
Abstract
Objective:
Clinical practice guidelines recommend that community mental health services provide preventive care for clients’ chronic disease risk behaviours; however, such care is often not routinely provided. This study aimed to assess the effectiveness of offering clients an additional consultation with a specialist clinician embedded within a community mental health service, in increasing client-reported receipt of, and satisfaction with, preventive care.
Method:
A randomised controlled trial was undertaken in one Australian community mental health service. Participants (N = 811) were randomised to receive usual care (preventive care in routine consultations; n = 405) or usual care plus the offer of an additional consultation with a specialist preventive care clinician (n = 406). Blinded interviewers assessed at baseline and 1-month follow-up the client-reported receipt of preventive care (assessment, advice and referral) for four key risk behaviours individually (smoking, poor nutrition, alcohol overconsumption and physical inactivity) and all applicable risks combined, acceptance of referrals and satisfaction with preventive care received.
Results:
Analyses indicated significantly greater increases in 12 of the 18 preventive care delivery outcomes in the intervention compared to the usual care condition from baseline to follow-up, including assessment for all risks combined (risk ratio = 4.00; 95% confidence interval = [1.57, 10.22]), advice for all applicable risks combined (risk ratio = 2.40; 95% confidence interval = [1.89, 6.47]) and offer of referral to applicable telephone services combined (risk ratio = 20.13; 95% confidence interval = [2.56, 158.04]). For each component of care, there was a significant intervention effect for at least one of the individual risk behaviours. Participants reported high levels of satisfaction with preventive care received, ranging from 77% (assessment) to 87% (referral), with no significant differences between conditions.
Conclusion:
The intervention had a significant effect on the provision of the majority of recommended elements of preventive care. Further research is needed to maximise its impact, including identifying strategies to increase client uptake.
Keywords
Background
Modifiable health risk behaviours are a key contributor to chronic disease morbidity and mortality worldwide (Australian Institute of Health and Welfare, 2016; Lim et al., 2012; World Health Organisation, 2009). Compared to the general population, people with a mental illness have a higher prevalence of four key risk behaviours: tobacco smoking, poor nutrition, alcohol overconsumption and physical inactivity (Bartlem et al., 2015a; Kilian et al., 2006). These risk behaviours influence the development of metabolic risks, such as overweight, obesity and high blood pressure (Australian Institute of Health and Welfare, 2016; Forouzanfar et al., 2015). Accordingly, the prevalence of chronic diseases is considerably higher among people with a mental illness in Australia (Harris et al., 2018; Morgan et al., 2011) and other high-income countries (Druss and Walker, 2011), contributing to a substantially reduced life expectancy in this population group (Lawrence et al., 2013; Walker et al., 2015).
The routine provision of ‘preventive care’ to address chronic disease risk behaviours is recommended by clinical practice guidelines for mental health services (NSW Department of Health, 2017; World Health Organisation, 2018). In particular, community mental health services (providing ambulatory specialised mental health care) present a key opportunity to provide preventive care, given their role in treating a large proportion of people with a mental illness (Australian Institute of Health and Welfare, 2017). The ‘AAR’ framework has been recommended to guide the provision of preventive care by health services generally, comprising assessment of clients’ risk behaviours, provision of brief advice to modify risk behaviours and referral to specialist services (Glasgow et al., 2004; Schroeder, 2005). Despite such recommendations, preventive care is infrequently provided by community mental health services (Bailey et al., 2019; Bartlem et al., 2015b; Bartlem et al., 2014). Low rates of screening and referral for associated metabolic risks among people with a mental illness have also been reported (Mitchell et al., 2012).
