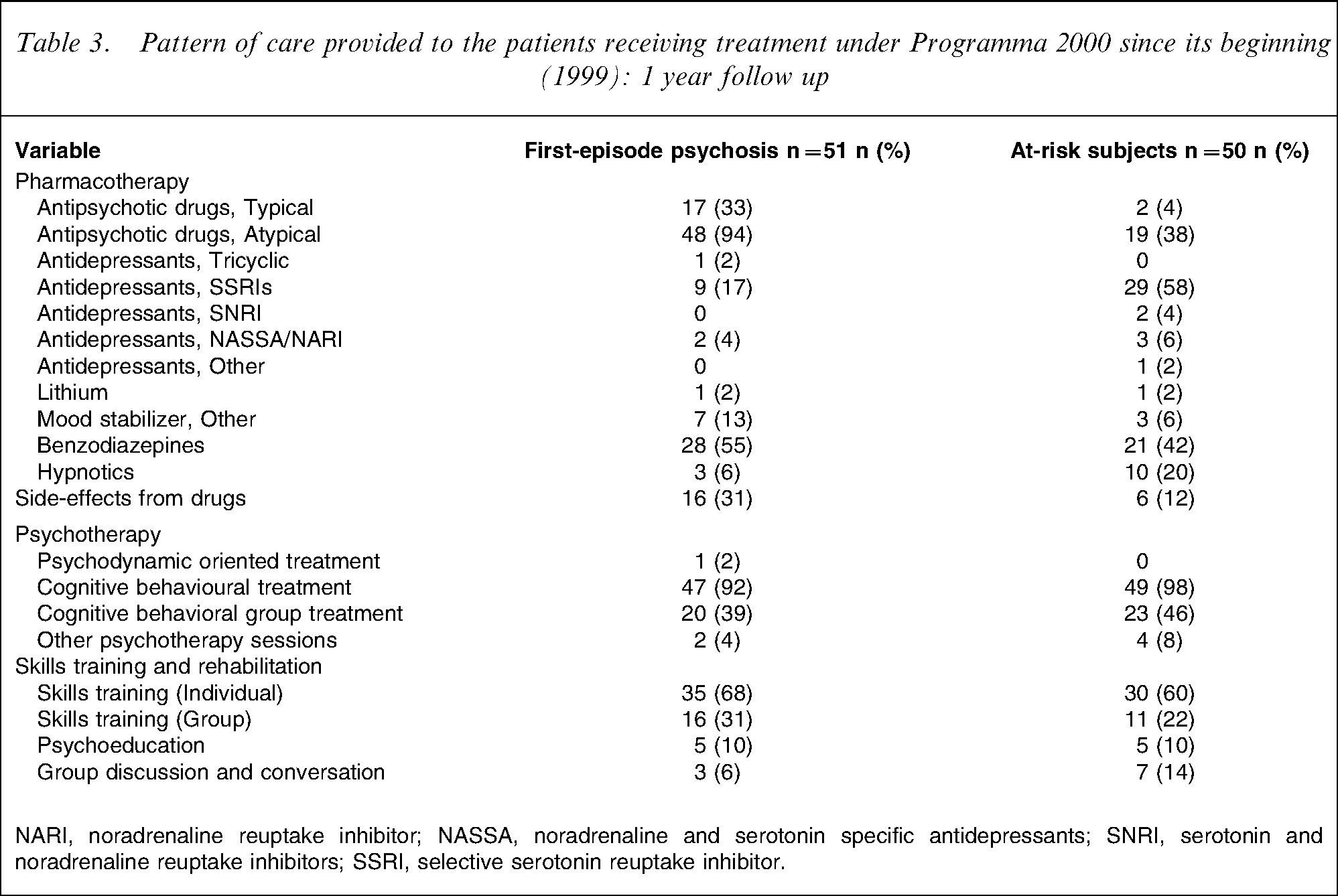
NARI, noradrenaline reuptake inhibitor; NASSA, noradrenaline and serotonin specific antidepressants; SNRI, serotonin and noradrenaline reuptake inhibitors; SSRI, selective serotonin reuptake inhibitor.
