
Abstract
The literature on therapy over the Internet is expanding quickly. There have been three recent meta-analyses of Internet-delivered cognitive behaviour therapy (iCBT) for people with anxiety or depression [1–3]. The first two meta-analyses included studies of participants with a range of severity levels ranging from those with sub-threshold symptoms to those with DSM-IV defined disorders. In anxiety states [1], the effect size superiority of iCBT over control conditions was large (23 studies, Cohen's d = 1.1). A second meta-analysis reporting the resulting of iCBT for depressive states [2] reported a moderate effect size (12 studies, d = 0.41). The third meta-analysis [3] was restricted to randomized controlled trials of iCBT in participants who met diagnostic criteria for major depression, social phobia, panic disorder or generalized anxiety disorder. A total of 22 studies were identified, six on major depression, eight on social phobia, six on panic disorder and two on generalized anxiety disorder. All studies reported that the outcome of the treated group was superior to that of the waiting list or treatment-as-usual control group (mean Hedges g = 0.88, number needed to treat = 2.2). There was evidence that outcomes were stable and that participants found iCBT to be acceptable and satisfactory. The subjects in most of the studies were volunteers responding to publicity about the availability of Internet treatment.
A question that remains is whether iCBT would be equally beneficial in regular patients referred for CBT and randomized to either iCBT or to face to face CBT. There are five studies [4–8] in which computerized CBT was compared to face-to-face CBT for major depression or panic disorder (total number of patients was 567; 300 in the computerized and 267 in the face-to-face conditions). The effect size indicating the difference between computerized treatments and face-to-face treatments was a non-significant g = 0.09 in favour of Internet-based treatments (95%CI: −0.34∼17) [3]. We now report an effectiveness trial in which patients with social phobia accepted for face-to-face treatment at an anxiety disorders clinic were asked to volunteer to be randomized to either iCBT or face-to-face CBT.
Method
Participants
Patients were referred by their general practitioner to the Anxiety Disorders Clinic at St Vincent's Hospital, Sydney, for possible treatment of an anxiety disorder. They were seen by a consultant psychiatrist and those meeting criteria for social phobia were offered treatment and then asked if they would participate in a trial in which they would have an even chance of being offered web-based treatment instead of the face to face treatment they and their referring doctor had expected. Details of participant flow are in Figure 1. During the 26 weeks of recruitment, 75 met criteria for social phobia, and were offered face-to-face CBT; 37 agreed to participate in the trial and be randomized to iCBT or face-to-face CBT.
