
Abstract
Over the past few decades, there has been growing interest in social functioning and its determinants in schizophrenia. Social functioning, a broad term without a clear universal definition, encompasses several areas, such as social engagement, interpersonal communication, activities of daily living, social activities and occupation/employment [1]. Such functioning is a fundamental aspect of recovery and quality of life, and its measurement allows mental health professionals to plan appropriate interventions [2,3]. Of all of the factors involved, neurocognitive deficits and negative symptoms have been consistently found to contribute to poor functional outcomes [4,5], although the mechanism of their contribution remains uncertain [1,4,6] partly because of methodological discrepancies [7]. Because core psychiatric concepts do not exist independently of their socio-cultural environment [8], the results of western studies may not be applicable to patient populations of different ethnicities and cultures.
Prospective memory (PM), which is defined as ‘remembering to do something at a particular moment in the future’ [9], is gaining attention in both research and clinical practice [10] because intact or well-functioning PM is considered essential for independent social functioning and the management of illness. The proper organization of daily life in the community among schizophrenia patients, including household chores, money management, leisure activities, medical and psychiatric follow-ups, and drug treatment, is, in part, dependent upon PM.
Recent studies on PM in psychiatry have mainly focused on schizophrenia patients [11,12], who have been reported to perform significantly worse than healthy controls on all types of PM tasks. Although PM has a major impact on social functioning, only two studies to date have addressed the issue. Twamley et al. [13] reported PM to be predictive of greater functional capacity, as measured with the University of California San Diego Performance-Based Skills Assessment Brief Version, in 72 schizophrenia patients, whereas our group found no significant association between social functioning and PM [14]. However, our earlier study failed to control for two important mediating neurocognitive variables of PM, retrospective memory (RM) and intelligence [15]. As the association between schizophrenia and RM and intelligence deficits has been established [16,17], the failure to control for the potentially confounding effects of these variables could significantly bias the results.
This study set out to explore the influence of basic socio-demographic and clinical factors, symptomatology, and neurocognitive variables, including PM, RM, executive functioning, and intelligence, on social functioning in Chinese schizophrenia patients. As mentioned, social functioning is a multidimensional construct [1]. This study focused mainly on the self-care and community living skills domains of social functioning.
Methods
Study setting and participants
This study is part of a large-scale project on neurocognitive deficits in schizophrenia. Its methodological details have been provided elsewhere [12,14]. Briefly, schizophrenia inpatients were recruited from the long-term rehabilitation unit of a university-affiliated general hospital with a catchment area of approximately 800 000 people. Patients of either sex were included if (i) they were aged between 18 and 50 years, (ii) were diagnosed with DSM-IV schizophrenia, (iii) had an illness length of at least two years, (iv) received at least a primary education, (v) were taking antipsychotic drugs in a dose of less than 800 mg/day in a chlorpromazine equivalent, and (vi) were able to understand the study requirements. The exclusion criteria were (i) electroconvulsive therapy (ECT) within the past year, (ii) concomitant administration of antidepressant or benzodiazepine drugs or benzhexol in a dose exceeding 6 mg/day, (iii) a history of or current significant medical condition, including head trauma, and (iv) past or current significant drug/alcohol abuse. The study protocol was approved by the Human Research and Ethics Committee of the Chinese University of Hong Kong-New Territories East Cluster (CUHK-NTEC). Written consent was obtained from all patients.
Clinical assessment
Two subscores of the Brief Psychiatric Rating Scale (BPRS) [18] were used to measure psychotic symptoms:
Positive symptoms of conceptual disorganization, suspiciousness, hallucinatory behaviour, and unusual thought content;
Negative symptoms of emotional withdrawal, motor retardation, blunted affect, and disorientation [19].
Neuropsychological assessment
The assessment domains included intelligence, executive functioning, RM, and PM using the following tests.
Raven's Progressive Matrices to measure intelligence [20].
The Wisconsin Card Sorting Test (WCST) [21] to assess the ability to form abstract concepts, shift and maintain a set, and use feedback. The three measures employed in this study were perseverative errors, the number of categories completed, and the number of trials required to complete the first category.
The Design Fluency Test (DFT) [22] to measure the number of novel outputs for the free and fixed response conditions.
The Tower of London (TOL) [23,24] to assess the prefrontal lobe process of planning.
