
Abstract
Mental health first aid program
Although people often know a lot about common physical health problems, there is widespread ignorance of mental health. This ignorance adds to the stigma of mental health problems and prevents people from seeking help early and seeking the best sort of help. It also prevents people from providing appropriate support to colleagues and family members, simply because they do not know how. A recent survey of the Australian public found that many people had a less than adequate range of first aid responses to people with mental disorders [1]. In order to improve this aspect of mental health literacy, a mental health first aid (MHFA) training course was developed following the model that has been successfully applied in many countries with conventional first aid.
The MHFA Program trains members of the public to give early help to people with developing mental health problems and to give assistance in mental health crisis situations. The course currently involves 12 hours of training spread over four sessions of 3 hours each. The course gives an overview of the major mental health problems in Australia, introduces the five steps of MHFA, as shown in Table 1, and then applies these steps to problems of depression, anxiety disorders, psychosis and substance use disorder. The course also covers the following mental health crisis situations: how to help a suicidal person, a person having a panic attack, a person who has experienced a traumatic event, a psychotic person who is perceived to be threatening and a person who has overdosed.
The five steps of mental health first aid (MHFA)
There is a course manual [2] that is available for sale or can be downloaded as a PDF from the MHFA website: http://www.mhfa.com.au. Instructors receive a 1-week training course and ongoing support. They have a range of backgrounds but must fulfil the following criteria: good interpersonal skills, good teaching and communication skills, favourable attitudes toward people with mental health problems, personal or professional experience of people with mental health problems, good knowledge of mental health problems and good background knowledge of mental health and community services.
At present there are approximately 350 MHFA Instructors in Australia who work for area health services, nongovernment organizations, government departments or as private practitioners. The training program has also spread to every state and territory of Australia and internationally to Scotland, Ireland, Hong Kong and the US.
Evaluation of the training course
Uncontrolled trial with the public
The first evaluation study of MHFA was an uncontrolled trial in 2001 with members of the public living in Canberra [3]. This trial examined the effects of the course on knowledge of mental disorders, stigmatizing attitudes and help provided to others. There were 210 participants who were given questionnaires at the beginning of the course, at the end and at 6months follow-up. Participants were typically middle aged, predominantly female (80%) and well educated (44% with a university degree). The course was found to produce the following benefits: better recognition of mental disorders from case vignettes, changed beliefs about treatment to be more like those of health professionals, decreased social distance from people with mental disorders (a measure of stigma), increased confidence in providing help and an increase in the amount of help provided to others.
Although this trial showed positive benefits, there was no control group, so that change could not be distinguished as being due to the course itself, multiple testing or other factors in the participants' lives.
Controlled trial in the workplace
Because the first study had no control group, a second trial was conducted in which course participants were compared with a wait-list control group [4]. This randomized controlled trial was carried out in 2002 with employees of two Australian government departments who did the course during their work time. The trial involved 301 participants who were randomized to either participate immediately in a course or to be wait-listed for 5 months before undertaking the training. The trained group improved more than the wait-list control group in the following areas: greater confidence in providing help to others, greater likelihood of advising people to seek professional help, improved concordance with health professionals about treatments, decrease in stigmatizing attitudes and improved mental health in the participants themselves. The mental health benefits of the course to participants were unexpected because the course does not provide therapy and promises no personal benefits. We think the course may produce mental health benefits by providing participants with good quality information which allows them to make better choices about their own mental health care.
Although this trial had the advantage of a control group, it was an efficacy trial carried out under ideal conditions: it was a well-educated group, doing it in their work time and all the instruction was carried out by the originator of the course and may not be generalizable to other instructors.
Controlled trial with the public in a rural area
To evaluate the generalizability of these findings, we next carried out an effectiveness trial using a cluster randomized design. The trial was carried out with members of the public in a large rural area of New South Wales using five staff members of the area health service trained as MHFA Instructors [5]. In this trial, the catchment area of the area health service was divided into 16 local government areas. Eight of these areas received the course immediately and the other eight were placed on a waiting list to receive the training later in the year (the controls). There were 753 participants in the trial: 416 of these were in the areas that received the course immediately and 337 were in the control group. The participants in this trial were similar to those in the earlier uncontrolled trial: mean age 47 years, 80% female and 50% did the training for reasons relating to their work, such as carers or health service providers, although not quite as well educated (22% with a university degree). People who did the course showed a number of changes relative to the control group: better recognition of disorders from case descriptions of a person with either depression or schizophrenia, decreased social distance toward people with mental disorders, more like health professionals in their beliefs about what treatments are likely to be helpful, greater confidence in providing help to someone and more likely to actually provide help.
As a follow-up to this trial, an ongoing qualitative study is asking participants about their experiences in providing help after doing the course. Wewant to find out howmany people actually used their skills following the course and whether they had good or bad outcomes in doing so.