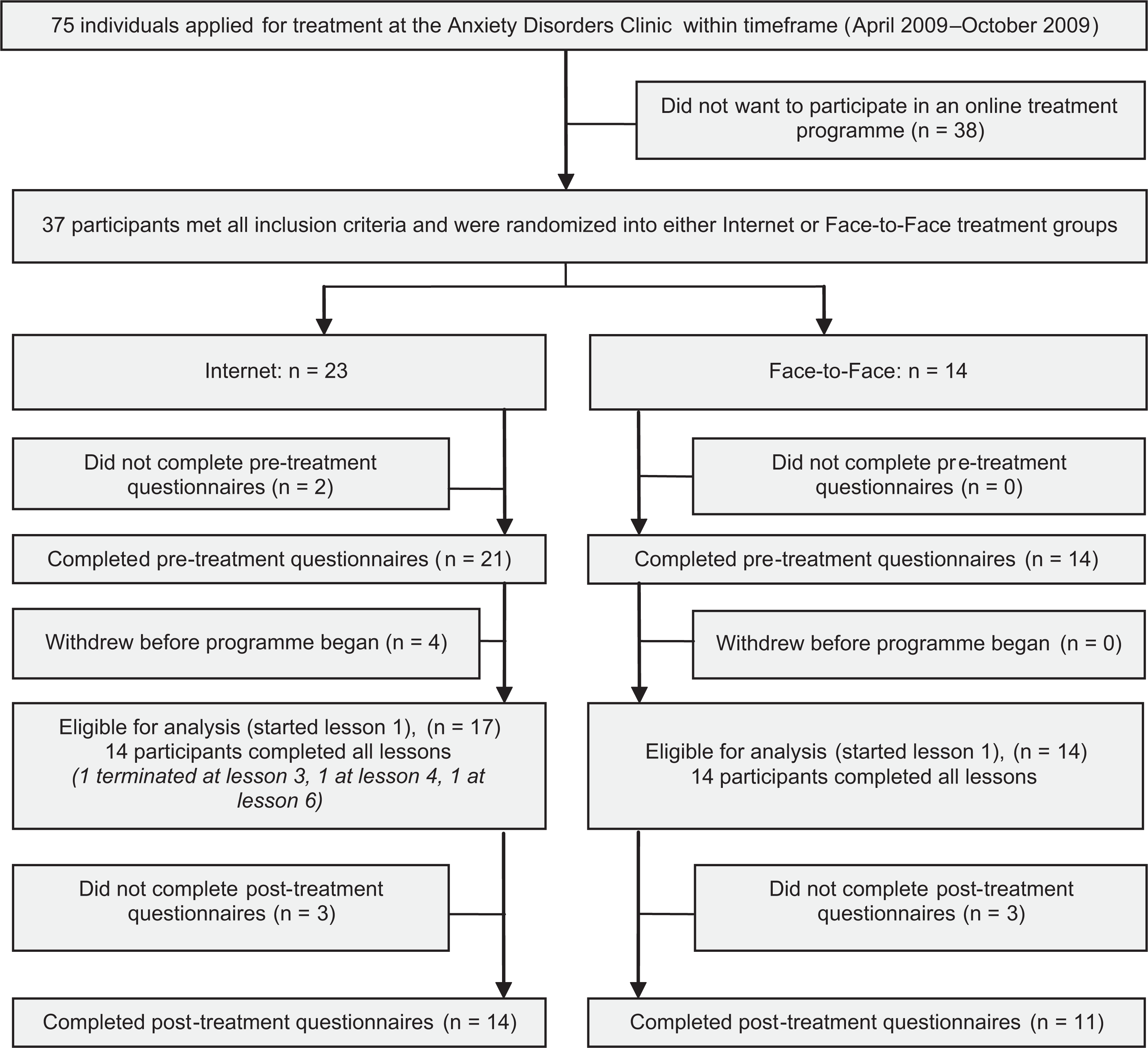
Flow chart of recruitment and treatment.
Interventions
Internet CBT: The iCBT programme was the Shyness programme reported as efficacious in previous RCTs for treating social phobia (Shyness 6) [9]. This treatment, delivered by computer, comprised six online lessons; a summary/homework assignment for each lesson; comments by participants on a forum moderated by the clinician (M.D.); access to supplementary materials; automatic emails and fortnightly short message service (SMS). Part of the content of each lesson was presented in the form of an illustrated story about a young man with social phobia who, with the help of a clinical psychologist, successfully gains mastery over his symptoms. Lessons 1 and 2 provided education about the symptoms and treatment of social phobia; Lesson 3 provided instructions on how to develop an exposure hierarchy and about practising graded exposure; Lessons 4 and 5 reinforced principles of graded exposure and demonstrated principles of cognitive restructuring; while Lesson 6 included information about relapse prevention. Participants were encouraged to complete the first four lessons within the first two weeks, in order to provide more opportunity to practise the graded exposure, cognitive skills and other coping techniques. All participants were asked to complete the six lessons within eight weeks of starting. Participants were telephoned or emailed each week by the clinician.
Face-to-face CBT
The format of the programme was a group setting with all participants meeting criteria for social phobia. Each group had a maximum of seven participants (not all of whom were research participants) who met weekly for seven weeks for 4 h under the guidance of the same clinician (M.D.). The content of the programme followed the programme outlined in a standard text [10, pp. 197–260]. All participants were given a copy of the programme to use in the sessions and to revise between sessions.
Outcomes
Applicants completed the Social Interaction Anxiety Scale (SIAS) [10]; the Social Phobia Scale (SPS) [11]; and the World Health Organization Disability Assessment Schedule (WHODAS2) [12], a measure of disability. Changes in the SIAS and SPS were considered the primary social phobia outcome measures, the WHODAS2 a secondary outcome measure. At post-treatment, participants completed the same questionnaires.
Sample size
The sample was controlled by the proportion of people being offered face to face CBT for social phobia at the Anxiety Disorders Clinic between April and October 2009 who agreed to be randomized.
Randomization
The 37 patients accepted into the programme were randomized by NT via a true randomization process (www.random.org) to either the iCBT (n = 23) or face-to-face CBT (n = 14) (Table 1). Self report measures precluded blinding.
