
Abstract
Keywords
Over the last decade Australian mental health services have experienced a significant increase in demand, especially for acute inpatient care [1]. Many mental health professionals have argued that increased use of amphetamines has been a significant driver of this demand [2].
Amphetamines are associated with physical and psychological harm [3]. They may trigger episodes of acute psychosis in vulnerable individuals, and worsen symptoms in patients with pre-existing psychotic disorders [3–5]. However, Degenhardt and colleagues [6] have cautioned against overstatement of the extent of amphetamine related harm. They reviewed Australian drug use and health indicators to 2005–2006 and reported that health-related ‘indicators of meth/amphetamine-related harm did not show the dramatic increases that might have been expected given recent media attention, with indicators stabilizing over the past few years’ (p.250).
From 1993 to 2004 there was a five-fold increase in admissions to Australian hospitals with a primary diagnosis of drug-induced psychosis, increasing from 55 admissions per million population aged 10–49 to 253 admissions per million population [7]. Amphetamine-induced psychoses accounted for an increasing proportion of these admissions (55% in 2003–2004, up from 41% five years earlier). There have been several reports of increased amphetamine-related presentations to hospital emergency departments (ED) [8,9]. In New South Wales (NSW) the number of ED admissions for amphetamines and related substances increased 139% between 2002 and 2007 [10]. While proportionally large, these are increases from a low base rate, and specific amphetamine-related disorders remain a small percentage of overall mental health service or emergency department activity.
This study examines relationships between amphetamine availability and admissions for psychosis in NSW from 2000 to 2009. If amphetamines are a significant driver of changes in mental health service demand, then there should be a relationship between community availability of amphetamines and admissions for amphetamine-related mental health problems. Increased incidence of amphetamine-related episodes of psychosis is likely to result in increased admissions for psychosis. It is also likely to result in a change in the mix of persons admitted to inpatient units, increasing the acuity of those units by increasing the proportion of admissions that are due to psychotic disorders.
Arrests for drug possession have been shown to be a valid measure of community drug availability [11], although they are likely to be influenced both by supply factors (fluctuations in drug availability) and policing factors (changes in police resources and focus). A recent study [10] has shown a steady increase in amphetamine arrests in NSW over the last decade, and has also shown that over this same period arrests for narcotics and amphetamines were strongly correlated with emergency department presentations for problems related specifically to these drugs.
We hypothesize that greater community availability of amphetamines will be associated with an increase in admissions for stimulant use disorders (abuse, dependence, etc.) and stimulant-induced psychoses. In addition amphetamine use may lead to exacerbations of illness in individuals with schizophrenia or other psychotic disorders.
The diagnosis of specific drug-related conditions is often imprecise due to lack of recognition of the role played by specific drugs, or systematic under-recording of secondary or comorbid diagnoses even when they are clinically recognized. Therefore the current study also examines the relationship between amphetamine availability and admissions for non-drug-related psychoses.
This study aims to add to the existing evidence in several ways. Firstly, no published study has examined for a direct relationship between a measure of community amphetamine availability and admissions for mental health care. Secondly, Australian national hospital data collections include only a single ‘primary’ diagnosis for each admission. A study using a large state-based data collection can also examine additional ‘secondary’ or comorbid diagnosis. In routine mental health care, substance-related conditions are often recorded as secondary diagnoses, and therefore examination of these diagnoses may be more sensitive than examination of primary diagnoses alone. Thirdly, the most recent publication of an Australian time series [7] examines hospital admissions from 1993 to 2004, and changes in both drug availability and admissions for psychosis may have occurred since that time.
Methods
Data sources
Aggregated data was obtained from routinely collected crime and health datasets, and is used with permission of the relevant data custodians. No data on individual admissions or arrests was obtained.
Amphetamine supply
Amphetamine supply data was provided by NSW Bureau of Crime Statistics. This comprises the total number of ‘criminal incidents’ of amphetamine possession and/or use detected by or reported to NSW Police, and recorded in the NSW ‘COPS’ database. ‘Criminal incidents’ differ from arrests in that they also include cautions and individuals diverted from court through use of infringement notices or youth justice conferences. Criminal incidents of amphetamine dealing and supply are not included in this analysis as these are smaller in number, more variable and are likely to be more influenced by policing rather than supply factors. It is also possible that substantial amphetamine seizures for possession or supply could be a cause of reduced community drug availability rather than a marker of increased availability.
