
Abstract
Adolph Stern is seen as the first main descriptor of borderline personality disorder (BPD) [1]. His delineation of the syndrome is sensitive and insightful. The DSM IV catalogue of diagnostic criteria, however, barely overlaps with the phenomena he described. Nevertheless, clinicians who work in the field would see both sketches of the syndrome as accurate. This apparent discrepancy between authoritative accounts of the disorder raises a number of questions about the diagnosis of BPD. Is it merely a term used to refer to a number of more or less unrelated patterns of symptomatology occurring in difficult patients who do not fit traditional diagnostic moulds, or is it, on the other hand, a distinct entity manifest in a variety of ways? The former interpretation is seemingly supported by the way in which BPD is identified in DSM-IV. Nine criteria are given for the specification of the syndrome but only five are required for the diagnosis. Two people, both diagnosed as suffering BPD, may therefore have only one criterion in common. This polythetic method allows for the BPD diagnosis to be made by 256 different combinations of DSM-IV symptoms [2]. The method implies that there is no single unifying pattern, no core symptom, or complex of symptoms which is a particular marker of the condition.
Tyrer [3] has recently put forward a view that encompasses both interpretations of the protean character of BPD. Writing of the term ‘borderline’ and its place in psychiatric nosology he wrote: ‘I suggest that it does not belong anywhere; it should be abolished as it is a passport to heterogeneity. Unless it is redefined and reformulated, it will remain a condition that undoubtedly exists but will do so in so many forms that it defies predictions about treatment and prognosis’ (p. 94). The sense of clinicians who work in the field is not only that BPD ‘undoubtedly exists’ but also, despite its elusive nature, that it has a phenomenal core, not as yet agreed upon.
As Tyrer implies, identification of the core of BPD is essential if progress is to be made in developing more effective means of treatment, which must be primarily directed at what is most fundamental among the many phenomena associated with the diagnosis. A number of suggestions have been made about the nature of this notional core. These suggestions, in the main, concern individual phenomena such as a particular affect, a style of relatedness, a form of consciousness or characteristic way of behaving. Such phenomena, however, cannot stand alone. An affect for example, is always part of a form of consciousness, which in turn is part of a system which involves a particular relationship, whether external or internal. They are collectively linked to a way of behaving. Each phenomenon is part of a larger dynamism which includes the others. An investigation then, into the nature of the core pathology of BPD necessarily focuses on appropriate groupings of symptoms.
Groupings of symptoms and other phenomena which can be considered as the nucleus, or core, of BPD are those which persist over time, since the cardinal feature of personality disorder, as Tyrer points out, is endurance. The quality of endurance will be taken in this study as the criterion of coreness.
Groupings of phenomena can be discerned by means of factor analysis. The best known and most influential of such studies came from Clarkin, Hull and Hurt in 1993 [4]. In an exploratory factor analysis involving 75 hospitalized female borderline patients they found three main factors of DSM-III-R criteria which have been labelled as 1: self, 2: affect, and 3: impulsivity. Factor 1 loaded most strongly on emptiness/boredom, identity problems, fear of abandonment, and unstable relationships. The second factor was made up of suicidality, anger and labile affect. It was considered to reflect emotional dysregulation. Factor 3 loaded heavily on impulsivity. Clarkin and his colleagues saw this factor as standing alone as a separate dimension in borderline pathology. Other exploratory factor analyses producing a three-factor structure have come from Blais et al., Sanislow et al., and Taylor and Reeves [5–7].
Confirmatory factor analysis tends to favour a unidimensional structure [8–12]. A multi-factor structure, however, seems plausible as evidenced by the apparent separateness of the impulsivity criterion which has a distinct natural history [12], a fact remarked upon by Aggen et al. [13]. A reasonable interpretation of these findings might be that the conflict between them is only apparent, and that both are valid. BPD can be conceived as a unitary disorder made up of several groupings of phenomena which are both distinguishable and related. It is on the assumption that we have used the Clarkin et al. [4] factor analysis in our study. Furthermore, our data were collected using DSM-III-R, which Clarkin et al. had used.
The Clarkin tri-factor structure neatly separates out the two main view points about the core of BPD. The prevailing viewpoint is that affect dysregulation (Factor 2), perhaps combined with impulsivity (Factor 3), constitutes such a core. The most prominent proponent of affect dysregulation is Linehan [14] who receives influential support [15–17]. Links and his colleagues’ propose impulsivity as the core symptom [18].
