
Abstract
Mental illness is the leading cause of non-fatal disease burden in Australia [1] and while there have been improvements in the mental health literacy of the Australian public over the past 10 years [2,3]; stigma remains the major barrier to receiving effective mental health care [4–6]. Mental health stigma is not restricted to members of the public and can extend to health care professionals, including pharmacists. Medicines are a major modality of treatment for most mental illnesses and pharmacists are frequently consulted for advice on psychotropic medicines [7]. Medication counselling by pharmacists has shown to improve adherence to medicines for mental illnesses [8,9]. However mental health stigma and lack of knowledge of mental illness can interfere with professional practice [10,11]. The lack of mental health pharmacy education has been described as a main barrier to the successful provision of pharmaceutical services for consumers with a mental illness [12].
Mental Health First Aid (MHFA) is a training programme in how to support someone in a mental health crisis or who is developing a mental disorder [13]. It has been shown to increase knowledge, reduce stigma and increase supportive actions [13–17]. MHFA training can assist in the early intervention and in the on-going community support of people with mental illnesses and may be useful for people employed in areas which involve increased contact with mental health issues such as pharmacists, pharmacy interns and pharmacy students [13,15].
Jorm and colleagues have defined the term ‘mental health literacy’ as ‘the knowledge and beliefs about mental disorders which aid their recognition, management or prevention’ [18]. Mental health literacy also includes the ability to recognize specific mental disorders; knowing how to seek mental health-related information; knowledge of risk factors and causes, of self-treatments and of professional help available for mental disorders [19,20]. Poor mental health literacy may hinder public acceptance of evidence-based mental health care and may limit the early detection and recognition of mental illness in the community [19,20]. MHFA training has been demonstrated to improve mental health literacy within the general population but there are limited data on its use in educating future health care professionals [13].
Pharmacists are frontline primary healthcare workers and it is essential that they are adequately trained in mental health to ensure they are confident and have the skills to effectively communicate with consumers with a mental illness. While pharmacists have been shown to be able to recognize mental disorders, they rate long-term outcomes more negatively than the public and may not recognize the link between mental disorders and the risk of suicide [21]. The aim of this study was to assess the impact of providing MHFA training for pharmacy students and to evaluate its impact on their mental health literacy, stigma and self-reported behaviour towards mental illness. The null hypothesis was that MHFA training would have no impact on pharmacy students’ mental health literacy, stigma and self-reported behaviour towards mental illness.
Methods
Study design
All pharmacy students (n = 272) in their third year of a four-year Bachelor of Pharmacy degree at the University of Sydney, Australia in 2009, were invited to participate in the study. A non-randomized controlled design was used to evaluate the impact of this educational intervention. All students were invited to complete the baseline survey in July 2009. The students then participated in a series of seven 1-h mental health lectures, undertook supervised weekly placements in a community pharmacy and completed a 2-h tutorial on a mental health topic. These were all part of the standard mental health related curriculum. In August 2009 all students were invited, in person and via email, to participate in MHFA training. A total of 174 students applied to attend the training. However, as places were limited to 60, 60 students were randomly selected from the 174 who applied to attend. The 114 students who applied to attend training but were not selected were considered to be part of the non-MHFA group, together with the 98 students who did not apply to attend the training. Hence there were 60 participants in the MHFA group and 212 in the non-MHFA group. In November 2009, six weeks after the MHFA courses, all students were invited to complete the post-intervention survey instrument (Figure 1). This study was approved by the University of Sydney Human Research Ethics Committee.
