
Abstract
Social determinants of health have come to greater prominence through the recent work of the WHO Commission on the Social Determinants of Health, and the Marmot Review of Health Inequalities in England. These reports also have significant implications for promotion of mental health in developed countries. In particular they reflect a growing research interest in the view that certain adverse social conditions may detrimentally affect mental or physical health by acting as chronic stressors. However, although the case for chronic arousal of stress systems as a risk factor for mental health is empirically well-founded, questions remain about how and why psychological exposure to certain kinds of proximal social conditions might contribute to such arousal. In this paper we argue that combining evidence and ideas from a number of disciplines, including public health research and psychiatry, presents an opportunity to understand the relationship better, and so inform complementary strategies in treatment, prevention and health promotion.
The World Health Organization (WHO) Commission on the Social Determinants of Health (CSDH) recently released its final report [1] calling for action to address social and economic conditions implicated in major health inequalities both between countries and within individual countries. The report calls for action in areas such as child development, housing, employment conditions, health services, and global trade policy reform. Many of these proposals are concerned with effects of adverse living conditions on physical health. However, the incidence of mental health problems also feature prominently in the report, and is recognized by WHO as a major factor shaping the overall burden of disease in both developed and developing countries [1,2].
Public health research on social determinants of health (SDH) within a particular society investigates and compares patterns of health status within and between sub-populations defined according to characteristics such as socioeconomic status (SES) assessed by level of income or education, living or working conditions, gender or ethnicity [3]. Similar research looks at differences of health status between whole countries [2,4], however, here we will focus on the first form of research, especially as it relates to mental health.
Research on SDH in developed countries such as Australia has repeatedly demonstrated a similar pattern in certain physical and mental health outcomes across the SES spectrum. Typically, the prevalence of many common, non-communicable conditions including heart disease, diabetes, obesity and major depression tends to increase on a gradient as one goes ‘down’ the SES spectrum, and is highest in the ‘lowest’ status groups [5,6]. Where this occurs (in relation to one or several such conditions) it is referred to as a social gradient in health. It is also common to find marked differences in health outcomes between ethnic or gender groups, as for example those between Aboriginal and non-Aboriginal people in Australia [7,8]. Prima facie this body of evidence suggests that exposure to the proximal living or working conditions associated with forms of social disadvantage may be playing a part in the aetiology of health problems within those population groups. Thus it also raises the possibility of preventative interventions to improve public health, or to reduce health inequalities, by reducing population exposures to the relevant conditions [7].
It is also recognized that prior genetic or acquired differences between individuals may give rise to different levels of susceptibility to forms of chronic disease, and this might contribute to selection effects, where people predisposed to health problems also tend to do less well in SES terms. Thus, as we shall discuss below, significant research effort has also gone into testing whether statistical associations between exposures to relatively adverse social conditions and worse health outcomes remain significant even after adjusting for previous health status or other potential confounding factors [9].
Social conditions, chronic stress and mental health
Broadly, public health research on mental health from Australia and comparable countries presents a case in point of the picture outlined above. A number of large-scale population studies using diagnostic interviews indicate the overall prevalence of common mental health disorders or problems tends to follow a social gradient [10–14]. Also, contemporary studies have demonstrated higher rates of problems associated with specific kinds of social conditions: low income [13], insecure housing [15], limited education [14], recent unemployment [16], high-demand or low-control work [17], child abuse or neglect [18], poor neighbourhood conditions [19], and low social support [20]. Forms of mental illness are often co-morbid with physical health problems [21].
In seeking to explain such findings, public health researchers have paid increasing attention to the view that certain adverse social conditions may detrimentally affect mental or physical health by acting as stressors, triggering arousal of neural and somatic stress responses. Extended exposure is thus seen as likely to produce chronic stress arousal, contributing to increased risk of physical conditions such as premature heart disease, or a mental health problem such as a depressive or anxiety disorder, or an addiction [9,22]. These relationships are indicated within a working model of multiple factors potentially contributing to an individual's mental illness, as shown in Figure 1.