On the other hand, without in general using the term ‘self’, pioneers of the BPD concept proposed nuclear features of the disorder which correspond to three of the four DSM criteria making up Clarkin's ‘self’ factor, i.e. Factor 1. Stern [1], Adler and Buie [19,20], Masterson [21] and Gunderson [22,23], noted the centrality of abandonment fears, Adler and Buie also spoke of the significance of emptiness. Kernberg [24] described ‘identity–diffusion’. A more recent formulation, from Bateman and Fonagy [25] is also congruent with the ‘self/identity’ criterion. They see a failure of ‘mentalization’ as the central deficit of BPD. ‘Mentalization’ refers to the awareness of mental states, one's own and those of others. This is a cardinal characteristic of a concept of a self system derived from the descriptions of William James [26].
In 1993 Meares proposed that a deficit in the self system is the central disturbance of BPD [26]. In terms of DSM criteria, the self system is made up of the self-identity criterion, fears of abandonment, and emptiness. This complex of criteria is theoretically derived, based on the idea that the sense of self depends upon, and arises with, a sense of the other. Where self is fragile so also is the sense of the other. When the sense of self is lost entirely, ‘emptiness’ remains [26, 1993, p. 196; 2005, pp. 222–223].
In this study we test the hypothesis that a deficit in the self system is the core disturbance in BPD using endurance as the index of coreness. A cohort of BPD patients treated by the Conversational Model for 1 year were compared in terms of the endurance of Clarkin's three factors with another cohort of BPD patients who continued treatment with their referring practitioners for one year. In addition, a similar comparison was made on the outcome of three theoretically derived complexes. Complex 1 consisted of the triad of criteria of the self system referred to above. Complex 2 was made up of the criteria relating to affect dysregulation in Clarkin's Factor 2. It also included ‘unstable relationships’, which loaded on both Factors 1 and 2 in Clarkin's study. Complex 3 was the single criterion of ‘impulsivity’.
The data came from the replication [27] of our earlier outcome study of the treatment of BPD [28–30].
A second aspect of this investigation focuses on the nature of the ‘core dysphoria’ [31] which evidence such as that from Zanarini and colleagues [32] and Paris [33] suggest is the most enduring, and thus most central, feature of BPD. Zanarini and her colleagues have likened it to ‘psychic pain’ [32]. A number of investigators distinguish it from typical unipolar depression [34]. In the present study the Zung depression scale, a measure of typical depression, is correlated with the three factors and three complexes in order to judge whether or not it is related to that grouping of phenomena which shows endurance.
Methods
Participants
The participants in this study entered treatment between 1993 and 2001 and were in therapy for 12 months. One group of 29 subjects were treated by the Conversational Model (CM) while the other, of 31 patients, waited for a period of 12 months continuing with the ‘usual treatment’ (TAU) as carried out by their referring clinicians. Allocation to the different groups depended upon what can be seen as a naturalistic randomization. Entry into the CM group depended on the chance event of a therapist being available at the time of referral. People who were referred to the programme, as well as referring clinicians, understood that there was a waiting list due to the demand for the programme and its limited resources. All patients continued to receive ongoing care and crisis support. In other words, all patients continued to receive a standard of care comparable to all other area health services in the city. Allocation to the different groups by standard means of randomization, such as random number sheets and so forth, was not acceptable to the hospital administration, to ourselves, to the patients, or to their referring physicians, since the clinic at the time was the only one in the state.
All patients entering the programme gave informed consent to the research procedures. The length of time that patients spent on the waiting list varied to some degree, again depending on the naturalistic factors of supply and demand. All 31 patients in the TAU group completed their 12-month review without having entered into therapy. In terms of the demographic variables of age, marital status, occupational and educational status there was no statistically significant difference between the study and control groups. With respect to symptom measures there was no significant difference between the study and control groups at baseline.