One model for enhancing preventive care provision in community mental health settings is to dedicate a specific clinical position to the provision of such care. Four studies have quantitatively examined the effectiveness of this model for increasing the provision of preventive care in such settings. For one study, the role of the ‘specialist preventive care clinician’ was focused on encouraging and supplementing preventive care provision by clinicians during routine consultations (Osborn et al., 2010), whereas for the remaining three studies the role focused on offering preventive care in an additional consultation (Druss et al., 2010; McKenna et al., 2014; Rogers et al., 2016). Two of the three studies examining the provision of an additional preventive care consultation reported outcomes relating to the provision of preventive care (Druss et al., 2010; McKenna et al., 2014). In the first study, a randomised controlled trial (RCT) conducted in the United States, clients were randomised to receive either usual care or the offer of additional consultations with a ‘care manager’ located in the community mental health service (Druss et al., 2010). The care manager provided health education regarding smoking, exercise, nutrition, weight and self-examination, as well as assistance in overcoming barriers to accessing primary medical care. Outcomes were reported as the proportion of preventive care elements received across four domains: physical examination, screening tests, vaccinations and health education, at 12-month follow-up. The intervention condition was found to receive a significantly higher proportion of preventive care elements compared to the usual care condition (average of 58.7% vs 21.6%, respectively, p < 0.0001). The effect of the intervention on the provision of preventive care for individual risk behaviours was not assessed.
The second study, a cross-sectional study from Australia, compared rates of metabolic monitoring (for exercise, smoking, body mass index, fasting blood glucose, blood pressure, waist circumference, cholesterol, triglycerides and lipoprotein level) between two community mental health services (McKenna et al., 2014). Metabolic monitoring was provided within routine consultations in one service and provided by a specialist clinician in the other. Data collected from medical records over 12 months indicated that the proportion of clients who received at least one component of metabolic monitoring was significantly higher when provided by a specialist clinician, compared to provision in routine mental health consultations (78% vs 3%, respectively, p = 0.01). The effectiveness of this model on other care elements (advice and referral) was not assessed quantitatively. A further limitation of both studies was the non-reporting of client uptake of the additional preventive care consultation(s), which is suggested to influence the effectiveness of the model at the population level (Ostermann et al., 2017).
To address these evidence gaps, an RCT was conducted in a community mental health service to determine the effectiveness of the offer of an additional consultation with a specialist preventive care clinician, in increasing client-reported receipt of, and satisfaction with, preventive care. The outcomes of interest were client-reported receipt of three elements of preventive care (assessment, advice and referral) for four risk behaviours (tobacco smoking, poor nutrition, alcohol overconsumption and physical inactivity) and client satisfaction with preventive care received.
Methods
Study design and setting
A two-arm, parallel-group RCT was conducted in one community mental health service in regional New South Wales, Australia. The service provides treatment to clients with a range of diagnoses and acuity. The local health care policy directs the provision of preventive care (assessment, advice and referral to telephone coaching services) for four chronic disease risk behaviours (tobacco smoking, inadequate fruit and vegetable consumption, alcohol overconsumption and physical inactivity) by mental health clinicians within routine mental health consultations (Hunter New England Local Health District, 2010). The reported proportion of clients receiving preventive care under this policy is low (Bartlem et al., 2015b). A published study protocol described the methods for this study (Fehily et al., 2017). This paper reports secondary outcomes: client-reported receipt of preventive care and satisfaction with care received.
Between March and September 2017, a ‘specialist preventive care clinician’ was embedded in the community mental health service. In this real-world trial undertaken in the context of routine clinical care, clients were randomly allocated to receive either usual care (provided by community mental health clinicians within routine consultations, in accordance with the service policy) or usual care plus the offer of the additional consultation and telephone follow-up with the specialist preventive care clinician. Outcome data were obtained via client telephone interviews at baseline (February–September 2017) and at 1-month follow-up (March–October 2017). For participants in the intervention condition, the additional consultation was scheduled to occur between these two time points. The Human Research Ethics Committees of Hunter New England Health (Ref No. 16/02/17/4.09) and the University of Newcastle (Ref No. H-2016-0123) approved the research. The trial was prospectively registered on the Australian New Zealand Clinical Trials Registry (No. ACTRN12616001519448).
