
Abstract
Hospital-treated deliberate self-poisoning (DSP) is common. In Australia, up to 5% of all general hospital admissions are for the treatment of an episode of DSP [1]. Psychiatric disorder is common in hospital treated DSP patients. In a population of hospital-treated deliberate self-harm (DSH) patients in the UK, mood disorders were reported in 72% and personality disorder in 45.9% of patients [2], suggesting that these are commonly encountered diagnoses in DSH populations. Although there are clinical practice guidelines which outline management of DSH in general [3], [4], or for borderline personality disorder (BPD) patients in particular [5], these studies make few specific recommendations for psychiatric care after discharge from the general hospital. Guidelines such as these are typically determined by processes that include systematic reviews of the literature, expert panel opinion and surveys of what clinicians
There are several reasons to suspect that the management of hospital-treated DSP patients with BPD and major depressive disorder (MDD) could be different. Three important possibilities are:
1
2
3
Consequently, the objective of this paper is straightforward, to compare the clinical management of hospital-treated DSP subjects with MDD or BPD in a well-established regional general hospital service, after controlling for demographic factors and level of suicide ideation.
Method
Setting
The Hunter Area Toxicology Service (HATS) is a regional toxicology unit situated at the Newcastle Mater Hospital serving a population of 385 000 adults and is a tertiary referral centre for a further 170 000. All poisoning presentations to emergency departments in the region are either admitted to this unit or notified to HATS and entered prospectively into a clinical database [18]. The Consultation-Liaison Psychiatry Department sees all DSP patients for psychiatric assessment, diagnosis, and to determine discharge destination and follow-up. Clinical diagnoses are made according to DSM-IV [19] by psychiatric registrar, clinical nurse consultant or consultant psychiatrist, and all cases are reviewed at a weekly meeting before final entry in the HATS database [7]. A preformatted admission sheet is used by medical staff to collect data during admission [20] and additional data from the medical record is entered into the database by two trained personnel blinded to any study hypotheses.
Sample
A cohort of sequential hospital-treated DSP patients was identified from the HATS database for the period 1996–2002 with the first episode of DSP during that period used as the index admission for all selections and analyses (n = 3160). From this group was selected any patient whose DSM-IV diagnosis was MDD (n = 974) or BPD (n = 332). Patients with a comorbid diagnosis of adjustment disorder, or ‘other conditions that may be a focus of clinical attention’, were retained for analysis but any other comorbid axis I or axis II disorders were excluded, since these other disorders could effect treatment decisions, and understanding the clinical management of these two diagnoses was the aim of this study. This left a sample of 639 patients (MDD n = 484, BPD n = 116, both MDD/BPD n = 39). Of these subjects, complete data was available for 570 subjects, which were used in the multivariate analyses in this study.
Independent and dependent variables
There were five independent variables of interest: gender; age; and marital status (all of these were self-report measures drawn from the clinical record); strength of suicidal ideation at the time of psychiatric assessment (a clinical assessment on a 6-point (0–5) semantic differential scale); and DSM-IV diagnostic group (MDD, or BPD, or both BPD/ MDD based on clinical assessment by psychiatric staff). Suicidal ideation was stratified into three categories for analyses: 0 = no suicidal ideation; 1–3 = mild to moderate ideation; and 4–5 = high suicidal ideation. Four dependent variables (i.e. outcomes) were modelled: (i) length of stay (LOS) in the general hospital, classified as ≤ 24 hours; (ii) discharge to a psychiatric hospital for after-care; (iii) any arranged psychiatric follow-up in the community for those discharged to home; and (iv) any arranged follow-up with GPs for those discharged to home. Subjects discharged to home could be referred to either psychiatric community based services, GPs or both for follow-up.
Analyses (multivariate)
For each of the binary-dependent variables above, a hierarchical logistic regression model was developed, using forced entry and three fixed levels of independent variables: demographic factors; suicidal ideation; and diagnostic group. The structure of these models ensured that for each dependent variable the model first statistically controlled for the selected potential confounders (i.e. demographic factors, then suicidal ideation), and then tested the effects of diagnostic group on the dependent variable. Subjects were excluded from these multivariate analyses if they had any missing data. This resulted in an overall sample of 570 subjects, whose data were used to model two separate outcomes: general hospital length of stay; and discharge to a psychiatric hospital. There were 350 subjects discharged to home, whose data were used to model two further outcomes: any psychiatric outpatient or community service follow-up; and any GP follow-up. The threshold for statistical significance was set at p < 0.05 for all analyses.