The immediate and delayed recall Logical Memory subtests of the Wechsler Memory Scales-Revised (WMS-R) to measure RM.
A computerized measure of the time-, event-, and activity-based PM tasks developed with Visual BASIC for this study on the basis of the classical dual-task experimental paradigm [25], the details of which have been described elsewhere [12].
Assessment of social functioning
Social functioning was evaluated with the Chinese version of the Functional Needs Assessment (FNA-C; [26,27]), a 26-item interviewer-rated, comprehensive scale of social functioning. Its components of social functioning include self-care (e.g. personal hygiene, care of belongings and eating) and community living skills (e.g. safety, use of transport, shopping, preparing food, laundry, budgeting and social manners). Each component is scored between 0 and 25 points. Higher score indicates better social functioning. The sum score of the FNA was entered in the statistical analysis.
Assessment procedures
The neuropsychological tests were administered first, followed by the PM tasks. Testing usually took two to three hours and was completed within two consecutive days. The FNA-C and BPRS were rated on the same day as the psychological tests.
Statistical analysis
Data were analysed using SPSS for Windows (Version 13.0). Associations between social functioning and the socio-demographic, clinical, and neurocognitive variables were analysed with Pearson's correlation coefficients when the data followed a normal distribution; otherwise, Spearman's rank correlation analysis was performed. Stepwise multiple linear regression analyses were employed to identify the independent contributions of the demographic and clinical variables (age, gender, education, age of onset, length of illness, symptomatology and antipsychotic doses), intelligence, PM and RM, and executive functioning to social functioning. To avoid co-linearity, tolerance was used to measure the strength of the linear relationships between the independent variables: a tolerance value of 0.6 or above was regarded as acceptable. The normality of distributions for the continuous variables was checked with the one-sample Kolmogorov-Smirnov test. Two-tailed tests were used in all analyses, with the significance level set at 0.05.
Results