Measures
Following the method of a previous study, all subjects were screened at an assessment interview with the Westmead Severity Scale (WSS) for Borderline Personality Disorder (BPD). This scale was constructed from the 27 items making up the diagnostic criteria. In scoring the scale, the presence or absence of each item is elicited by means of a semi-structured interview, involving a series of probing questions. These questions require a dichotomous response. An affirmative response receives a score of one. The weighted kappa, used to test the inter-rater reliability was satisfactory, with a kappa + 0.81 for the total scale. Further details are given in previous reports [27,28]. The theoretical range of responses is 0–27. In this study the range was 7–24. The psychiatrist responsible for this part of the assessment was one of the same people who had collected the original data (J.S.). The participants also completed the Zung depression questionnaire, a 20-item scale with each item scored 1 to 4. The scale has been standardized on a New Zealand population. It has internal consistency of 0.79. Studies support the validity of the Zung in relation to the Beck Depression Inventory (BDI) [35]. As a self rating scale, the Zung is likely to reflect the patient's internal perception of dominant affective experience more closely than an observer-rated scale.
We used the scores of each participant on the Westmead Severity Scale to compute the three factors identified by Clarkin, Hull and Hurt [4] and the three theoretically derived complexes as described in the previous section. The complexes differed in only one respect from the factors. ‘Unstable relationships’ appears in Complex 2 rather than in the ‘self factor’.
Results
Data analysis
The data analysed by repeated measures ANOVA using the statistical software package SPSS for Windows version 16. The group-by-time interaction provided the measure of the significance for the treatment effect.
Demographics
The mean age of the 1-year Conversational Model (CM) group was 27.9 years (SD = 5.9) with 17 women and 12 men. In comparison the TAU group had a mean age of 29.7 (SD = 6.1) with 16 women and 15 men. The majority of the overall group (n = 47 or 78%) were unemployed and receiving government benefits. Amongst those that were in work (n = 13), only four worked in skilled occupations. Most left school early (before age 15 − 81.67%) and 11 had undertaken some form of tertiary study. More than a third (n = 22) had been separated from parents and had received long-term institutional or foster care.
Factor structure comparisons
Factor 1: identity/self disturbance
A repeated measures ANOVA was performed on Factor 1 scores identified by Clarkin et al.[4], with one within-subject factor: time (2 levels: baseline, 12 months) and one between subjects factor: group (2 levels: therapy group, TAU). The group-by-time interaction provided the measure of the significance for the treatment effect. Overall there was a significant main effect for time between baseline and 12 months therapy (Wilks’ Lambda = 0.868, F(1,55) = 8.386, p < 0.005), and there was also a significant interaction between time and group (Wilks’ Lambda = 0.878, F(1,55) = 7.664, p < 0.008).
This finding was then explored further by looking at each group separately over time. The repeated measures ANOVA revealed a highly significant clinical improvement over the 12 months for the therapy group (Wilks’ Lambda = 0.687, F(1,28) = 12.74, p < 0.001). In comparison the TAU group showed no statistical significant improvement (Wilks’ Lambda = 1, F(1,27) = 0.011, p = 0.916).
Factor 2: affect dysregulation
A repeated measures ANOVA was performed on Factor 2 scores identified by Clarkin et al.[4], with one within-subject factor: time (2 levels: baseline, 12 months) and one between subjects factor: group (2 levels: therapy group, TAU).
Overall there was a significant main effect for time between baseline and 12 months therapy (Wilks’ Lambda = 0.627, F(1,55) = 32.72, p < 0.001), and there was also a significant interaction between time and group (Wilks’ Lambda = 0.888, F(1,55) = 6.92, p < 0.011).
This finding was then explored further by looking at each group separately over time. The repeated measures ANOVA revealed a significant improvement over the 12 months for the therapy group (Wilks’ Lambda = 0.425, F(1, 28) = 37.91, p < 0.001) and also a significant change for the TAU group (Wilks’ Lambda = 0.86, F(1,27) = 4.4, p = 0.045).
Factor 3: impulsivity
A repeated measures ANOVA was performed on Factor 3 scores identified by Clarkin et al. [4].
There was a significant main effect for time between baseline and 12 months therapy (Wilks’ Lambda = 0.619, F(1,55) = 33.91, p < 0.001), but there was no significant interaction between time and group (Wilks’ Lambda = 0.953, F(1,55) = 2.7, p < 0.11). Both groups improved at approximately at the same rate.
The findings for the Clarkin factor outcomes are displayed in Figure 1.