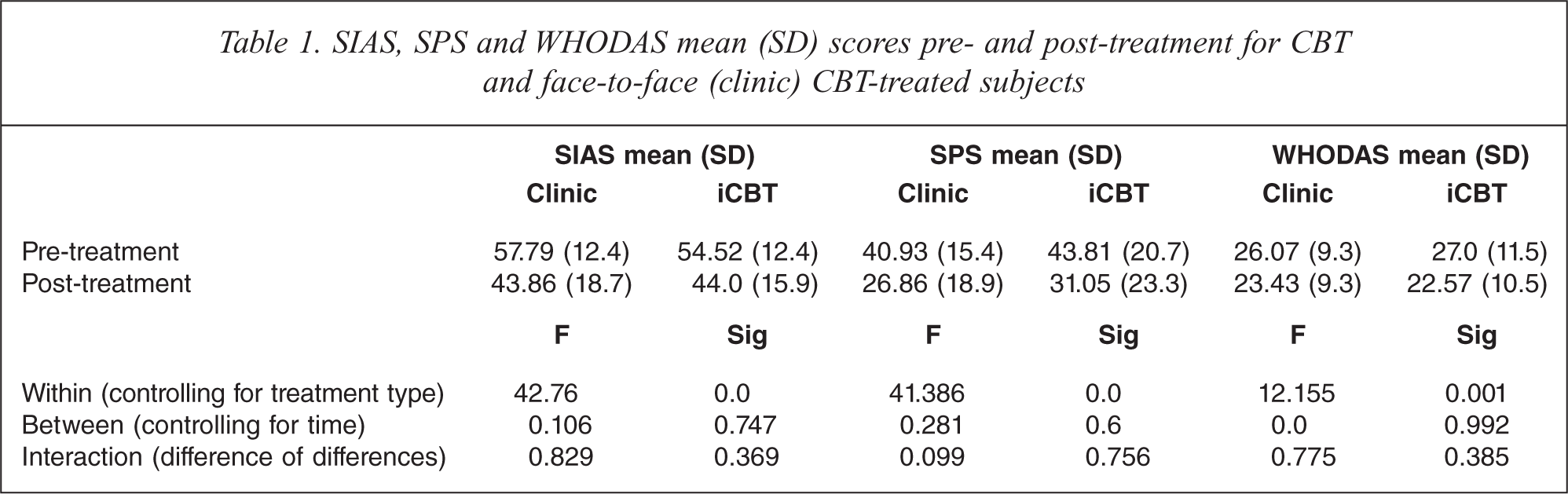
SIAS, SPS and WHODAS mean (SD) scores pre- and post-treatment for CBT and face-to-face (clinic) CBT-treated subjects
Statistical methods
All post-treatment analyses involve an intention to treat design. Pre- to post-treatment changes in participants’ questionnaire scores were analysed using univariate analyses of covariance (ANCOVAs).
The study was approved by the Human Research Ethics Committee (HREC) of St Vincent's Hospital (Sydney, Australia) and the HREC of the University of New South Wales (Sydney, Australia). This trial was registered as ACTRN12609000212257.
RESULTS
Participant flow
The flow is shown in Figure 1.
Recruitment
Recruitment occurred between April and October 2009.
Baseline data
The mean age of participants was 31.9 (7.8), 59.5% male.
Numbers analysed
Post-treatment data was collected from 11/14 face-to-face CBT group participants and 14/21 iCBT group participants. In accordance with the intention-to-treat paradigm, the pre-treatment scores of the 10 participants who did not complete the post-treatment questionnaires were replicated as their post-treatment scores.
Outcomes
A univariate ANCOVA on post-treatment on the SIAS or SPS scores, controlling for pre-treatment scores, (see Table 1) revealed no differences between the iCBT or face-to-face CBT groups. There were no significant differences between groups on the WHODAS2, the secondary outcome measure.
Therapist time
Each participant in the iCBT condition received emails and telephone calls in addition to those that are automated. This required a total of 18 min per patient of clinician time. Each patient in the face-to-face CBT condition received seven 4-h sessions of clinician time but as there were seven people in each group the total amount of clinician time given to each patient averaged 240 min, 13 times more than that required for each iCBT patient.
Adverse events
None of the participants from the face-to-face CBT group, but three participants from the iCBT group formally withdrew from treatment. There were no other adverse events.
Discussion
A total of 37 adults who were referred to the anxiety disorders clinic for face-to-face CBT and who were judged to meet criteria for social phobia agreed to be randomized to either iCBT or face-to-face CBT. The randomization process allocated 23 to iCBT (but two dropped out before commencing) and 14 to face-to-face CBT. Both groups made substantial progress, and there were no between-group differences post-treatment.
Both groups were treated by the same therapist (M.D.), but the time spent on the iCBT group was 13 times less per person than the time spent with the face-to-face group. The face-to-face CBT group were treated in groups of seven and the time required would have been considerably longer if they had been treated individually.
That face-to-face CBT and iCBT produce equivalent benefit in social phobia is in accord with the five studies reviewed earlier in depression and panic disorder [4–8]. This study was smaller than those studies but there is no suggestion that an increase in sample size would have revealed a significant difference between the two modes of treatment. The efficiency of iCBT in all three disorders leads to the conclusion that iCBT should be offered to people with depression, panic or social phobia as standard of care and that face-to-face CBT should be reserved, in a stepped care design, for people who have not benefited sufficiently from iCBT.
Footnotes
Acknowledgements