The study sample consisted of 110 (72 men) schizophrenia patients whose socio-demographic data are presented in Table 1. Table 2 shows the results of correlation analyses of social functioning with the socio-demographic, clinical, and neurocognitive variables. Higher education and better performance on the WCST (categories completed) and the Logical Memory subtests (delayed and immediate) of the WMS-R are significantly correlated with better social functioning, whereas a lower WCST score (perseverative errors) and more severe negative symptoms are associated with poorer social functioning. Mann-Whitney U test indicated that there was no significant difference between the two sexes in social functioning (z = −1.1, p = 0.3).
Socio-demographic, clinical, and neurocognitive characteristics of the sample
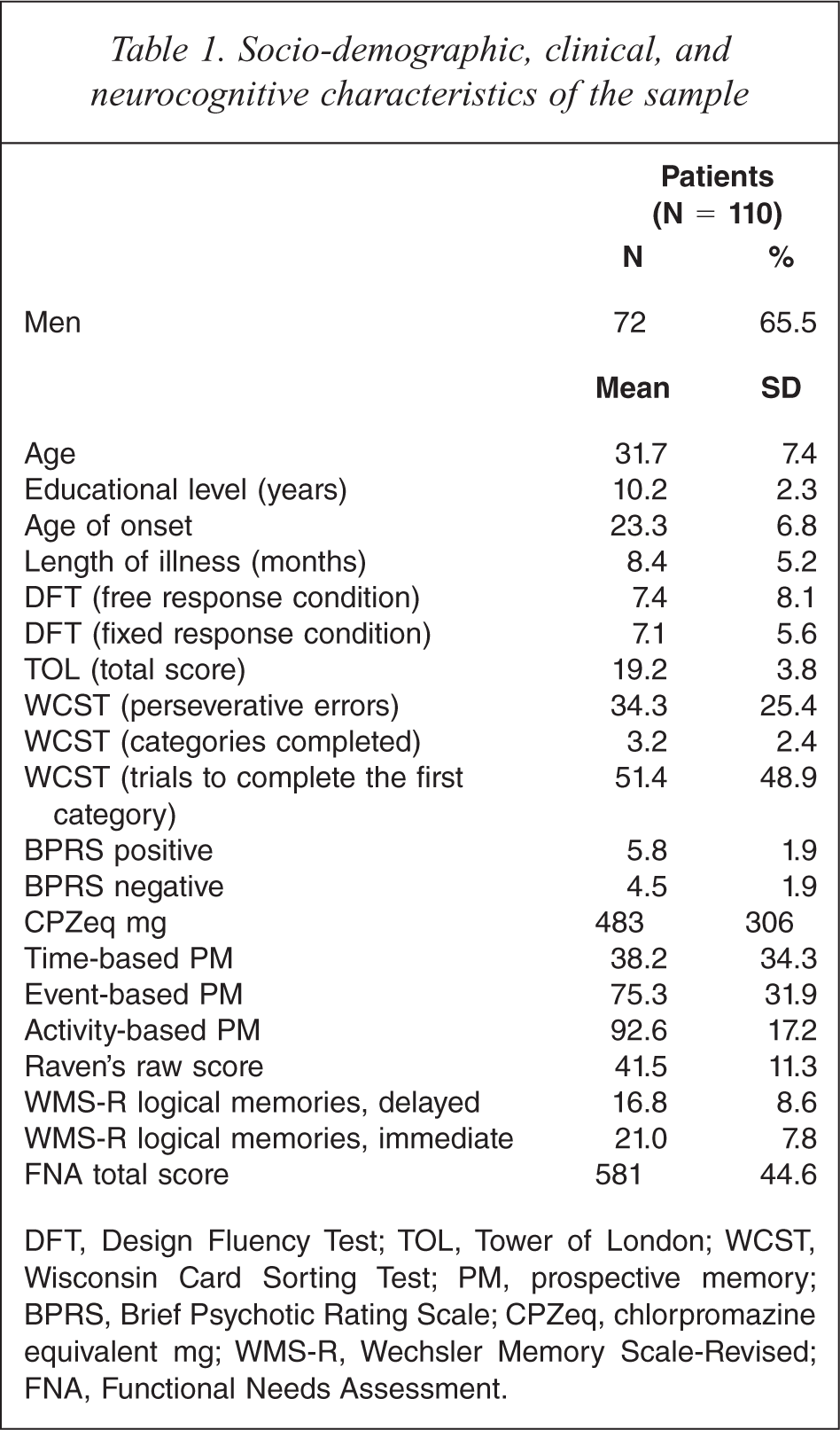
DFT, Design Fluency Test; TOL, Tower of London; WCST, Wisconsin Card Sorting Test; PM, prospective memory; BPRS, Brief Psychotic Rating Scale; CPZeq, chlorpromazine equivalent mg; WMS-R, Wechsler Memory Scale-Revised; FNA, Functional Needs Assessment.
Correlation between social functioning and socio-demographic, clinical, and neurocognitive variables (n = 110)
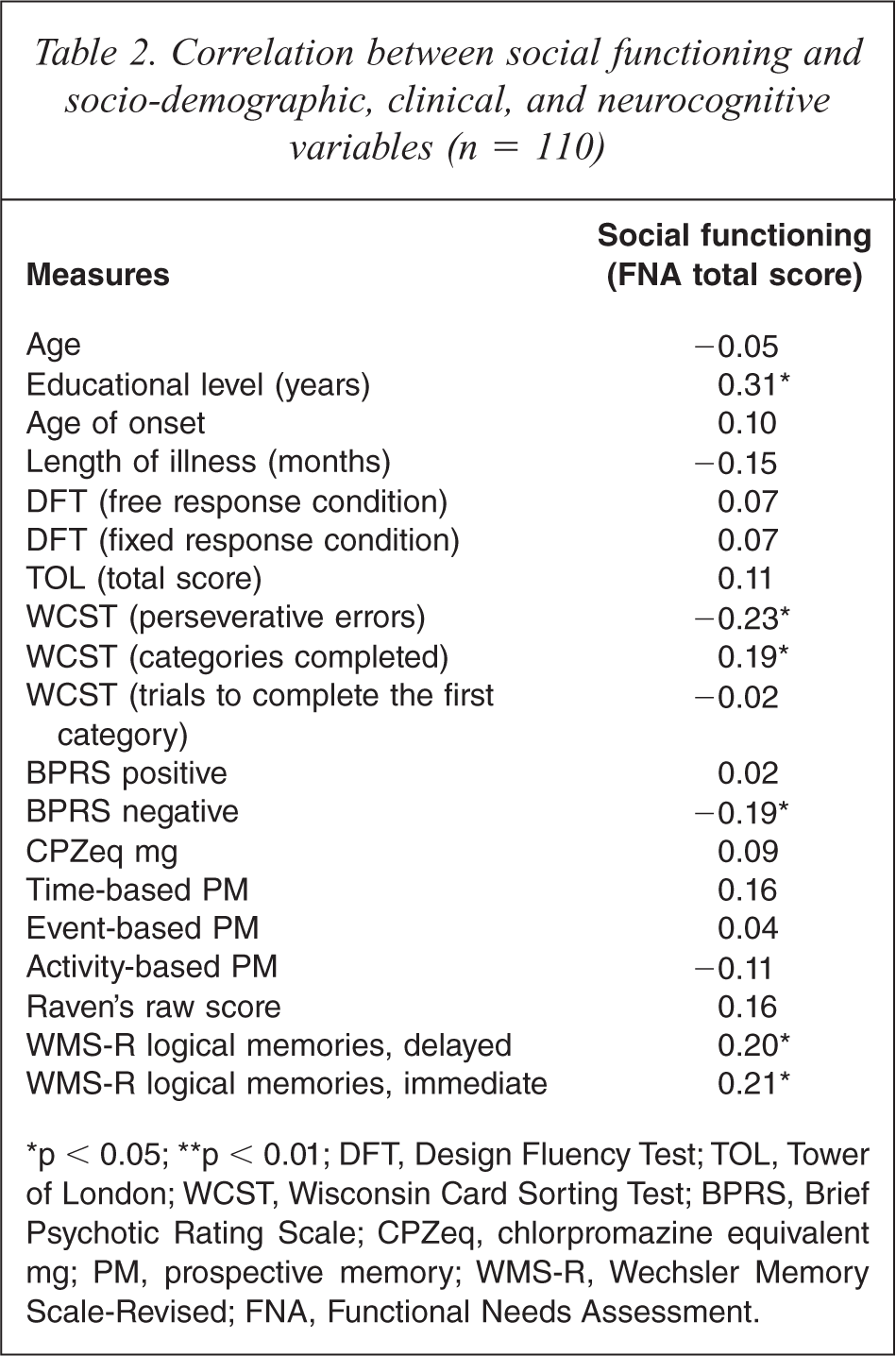
∗p < 0.05; ∗∗p < 0.01; DFT, Design Fluency Test; TOL, Tower of London; WCST, Wisconsin Card Sorting Test; BPRS, Brief Psychotic Rating Scale; CPZeq, chlorpromazine equivalent mg; PM, prospective memory; WMS-R, Wechsler Memory Scale-Revised; FNA, Functional Needs Assessment.
Table 3 presents the results of stepwise multiple regression analyses carried out to explore the predictors of social functioning. Higher education and less WCST perseverative errors are independently associated with better social functioning.
Predictors of social functioning by stepwise multiple regression analysis
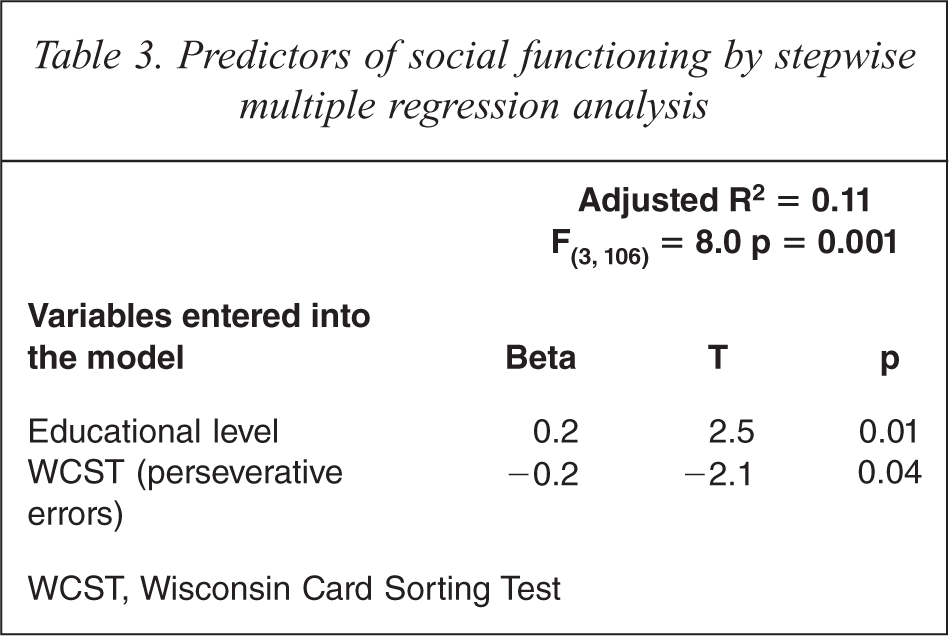
WCST, Wisconsin Card Sorting Test
Discussion
The association found between education and social functioning confirms earlier findings that higher education is significantly related to better outcomes in schizophrenia [28,29]. Several studies have demonstrated that negative psychotic symptoms predict one or more domains of social functioning. Dickerson et al. [30], for example, reported that negative symptoms are associated with