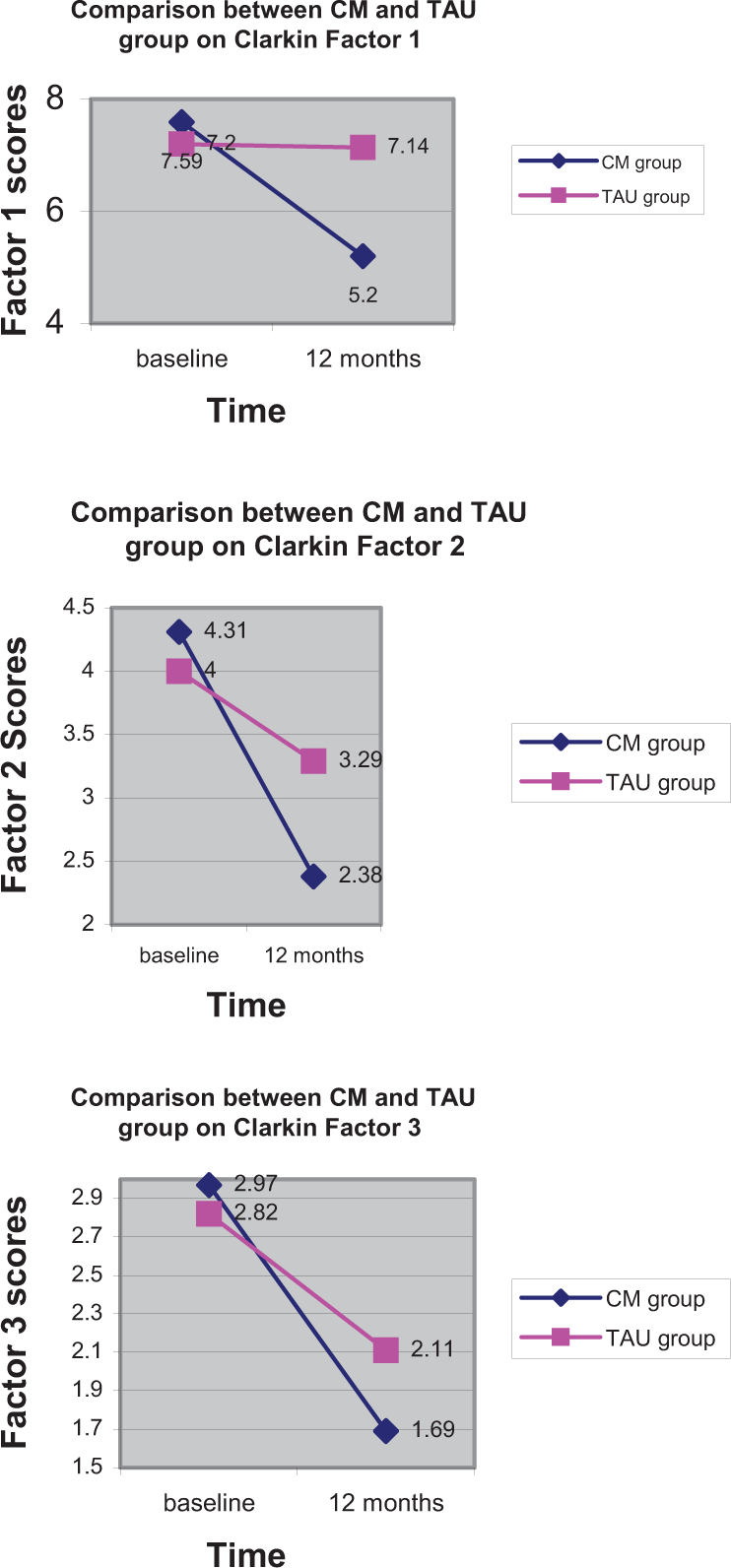
Changes in BPD Factors of 1. Self, 2. Emotional Dysregulation, 3. Impulsivity over one years treatment by two different forms of treatment, Conversational Model (CM) and Treatment as Usual (TAU).
Complex structure comparison
Complex 1: self
A repeated measures ANOVA was performed on Complex 1 with one within-subject factor: time (2 levels: baseline, 12 months) and one between subjects factor: group (2 levels: therapy group, TAU).