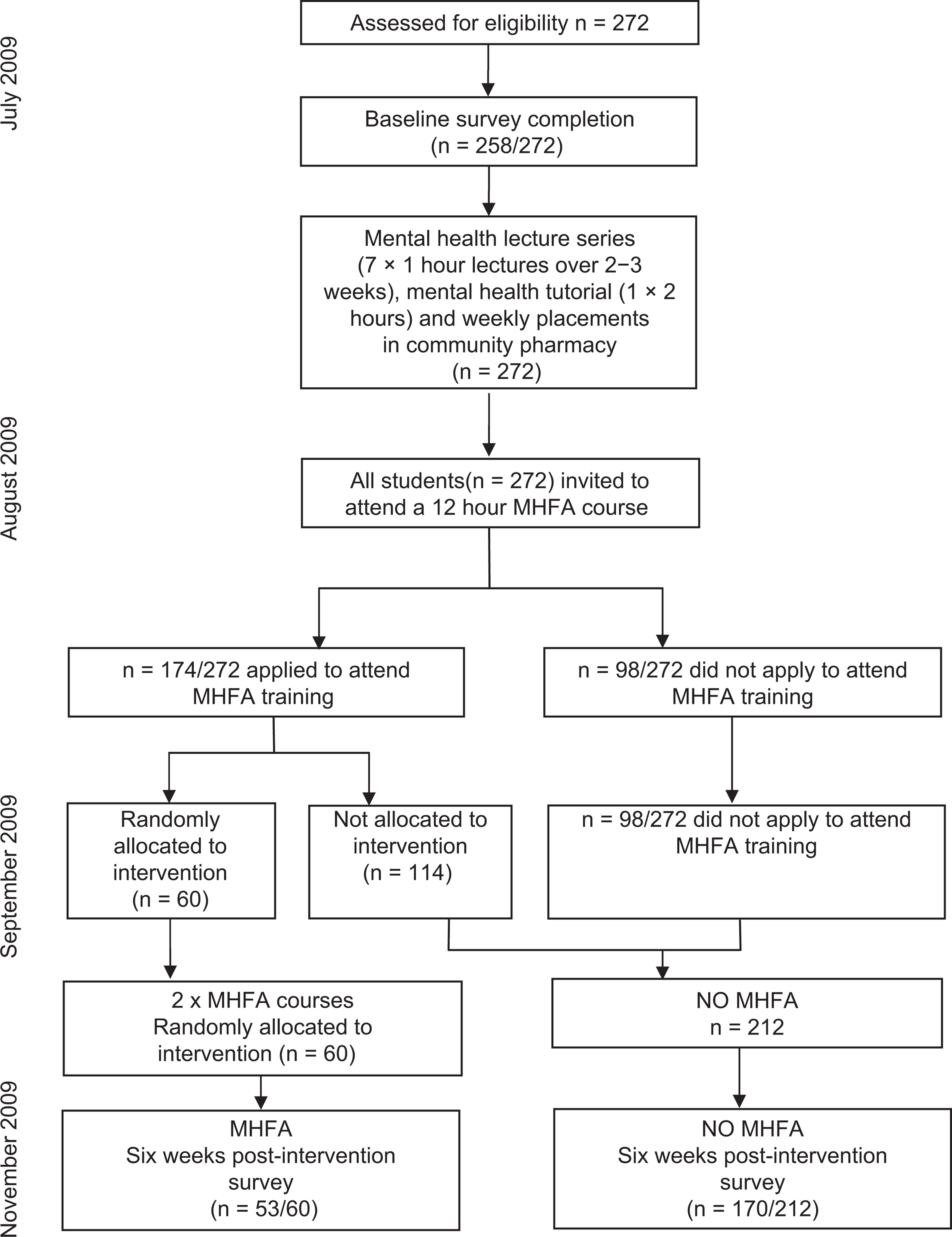
Outline of study design.
The intervention
Two MHFA courses (standard adult MHFA training programme, first edition), of 12 h duration were conducted in September 2009. MHFA teaches participants skills to recognize the early warning signs of mental illness and how to provide initial help to someone in a mental health crisis. The course teaches the symptoms, causes and evidence-based treatments for depression, anxiety disorders, psychosis and substance use disorder. It also addresses the possible crisis situations arising from these mental health problems, such as feeling suicidal, panic attacks, recent trauma, acutely psychotic and perceived to be threatening violence or an overdose [22]. The courses; which also involved case studies, filmed video clips of consumers’ experiences with mental illness and group activities, were conducted by one of the authors who is an accredited MHFA instructor (COR).
Survey instrument
The survey instrument contained the 7-item social distance scale, a measure of mental health literacy and 16 items on participation in medication counselling and identification of drug-related problems (in mental illness and cardiovascular disease). The social distance scale is a widely used instrument to measure stigma towards people with mental disorders and has been previously tested for reliability and validity [23,24]. The social distance scale asks how willing they are to associate with a person previously hospitalized for schizophrenia. Mental health literacy is tested using a structured interview, previously developed by Jorm and colleagues [18], from the National Survey of Mental Health Literacy [18]. The interview has previously been modified to a questionnaire for self-completion by health care professionals [25,26]. Vignettes of a person with either depression or psychosis were presented. The sex of the person described in the vignette was randomly assigned to be either male (John) or female (Mary). The vignettes are based on the DSM-IV [27] and ICD-10 [28] diagnostic criteria for major depression and schizophrenia. Participants in this study randomly received one of four versions of the MHL vignette.
The depression vignette was as follows:
John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn't feel like eating and has lost weight. He can't keep his mind on his work and puts off making any decisions. Even day-to-day tasks seem too much for him. This has come to the attention of John's boss who is concerned about his lowered productivity.