long-term functional outcomes (such as residential status), whereas positive symptoms have little influence on functional capacity rated with the Social Functioning Scale [31]). Norman et al. [6] concluded that negative symptoms are more predictive of functional skills as measured with the Life Skills Profile [32] than neurocognitive dysfunction, and other studies have indicated that neurocognitive deficits are more predictive than psychotic symptoms [1,33]. In this study, negative symptoms, executive functioning, and RM deficits were associated with poor social functioning in the correlation analyses, although multivariate analysis showed perseverative errors on the WCST to be the only independent contributor, thus suggesting that variables other than those examined here are responsible for mediating the association between negative symptoms and social functioning. The independent association between social functioning and perseverative errors on the WCST in this study replicated the earlier findings [34].
Both verbal and working memories play important roles in determining functional outcomes in schizophrenia [3,17]. Studies in this area have predominantly focused on RM, and little is known about the independent association of social functioning with PM and RM. The present study found that only RM deficits to be significantly associated with poor social functioning, although this association disappeared after controlling for other variables. It is important to stress that the negative results of this study cannot be taken to prove that memory deficits, particularly PM deficits, make no contribution to poor psychosocial functioning in schizophrenia. Several additional factors must be considered to account for these results. First, psychosocial functioning is a multidimensional construct consisting of, among other factors, social problem solving, skill acquisition, and community functioning, each of which requires specific cognitive abilities [35]. In this study, psychosocial functioning was assessed by the FNA sum score, and thus the association between some specific domains of psychosocial functioning not measured by the FNA and PM could not be reliably determined. Second, the confounding effects of the possible moderating variables that were not evaluated, such as social