
Abstract
The link between attachment styles and overt psychiatric symptoms has attracted extensive theoretical attention, particularly in relation to early childhood [1, 2]. The recent identification of adult separation anxiety disorder (ASAD) [3–5] offers the potential to examine this association over the course of later development.
Attachment theory postulates that early parent–child bonds play a major role in the development of internal working models of close interpersonal relationships, thereby establishing a template for enduring attachment styles [1, 6]. Once established, attachment styles are thought to modulate ongoing interpersonal interactions and influence expectations of future relationships. Securely attached adults have confidence in developing close, intimate relationships characterized by reciprocal support, care and affection. In contrast, adults with anxious or preoccupied attachment styles tend to be hypervigilant about their relationships, being sensitive to loss or threat of ruptures in relation to close interpersonal bonds. They seek close proximity to or contact with attachment figures, requiring repeated reassurances that they will not be abandoned. It is hypothesized that anxious attachment styles in turn predispose to a range of anxiety and depressive symptoms, particularly at times of later interpersonal stress [7–9].
Of all the forms of anxiety, separation anxiety disorder would seem to be the most likely to be associated with an anxious attachment style, because sufferers are by definition highly sensitive to real or perceived threats to relationships [2, 10]. Dysfunctional parenting and hereditary factors appear to play a role in generating early separation anxiety [11], recognizing however that the child's anxiety itself may generate overprotective parenting [12]. As yet, no studies have examined whether anxious attachment styles represent a risk to separation anxiety disorder in adulthood.
The status of ASAD has been clarified only recently [4, 5]. The delay in focusing on that category may have been a consequence of Bowlby's assertion that agoraphobia represents underlying separation anxiety in adulthood [1]. In DSM-III the link with separation anxiety shifted to panic disorder (PD), with agoraphobia being regarded as a strategy to avoid panic triggers. Yet, studies attempting to link early separation anxiety with adult PD with agoraphobia have yielded contradictory results [13–15], with some studies showing specific links and others suggesting that separation anxiety is a general risk factor to a range of anxiety disorders [16, 17]. But these former studies did not take into account the category of ASAD.
The phenomenology of ASAD was described in the late 1990s [3, 4]. Subsequently, an independent research group has identified the same constellation of symptoms [5]. ASAD symptoms are analogous to those manifested in childhood separation anxiety disorder apart from expectable maturational differences (e.g. adults fear leaving home for work while children may exhibit school refusal). Affected adults described intense anxiety about separation from key attachment figures (not only parents, but also spouses and children), fears that harm might befall those close to them, and an intense yearning to return home [3]. They report high levels of early separation anxiety, suggesting that there is a developmental continuity for this form of anxiety. Specifically, repeated studies have found substantial correlations between the Separation Anxiety Symptom Inventory (SASI) [18], a retrospective self-report measure of juvenile separation anxiety symptoms, and scores on the Adult Separation Anxiety Questionnaire (ASA-27) [4, 12]. Furthermore, approximately two-thirds of adults diagnosed with ASAD fulfilled criteria for a retrospective diagnosis of juvenile separation anxiety using DSM-IV criteria [4]. Once ASAD is included as a subcategory of adult anxiety, any apparent relationship between early separation anxiety and PD or PD with agoraphobia (PD/PD-AG) disappears [17]. Recently, the National Comorbidity Survey Replication [19] included a module for ASAD, reporting a 12 month prevalence of 0.9% and a lifetime prevalence of 6.6% [20].
Clinic-based studies have indicated that adults referred with a presumptive diagnosis of PD/PD-AG can often be re-assigned to ASAD after systematic assessment using structured diagnostic measures [12, 19, 21, 22]. In the majority of cases symptoms of separation anxiety occurred first, with panic attacks, when present, being triggered by typical fears of separation. Also, when panic was present, separation anxiety symptoms were regarded as having greater salience to the patient and being most responsible for ongoing psychosocial disability. A recent clinic-based study of cognitive behavioural therapy for PD/PD-AG has shown that of all the variables assessed, only two factors predicted treatment outcome. Recovery was associated with greater severity of panic symptoms at the commencement of therapy; and, in contrast, the presence of ASAD was a strong predictor of poor outcome (odds ratio=3.74) [23]. It seems possible that a cognitive behavioural therapy approach focusing solely on symptoms of panic and agoraphobia may not have addressed the core problems associated with separation anxiety and/or an underlying disturbance in attachment styles.