Demand for mental health care
Mental health admissions data was extracted from Inpatient Statistics Collection, NSW Health Information Exchange (HIE). It included all same day and overnight episodes of inpatient care where the person was aged 14–65 and admission occurred to a designated acute adult mental health unit in NSW. Specialist acute child and adolescent mental health units (CAMHS) were not included because of difficulties in separation of mental health from general medical admissions at several hospital sites. The study focuses on admission for acute or emergency care from community settings where exposure to amphetamines may have been a risk factor and where the timing of admission to a mental heath unit could be influenced by that exposure. Therefore the following were excluded: (i) psychogeriatric units, non-acute adult and non-acute CAMHS units; (ii) acute adult units with a specialist or tertiary role (e.g. forensic units, neuropsychiatry units, day programmes, ECT); (iii) admissions following transfer from another hospital, a nursing home or due to statistical type-change within a facility; and (iv) episodes where greater than one week elapsed between admission to hospital and transfer to an acute mental health unit. Admissions to psychiatric emergency care centres (PECCs) were included.
Diagnosis
NSW Health inpatient data records primary and additional ICD-10 diagnoses for all inpatient episodes. ICD includes amphetamines within stimulant use disorders (F15). ICD-10 introduced coding of a fifth digit to specify methamphetamine within these disorders. However, this additional coding was present in only a minority of records and has not been examined. Diagnosis codes were grouped into three broad diagnostic groupings: stimulant use disorders, stimulant-induced psychoses and non-drug-related psychoses (see Table 1).
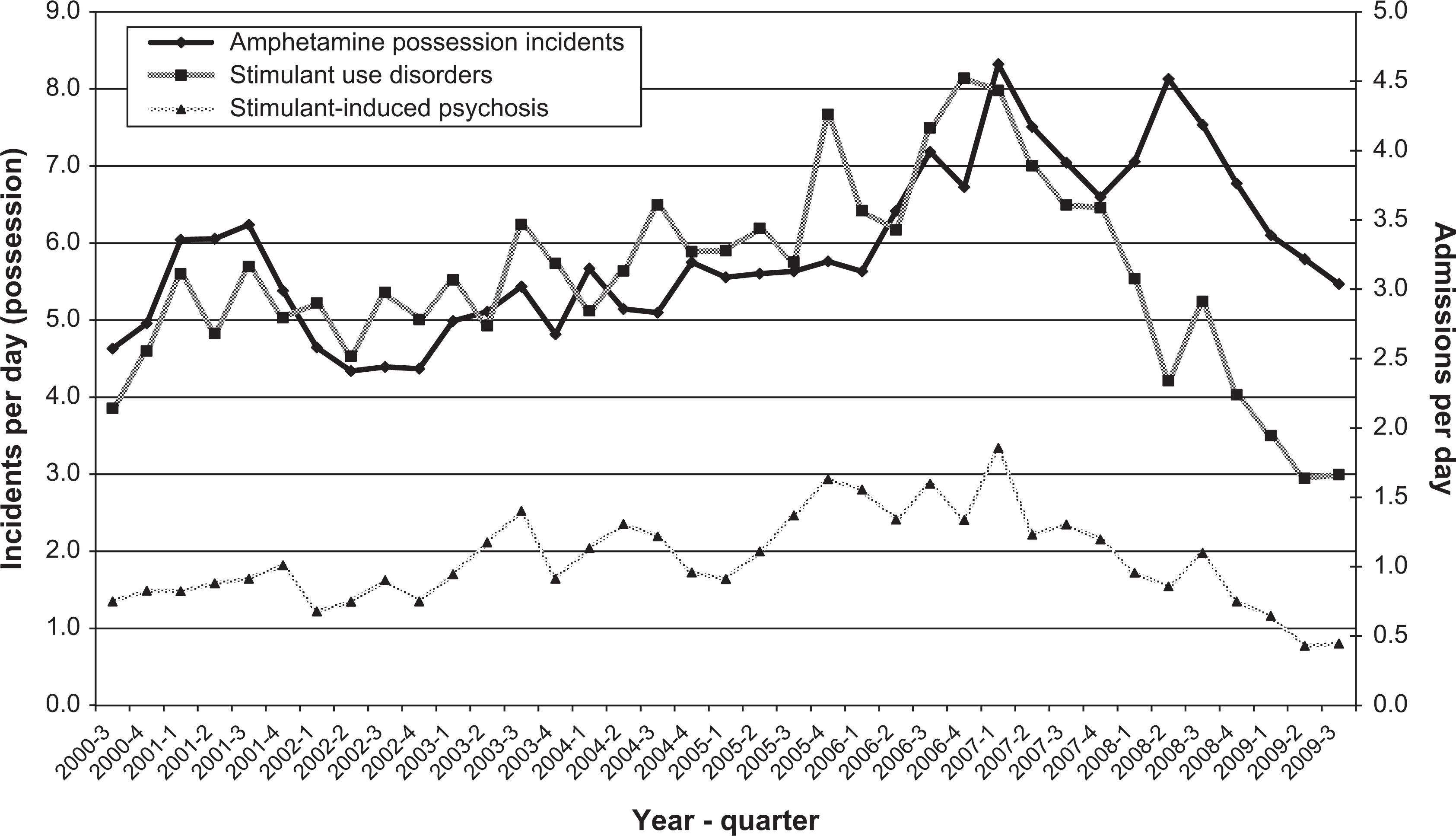
Amphetamine possessions and admissions for stimulant-related disorders, 2000–2009.