The schizophrenia vignette was as follows:
John is 24 and lives at home with his parents. He has had a few temporary jobs since finishing school but is now unemployed. Over the last six months he has stopped seeing his friends, and has begun locking himself in his bedroom and refusing to eat with the family or to have a bath. His parents also hear him walking about in his bedroom at night while they are in bed. Even though they know he is alone, they have heard him shouting and arguing as if someone else is there. When they try to encourage him to do more things, he whispers that he won't leave home because he is being spied upon by the neighbour. They realize he is not taking drugs because he never sees anyone or goes anywhere.’
Respondents were then asked an open-ended question, ‘from the information given, what, if anything, is wrong with John/Mary?’ Responses were coded as correct for the depression vignette if ‘depression’, ‘depressed’, ‘affective disorder’ or ‘mood disorder’ were mentioned. For the schizophrenia vignette responses were considered correct if ‘schizophrenia’, ‘schizoaffective disorder’ or ‘psychosis’ were mentioned. Respondents were then asked a series of questions about the helpfulness of various interventions, which they rated as either ‘helpful’, ‘neither’ or ‘harmful’. Further questions related to the person in the vignette's likely prognosis with and without professional help and the likelihood of the person being discriminated against.
The section on self-reported behaviour comprised 16 questions based on a survey of pharmacists’ attitudes towards mental illness and providing pharmaceutical care to these patients [29]. These questions asked how confident, comfortable, interested and likely they are to provide medication counselling and to screen for drug-related problems for patients with a mental illness compared to patients with a cardiovascular illness. Demographic data were also collected including age, gender, country of birth, parent's country of birth, previous work experience in pharmacy, and personal and family experience of mental illness.
Data analysis
Data were analysed using SPSS Version 18.0 and SAS 9.2. Pearson's Chi-square was used to investigate any differences between the MHFA and non-MHFA groups’ demographic characteristics including gender, country of birth, parents’ countries of birth, work experience in pharmacy, and experience with mental illness.
Mixed between-within analysis of variance (ANOVA) was conducted to assess the impact of MHFA training on the participants social distance scores, mental health literacy and self-reported behaviour in service provision across two time points (pre-intervention and six weeks post-intervention). The assumptions for mixed between-within ANOVA were met, and if the sphericity assumption was violated, the Huynh-Feldt degrees of freedom were reported. The seven items from the social distance scale were aggregated to give a total score out of 28. To score the literacy items regarding the beliefs about the helpfulness of interventions in depression and schizophrenia, a scale was created to show the extent the students agreed with health professionals’ views about which interventions are helpful. This scale was adopted from previous mental health literacy studies [13,14,16], and has been used in studies evaluating the impact of MHFA training [30,31]. It is based on professional consensus that GPs, psychiatrists, clinical psychologists, antidepressants, counselling and cognitive behaviour therapy are helpful for depression; while GPs, psychiatrists, clinical psychologists, antipsychotics and admission to a psychiatric ward are helpful for schizophrenia [26]. Thus for the depression vignette students were given a score from 0 to 6 and for the schizophrenia vignette a score from 0 to 5.
For the dichotomous outcome measures, logistic regression was used. Exact logistic methods were used due to zero or low frequencies in some cells [32,33]. The models included baseline scores and the group as explanatory variables for the post-intervention scores.
All analyses were conducted using the intention-to-treat principle, to ensure that all participants who completed the baseline survey were included, even if they subsequently failed to complete the post-intervention survey. In such cases, the baseline score was carried forward to the post-intervention score, so that no improvement was assumed. A significance level of p <0.05 was chosen for all analyses.
Results
The survey instrument was completed by 258 participants at baseline (59 MHFA and 199 non-MHFA) and 223 participants at the six week follow up (53 MHFA and 170 non-MHFA); representing response rates of 95% and 82% respectively. The mean age of participants was 21 years (SD 1.99, range 19–35) and the majority were female (64%) (Table 1). Most participants had previous experience working in a pharmacy (82%) and 11% reported having a previous personal experience with mental illness. There were significantly more females (p = 0.028) and more participants with previous work experience in pharmacy (p = 0.011) in the MHFA group. All other participant characteristics had no statistical differences between the groups.