Results
Sample characteristics
The characteristics of the 570 subjects used in the multivariate analyses are shown in Table 1. Of the 350 subjects discharged to home, 169 (48.3%) had follow-up arranged with the psychiatric community or outpatient services, 195 (55.7%) had follow-up arranged with a GP and 344 (98.3%) had follow-up arranged with at least one of these services.
Patient characteristics for the sample (n = 570)
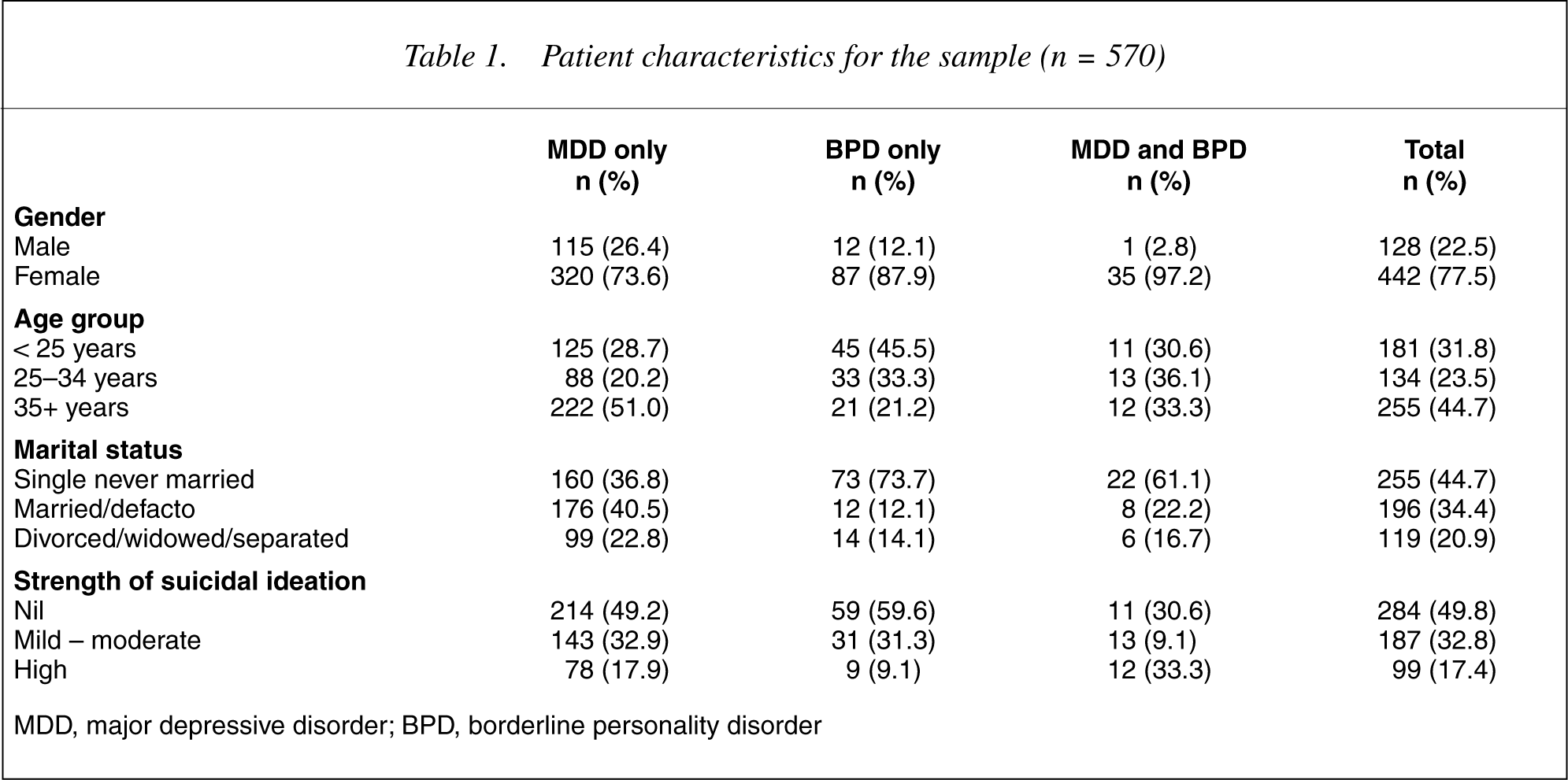
MDD, major depressive disorder; BPD, borderline personality disorder
Predictors of length of stay and referral
Tables 2 and 3 summarize the findings from the four hierarchical logistic regression analyses. In short, the logistic regression models showed:
1 General hospital length of stay was associated with older age (35+ years, adjusted OR = 1.94, 95% CI = 1.04–3.62) but was not associated with diagnostic status (see the left-hand columns of Table 2).