Mapping of ICD diagnostic codes
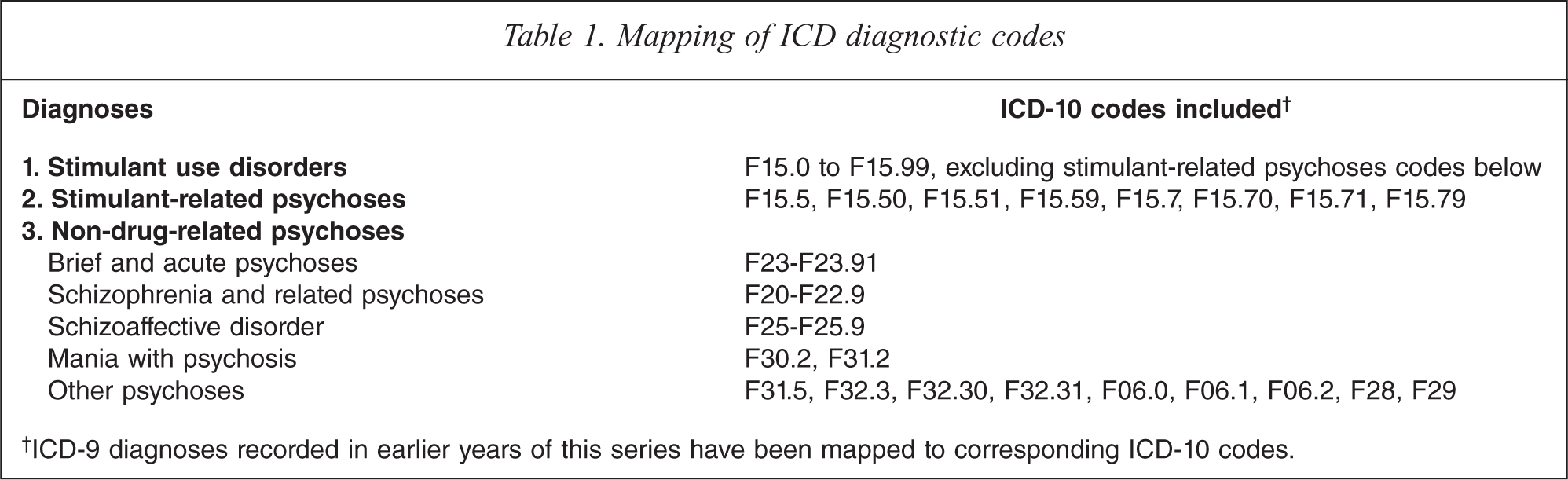
†ICD-9 diagnoses recorded in earlier years of this series have been mapped to corresponding ICD-10 codes.
For each admission, each diagnosis of interest was recorded as present if it occurred as either a primary or an additional diagnosis. The unit of counting was the hospital episode, not the diagnosis. More than one diagnosis of the same group was often made in a single episode: for example, many episodes recorded more than one diagnosis in the stimulant use disorders group (e.g. stimulant intoxication and stimulant dependence). These were counted as a single episode with amphetamine use disorders rather than as two episodes.
Time period and incident/admission rates
Monthly data for both sources was available from June 2000 to September 2009 inclusive. Monthly data were aggregated to produce quarterly rates. As quarters differ in length, amphetamine incident and admissions data were calculated using daily rates (quarterly total/days in quarter).
Over the period studied there was a 34% increase in public mental health beds in NSW, increasing from 1861 beds in July 2000 to 2491 beds in July 2009 [12–13]. Over the same period there has been an overall upward trend in amphetamine arrests in NSW.
Analysis
The major independent variable (amphetamine possession) was examined to exclude seasonal effects: dummy variables were created for quarter (1–4) and sequence (1–37), and a linear regression calculated for predicted amphetamine possession over time. Variance on the distribution of residuals was analysed (one way ANOVA, factored by quarter). There were no significant differences between quarters (F = 0.17, df = 36, p = 0.916). Therefore subsequent analyses did not consider possible seasonal effects.
Linear regression was conducted separately for each of the three major dependent variables: (i) admissions with stimulant use disorders, (ii) admissions with stimulant-related psychoses; and (iii) admission with non-drug-related psychosis (i.e. schizophrenia, brief psychoses, schizoaffective disorders, mania).