Sample eligibility and procedures
Clients attending the community mental health service were eligible to participate in the study if identified by service staff as new or existing clients, 18 years or older and not deemed too unwell to be enrolled, as determined by their treating team. Sample size was determined based on the number of eligible clients attending the service and a previously reported power analysis (Fehily et al., 2017). Approximately 30 eligible clients were randomly selected each week and allocated in a 1:1 ratio to either the usual care or the intervention condition (prior to baseline data collection) according to a statistician-generated random allocation sequence (permuted block randomisation with block sizes of 2, 4 and 6). Clients and clinicians were not blinded to study allocation, consistent with what would be expected if this model of care was provided under routine care delivery conditions.
Intervention condition
The specialist preventive care clinician was an occupational therapist with 12 years’ experience working as a community mental health clinician. The clinician was provided with 2 days of training in motivational interviewing and the delivery of the intervention in line with a manualised protocol.
Clients in the intervention condition were offered a 40-minute consultation and telephone follow-up with the specialist clinician, in addition to usual care. Clients were mailed a letter detailing the offer and phoned by the specialist clinician to make an appointment (up to five call attempts).
A manualised protocol was developed based on motivational interviewing principles (Lai et al., 2010; Morton et al., 2015) to guide intervention delivery. The following elements were included:
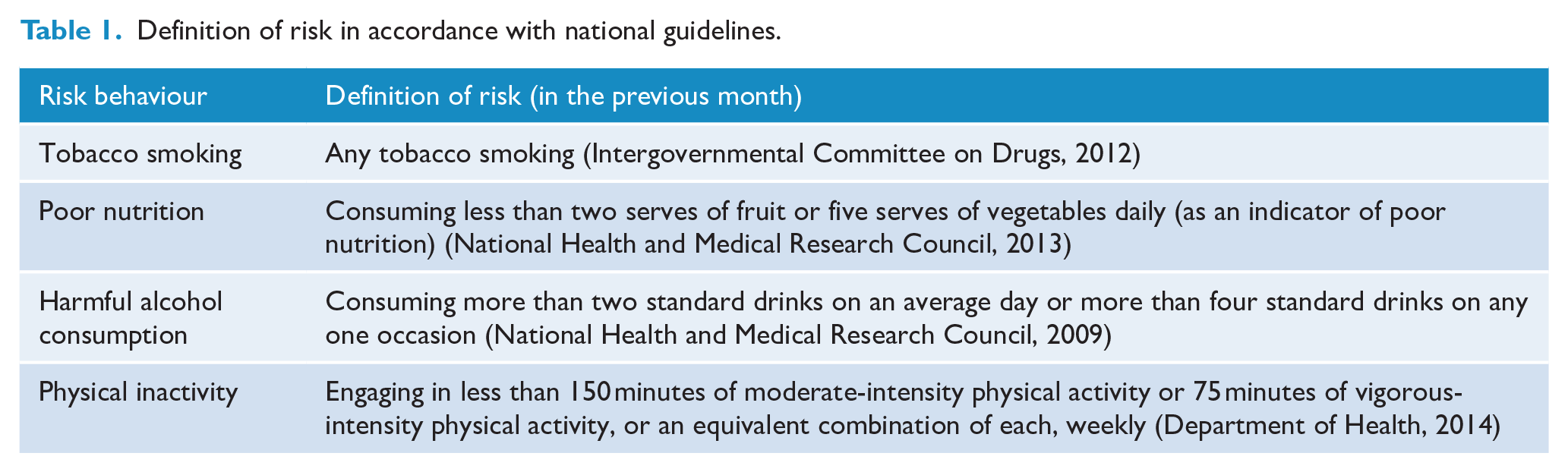
Assessment of clients’ risk behaviours, where risk was defined in accordance with Australian national guidelines (Table 1).
Brief advice regarding how clients’ risk behaviours compared to national guidelines and motivational interviewing to motivate desire for change.
Referral offered to free telephone coaching services – the NSW Quitline to support clients who reported smoking tobacco or expressed concern regarding smoking to cease smoking (Miller et al., 2003) and to the NSW Get Healthy Information and Coaching Service, to support clients who were at risk or expressed concern regarding poor nutrition, alcohol overconsumption and/or physical inactivity to make positive lifestyle changes (O’Hara et al., 2014). Additionally, all clients were offered a referral to a general practitioner (GP) for management of metabolic risks (NSW Department of Health, 2017).