Demographics of third year pharmacy students at the University of Sydney
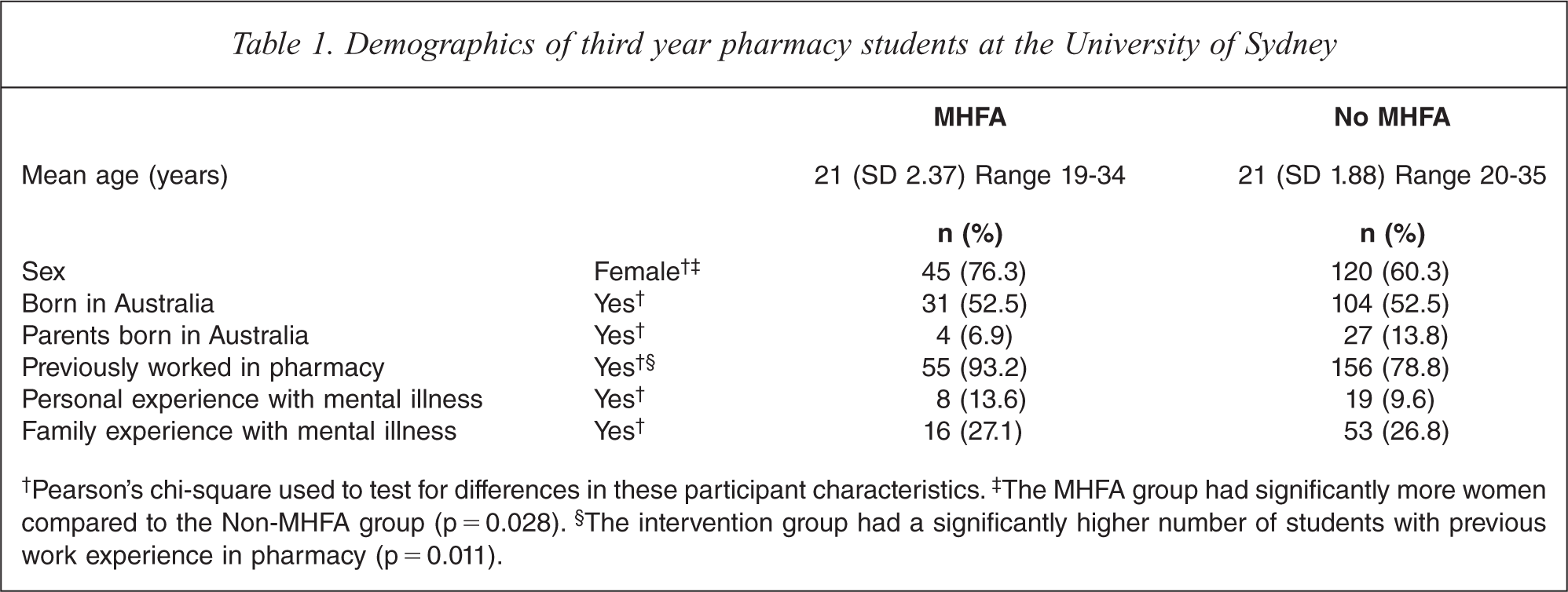
†Pearson's chi-square used to test for differences in these participant characteristics. ‡The MHFA group had significantly more women compared to the Non-MHFA group (p = 0.028). §The intervention group had a significantly higher number of students with previous work experience in pharmacy (p = 0.011).
Participants in the MHFA group had significant decreases in social distance scores with a significant interaction effect between intervention type and time (p < 0.001). These significant decreases in social distance (p < 0.001) indicated that participants who completed MHFA training were more willing to associate with a person previously hospitalized for schizophrenia than those who didn't complete the training (Table 2).