Initial data analysis and descriptive statistics were conducted using PASW Statistics version 18 (Chicago: SPSS). Regression analyses were conducted using STATA (StataCorp. 2009. Stata Statistical Software: Release 11. College Station, TX: StataCorp LP).
Results
Summary data
Data was obtained for 111 months (37 quarters) from July 2000 to September 2009. In this period there were 19 897 incidents of amphetamine possession or use recorded.
In the study period 187 161 admissions to acute mental health units met the inclusion criteria for the study, of which 90 296 (48%) included at least one primary or secondary diagnosis of psychosis. Diagnoses of non-drug-related psychoses (82 684, 44% of admissions) were more frequent than drug-related psychoses (10 167, 5% of admissions). There were 10 423 admissions with a stimulant use disorder recorded, comprising 5.6% of all admissions. There were 3557 stimulant-induced psychoses recorded (1.9% of admissions).
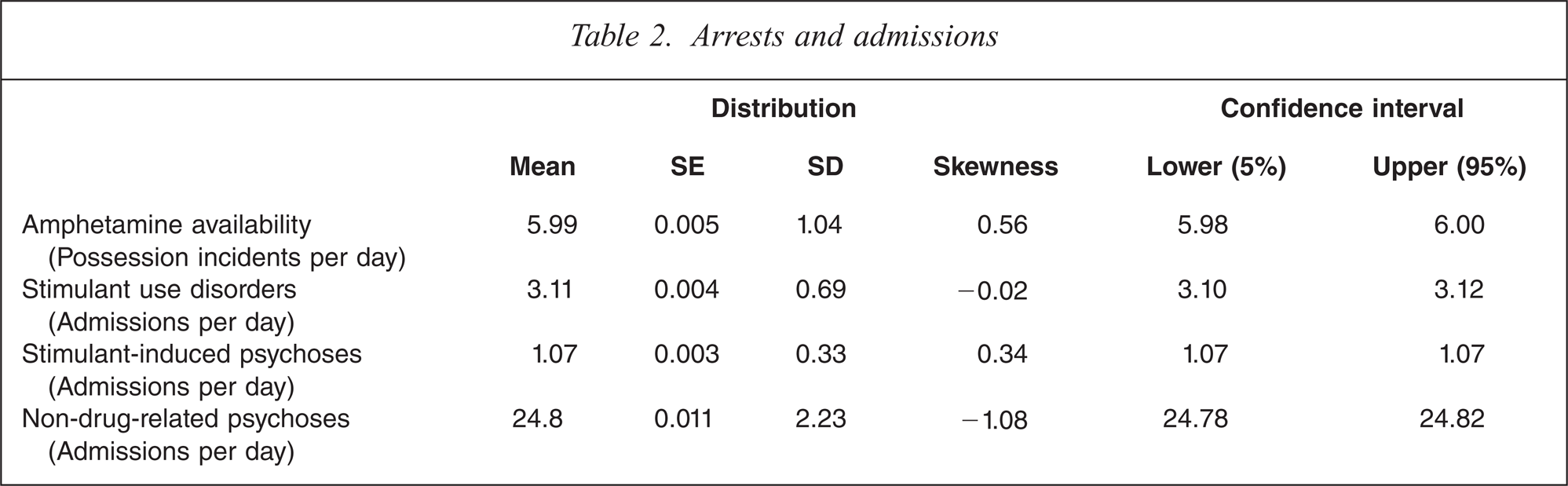
Table 2 summarizes the main dependent and independent variables.
Arrests and admissions
Trends over time
Figure 1 shows trends in amphetamine possessions and amphetamine-related admissions. Amphetamine possessions increased from 2002, peaking in the first quarter of 2007. There has been an overall downward trend since 2007, with an apparent steady decline since that time. Stimulant-induced psychoses and stimulant use disorders appear to follow a similar trend to amphetamine possessions, with an overall gradual increase from 2002 to 2007 but a consistent decline from a peak in early 2007; rates in the first three quarters of 2009 are between one third and one quarter of those recorded in late 2006 and early 2007.
Admissions for non-drug-related psychosis are more frequent and have less variability. They appear to show a similar but less marked trend, with an apparent reduction of around 20% in admission rate since early 2007 (See Figure 2).