2 Discharge to a psychiatric hospital was associated with older age (35+ years, adjusted OR = 2.36, 95% CI = 1.30–4.27), level of suicidal ideation (mild to moderate, adjusted OR = 3.07, 95% CI = 1.98–4.76, high, adjusted OR = 43.58, 95% CI = 20.93–90.70), and diagnostic group (BPD, adjusted OR = 1.79, 95% CI = 1.01–3.18; comorbid BPD/MDD, adjusted OR = 2.51, 95% CI = 1.05–6.01) (see the righthand columns of Table 2).
3 Psychiatric follow-up arranged for those discharged to home was not associated with any of the independent variables (see the left-hand columns of Table 3).
4 GP follow-up arranged for those discharged to home was associated with age group (25–34 years, adjusted OR = 2.28, 95% CI = 1.20–4.35), and negatively associated with level of suicidal ideation (mild to moderate, adjusted OR = 0.6, 95% CI = 0.38–0.97; high, adjusted OR = 0.09, 95% CI = 0.01–0.72) and diagnostic group (BPD, adjusted OR = 0.44, 95% CI = 0.24–0.81) (see the right-hand columns of Table 3).
Predictors of: (a) general hospital length of stay >24 h; and (b) discharge to a psychiatric hospital (n = 570)
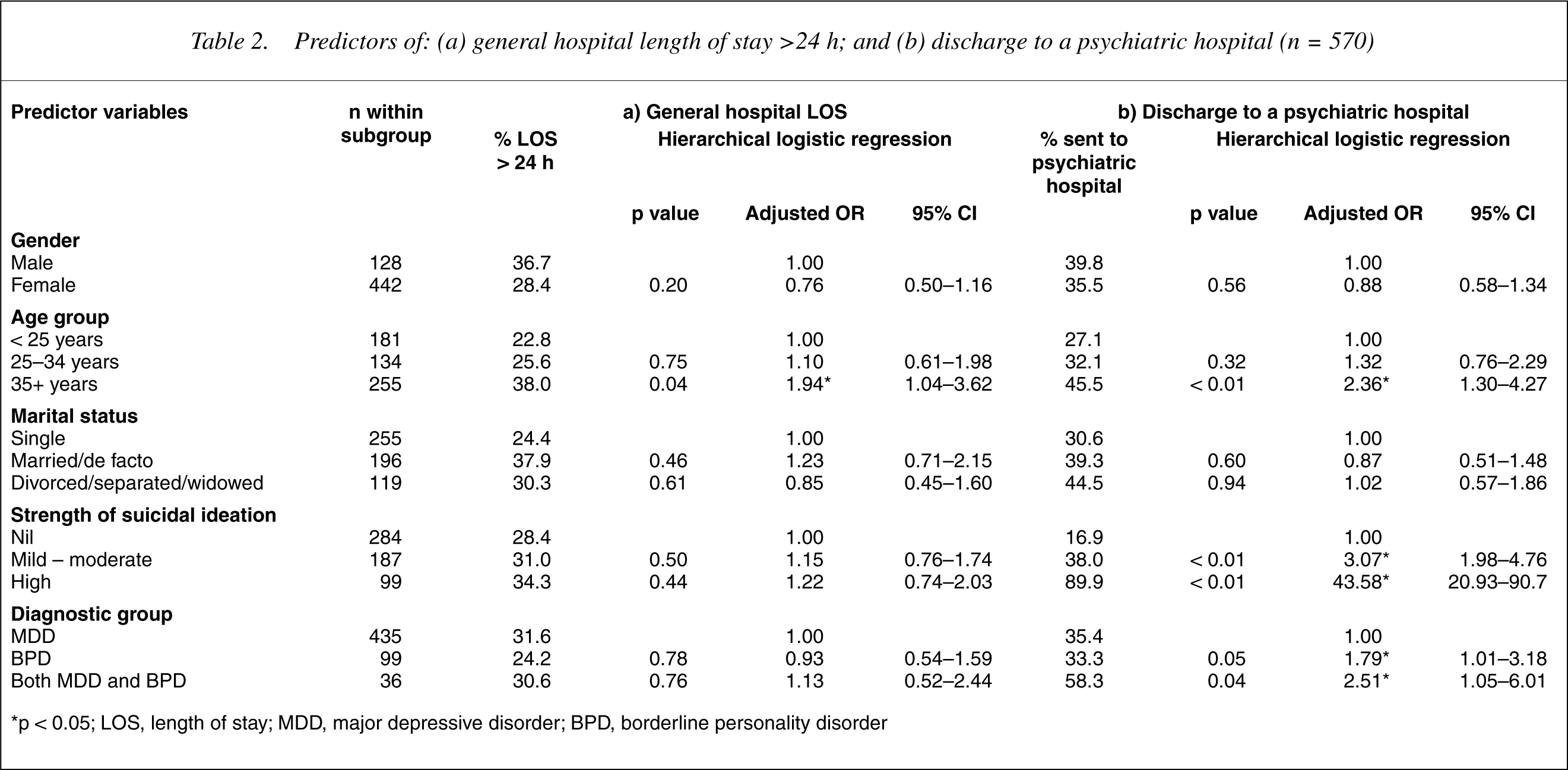
∗p < 0.05; LOS, length of stay; MDD, major depressive disorder; BPD, borderline personality disorder
Predictors of referral to: (a) psychiatric community services; and (b) General Practitioner, if discharged home (n = 350)
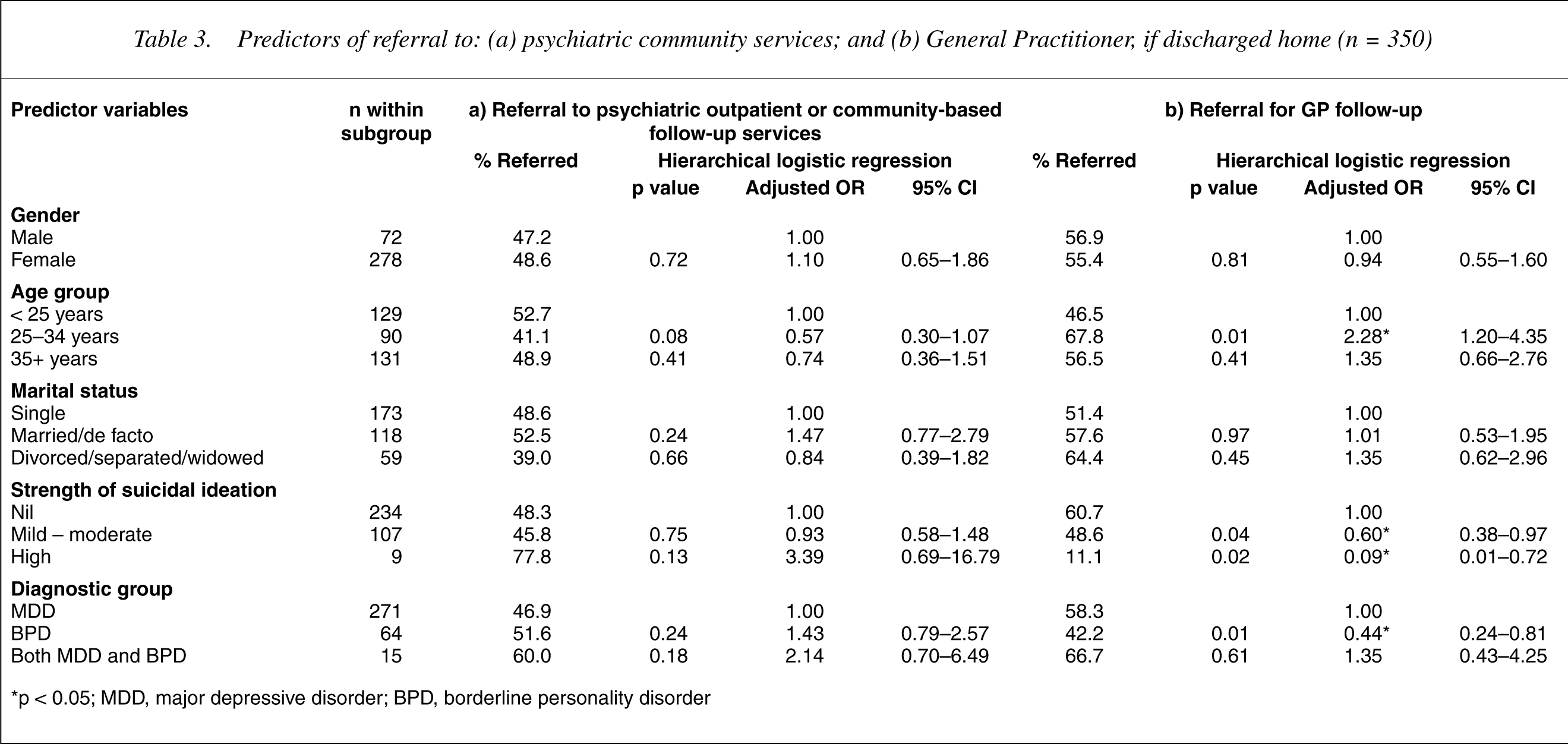
∗p < 0.05; MDD, major depressive disorder; BPD, borderline personality disorder
Discussion
Methodological issues
For the results of this study to be valid, it is necessary to consider possible biases and confounding. The subjects were consecutive patients drawn from a regional service and so ascertainment bias should be insignificant. Diagnosis assignment was by clinical assessment according to DSM-IV criteria. This is a substantially different procedure to the use of structured