Social Distance Scale†
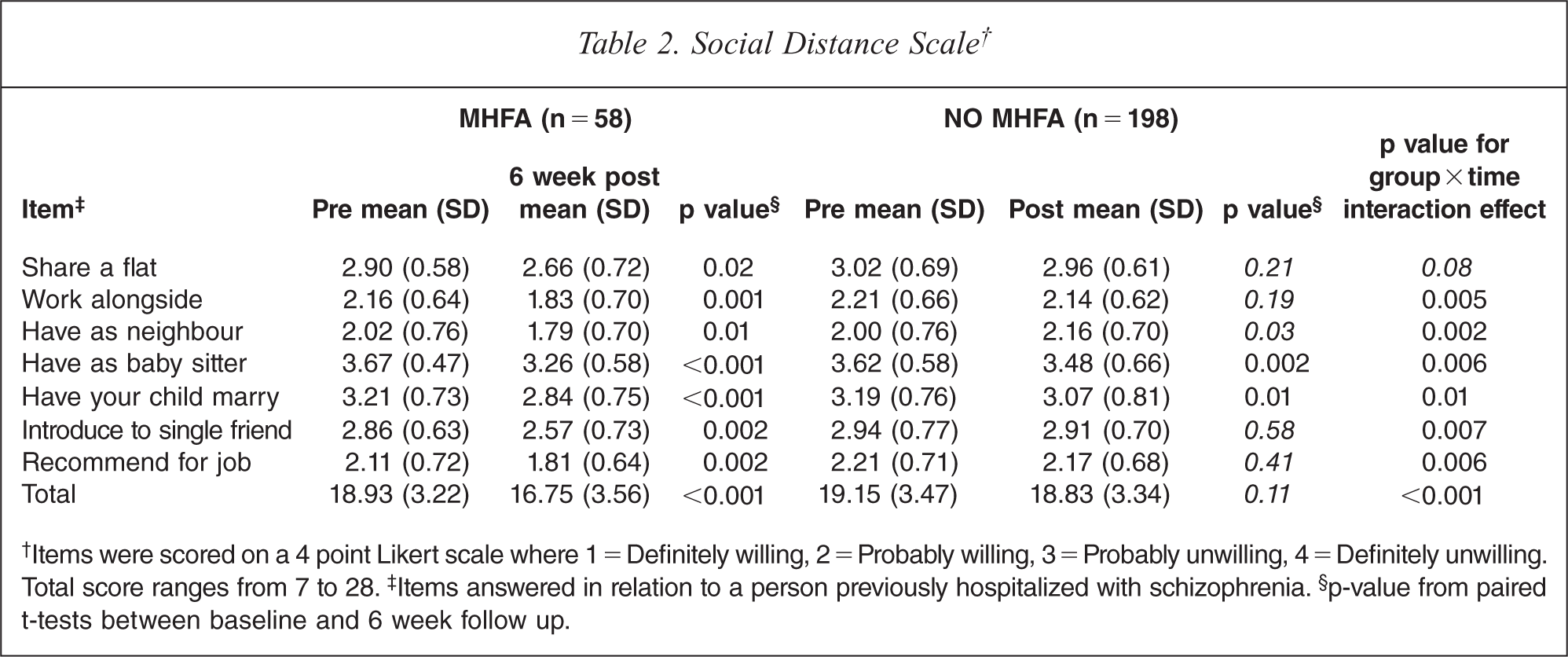
†Items were scored on a 4 point Likert scale where 1 = Definitely willing, 2 = Probably willing, 3 = Probably unwilling, 4 = Definitely unwilling. Total score ranges from 7 to 28. ‡Items answered in relation to a person previously hospitalized with schizophrenia. §p-value from paired t-tests between baseline and 6 week follow up.
The ability of participants to correctly identify a mental illness significantly improved after MHFA training (p = 0.004) (Table 3). While the participants’ ability to recognize specific mental illnesses such as schizophrenia or depression did improve, the results did not reach statistical significance at the 5% level.
Number of participants who correctly identified the mental disorder in the vignette
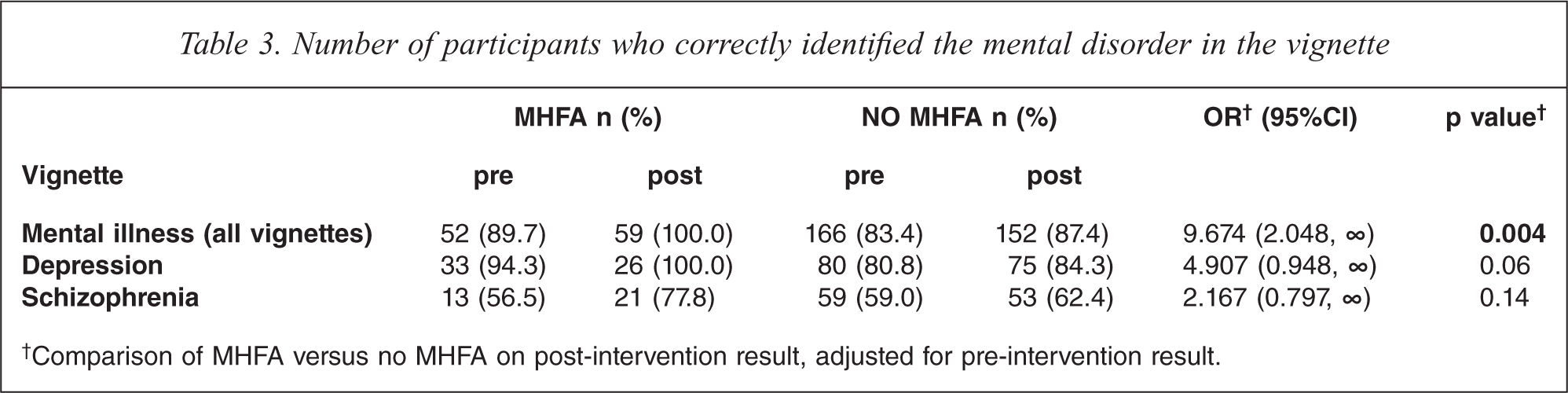
†Comparison of MHFA versus no MHFA on post-intervention result, adjusted for pre-intervention result.