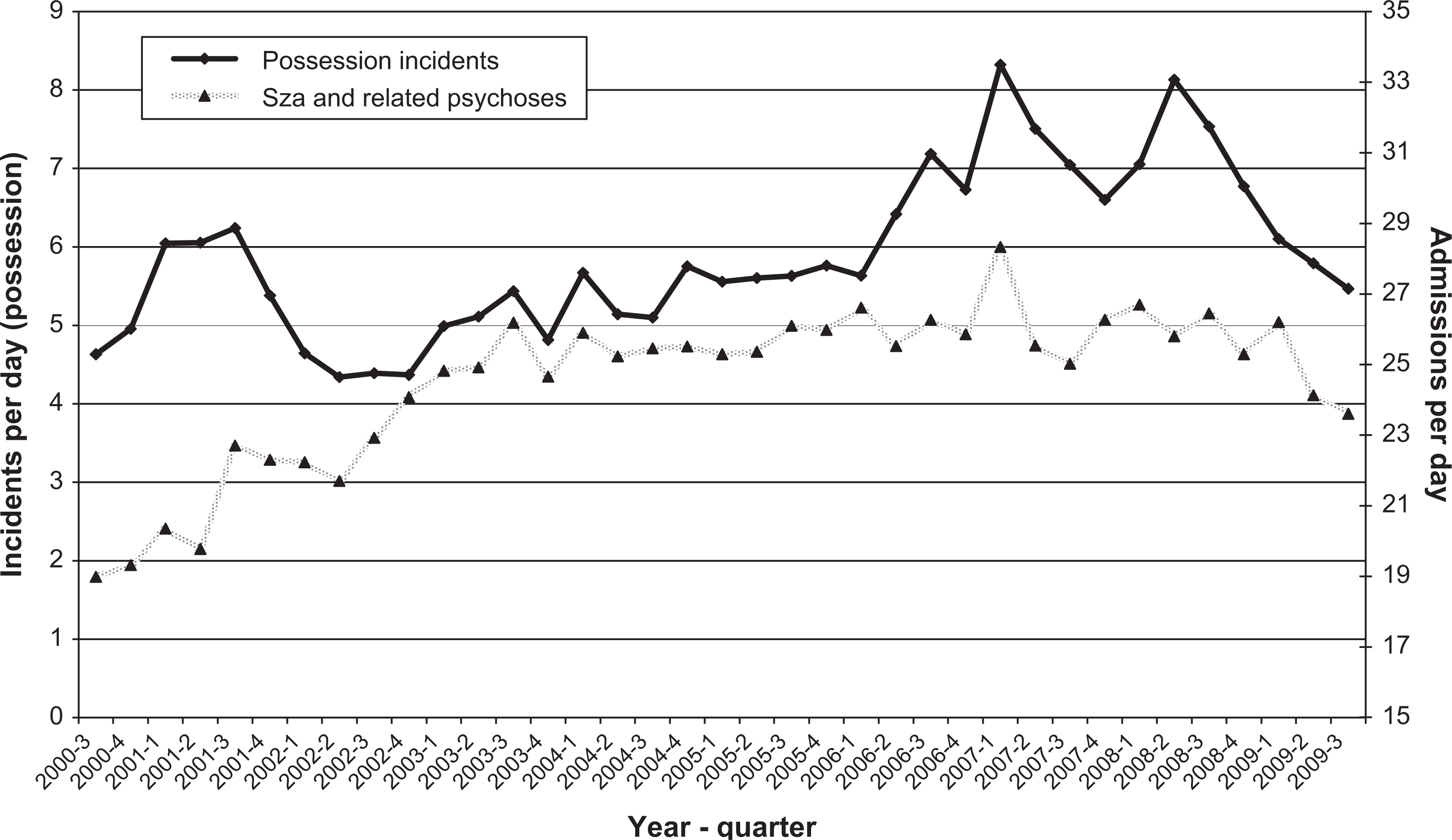
Amphetamine possessions and admissions for schizophrenia (Sza) and related psychoses, 2000–2009.
Analysis of admission rates over this period is complicated by an increase in acute mental health beds in NSW over the period being studied, largely due to the construction of new acute beds. For the acute units in scope for this study, average occupied beds rose steadily from 682 at the beginning of the period to 1114 in the third quarter of 2006 (See Figure 3). The increase has not been constant over the period examined: since late 2006 average occupied beds in the units included in this study have levelled off, fluctuating between 1114 and 1069 occupied beds. A small proportion of this increase in occupied beds may also have been due to increasing occupancy of existing units.