cognition [36,37], could have obfuscated the association between psychosocial functioning and PM. This study calls attention to the complexity of gauging PM's impact on psychosocial functions. Additional potential mediating factors, such as social and family support, and the use of more sensitive instruments should be taken into account in future studies.
The strengths of this study include its relatively large sample size, use of standardized assessment tools, and independent assessment of the various aspects of investigation. The study included all available schizophrenia patients hospitalized during the study period, thus approximating a real clinical situation and conferring clinical relevance. There are, however, several limitations that weaken the robustness of our findings. First, illness severity was not controlled, and thus state-dependent biases of the neurocognitive variables cannot be discounted. Second, the study was cross-sectional in nature, and therefore the causality of the relationships identified cannot be determined. Third, illiterate patients who were unable to cooperate were excluded. In addition, only one measure of social functioning was used in this study. Fourth, more aspects of the multidimensional construct of social functioning should have been assessed. Finally, only 11% of the variance of social functioning was explained by education level and perseverative errors on the WCST in multivariate analysis, suggesting that other variables not examined in the study could impact on social functioning.
In conclusion, the findings of this study suggest that schizophrenia patients with good social functioning have higher education and score less perseverative errors on the WCST. The findings also underscore the importance of negative symptoms and deficits in executive functions and memory in determining social functioning, a core aspect of schizophrenia. Atypical antipsychotic medications may have an ameliorative effect on negative symptoms and cognitive deficits [38,39], as a result, patients taking these drugs are expected to have greater improvements in social functioning.
Footnotes
Acknowledgements
The authors are grateful to Jacky Yuen for his assistance in data collection and to the late Jin Pang Leung for his contribution to setting up the study.