The vast majority of patients in both groups received tailored CBT (>90%); approximately half also participated in CBT-oriented group intervention. Individual sessions of skills training were provided to two-thirds of patients in both groups, while group interventions aimed at improving social and relationship skills were provided to one-third or less of the sample. Skills training was offered more often to patients at the first episode of psychosis, but the difference was not statistically significant.
Effectiveness of treatment
Duration of treatment is 5 years from initial assessment: frequency of contact is tailored to the needs and clinical status of each patient. To date, the majority of patients are compliant with treatment: 92% among first-episode and 90% among high-risk patients, respectively: we recorded four dropouts among first-episode patients (one at 24 months, one at 30 months, one at 36 months and one at 42 months), and five among high-risk patient (one at 18 months, three at 24 months, one at 54 months).
Overall, up to March 2008 29 patients with first-episode psychosis completed the 5 year treatment: eight (27.6%) were considered fully remitted, 15 (51.7%) showed relevant signs of improvement (specifically concerning the core symptoms of schizophrenia), and six (20.7%) were still severely symptomatic.
The corresponding picture for the high-risk group was 19 (total sample of completers at 5 years), with two (10.5%) fully remitted, 10 (52.6%) improved, and seven (36.8%) still severely symptomatic. To date, only two patients in the high-risk group have become fully psychotic (one within 6 months, the other within 18 months), leading to a transition rate of 2.8%.
Concerning those who accepted the treatment proposal, complete data are available for 6 month and 1 year follow up for 51 out of 72 patients at first episode of psychosis, and 50 out of 71 subjects at high risk of psychosis (more data will be available in the future: we are still completing the archive of data for ≥24 months).
Within the first year of treatment a total of five patients with active psychosis required hospitalization to control disruptive symptoms (9% of the sample, corresponding to a crude rate of 2.5 per 100 000 per year), while two patients from the high-risk group were hospitalized for treatment (4% of the sample, corresponding to a crude rate of 1 per 100 000 per year).
In both groups treatment favoured alleviation of symptoms: significant improvement was found in both the BPRS and HoNOS and in the level of global functioning, as assed by GAF, at the 6 month and 1 year follow up. Statistically significant differences on BPRS characterized both the first-episode (repeated measures: Friedman test = 43.01, df = 2, p < 0.0001) and the high-risk groups (repeated measures: Friedman test = 52.03, df = 2, p < 0.0001). Differences were also statistically significant on the HoNOS (first-episode: Friedman test = 39.42, df = 2, p < 0.0001; high-risk group: Friedman test = 46.34, df = 2, p < 0.0001).
Concerning the patients in their first episode of psychosis, at 6 month follow up a significant decline in symptom severity was detected (BPRS and HoNOS: Dunn's p < 0.01), and a further decline at 1 year (BPRS and HoNOS: Dunn's p < 0.001). The differences between the 6 month and the 1 year follow up, however, were not statistically significant (BPRS and HoNOS: Dunn's p > 0.05). In this group global functioning was more sensitive to treatment, with a marked and progressive increase in functioning from entry to 1 year later (GAF: all comparisons, Dunn's p < 0.001).
In the high-risk group the severity of symptoms decreased progressively and at follow up evaluation lower scores were reported on both the BPRS and HoNOS, compared to the initial assessment at admission to the programme (6 months: Dunn's p < 0.01; 1 year follow up: Dunn's p < 0.001). An increase in global functioning on the GAF was observed at the same time (6 months: Dunn's p < 0.001; 1 year follow up: Dunn's p < 0.0001). Progression in improvement was evident also from the comparison between the 6 month follow up and the 1 year follow up (BPRS: Dunn's p < 0.01; HoNOS: Dunn's p < 0.01; GAF: Dunn's p < 0.001).
In both groups standard deviation in the measurement of BPRS, HoNOS and GAF was very large, approximately one-third or half of the mean; this means that patients were not improving in the same proportion.