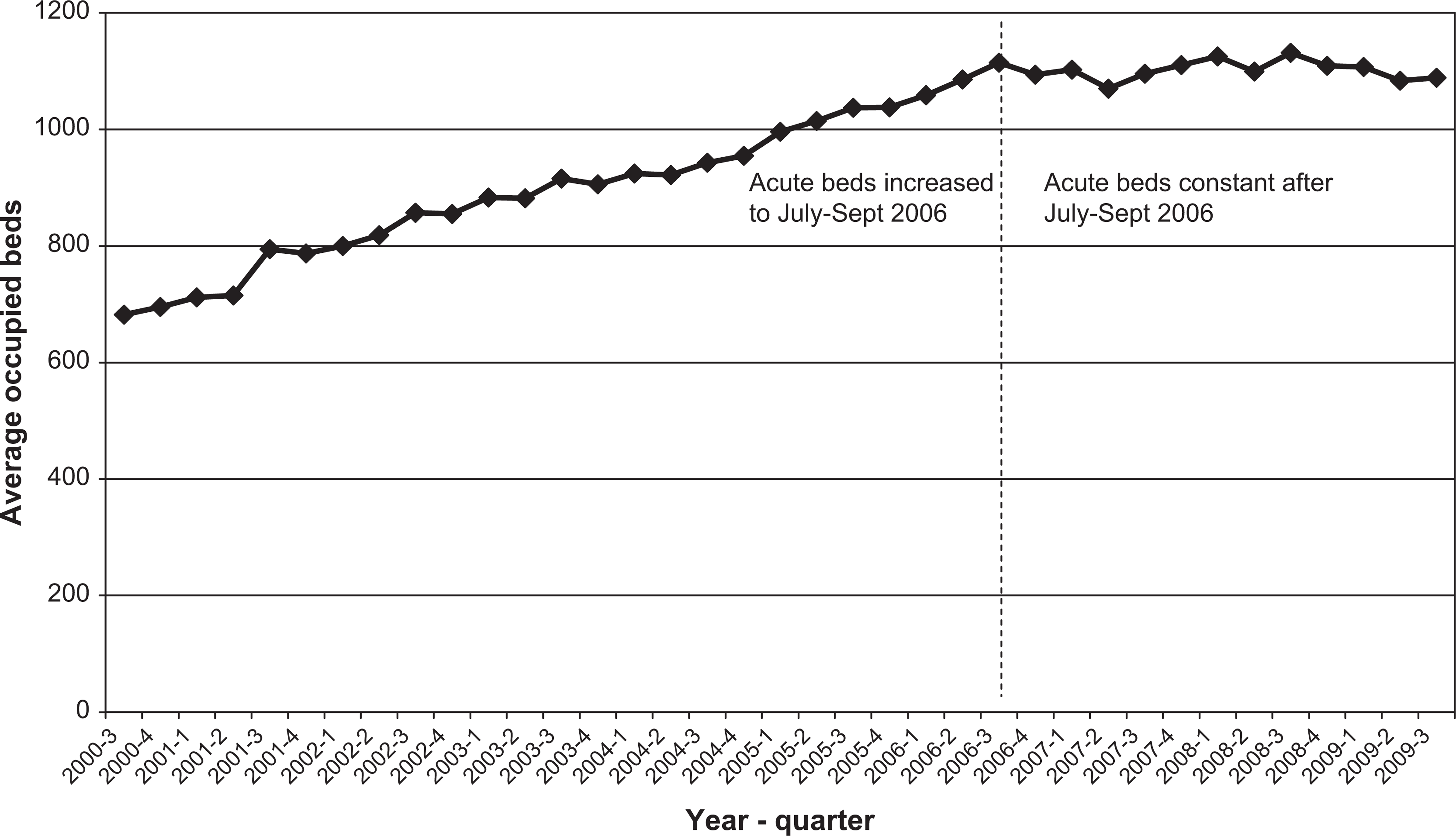
Average occupied beds in in-scope NSW acute mental health units, 2000–2009.
As increasing bed numbers leads to increased admissions it is also possible that any increase in admissions for stimulant-related disorders over the period may simply reflect greater bed access rather than greater demand. Therefore analyses have included occupied bed days as a second dependent variable. As the increase in bed numbers has not been linear, a ‘bed peak’ dummy variable has also been created, dividing the time series into a component prior to July–Sept 2006 where beds increased in a linear fashion, and a component after that period where beds have been steady.
This analysis treats increased bed numbers as if they are independent of and precede increased presentations and admissions. The relationship between bed numbers and admissions is of course likely to be complex and recursive: the increased construction of beds in NSW during this decade was itself driven by community, consumer and clinician concerns about increased rates of admission and occupancy. However, for this analysis it is not possible to model the relationship in this way.
Association between possession and admissions
Linear regression was conducted separately for each of the three main dependent variables. The regression model included three variables: (i) amphetamine possession incidents per day, (ii) average occupied beds in in-scope units and (iii) a binary ‘bed peak’ variable indicating whether the month examined was during or after the period of increasing bed numbers. Results of these regressions are summarized in Table 3.