There were improvements in the recognition of helpful interventions, with participants’ views becoming more concordant with health professional views about treatments for depression and schizophrenia. Participants agreed significantly more strongly with health professional consensus about the helpfulness of interventions in depression (p = 0.009) after the MHFA training, and while there were improvements in the schizophrenia scores, they were not significant (p = 0.08) (Table 4). In relation to long term outcomes, a significantly higher number of participants in the MHFA group (p <0.001) recognized the person in the vignette would get worse as a result of receiving no professional help.
Beliefs about treatments for schizophrenia and depression
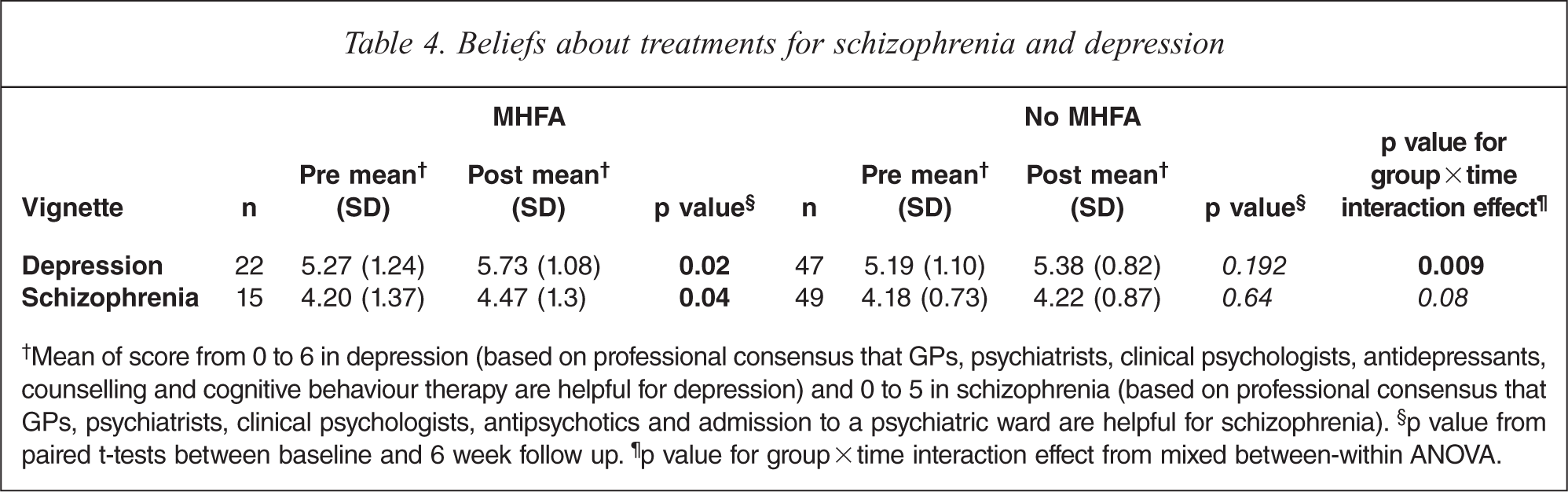
†Mean of score from 0 to 6 in depression (based on professional consensus that GPs, psychiatrists, clinical psychologists, antidepressants, counselling and cognitive behaviour therapy are helpful for depression) and 0 to 5 in schizophrenia (based on professional consensus that GPs, psychiatrists, clinical psychologists, antipsychotics and admission to a psychiatric ward are helpful for schizophrenia). §p value from paired t-tests between baseline and 6 week follow up. ¶p value for group × time interaction effect from mixed between-within ANOVA.
Participants who attended the MHFA training were significantly more confident at providing medication counselling (p < 0.001) and identifying drug-related problems (p = 0.006) in mental illness compared to those students who did not attend the training (Table 5). However, when the mental illness self-reported behaviour results were compared to the cardiovascular disease results, the participants were still significantly more confident, comfortable, interested and likely in relation to providing medication counselling and identifying drug related problems with cardiovascular disease (p <0.001) than they were with mental illness.