Overall there was a significant main effect for time between baseline and 12 months therapy (Wilks’ Lambda = 0.891, F(1,55) = 6.72, p = 0.012), and there was a significant interaction between time and group (Wilks’ Lambda = 0.858, F(1,55) = 9.13, p < 0.004).
This finding was then explored further by looking at each group separately over time. The repeated measures ANOVA revealed a highly significant clinical improvement over the 12 months for the therapy group (Wilks’ Lambda = 0.697, F(1,28) = 12.164, p < 0.002). In comparison the TAU group showed no statistical significance (Wilks’ Lambda = 0.995, F(1,27) = 0.136, p = 0.715).
Complex 2: affect dysregulation
A repeated measures ANOVA was performed on Complex 2. Overall, there was significant main effect for time between baseline and 12 months therapy (Wilks’ Lambda = 0.659, F(1,55) = 28.4, p < 0.001), and a significant interaction between time and group (Wilks’ Lambda = 0.902, F(1,55) = 5.95, p < 0.02).
This finding was then explored further by looking at each group separately over time. The repeated measures ANOVA revealed a highly significant clinical improvement over the 12 months therapy group (Wilks’ Lambda = 0.502, F(1,28) = 27.785, p < 0.001) but the TAU group also showed a significant improvement (Wilks’ Lambda = 0.854, F(1,27) = 4.61, p = 0.041).
Complex 3: impulse
A repeated measures ANOVA was performed on Complex 3. Overall, while there was a significant main effect for time between baseline and 12 months therapy (Wilks’ Lambda = 0.619, F(1,55) = 33.91, p < 0.001), there was no significant interaction between time and group (Wilks’ Lambda = 0.953, F(1,55) = 2.7 p = 0.106. Both groups improved at more or less the same rate.
The findings for the complexes outcomes are displayed in Figure 2.
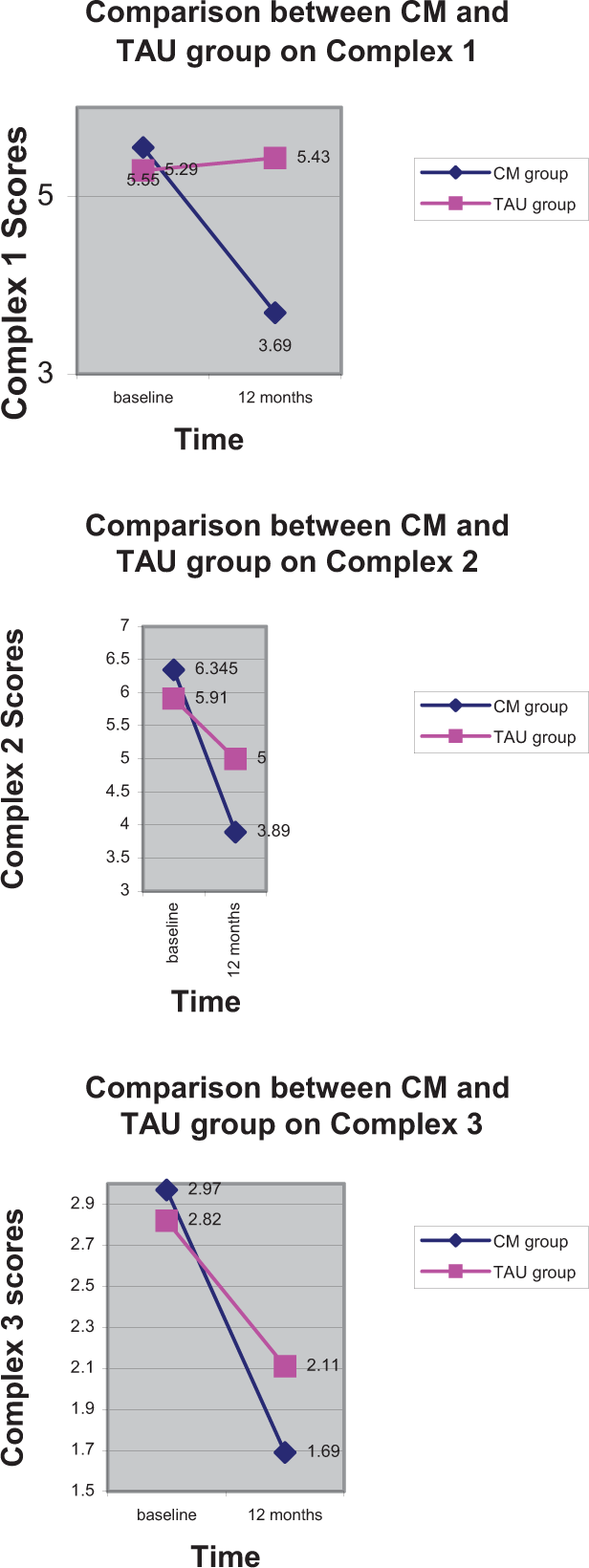
Changes in BPD complexes of DSM-IV criteria 1. Self, 2. Emotional Dysregulation, 3. Impulsivity over one years treatment by two different forms of treatment, Conversational Model (CM) and Treatment as Usual (TAU).