The aim of the present study, therefore, was to investigate whether patients initially diagnosed with PD/PD-AG who also met criteria for ASAD differed from the remaining group in manifesting insecure attachment styles.
Methods
Sample
The sample was recruited from a public hospital anxiety clinic in Sydney, Australia. All patients signed a consent form approved by the Ethics Committee for the Sydney South West Area Health Service. The sample consisted of consecutive patients diagnosed with PD/PD-AG according to the Structured Clinical Interview for DSM-IV (SCID) [24].
Measures
Structured Clinical Interview for DSM-IV
The SCID is a clinician-administered semi-structured interview used for diagnosing major Axis I disorders [24]. The measure was used to assign a current diagnosis of anxiety subtypes (but not separation anxiety, which is currently not included in the adult SCID). Studies of earlier versions of the SCID have yielded adequate test–retest reliability indices in patients (ranging from 0.54 to 0.85) [25, 26]. Kappa coefficients across disorders have ranged from 0.43 to 0.67 for clinic samples [26].
Attachment Style Questionnaire
The Attachment Style Questionnaire (ASQ) is a 40-item self-report questionnaire consisting of five subscales: Confidence, Discomfort with Closeness, Need for Approval, Preoccupation with Relationships, and Relationships as Secondary (to achievement) [27]. Items are rated on a 6-point scale from 1 ‘totally disagree’, to 6 ‘totally agree’. The subscales correspond to the three broad domains of attachment styles identified in the literature [2, 10], namely secure, avoidant, and ambivalent. High scores on the Confidence subscale are thought to reflect a secure attachment style, while high scores on the other subscales reflect pathological styles of attachment. Discomfort with Closeness and Relationships as Secondary correspond to an avoidant (of intimacy) attachment style while Need for Approval and Preoccupation with Relationships correspond to an anxious (about abandonment) style [27].
Alpha coefficients for the subscales have been satisfactory, ranging from 0.76 (for Relationships as Secondary) to 0.80 (for Confidence). Test–retest reliabilities for the subscales at a 10 week interval have ranged from 0.67 (Relationships as Secondary) to 0.78 (Need for Approval) [27]. Normative data drawn from a sample of healthy volunteers (n=64, mean age=23.0 years, SD=2.8 years) [28] are presented in Table 1 and are used as an approximate comparison with the data derived from the anxiety clinic.
Adult Separation Anxiety Questionnaire
This scale is a 27-item self-report measure developed to assess core separation anxiety symptoms [29]. Each item is rated on a 4-point scale where 0 indicates ‘this has never happened’ and 3 indicates ‘this happens very often’. The measure has a coherent single factor that has been found to account for 45% of variance in separation anxiety symptoms. Cronbach's alpha was 0.95 and test–retest reliability at 3 weeks was high (0.86) [29]. A receiver operating characteristic (ROC) analysis comparing an ASA-27-derived diagnosis of ASAD with one obtained using a clinician-administered semi-structured interview yielded a high area under the curve index (AUC=0.9). Using a cut-off score of 22 on the ASA-27 to assign subjects to the putative category of ASAD yielded a sensitivity of 81% and a specificity of 84% compared to diagnoses assigned by clinicians using the structured interview.
Separation Anxiety Symptom Inventory
The SASI is a 15-item self-report measure that assesses adults’ memories of separation anxiety symptoms experienced up to the age of 18 years [18]. Items are rated on a 4-point scale similar to that of the ASA-27, with the square root being calculated for the aggregated score to normalize the distribution. The measure has a coherent factorial structure, high internal consistency (Cronbach's alpha ranging from 0.84 to 0.88) and sound test–retest reliability (intra-class correlations ranging from 0.86 to 0.98) [18].