Self-reported behaviour in mental illness and cardiovascular disease
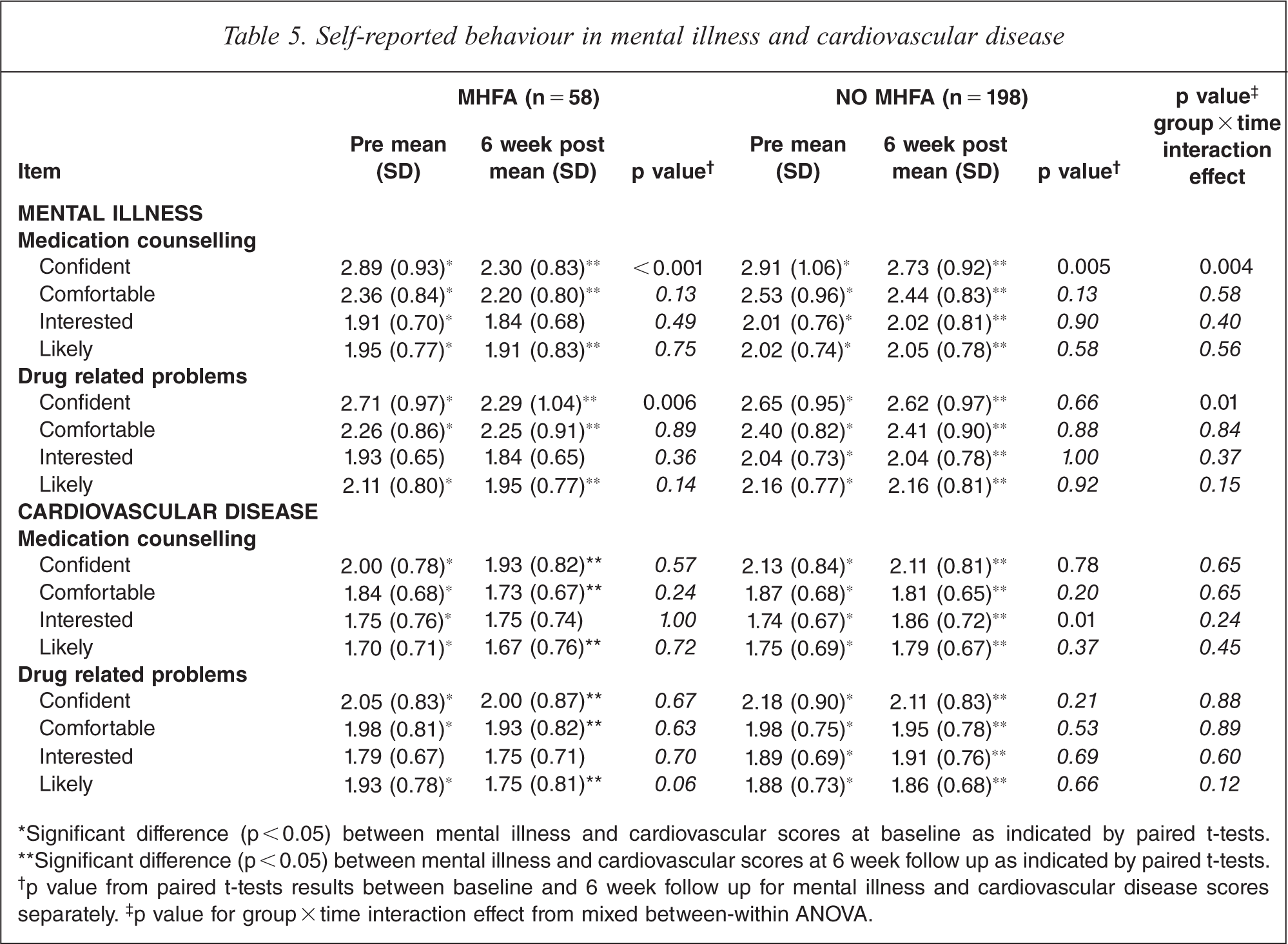
*Significant difference (p<0.05) between mental illness and cardiovascular scores at baseline as indicated by paired t-tests.
**Significant difference (p < 0.05) between mental illness and cardiovascular scores at 6 week follow up as indicated by paired t-tests.
†p value from paired t-tests results between baseline and 6 week follow up for mental illness and cardiovascular disease scores separately. †p value for group × time interaction effect from mixed between-within ANOVA.