Correlations between Zung, factors and complexes
In order to explore the relationship between symptom change on the depression scale of Zung and the changes we have observed on the factors and complexes we created new variables, the Zung change score, by subtracting baseline Zung scores from the Zung score at 12 months, and created similar change scores for the three factors and three complexes in the same manner.
We correlated the Zung change with factor and complex changes for the TAU and CM groups separately. For Factor 1 a moderate positive correlation was found for the CM group, (Pearson correlation r = 0.481, p = 0.013), but no significant relationship for the TAU group (Pearson correlation r = −0.185, p = 0.398). For Factor 2 again a moderate positive correlation was found for the CM group, (Pearson correlation r = 0.476, p = 0.014), but no significant relationship for the TAU group (Pearson correlation r = 0.24, p = 0.269). For Factor 3 a stronger positive correlation was found for the CM group, (Pearson correlation r = 0.594, p = 0.001), but no significant relationship for the TAU group (Pearson correlation r = −0.299, p = 0.166).
A similar pattern was seen for the complexes. The CM group showed moderate positive correlations for Complex 1 (Pearson correlation r = 0.459, p = 0.018) and Complex 2 (Pearson correlation r = 0.49, p = 0.011) and a stronger positive correlation for Complex 3 (Pearson correlation r = 0.594, p = 0.001), while for the TAU group no significant relationships were found, Complex 1 (Pearson correlation r = −0.17, p = 0.438); Complex 2 (Pearson correlation r = 0.109, p = 0.621); Complex 3 (Pearson correlation r = 0.299, p = 0.166).
Discussion
Since the cardinal feature of personality disorder is endurance, those phenomena which persist over time can be seen as the core, or the essence, of the condition. This study shows that the groupings of DSM criteria making up Clarkin et al.'s Factor 1, which concern ‘self’, endured with unchanged severity over a period of one year in a TAU cohort of BPD patients. On the other hand, Factors 2 and 3, improved significantly over the period of a year. Factor 2 reflects emotional dysregulation, while Factor 3 measures impulsivity.
Treatment with the Conversational Model produced a different outcome picture for this cohort of patients. Factor 1 (self) improved significantly over a year. Factor 2 (affect dysregulation) also improved significantly, and significantly more, than those in the TAU cohort. Factor 3 (impulsivity) improved significantly but not significantly more than those in the TAU cohort.
The theoretically derived complexes of BPD criteria provided outcomes indistinguishable from Clarkin's factors. Accordingly, the discussion will be confined to those groupings of BPD phenomena created by factor analysis.
The TAU findings suggest that a measure reflecting a disturbance of self is the enduring aspect of the DSM diagnosis of BPD. They give support to the view that a constellation of phenomena related to such a disturbance is at the core of borderline pathology. The other groupings of DSM criteria which do not persist in severity over one year mainly describe disturbances of emotion and impulse regulation. This distinction between two groupings of phenomena, based on their relative endurance, gives rise to a demarcation between two zones of BPD symptomatology, one relating to self and the other to regulation. Such a division resonates with the two-component conception of Livesley [36].
The second aspect of this study concerned the chronic dysphoria which characteristically accompanies the diagnosis of BPD. This is an atypical depression having a number of different facets [34]. The findings, although not clear-cut, support the supposition that typical depression is not at the core of BPD. Our observations suggest that scores for typical depression do not correlate particularly with the constellation of features which emerge as the core of BPD in this study. Changes in the scores on a self-report scale for depression, which correlates well with the BDI, were more closely related to changes in the impulsivity factor than the self factor.