clinical interviews, which often yield higher rates of disorder, possibly reflecting the time-limited and prioritized nature of routine diagnostic assessments [21]. However, this should not necessarily involve any differential effect on diagnostic procedures for MDD or BPD [22]. Similarly, none of the other variables are likely to suffer from systematic differential measurement and so should not affect the calculation of odds ratios. Interrater reliability has been found to be modest for psychopathology, impulse control and disposition by other authors [23]. The four logistic regression models used the same structure, allowing for statistical control of common confounders, age, gender, marital status and strength of suicidal ideation. However, there may be other confounders of interest not addressed by the current analyses.
Several factors may influence the generalisability of these findings to other settings. The referral population from Newcastle and the Hunter Valley may not be similar to other areas or countries. Our clinical service provides a model of service delivery which may be unlike others [7] and has access to a full range of psychiatric care and GP services for all patients after discharge. Our study excluded major psychiatric comorbidity and only included hospital treated deliberate self-poisoning patients and so generalizability to other populations may not be warranted.
If the results are valid, how do the results help to advance the field? There have been attempts to develop evidence-based guidelines for the treatment of BPD [5], [6]. In Australia and New Zealand the methodology adopted involved a literature review, expert panel and a survey of clinicians reporting what they
Review of findings
Staff attitudes