Discussion
MHFA training was demonstrated to be an effective method at improving mental health literacy and decreasing mental health stigma among pharmacy students. This was the first study to demonstrate the value of MHFA training for pharmacy students. This study demonstrated that participants who received MHFA training were better able to recognize mental illnesses and support evidence-based interventions for mental illnesses. The training also decreased their social distance and stigmatizing attitudes towards mental illness, and improved their confidence in being able to provide pharmaceutical services to consumers with mental illness. These are important findings as pharmacists are among the most accessible primary health professionals, have regular contact with patients and have a potentially important role in the screening and referral of people when early warning signs of a mental illness first appear [34]. Our research further demonstrates the benefits of MHFA training previously shown in studies of the public, teachers, farmers and in various ethnic communities in Australia [13,15,17,30,31,35].
This project demonstrated the feasibility of using an evidence-based training programme to improve participants’ ability to handle mental health situations in their future professional practice as pharmacists. This training complemented the standard teaching methods used in mental health pharmacy education and our data suggests that participants had a more in-depth understanding of mental health issues and the self-reported confidence to handle mental health crisis situations when confronted with them. The MHFA training programme was well received by participants with a high demand for the 60 places available in the training courses. Anecdotal feedback revealed that participants felt the training gave them a greater insight into how to handle mental health situations in their future professional practice.
MHFA training significantly improved the self-reported confidence of participants in providing medication counselling and identifying drug-related problems in mental illness; two core professional roles of a pharmacist. The baseline data showed that the participants were significantly more confident and comfortable in providing pharmaceutical services to a consumer with cardiovascular disease than mental illness. This is consistent with previous studies indicating pharmacists are more confident with physical illnesses compared to mental illnesses [10,36]. There is a high demand from consumers to receive advice about psychotropic medicines [37] and this finding demonstrates the potential for facilitating increased provision of pharmacy services to consumers with a mental illness. However, when compared to cardiovascular disease at post-intervention, participants were still significantly more confident and comfortable with cardiovascular disease following the training. Furthermore, there were no significant differences for the items comfortable’, ‘interested’ or ‘likely’ to either provide medication counselling or identify drug-related problems in a person with a mental illness following MHFA training. Therefore, whilst MHFA training did have a positive impact on improving confidence, more specific training may be required for pharmacy students to alleviate this disparity between physical and mental illnesses and allow the students to feel more comfortable at providing pharmaceutical services to people with a mental illness.
The findings from this study are comparable to other studies of educational interventions with pharmacy students aimed at reducing mental health stigma and improving confidence in providing pharmaceutical services to people with a mental illness [38–40]. Contact with mental health consumers is considered an effective approach at reducing mental health stigma. While face-to-face contact with mental health consumers is considered the ideal method of contact, indirect contact via a film medium has also been shown to be effective and is a much more exportable intervention [41]. Furthermore, watching video clips as part of an online MHFA programme has been shown to have greater stigma reduction benefits than solely reading a MHFA manual [42]. Face-to-face contact-based interventions with mental health consumers in an educational setting have been shown to have sustained impacts on mental health stigma over a 12 month period [38]. However, it is unknown whether the improvements seen in evaluations of MHFA are sustained for the same length of time as face-to-face contact-based interventions.
A key strength of this study was the presence of a comparison group. All 272 students were invited to apply to attend MHFA training. Out of the 174 applicants, 60 were randomly allocated to attend one of two MHFA courses. So although students were randomly allocated to attend the MHFA courses, they self-selected to be offered training. Therefore, there was a possibility of self-selection bias between the MHFA and non-MHFA groups. Nevertheless, there was an extremely high demand for places; the 114 students who applied to participate in the training but who were not randomly allocated were then included in the non-MHFA group. This study was conducted in a pharmacy student population at one university and these results may not be generalizable to the broader pharmacist population or to other allied health care professionals. While the MHFA training programme was originally developed to educate members of the public and not health professionals, we demonstrated its applicability in the training of health professional students. Post-intervention data were collected at six weeks post MHFA training. It is unclear whether the intervention resulted in sustained improvements as other mental health pharmacy interventions have been able to demonstrate [38].
Future studies evaluating the impact of MHFA in pharmacists should consider engaging a longer follow up period to ascertain whether the positive effects can be maintained. Further studies should investigate the use of MHFA training in other pharmacist populations to ensure the generalizability of our findings.
Conclusion
This study demonstrated that MHFA training can reduce pharmacy students’ mental health stigma, improve recognition of mental disorders and improve confidence in providing services to consumers with a mental illness in the pharmacy setting.
Footnotes
Acknowledgements
We would like to acknowledge the support of Professor Anthony Jorm and Betty Kitchener in providing the mental health literacy survey instrument.