The atypical depression of BPD is likely to include the experience of emptiness, one of the ‘self’ grouping of criteria making up the core of BPD. Westen and his colleagues [34] found that the depression associated with BPD is qualitatively distinct and characterized by loneliness, desperation in relation to attachment figures, and a labile, diffuse negative affectivity. In a later paper, Westen, with his colleague Zittel Conklin, added to this inventory of the characteristics of the affect at the core of BPD the quality of intense psychological pain [37]. In this, they resonated with the view of Zanarini and her colleagues [32] who also consider that a characteristic dysphoria which they had termed ‘psychic pain’ is at the core of the borderline syndrome.
Since our findings suggest the self factor can be considered the core of BPD it should be a focal point concentrating future attempts to develop optimal care in this condition. Such a development demands a better elaboration of the nature of that system of phenomena relating to self. Unlike affect dysregulation and impulsivity, which can be behaviourally defined, the self system, as identified in a skeletal manner by DSM criteria, depends upon subjective factors, notably emptiness and so-called ‘identity problems’. Emptiness has already been touched upon. ‘Identity problems’ require a somewhat larger consideration.
The criterion in DSM which is framed as ‘identity disturbance’ is ambiguous since it is described in terms of self, as if identity and self are synonyms. They are not. In simplest terms, the distinction between identity and self can be seen as the difference between the individual's public reality and private experience. In ordinary healthy living, self and identity are seamlessly connected. Janus-like, they metaphorically face in opposite directions. Identity concerns the individual's relationship with his world. It involves a sense of place within family, profession, religion and other social groups. It is composed of roles, personal attributes, and conceptions of who one is in relation to others. Self, as William James described it, is categorically different. It is that flux of images, sensations, feelings, memories, imaginings and so forth which James likened to a stream. Here the focus is inward. The cardinal feature of self is a reflective awareness of inner events. The reflective process, James wrote, enables us ‘to think ourselves as thinkers’ [38, p. 296]. It brings with it a conception of ‘innerness’ [39] from which we derive a realization that certain experiences are uniquely our own.
The self aspect of the self-identity complex might be the more fundamental. The philosopher Owen Flanagan, for example, states that ‘the senses of identity, direction, agency and life plan are all grounded in the memorable connections of the stream’ [40, pp. 166–167].
The nature of the self-identity complex in borderline personality has been investigated by Wilkinson-Ryan & Westen [41]. Focusing on the concept of identity, they collated items from a number of authoritative sources [42–47] which included Westen's own work [48,49], in order to reach a definition of identity in BPD. From these items they constructed an instrument of 35 indicators of identity disturbance. Patient groups composed of BPD patients (N = 34), those having another personality disorder (N = 20), and no personality disorder (N = 41) were scored on these items. A factor analysis was then conducted on these scores. It produced four main factors. They were: 1: role absorption; 2: painful incoherence; 3: inconsistency; 4: lack of commitment. These four factors were used to distinguish between subjects with borderline personality disorder and those without borderline personality disorder. There were important differences between the predictive powers of the four factors. The investigators noted that ‘the weakest of the four factors in predicting borderline personality was the fourth, lack of commitment. This may be an important finding, given the heavy emphasis most identity research (as well as DSM-IV) has placed on this construct. For example, DSM-IV describes identity disturbance in borderline personality disorder as being ‘characterised by shifting goals, values, and vocational aspirations’ (p. 651). Their data showed that although this factor is a central component of identity disturbance, it does not distinguish borderline personality disorder from other types of psychopathology. ‘Painful incoherence’ was strongly related to borderline personality after controlling for both histrionic features and a history of sexual abuse. Sexual abuse was largely uncorrelated with the other three identity factors.