It has been found that nurses [29] and psychiatrists [30] respond in negative ways to BPD patients which could influence their management. These attitudes have been characterized as less empathic, more rejecting, believing the patients to be less deserving of care and capable of controlling their own self-destructive impulses. If these attitudes were present and effecting management substantially in the HATS treated patients, we would have expected to see a shorter length of stay for BPD in the general hospital, less frequent referral for psychiatric hospitalization, less psychiatric after-care and less general practice after-care organized for those patients discharged to home. This was contrary to our results for three of the four outcomes modelled.
Length of stay in the general hospital
We believe length of stay may be a reasonable proxy measure for quality of medical care in the general hospital. If a differential approach to medical management was based on the diagnosis of MDD or BPD rather than the medical needs due to the toxicity of the self-poisoning episode, then this could result in differences in length of stay. Although we did not control for any possible differential pattern of poisoning or medical management strategies, it was reassuring to note that diagnostic group had no effect on the length of stay. Longer length of stay for older DSP subjects is consistent with previous findings [31] and probably due to the increased vulnerability of older subjects to the toxicity of the ingested drugs and the pattern of drug ingestion by older subjects. A post hoc examination of the subjects in the current study showed that 65% of subjects aged 55 years and over had a length of stay of greater than 24 h. In the current study less than a third of the subjects overall required a length of stay of over 24 h, which is consistent with the overall profile for the HATS unit, in that the median length of stay is around 16 h, a figure significantly less than that for comparator Australian hospitals [7].