Definition of risk in accordance with national guidelines.
Approximately 2 weeks following the consultation, the clinician phoned clients to assess progress and address any barriers they may have encountered in contacting the telephone services or changing behaviours.
Usual care
Clients allocated to the usual care condition received routine preventive care in accordance with the previously described local health care policy provided by their usual treating clinician (Hunter New England Local Health District, 2010). A comprehensive practice change intervention was previously implemented to support the provision of such care (Bartlem et al., 2016).
Data collection procedures
Subsequent to allocation to groups, client verbal consent was sought to participate. An information letter was mailed to eligible clients which provided a number for clients to call if they wished to opt-out. Those who did not opt out represent the study sample and were contacted 2 weeks later by trained research interviewers blinded to participant allocation to complete the baseline assessment (up to 10 attempts over 2 weeks). Surveys were undertaken using computer-assisted telephone interviews (CATIs). Contact was attempted with all participants for the conduct of the 1-month follow-up data collection regardless of whether a baseline interview had been completed.
Measures
Risk behaviour status
To assess engagement in risk behaviours in the preceding month, participants were asked (1) if they currently smoked tobacco products; (2) the number of fruit and vegetable serves typically eaten per day; (3) how often they consumed alcohol, the number of standard drinks they consumed on a typical drinking day and how often they consumed more than four standard drinks in one occasion (Fehily et al., 2017) and (4) how many minutes they spent walking and doing moderate and vigorous physical activity (45 and Up Study Collaborators, 2008) during a typical week.
Receipt of preventive care
Participants were asked about their receipt of preventive care from the community mental health service in the preceding month, without distinction as to whether from a usual treating clinician or a specialist preventive care clinician:
Assessment – whether the service asked about each of the risk behaviours (yes; no; don’t know).
Advice – participants classified as at risk (Table 1) were asked whether the service had advised them to make any changes to that behaviour (yes; no; don’t know); all participants were asked whether the service had spoken to them about metabolic risk (yes; no; don’t know).
Referral – all participants were asked whether the service had offered them a referral to the Get Healthy Service (yes; no; don’t know), and, if so, whether they had accepted (yes; no; don’t know). The same questions were asked regarding the Quitline of those participants who reported smoking in the previous month, quitting smoking in the previous 6 months or quitting smoking greater than 6 months ago, but were concerned that they might start smoking again. All participants were asked whether the service offered a referral to their GP to have their metabolic risk checked (yes; no; don’t know), and, if so, whether they accepted this referral (yes; no; don’t know).
Satisfaction with preventive care
At follow-up, participants who reported receiving at least one element of care for at least one risk behaviour from the community mental health service were asked the following questions: how satisfied they were for each care element received (not at all; somewhat; mostly; very; don’t know); how they would rate, overall, the care they received around their risk behaviours (poor; fair; good; very good; excellent; don’t know) and if the service understood their needs and concerns about their risk behaviours (not at all; somewhat; mostly; very much; don’t know).
Acceptance of the preventive care consultation offer
The specialist clinician recorded consultation attendance (attended; declined; uncontactable; ineligible) and follow-up call status (completed; declined; uncontactable) for intervention participants.
Demographics and clinical characteristics
Data obtained from electronic mental health service records included name, contact details, age, gender, primary diagnosis and length of the current episode of care. Information collected during CATI included the highest level of education, employment status, current marital status and Aboriginal and/or Torres Strait Islander status.
Statistical analyses
All analyses were undertaken using SPSS Statistics, version 25. Chi-square and t tests were undertaken to compare the characteristics of participants and eligible non-consenters at each time point. Differences between the usual care and intervention condition participants at baseline and follow-up were similarly compared.
Receipt of assessment (four outcomes) and advice (four outcomes) for each risk behaviour was dichotomised (yes vs no/don’t know).