Statistical analysis
SPSS was used to undertake all analyses (SPSS, Chicago, IL, USA). Clinic patient data were compared with normative data using a single samples t-test, while the two anxiety subgroups were compared using independent samples t-tests. The multivariate analysis applied a stepwise regression to examine the relationship between the ASQ subscales and a measure of adult separation anxiety symptoms (ASA-27). A predetermined significance criterion of p=0.01 was used throughout.
Results
Sample characteristics
Eighty-three consecutive outpatients were diagnosed with PD or PD-AG. Seventy-four per cent (n=61) were female, and 51% (n=42) were either married or in cohabiting relationships. The mean age of the sample was 37.2 years (SD=12.7). Fifty-four patients from this group were also assigned to ASAD using a cut-off of 22 on the ASA-27. Means and standard deviations for the attachment subscales of the ASQ for the whole sample are provided in Table 1, showing broad comparisons with normative data provided by Troisi et al. [28].
ASQ subscale scores
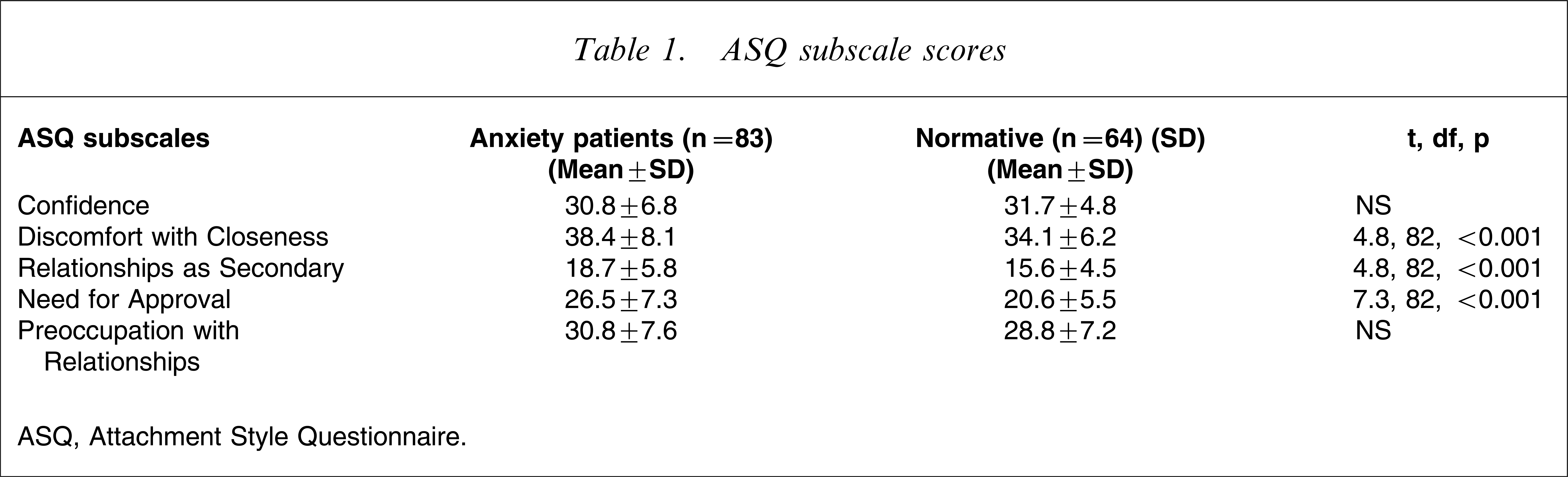
ASQ, Attachment Style Questionnaire.
Associations of SASI with ASA-27
The mean SASI and ASA-27 scores for the sample were 3.4 (SD=1.5) and 32.3 (SD=18.2), respectively. SASI and ASA-27 scores were significantly correlated (r=0.56, p=0.001).
Associations of ASA-27 with ASQ
Table 2 shows correlations between the ASA-27 and the ASQ dimensions. Discomfort with Closeness, Need for Approval and the Preoccupation with Relationships subscales all yielded significant associations with the ASA-27.