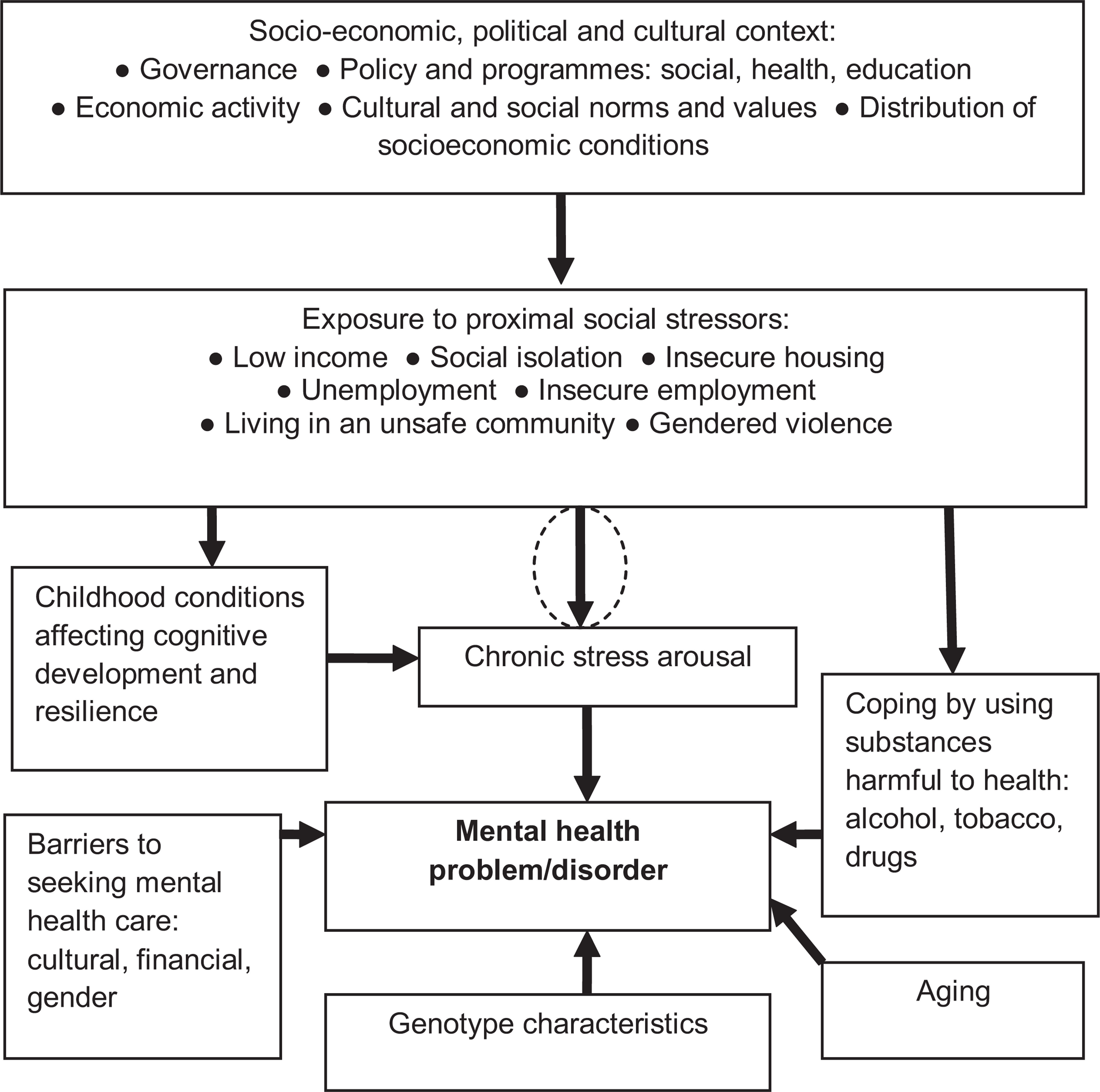
Factors influencing individual onset of a mental health problem/disorder (adapted from Commission on the Social Determinants of Health [1]).