The findings of this study tend to suggest that, rather than disturbance of identity as usually defined, what is central to borderline personality is a painful sense of personal incoherence. Westen's ‘painful incoherence’ factor is very like an expanded version of Clarkin et al.'s ‘self’ factor. The Westen factor is made up of emptiness; a fear that personal existence would end if a close relationship were lost; and a number of items relating to experience of self (unreality, lack of continuity, and an indeterminate sense of ‘who one's self is’). ‘Painful incoherence’ better describes the ‘identity problems’ of BPD than the three or four DSM criteria relating to this system. The term encompasses psychic pain and implies a fragmentation of personal existing which can be seen as the fundamental form of the dissociative experience [50]. Unreality and lack of personal continuity are cardinal features of the dissociative taxon of Waller Putnam and Carlson [51]. Personality fragmentation, resembling dissociation, as a central feature of BPD has also been demonstrated by Wildgoose et al., 2000 [52].
A difficulty is posed by the suggestion that a grouping of features around ‘self’ is the core of the BPD syndrome. Without the dysregulation features, BPD cannot be diagnosed. Dysregulation is an essential part of the BPD picture. A resolution of the difficulty might be achieved in the following way.
It may be that a failure of self sets off, or triggers, excessive dysregulation in individuals who are genetically predisposed. It is generally supposed that the dysregulation features are more genetically determined than the self features, as suggested by Siever et al., [53]. The neurophysiology of dysregulation, however, goes beyond genetic influences. Disruption of the self system is likely to lead, in itself, to a failure of higher order, pre-frontally connected inhibitory mechanisms [54]. This effect would be likely to exacerbate a pre-existing tendency to disinhibition and dysregulation. This formulation has the self component as the primary deficiency in BPD, with both components conceived as ‘core’.
Fragmentation, or what he called a failure of personal synthesis, was central to Janet's concept of dissociation. In essence, he was putting forward a ‘disintegration’ theory [55, p. 40]. The modern concept of dissociation, however, is more complex, consisting of two main factors, one involving fragmentation and the other what Holmes et al. [56], in their review of the various ways now used to conceive dissociation, called ‘compartmentalization’. Following Janet, fragmentation is the main component of dissociation. A measure of fragmentation correlates with a scale reflecting current concepts of dissociation [46]. Skodol et al. [57] note that the addition of the ninth criterion to the DSM criteria of BPD in DSM-IV, dissociative symptoms and paranoid ideation, have ‘excellent specificity, i.e. rarely occur in other diagnostic groups’.
The issue of fragmentation leads us to a consideration of the form of relatedness making up the third element of the self complex. The concept of fragmentation implies a number of shifting self states in BPD. Each one is necessarily part of relationship. This idea suggests that in BPD forms of relatedness are relatively unintegrated, so that the individual shifts between various forms of relatedness, in an unstable manner, as implied in the fourth criterion of Clarkin's self factor.
The kinds of relationship which are an aspect of a fragmented self system are multiple, extending beyond that involving abandonment fears. Studies of the relationships represented in memory in BPD usually involve the child-victim pole of the relationship leaving implicit the characteristics of the other. Using the notion of schemata, Young et al. [58], Johnston et al. [59] found in 30 BPD patients that the ‘angry and impulsive child’ and ‘abandoned and abused child’ modes uniquely predicted dissociation scores, consistent with the concept of fragmentation. Other characterizations of the typical forms of relatedness in BPD include the ‘anaclitic relatedness’ and ‘self-criticism’ [60,61], and ‘hostile-helpless’ [62].
Finally, this study is of a preliminary kind, offering directions for future research. It has a number of limitations. The most significant is imposed by the use of DSM criteria to explore issues of extreme complexity. In particular, the criteria relating to the self component are inadequately described in DSM. Furthermore, the dichotomized method of scoring DSM features in this study is coarse-grained and does not reflect the severity of the symptom. The method may be compared with that used in other studies, e.g. Torgersen et al. [63], and Aggen et al. [13] in which the items were scored as 0 = not present; 1 = sub-threshold; 2 = present; 3 = strongly present. ‘Strongly present’ was a rarity. Taylor and Reeves [12] used a three-point scale.
The naturalistic randomization method used in this study might also be seen as a limitation. Its outcome, however, was satisfactory in that it achieved the aim of standard randomization methods. The CM and TAU groups did not differ in symptom severity or demographically.
Despite these drawbacks, however, the main finding seems clear. Two groupings of DSM criteria are distinguished in terms of their endurance, leading to the inference that the self system is the more fundamental disturbance of the two. Such an inference has significant implications for the refinement and elaboration of current approaches to the treatment of BPD.
Footnotes
Acknowledgements