Relationship between amphetamine possession, beds and admissions
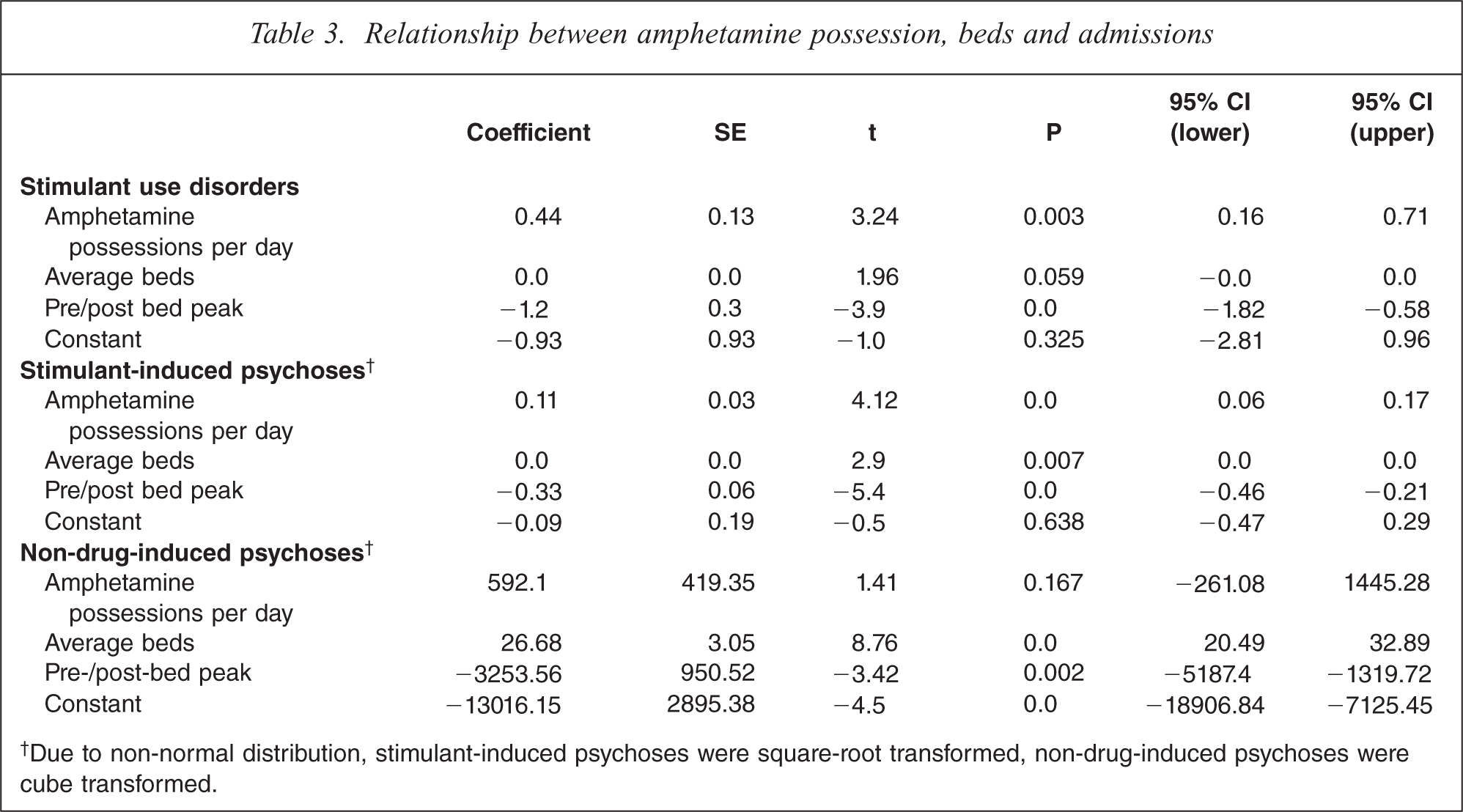
†Due to non-normal distribution, stimulant-induced psychoses were square-root transformed, non-drug-induced psychoses were cube transformed.
Admissions for stimulant use disorders and stimulant-induced psychoses showed a significant association with incidents of amphetamine possession. These associations persisted after adjustment for changes in bed numbers. The overall regression model, including possession rates and bed number/period variables accounted for 34% of variance in admissions for stimulant use disorders (F(3,33) = 7.28, p = 0.0007, R2 = 0.398, Adj R2 = 0.343) and 50% of the variance in stimulant-induced psychoses (F(3,33) = 13.17, p = 0.0000, R2 = 0.5449, Adj R2 = 0.5035).
Examination of admissions for non-drug-induced psychoses was complicated by the non-normal distribution of this variable. Of standard transformation options only a cubic transformation produced a distribution marginally suitable for regression (chi-square of original versus transformed distribution = 4.08, P = 0.13). Using this transformation the combined regression model accounted for 77% of variation in admissions (F(3,33) = 41.74, p = 0.0, R2 = 0.791, Adj R2 = 0.773); however, amphetamine possession made a non-significant contribution to this model, and nearly all variance in admissions was accounted for by changes in bed numbers.