Correlations between the ASA-27 and the ASQ dimensions
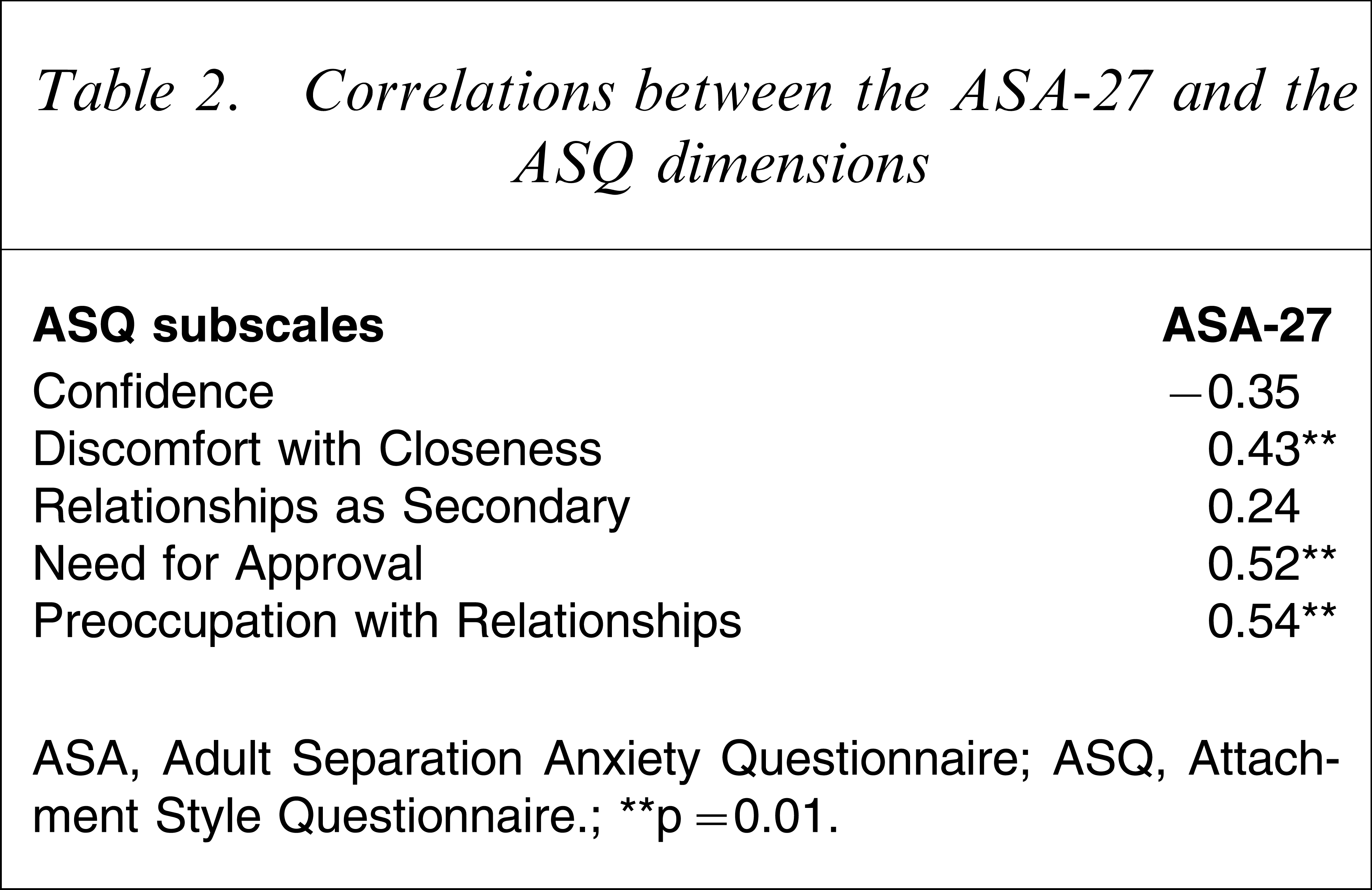
ASA, Adult Separation Anxiety Questionnaire; ASQ, Attachment Style Questionnaire.
∗∗p=0.01.