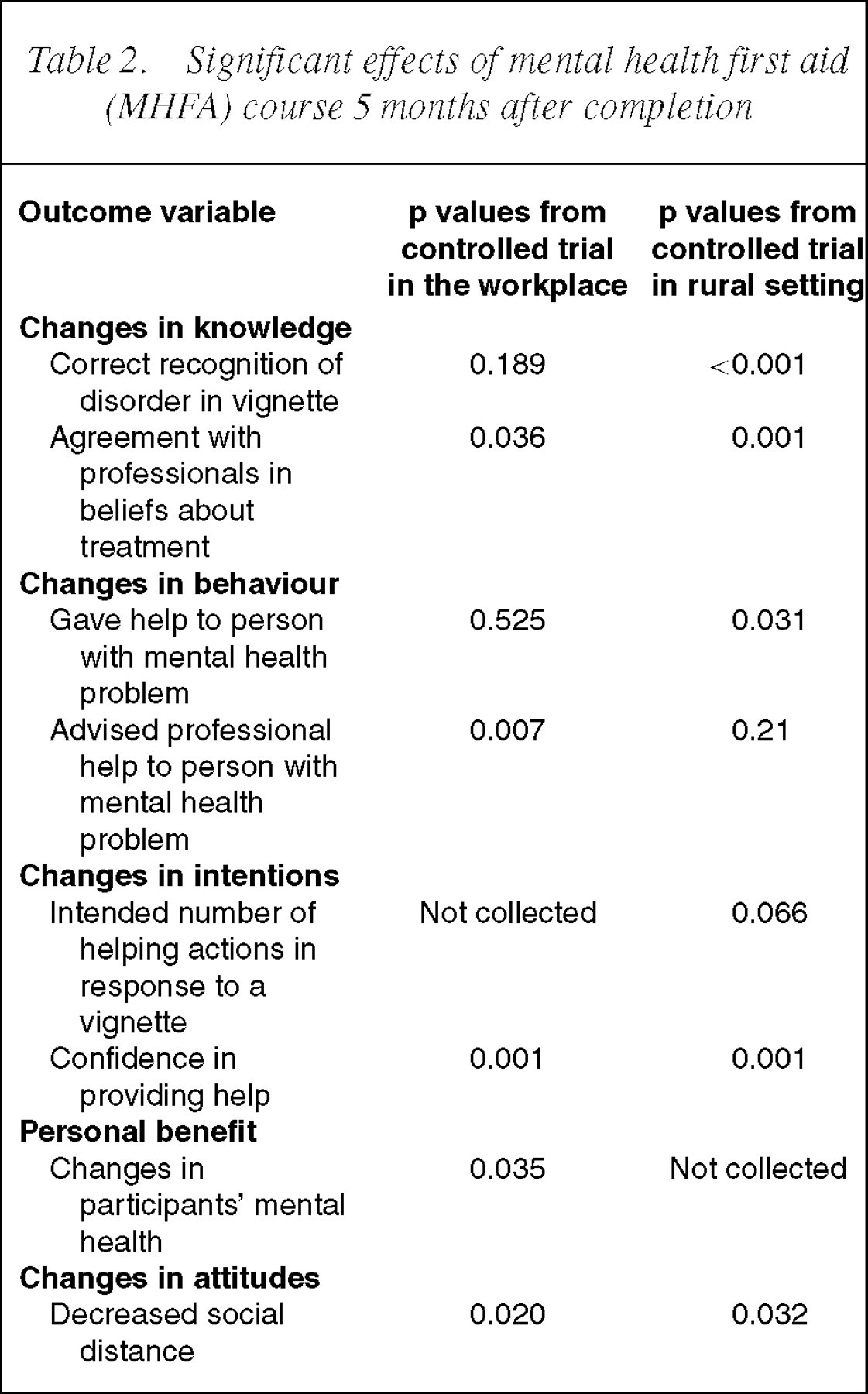
Table 2 summarizes the results from the two randomized controlled trials, showing the consistent positive benefits in knowledge (improved agreement with health professionals about treatments), in behaviour (improved helping behaviour), in intentions (greater confidence in providing help to others) and in attitudes (decreased social distance from people with mental disorders). The efficacy trial in the workplace evaluated the mental health benefits to participants and found positive effects.
Significant effects of mental health first aid (MHFA) course 5months after completion
Unanswered questions
There is a limited evidence base on the best way for a member of the public to provide help to people in mental crisis situations or with developing mental disorders. In fact, it is neither feasible nor ethical to carry out randomized controlled trials to answer questions such as ‘How should I respond to a friend who is suicidal?’. In writing the content of the MHFA course, we have tried to make it as evidence-based as possible and where there is no evidence we have sought expert opinion or, in the absence of any other information, just used common sense. However, we see a need to systematically gather expert opinion on the best first aid strategies. We are planning to carry out Delphi studies to achieve this. The outcome of this work will be a set of international standards for MHFA which any course can choose to adhere to.
Perhaps the most important unanswered question is the benefits of being a recipient of MHFA. In order to evaluate such benefits, we need to directly assess the recipients which is, in practice, very difficult to do. At this stage, we are researching the stories provided by mental health first aiders on the use theymake of their skills and any positive or negative effects on recipients. Ultimately, it may be possible to design studies in situations such as with school teachers or family carers where the recipients can be directly assessed. This will be the ultimate evaluation challenge.