We calculated the percentage of change on the BPRS from initial assessment to the 6 month and the 1 year follow up. End-points were: responder, reduction of ≥20% in symptom severity from initial assessment; non-responder, <20% reduction in symptom severity from initial assessment; and worsened, any increase of symptom severity from initial assessment.
At 6 months, in the first-episode group 33 subjects (64.7%) were classified as responders, 14 (27.4%) did not record any change, and four (7.8%) had worsened. Among the high-risk patients the ratios were 24 (48.0%), 17 (34.0%), and nine (18.0%), respectively. The 1 year follow up noted an increase in the proportion of responders in both first-episode (72.5%) and high-risk (62.0%) patients, while the number of patients that had worsened increased in the first-episode group marginally (n = 6), and declined in the high-risk group (n = 6).
At the 6 month follow up one patient in the high-risk group and four patients in the first-episode group had GAF < 39, indicating very poor level of functioning. At the 1 year follow up no patient showed such a low level of functioning.
According to the criteria of the Remission in Schizophrenia Working Group, 35 patients out of 51 (68.6%) among those in the first-episode psychosis group, and 45 out of 50 (90.0%) in the high-risk group were in remission after 1 year, as determined by core symptoms of psychosis.
In patients with first-episode psychosis, transformed DUI (but not DUP) was related to BPRS (Spearmann's ρ, p < 0.05), but not to HoNOS and GAF at 1 year: the longer the DUI, the higher the score on the BPRS. In the high-risk group, transformed DUI was related to GAF after both 6 months and 1 year (Spearmann's ρ, p < 0.05).
Discussion
Programma 2000 is entering its 10th year of activity: in the first 9 years of service provision it proved able to attract subjects in need for treatment. A large review of incidence studies on schizophrenia found a median yearly incidence of 15 cases per 100 000 [46]. In a catchment area of 200 000 inhabitants this would lead to 30 new cases per year: this means that Programma 2000 does not intercept all emerging new cases as yet (it enrols, on average, 12 patients per year). This is a likely reflection of the mixed nature of the mental health network of care in Italy, where public and private facilities compete to provide treatment for people in need [19].
Nevertheless active and valid collaboration has been established over time, with most institutional services involved in the detection and treatment of patients at onset of or at high risk of psychosis. Also, mental health services and departments operating outside Milan pay much attention to the activities of Programma 2000, as evidenced by the two team leaders’ being frequently invited to conferences and presentations. This confirms the pioneering role of the programme, seen by most as a pilot experience in the wake of the revolution of psychiatric care started in Italy by the 1978 reform law.
As in other studies assessing patients at their first episode of psychosis or at risk of it, male patients tend to prevail in the sample. This is at odds with the fact that more women request intervention for psychological symptoms [47], but is consistent with the earlier symptom onset, or recognition, in male compared to female subjects [48], [49].
In the present sample DUP was not related to symptoms severity or to global functioning at initial patient assessment. The role of DUP as a predictive indicator of symptom severity or outcome is still debated [50]. Two meta-analyses found a consistent small–moderate effect of DUP on outcome variables [51], [52]. The impact of DUP on symptom severity at presentation is more controversial [42], and samples recruited for early intervention programmes yielded negative results similar to those of the present study [53–55]. Nevertheless the samples from early detection and treatment programmes involved significant shorter DUP than those from standard treatment [56].
In the present sample DUP was shorter than in other studies on first-episode patients: with a mean of 148 days (21 weeks), the present subjects had a shorter DUP than in the First-Episode Psychosis Outcome Study of the Early Psychosis Prevention and Intervention Center (DUP = 325 days in non-affective psychosis, i.e. 46.4 weeks) [57], and a consistently lower DUP than that observed in standard treatment in a South Dublin urban catchment area, where mean DUP was 17.9 months (71.6 weeks, or 537 days, for a standard 30 day month) [58]. Our impression is that shorter DUP reflects the programme's ability to identify patients in need of treatment earlier: a reduction of DUI and DUP is exactly what is expected of an early intervention service, and a weaker negative impact of DUP on symptom severity and outcome might be the result of the intervention. There is no standard method, however, to assess DUI and DUP, so lower values in the present study might result from the use of a conservative approach during ascertainment.