Stepwise regression analyses were undertaken to test for the overall predictive power of the ASQ when covariance among the subscales was taken into account. The ASQ accounted for 31% of the overall variance of the ASA-27 score. Subscale analysis using a stepwise regression indicated that the Preoccupation with Relationships subscale accounted for almost all of the variance (28%) attributable to the ASQ.
Association between attachment styles and ASAD diagnosis
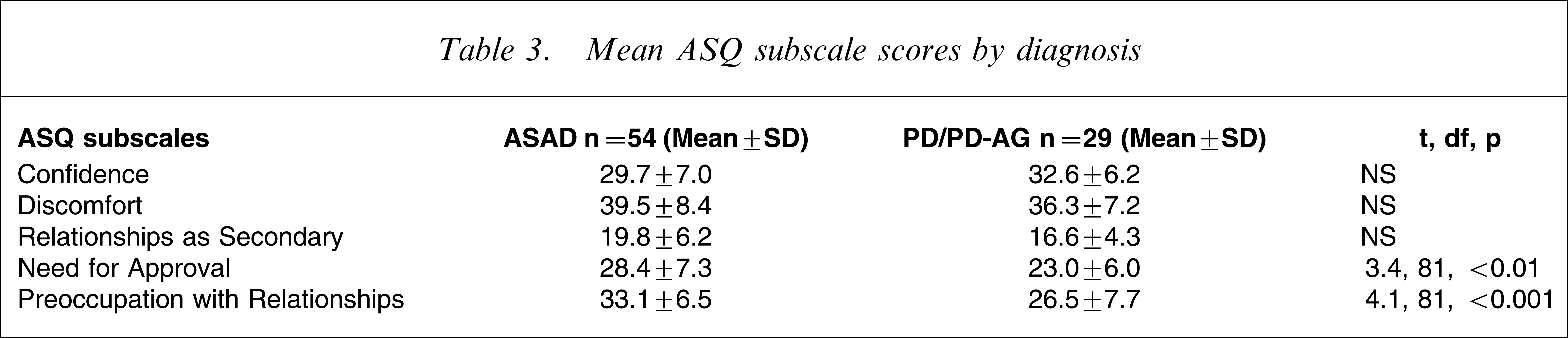
The sample was then divided into those with PD/PD-AG who reached threshold for a diagnosis of ASAD (n=55) using the established cut-off of 22 on the ASA-27 and a residual PD/PD-AG group (n=29). (For simplicity we will refer to the comorbid PD/PD-AG plus ASAD group as ASAD). ASAD patients returned statistically higher scores than the PD/PD-AG patients on two of the ASQ subscales: Need for Approval and Preoccupation with Relationships (Table 3). It is noteworthy that residual PD/PD-AG patients did not differ statistically from the normative data reported in Table 1 on any of the attachment style subscales.
Mean ASQ subscale scores by diagnosis
Discussion
To our knowledge this study is the first to examine attachment styles among patients with comorbid PD/PD-AG and ASAD. The results showed an association between a dimensional index of adult separation anxiety and particular attachment styles. In addition, patients with comorbid ASAD showed more aberrant attachment styles than those with PD/PD-AG alone. Moreover, the abnormalities associated with ASAD were primarily associated with anxious rather than avoidant attachment styles.
Prior to discussing the possible implications of these findings, the limitations of the study need to be considered. The diagnostic status of ASAD remains provisional despite its recent adoption by the NCS-R study [19]. The construct, however, seems to be gaining acceptance [5], with increasing evidence to support its status as a specific form of adult anxiety category equivalent to the established childhood diagnosis of separation anxiety disorder.
Nevertheless, given the low recognition of ASAD in primary care, patients are not yet referred to anxiety clinics specifically for that diagnosis. As such, referrals are usually assigned another diagnosis, commonly PD/PD-AG. The present data therefore are based on persons with comorbid diagnoses of PD/PD-AG and ASAD. Although our previous data suggest that when there is comorbidity, separation anxiety disorder precedes PD [3, 21], only community-based studies can test whether the present results apply to the majority of ASADs including those who do not have comorbid disorders [19]. In contrast, by comparing the data for ASADs against the residual PD/PD-AG group, we used a stringent design, if anything weighting the study against finding a difference.