This focus on possible health effects of chronic stress occurs against a background of extensive research identifying stress response systems and their actions during acute or chronic arousal [23,24]. There are two core elements of the stress response system: arousal of the hypothalamic-pituitary-adrenal (HPA) axis, centrally regulated by release of corticotrophin-releasing hormone (CRH) from the paraventricular nucleus of the hypothalamus, leading to release of glucocorticoids including cortisol by the adrenal cortex, and arousal of the sympathetic nervous system, regulated by noradrenergic nuclei in the brain stem, triggering release of adrenaline from the adrenal medulla [23–26]. Acute arousal of these systems induces further arousal in a range of central and peripheral areas of the nervous system and associated cognitive, behavioural and physiological changes, as an adaptive response suited to facing acute environmental challenges [27]. Cognitive-behavioural changes include heightened vigilance and attention, and behavioural motivation to adjust to changes in external conditions, achieved in part by stimulation of ascending mesocortical and mesolimbic dopamine (DA) systems. Physiological changes include increased blood pressure, heart rate, and blood glucose levels, and changes to immune system functions [24,25]. In species such as primates and humans acute stress arousal is also thought to play a part in adapting behaviour to social cues and in social learning [23,28–31].
Within this research programme it is widely recognized that, while acute stress responses can have potentially beneficial, adaptive effects, chronically repetitive or extended episodes of stress system arousal may have damaging effects on health. Chrousos argues that under conditions of chronic stress, associated physiological changes such as suppression of immune function, or elevated blood pressure and heart rate, may over time contribute to conditions as diverse as hypertension and cardiovascular disease, obesity and type-2 diabetes, osteoporosis and sleep disorders [23,27].
Chrousos and Gold argue that chronic stress ought to be seen as a key risk factor for mental illness, because it will tend over time to produce stabilized, dysregulated forms of chronic hyper- or hypoactivity and/or sensitivity in components of the stress system, which are also common biological markers of a range of recognized disorders. They suggest chronically increased activity in stress system components may contribute to conditions such as melancholic depression, panic disorder and obsessivecompulsive disorder (OCD). Chronically decreased activity they see as contributing to atypical depression, chronic fatigue syndrome and post-traumatic stress disorder (PTSD) [24,32].
The general thesis that chronic stress dysregulates elements of the stress system, and that such effects contribute to forms of mental illness, would appear to be supported by a range of stress research with humans and animals [26,33]. For example, elevated HPA activity and hypercortisolism are consistently associated with forms of anxiety disorder and major depression [26]. Patients treated for depression respond less well where disturbed activity of the HPA axis persists, and heightened HPA activity predicts higher risk of relapse [34].
Increased CRH secretion and activity is associated with melancholic depression, anorexia nervosa, panic disorder and OCD [24], and elevated CRH in cerebro-spinal fluid is symptomatic of PTSD [34].
Another stress system component, the amygdala, is aroused during acute episodes and able to trigger system arousal when a conditioned stressor is detected [29,31,35]. Chronic stress in animal models increases neuronal growth in the amygdala, which correlates with increased anxiety-like behaviour [36]. Amygdala hypertrophy is found in animals exposed to chronic variable stress [35], and after exposure to chronic stress, nuclei of the amygdala become more liable to hyperarousal during subsequent stress episodes [37]. Amygdala hypertrophy and/or hyperactivity are associated with a range of psychiatric disorders [26,38]; hyperactivity is commonly associated with major depression, and higher levels of activity correlate positively with severity of depression [39].
Chronic stress may induce tachyphylaxis in the ascending DA system, which may account for the dysphoria associated with major depression [23].
Thus there is a substantial body of theory and evidence to support a view that chronic arousal of the stress system in response to external stressors may be a key stereotypic precursor of, and causal contributor to, the onset of one or other of several forms of mental illness, characterized in part by dysregulation of stress system components. Although, equally, the manner and degree of vulnerability of any one individual in this regard to a particular set of proximal circumstances may be influenced by their genetic make-up, prenatal or early childhood experience, and/or currently available cognitive-behavioural resources [23,26].
That part of the basic public health hypothesis outlined above which appeals to chronic stress arousal as a factor able to significantly influence health outcomes in populations appears plausible and empirically well-grounded. However, biological evidence about health effects of chronic stress does not, in itself, identify any precise characteristics of social conditions found to be associated with higher rates of common forms of mental illness which might tend to arouse or exacerbate chronic stress in vulnerable individuals within exposed populations (as per the circled arrow in Figure 1), and thereby contribute to an overall social gradient in mental health.
We do not claim here to offer a definitive resolution to this issue, but to suggest below an approach which draws on information from across several disciplines with overlapping interests in stress, mental health, and health promotion.