Discharge to a psychiatric hospital
BPD and comorbid BPD/MDD patients were at higher risk for discharge to a psychiatric hospital than MDD after controlling for demographic factors and suicidal ideation. However, the raw percentages for those sent to psychiatric hospital (see Table 2) showed a lower proportion of BPD only patients compared to MDD patients. Further exploration of this finding showed that the weighted percentage of patients discharged to a psychiatric hospital after controlling only for the level of suicidal ideation was: MDD, 35.0%; BPD, 39.6%; and comorbid MDD/BPD, 46.2%. So, for subjects with a high level of suicidal ideation, discharge to the psychiatric hospital was similar for all diagnostic groups (MDD, 88.5%; BPD, 88.9%; and MDD/BPD, 100%). However, for mild to moderate suicidal ideation, BPD (45.2%) and co morbid MDD/BPD (46.2%) were more likely to be discharged to a psychiatric hospital than MDD subjects (35.7%) with the same level of suicidal ideation.
The prevailing philosophy within the HATS unit is that BPD patients may benefit from brief psychiatric hospitalization mainly for their short-term protection against suicidal risk, dangerousness to others, severe dissociation or psychotic phenomena. This is consistent with several of the recommended indications in the American Psychiatric Association Practice Guidelines [5]. The decision to recommend psychiatric hospitalization is probably a complex one involving many factors, not just protection from immediate suicidal risk although that may be very important. Other suicidal risk factors like previous self-harm/attempted suicide, previous inpatient psychiatric treatment or the presence of a suicidal plan [32] were not included in our analysis and may be confounders.
The differences in discharge destination may be due to lower levels of social support, availability or perceived unsuitability of psychiatric outpatient care, or the greater level of impulsiveness in the BPD group. The differences could be due to a more punitive or controlling attitude of psychiatric staff to BPD patients, or even a more benevolently protective or paternalistic attitude. It has also been suggested that more severe dissociation episodes that may occur in BPD may vitiate individual responsibility [33], and perhaps increase the likelihood of psychiatric hospitalization. BPD patients have also been reported to be at greater risk of lifetime psychiatric hospitalization than MDD patients (OR = 4.95, 95% CI = 2.79–8.77) [34]. This excess may be due in part, to the psychiatric hospitalization recommended after a DSP episode. In our study around a third of subjects were discharged to a psychiatric hospital, a similar rate to all DSP patients treated by HATS [35].
Psychiatric follow-up for those discharged home
There were no significant differences between the diagnostic groups in psychiatric follow-up. This suggests that among patients not sent to psychiatric hospital there is equal initial access to follow-up in the general and specialty psychiatric services. We did not undertake an analysis of the type of psychiatric services arranged. However, it has been reported that patients with BPD have greater lifetime use of a variety of psychiatric interventions than MDD patients [34].
GP follow-up for those discharged home
BPD (but not comorbid BPD/MDD patients), were less likely than MDD patients to have general practitioner follow-up arranged. This result invites several speculative explanations. It seems possible that BPD patients may be less likely to have a general practitioner or at least a steady relationship with a single practice, or that general practitioners are expected to be able to assess and manage depressive disorders adequately but not BPD. It has been reported that Australian GPs believe that they have a reasonable ability to recognize and treat depression [36]. It was also noted that patients with higher levels of suicidal ideation were less likely to have general practitioner follow-up arranged. More ‘difficult’ patients in a psychiatric sense may be seen as less suitable for general practice follow-up or may benefit from the specialized treatments available within the community based psychiatric services. However, BPD patients were referred to GPs at a substantial rate, which suggests that there is an expectation that GPs will be able to assist in the management of many BPD patients.
Conclusion
Overall, BPD patients were more likely to be referred for psychiatric admission on discharge and less likely to be referred to general practitioners if discharged to home. Both groups were referred equally to psychiatric services in the community if discharged home. These findings have implications for service planning and costs. In order to better understand the effect of clinical management strategies on subsequent suicidal behaviours, it would be necessary to examine variables like: the types of treatment provided by mental health services and GPS after the DSP episode, treatment compliance, LOS in psychiatric inpatient facilities, prescription of psychotropic medications and symptom resolution amongst others. These elements and the outcomes of further suicidal behaviours were beyond the scope of the current study but worth examination in future studies. However, further research questions raised by this study include the effect of comorbid psychiatric disorder on referral for psychiatric hospitalization, identification of subjects who actually receive the recommended psychiatric admission and an assessment of any effect that such an admission has on repetition of DSP or subsequent death by suicide.