Discussion
Summary of findings
In this NSW data, from 2000 to 2009 there was a relationship between amphetamine availability (as measured by police incidents of amphetamine possession) and admissions to acute mental health units for amphetamine use and amphetamine-related psychoses. From 2000 to 2007 there was a steady increase in amphetamine possession incidents and in amphetamine-related admissions. Acute mental health beds have also increased in this period; however, the relationship between amphetamine availability (possession incidents) and amphetamine-related admissions persisted after controlling for this bed increase.
An unexpected finding was an apparent downward trend in both amphetamine availability and amphetamine-related admissions from a peak in the first quarter of 2007 to a low in late 2009. Over this period amphetamine possession incidents reduced by 33% (from 749 in Q1 2007 to 503 in Q3 2009), stimulant use disorders by 62% (from 399 to 153 admissions per quarter), stimulant-related psychoses by 75% (from 167 to 41 admissions per quarter) and admissions for schizophrenia by 18% (from 1625 to 1334 admissions per quarter). Mental health bed numbers have remained stable during this period.
Limitations
The current study has the limitations of ecological studies in comparing two sets of aggregate, state level data [14], and we cannot demonstrate exposure of admitted individuals to stimulants, or that increased amphetamine availability and increased admissions occurred in the same geographical regions of NSW.
The study essentially compares two relatively imprecise measures. Amphetamine-related criminal incidents provide an indirect measure of community drug availability, but are clearly subject to influence from other factors. Diagnostic information collected from routine administrative collections reflects diagnoses made by many hundreds of clinicians using diverse diagnostic practices rather than structured diagnostic instruments. In considering substance-related disorders in particular, the reliability of routine clinical diagnoses is limited, and there is frequent under-recognition and under-diagnosis of substance-related disorders in routine clinical practice. These factors clearly limit the conclusions that can be drawn from the current study. However, the imprecision of the available measures is likely to bias against finding an association in this study.
Both drug use and admissions may be influenced by broader social factors, including broad trends in economic activity and employment over the period being studied. Increased arrests for amphetamine possession due to increased police activity may result in increased detection and diversion of individuals with psychosis to mental health services by police. Therefore we cannot conclude that the association found between varying amphetamine availability and admissions is a causal one.
Both health and police data may have been influenced coincidentally by changes in practice and procedure or coding within their respective systems: there have been changes to NSW Police resources and the introduction of new diversion and cautioning systems within NSW within this period. NSW Health services have moved from ICD-9 to ICD-10 coding: the current study has mapped ICD-9 codes where present to equivalent ICD-10 codes, but these changes, or changes in NSW documentation requirements, or source systems over the period, may have resulted in changes in diagnostic recording or coding.
Regarding the recent downward trend in criminal incidents and admissions, both sets of data are subject to underestimation for recent time periods and may be revised upwards as time elapses. Diagnosis in NSW Health data is not completed until after separation from hospital and following a further period required for coding and data entry: diagnosis completion may continue to increase for 3–6 months after the close of a period. Data for the current study were extracted approximately 4 months after the close of the last period being analysed, and so data for the last quarter may be underestimated by up to 5–10%. However, the decline since 2007 has been steady and consistent, and the overall trend seen is unlikely to be an artefact of diagnostic coding delays.
The study sought to examine for a relationship between amphetamine availability and admission for non-drug-related psychoses including schizophrenia. The confounding effects of changing bed numbers over this period have made it difficult to examine this question statistically. Figure 2 compares amphetamine availability with admissions for non-drug-related psychoses, including schizophrenia. There appear to be some similarities between these two data series, and since early 2007 the reduction in overall admissions for psychosis has mirrored that for amphetamine-related disorders. If increased drug-related presentations for psychosis were themselves a driver for increases in bed numbers, our approach of adjusting for bed numbers as an independent variable may have prevented demonstration of an association. We think that the issue requires further study, examining a longer time-series of data for the period after bed numbers have stabilized. Even a minor impact of amphetamines on admission rates for schizophrenia and related psychoses may have significant personal and service impact; in the period studied there were approximately 10 000 admissions per year to acute mental health units with diagnoses of psychotic disorders, comprising 48% of all admissions to those units.
Conclusions
Within the limitations described above, increased amphetamine availability and use appear to have been one factor increasing demand for mental health admission in NSW over the last decade. Conversely, there appears to have been a significant downward trend in amphetamine availability and admissions for amphetamine-related disorders from early 2007 to the end of the study period (September 2009).
Polices and strategies which reduce the community availability of amphetamines may result in reduced admissions for amphetamine-related mental health conditions, including amphetamine-induced psychoses. These psychoses result in significant trauma and morbidity, and for some vulnerable individuals may represent the first phase of a continuing or recurrent psychotic disorder. Therefore, limiting community amphetamine availability may be one strategy contributing to the prevention of psychosis.
Footnotes
Acknowlegements
We thank Don Weatherburn and Jessie Holmes of NSW Bureau of Crime Statistics and Research.