Control and evaluation of social threats
Public health researchers have recognized these issues and designed research intended to specify more clearly attributes of social conditions with the potential to act as stressors. For example, the ‘Whitehall II’ research project investigated the possible effects of a deficit of control within a structured, hierarchical work environment. This project collected data over 15 years within a cohort of 10,000 British public servants, across 12 employment grades, and found a social gradient in mental health; i.e. prevalence of problems was highest in the lowest grades, and decreased progressively across grades from low to high status [9]. Within the project design, degree of control was assessed according to level of choice over work activity, opportunities for use of skills or initiative, and work variety [40]. Mental health was regularly assessed by General Health Questionnaire (GHQ). Several project studies have found a statistically significant association between lower levels of work control and higher rates of mental illness, after controlling for potential confounding factors. For example, Stansfeld
Research on effects of chronic stress in animals offers a different perspective on ‘control’. Of particular interest are methodologies employing a paradigm of chronic, uncontrollable stress. Joëls
Turning now to issues of social evaluation, notions about the potential effects of social hierarchy as a stressor find some support in research on social animals. For example, Sapolsky has found higher levels of HPA activation in subordinate primates compared with those of higher rank, and cortisol levels of subordinate animals are also especially high when status conditions are uncontrollable or unstable [30]. Another study found that subordinate male shrews subject to chronic, inescapable exposure to the sight or smell of a dominant shrew display chronic HPA hyperactivity and elevated basal cortisol [31].
In the Whitehall II studies, conflicting or inconsistent demands from supervisors were also found to be a significant risk factor for subsequent mental health problems [40].
To what extent might such research related to control and/or social evaluation be relevant to delineating characteristics of social conditions which tend to arouse human stress responses? Dickerson and Kemeny addressed that question in a meta-analysis of over 200 laboratory studies using cortisol levels as an index of acute psychological stress in healthy human subjects. They found that ‘motivated performance tasks elicited cortisol responses if they were uncontrollable or characterized by social-evaluative threat (task performance could be negatively judged by others). Tasks containing both uncontrollable and social-evaluative elements were associated with the largest cortisol and adrenocorticotropin hormone changes and the longest times to recovery’ [43,p.355].
Social conditions and stress
Considering such evidence in the light of research on stress systems, we suggest it is useful to highlight two points. Firstly, acute stress arousal is generally seen as delivering potentially positive benefits in areas of learning and behavioural adaption in social environments. In this context, the amygdala is seen to play an important role in formation of learned associations between salient external stimuli and behaviourally aversive or emotionally unpleasant states of acute stress arousal. It would appear to either do this itself or, with more complex stimulus conditions, to assist valanced associational learning in higher areas of the frontal cortex [28,29,44]. These associations can then be re-aroused when similar conditions are encountered, in effect predicting a possible repeat of an aversive or unpleasant event [28,44]. In those instances the amygdala appears to mediate ‘top-down’ arousal in stress systems, and in other areas such as the medial prefrontal cortex well-suited to producing changes in behaviour to adapt to changes in stimulus conditions [45,46]. Behaviour which succeeds in avoiding or decisively resolving a predicted unpleasant event may then be assimilated for future use [23,44].
It would seem reasonable to assume that sustained stress responses occurring as a part of adult interactions with modern social environments will often be produced via these kinds of higher level appraisal processes. It would also seem likely that associational learning occurring in relation to aversive or unpleasant events within these environments will often involve the behaviour of other people, in one form or another.
Proceeding on these assumptions, this suggests that even the process of competently navigating contemporary social environments is itself likely to generate a ‘load’ of intermittent acute stress arousal [23]. Beyond that, and with the several elements of previous discussion in mind, we suggest that a shift from acute to more chronic states of arousal may be likely to occur when two general features of a person's circumstances are present: when current stimulus conditions predict the possibility of a future aversive or emotionally unpleasant event, based on prior learning, and when this is combined with a lack of perceived behavioural opportunities to decisively avoid or resolve the predicted event. In other words, chronic stress arousal might be as much about repetitive or extended (conscious or sub-conscious) anticipation of possible unpleasant events, as about direct exposure to such events; coupled with a lack of behavioural control to resolve the predicted ‘problem’ [43,47]. The first part of this combination might include anticipated encounters with behaviour from others which is aggressive or distressed, or interpreted as interference with one's own goal-directed activity, or which threatens social isolation or loss of social position. As to the second element, a person might not arrive at any decisive behaviour to resolve such anticipated problems because: the obtaining external conditions don't allow for it, their current cognitive-behavioural resources don't have anything to offer, or perhaps the consequences of ‘doing something’ are appraised as potentially worse than the consequences of doing nothing.