Treatment under the programme caused a reduction in the risk of hospitalization, a stressful event that increases the burden associated with psychotic illness: the recorded crude rates are 2.5 per 100 000 per year among those with first-episode psychosis, and 1 per 100 000 per year in the at-risk group. In England up to 70% of patients with a diagnosis of schizophrenia are admitted to hospital within 90 days of first contact [59]. In Italy, first-admission rates for people with schizophrenia were calculated between 5 and 8 per 100 000 per year [18], well above those observed in the present sample. This area, however, deserves further investigation.
Less data are available on high-risk subjects. There is evidence indicating that specific psychological and/or psychopharmacological interventions may reduce transition rates in high-risk subjects, that is, those who show attenuated symptoms of psychosis [60]. In naturalistic studies the transition rates in samples of subjects at high risk of psychosis vary from 9% to 54% [11]. Methodological issues, that is, heterogeneity of samples, differences in the definition of the condition, in the criteria of enrolment and in the design of the study, all raise the need for more sound replications of these promising results [11]. In the sample of people treated within Programma 2000, the transition rate in high-risk subjects in the first 2 years of care is 2.8% [61], which is worth the initial investment. Large-sample studies found a conversion rate of 49% in 110 subjects identified with the Bonn Scale of Basic Symptoms [62], and of 35% in 104 clinical high-risk subjects [63], and 291 individuals [64], respectively, identified on the basis of criteria that are very similar to those of Programma 2000. The lower transition rate in high-risk subjects emerging from Programma 2000 than that found in large samples might depend on a very inclusive application of enrolment criteria, which is likely to include people not really at risk of schizophrenia. Transition rates as low as the present ones, however, have been reported elsewhere [11], and in recent years a reduction in transition rates was reported by some centres for people at high risk of psychosis, an effect attributed to both the effectiveness of the programmes of care [65] and the dilution in truly high-risk subjects following the growing referral of false-positive cases [66].
Both first-episode and high-risk patients improved their measures of psychopathology (BPRS and HoNOS). Improvement in clinical status generally correlates with improvement in social functioning, with skills training apparently exerting a positive effect on both social functioning and self-esteem, probably because it acts on self-efficacy [67]. In both the first-episode and the high-risk groups, the improvement in patients’ social functioning is associated with a statistically significant reduction of highly expressed emotion in patients’ parents, as measured by the CFI [68]. Furthermore, preliminary financial analyses have produced promising data on the programme's positive cost-efficacy ratio [69].
On the whole this preliminary evidence points towards good replication of the results obtained in other countries [6], [50], but these positive results need a more in-depth evaluation, specifically concerning the follow up at 2 years, a sensitive deadline in the course of psychosis [70]. Nevertheless they indicate that the implementation of dedicated protocols of care for the early identification and treatment of young subjects at high risk of, or affected by psychotic illness, is a sustainable extension of traditional care for people with mental disorders in Italy.
Footnotes
Acknowledgements
The Programma 2000 group includes: Professor Angelo Cocchi, MD (team leader); Anna Meneghelli, PsyD (clinical and scientific coordinator); Andrea Alpi, PsyD, Laura Bislenghi, PsyD, Tiziana Bolis, PsyD, Noelia Moreno Granados, PsyD, Giovanni Patelli, PsyD, Marco Ponteri, PsyD, Nicoletta Pafumi, PsyD (all clinical psychologists); Claudia Caprin, PsyD (Assistant Professor of Psychology); Federico Galvan, MA (educator); Alessia Pisano, PsyD (psychologist); Simona Barbera, MD (psychiatrist); Stefano Romanò, MD (psychiatrist); Daniele von Morghen, MD (psychiatrist). The team also includes a very active group of psychologists in training. Antonio Preti, MD, is scientific advisor and consultant to Programma 2000. The authors wish to acknowledge the continuous and invaluable support and encouragement by Dr Giovanni de Girolamo. Programma2000 is entirely funded by a grant of the Lombardy Regional Health Authority (Italy).