It is possible that patients with ASAD are predisposed to report adverse attachment styles. It is noteworthy that they did not return statistically higher scores on all aberrant attachment dimensions, only on those associated with anxious attachment. A parsimonious explanation of the results could be that the two phenomena (ASAD and anxious attachment) simply reflect different aspects of the same construct, ‘anxiety about relationships’. Yet the analyses suggest otherwise: although there were strong associations between the two relevant measures, the greater portion of the variance remained unexplained, suggesting a high degree of independence of the two constructs.
Agoraphobia has evolved as a diagnostic construct over several decades. Bowlby made a specific link between early separation anxiety and adult agoraphobia, effectively proposing that the latter disorder was the adult manifestation of persisting separation anxiety [1]. He implicated overprotective parenting in the genesis of that developmental pathway. Notably, however, more recent studies have suggested that patients with agoraphobia tend to report exposure to uncaring rather than overprotective parenting [30]. A later formulation and one that informed the development of DSM-III and DSM-IV, gave primacy to PD, thereby assigning agoraphobia largely to the status of a behavioural reaction aimed at avoiding situations that triggered panic [31, 32]. That nosological shift focused attention on early separation anxiety as a possible risk factor to PD with or without agoraphobia. Yet, as indicated, the evolving body of research failed to provide consistent support for that putative developmental link [16, 17]. Based on the identification of ASAD and the present data, we propose a third formulation, that is, a developmental continuity theory of separation anxiety disorder. That model suggests that hereditary factors and early parental overprotectiveness combined to generate high levels of separation anxiety [11, 12]. Most often symptoms manifest in childhood but the onset can be in early adulthood. The overlap with PD-AG may occur for two reasons: acute separation anxiety (e.g. after a bond rupture) can lead to panic attacks, which in turn can become self-perpetuating; and/or contemporary operational criteria for agoraphobia overlap with those of ASAD – for example, both groups may be reluctant to leave the home, but further inquiry will clarify that the reasons differ across the two diagnostic categories.
It seems likely that persisting separation anxiety generates an enduring style of attachment in close relationships. Fears of abandonment and/or that harm will befall attachment figures will produce working models of relationships as being perpetually insecure. As the child grows older, attachment styles are likely to become entrenched, with exacerbations of separation anxiety resulting from real or imagined ruptures to bonds, reinforcing and consolidating these habitual patterns of response. We note, however, that the developmental pathway linking ASAD to anxious attachment cannot be elucidated definitively from a cross-sectional study of this kind. It seems likely that the relationship is complex, involving feedback loops linking insecure bonding experiences with anxious attachment styles and periodic exacerbations of overt separation anxiety symptoms. Only longitudinal studies might be able to unravel these interlinked relationships more clearly.
As yet no standard treatments for ASAD have been established. It is noteworthy, however, that two recent studies have indicated that comorbid ASAD among PD/PD-AG patients is a strong predictor of poor outcome for cognitive behavioural therapy [23, 33]. Standard cognitive behavioural therapy for PD/PD-AG does not address the core symptom problems of ASAD or the underlying anxious attachment styles that may predispose to that condition. There appears to be some urgency to develop treatment strategies, whether based on cognitive behavioural, interpersonal or dynamic psychotherapies that are specifically designed to address these core issues among patients with ASAD. In addition, there is room to explore pharmacotherapies that may be beneficial in addressing ASAD symptoms, with animal models suggesting that the tricyclics may have a role [34].
Conclusions
The present study suggests that anxiety patients with comorbid ASAD-PD/PD-AG have underlying anxious attachment styles. These enduring patterns of attachment may be responsible in part for the substantial disability associated with ASAD [19], exacerbating the impact on the sufferer's interpersonal relationships. As yet, persons with ASAD remain underdiagnosed and there are no specific treatment protocols aimed at addressing their core problems at a symptomatic level [3] or in terms of underlying attachment styles. There is an urgent need to advance clinical recognition of this problem and to develop effective treatment strategies to assist these patients.