Such an explanatory framework may offer some useful perspectives on evidence showing that common mental health problems and disorders are more prevalent among populations subject to forms of socioeconomic disadvantage according to income or education level [11,13], or to conditions such as insecure employment [42], recent unemployment [16], insecure housing [15], or unsafe neighbourhoods [19]. Firstly, it is likely that people in these situations will (like most) be subject to a level of stress arousal arising from negotiating the everyday social environment. Along with that ‘background load’, one may reasonably suppose that living with a relatively low income, for example, might regularly give rise to states of anxiety (based on prior learning) about the possible consequences of, say, not keeping up with rent, or an inability to pay medical or utilities costs; coupled with a perceived lack of opportunity to exercise decisive control over these concerns (possibly influenced by a lack of exposure to ways of learning how to cope). Insecure forms of employment might give rise to repetitive worry about the financial consequences of loss of employment, or loss of social role [48]; coupled with a perceived lack of opportunity to exercise control over work conditions or to gain more secure employment.
Within our proposed framework, one might also hypothesize that a relatively low level of educational attainment (also commonly associated with relatively worse mental health outcomes [5,14]) might be significant as limiting a person's internal or social resources available to decisively ‘solve problems’, and thus may constitute a deficit in resilience to social stressors. The anticipated social consequences of low-paid or insecure work might be very different for a university student and a single parent with limited education [48].
Finally, we also suggest that exposure to abusive or neglectful childhood conditions might have negative effects on either side of the proposed, problematic combination. In basic terms, severe exposure to stressors in early childhood resulting in long-term sensitization may increase vulnerability to chronic stress under the kinds of social conditions indicated [18,49]. And deficits in early cognitive-behavioural development might contribute to a more limited set of strategies and skills to decisively resolve anticipated, aversive social events.
In real-world environments, individuals are often subject to more than one of the conditions mentioned above. The work of the CSDH suggests that cumulative effects of a range of such social factors may ‘play out’ over time and across populations in a way which significantly influences an overall social gradient in mental health.
Conclusion
We suggest three implications for the material we have reviewed for research and health promotion strategies for mental health in Australia. Firstly, there are likely benefits in on-going cross-disciplinary research on the intersections between stress system biology and functions, social stimuli as stressors, cognitive-behavioural development, and mental health/illness. Public health research provides evidence that certain kinds of proximal social conditions in modern societies may contribute to chronic stress arousal and thereby increase the risk of mental illness; especially against a background of pre-existing genetic or acquired vulnerability [23]. Given the current scale and social costs of mental illness [50], there is good reason to work towards a more coherent theoretical view of these relationships, taking account of multiple forms of evidence which can inform improvements in treatment, prevention and health promotion strategies.
Secondly, if certain kinds of adverse social conditions across the life-course are a significant influence on overall health outcomes and their distribution across populations, this raises questions about the scope of public policies and programmes regarded as relevant to ‘health’. While the provision of quality medical and health care services is clearly important, if proximal social conditions such as those discussed can have significant effects on health, then decisions of governments and public institutions in areas outside the health portfolio may also potentially have distal effects, by influencing the extent and/or distribution of the proximal conditions in question [1,3,7]. For example, a spending increase on public housing or a change in interest rates, each might reasonably be expected, over time, to affect the extent and distribution of exposure to unaffordable or insecure housing. A comprehensive education programe for new parents could be expected to reduce later vulnerabilities to mental health problems among their children [49]. Thus, where a solid case can be made that public policies outside the health portfolio are likely to affect population health outcomes (for good or ill) this should be taken into account in policy-making processes [51]. And indeed, such approaches are beginning to be applied in Australia and other OECD (Organisation for Economic Co-operation and Development) countries [52,53].
Finally, public health perspectives on social determinants of mental (and physical) health present significant opportunities for broad-scale preventative measures, as are already demonstrably effective [51,54]. There is also a growing interest in policy measures which might help to promote resilience and positive mental health such as parenting education, or strategies to build social capital within localized settings (7,21). Wider recognition and use of such strategies can complement and enhance the effectiveness of mental health services and other interventions, when the latest information on the SDH is used to inform policy responses to mental illness.
Footnotes
Acknowledgements