Offer of referral to the Quitline or Get Healthy Service (two outcomes) was calculated for participants who were eligible for a referral according to the preventive care policy (Hunter New England Local Health District, 2010) (current smoker; at risk for at least one of poor nutrition, alcohol overconsumption or physical inactivity, respectively) (yes vs no/don’t know). Acceptance of a referral to each of these telephone services (two outcomes) was also calculated for all participants eligible for such a referral (yes vs no/don’t know/not offered).
Three variables were calculated to reflect the receipt of each preventive care element for all risks combined: (1) assessment for all four risks, (2) advice for all behaviours for which the participant was at risk and (3) referral to the relevant telephone service(s) for which the participant was eligible (i.e. the Quitline and/or the Get Healthy). The three outcomes pertaining to metabolic risk were dichotomised: advice provided (yes vs no/don’t know), GP referral offered (yes vs no/don’t know) and GP referral acceptance (yes vs no/don’t know/not offered).
Uptake of the preventive care consultation (attended vs did not) and telephone follow-up (completed vs did not) were dichotomised and assessed descriptively.
Responses regarding satisfaction with preventive care received were dichotomised: satisfaction with each element of preventive care separately (very/mostly vs somewhat/not at all/don’t know), overall satisfaction (excellent/very good vs good/fair/poor/don’t know) and understanding of needs and concerns (very much/mostly vs not at all/somewhat/don’t know).
Intervention effectiveness
Analyses were conducted on an intention-to-treat (ITT) basis, i.e., all participants in originally assigned conditions, utilising all the available data (n = 444) (Joshi et al., 2013; Little et al., 2012), for the 18 preventive care outcomes. Logistic regression was carried out using generalised linear mixed models (GLMMs) to assess changes in outcomes over time in the intervention compared to usual care condition. Intervention effects were determined by the risk ratio (RR) and allocation-by-time interactions. Missing data were estimated under the maximum likelihood function. Factors significantly associated with attrition were determined using logistic regression (diagnosis and length of current episode of care) and entered into all models to control for the missing-at-random assumption. Additional potential baseline confounders (age and gender) were also included in the models if significant. Based on recommendations in the literature, the threshold for statistical significance was α = 0.05 (Li et al., 2017). Estimated proportions, RRs and 95% confidence intervals (CIs) were determined from the fitted models. For one outcome (Quitline referral acceptance), a Bayesian simulation method was used as the number of events was zero. The beta posterior distributions used for simulation were based on conjugate binomial likelihoods and a uniform beta prior. Sensitivity analyses were conducted for the outcomes analysed using GLMMs (17 outcomes) to test the robustness of the results, using a conservative approach where all missing data were coded as ‘worst case scenario’ (Little et al., 2012).
Employing the same statistical method described for the primary analysis, post hoc per-protocol analyses were undertaken for the preventive care outcomes where intervention participants who did not attend the additional consultation were excluded from the analysis (usual care n = 215; intervention n = 79) (Armijo-Olivo et al., 2009).
Differences between the two conditions in regards to satisfaction with preventive care received were assessed using chi-square tests.
Results
Participants
Participant recruitment and progression through the trial are detailed in Figure 1. Clients identified as eligible for the study (n = 811) were randomised to the usual care (n = 406) and intervention condition (n = 405) (Supplementary Table S1). Of the 811 eligible clients, 2.7% (n = 22) opted out of the evaluation, with the remaining 789 clients forming the study sample. Of the study sample, 73.9% were able to be contacted at baseline (n = 583), of whom 66.7% (n = 389) completed or partially completed the interview. Of the 595 clients eligible for the follow-up interview, 73.9% were able to be contacted (n = 440), of whom 83.4% (n = 367) completed or partially completed the interview. Completion rates at baseline and follow-up did not differ by condition, χ2(1) = 0.698, p = 0.193; and χ2(1) = 0.121, p = 0.728, respectively. There were 444 participants who completed at least one interview, and 297 completed both. At baseline, participants were more likely to have been a client of the service for a shorter period of time (p = 0.003) and at both baseline (p < 0.001) and follow-up (p = 0.019) were less likely to have a diagnosis of schizophrenia, as compared to eligible non-consenters. There were no significant differences in participant characteristics between the conditions at baseline or follow-up (Table 2).
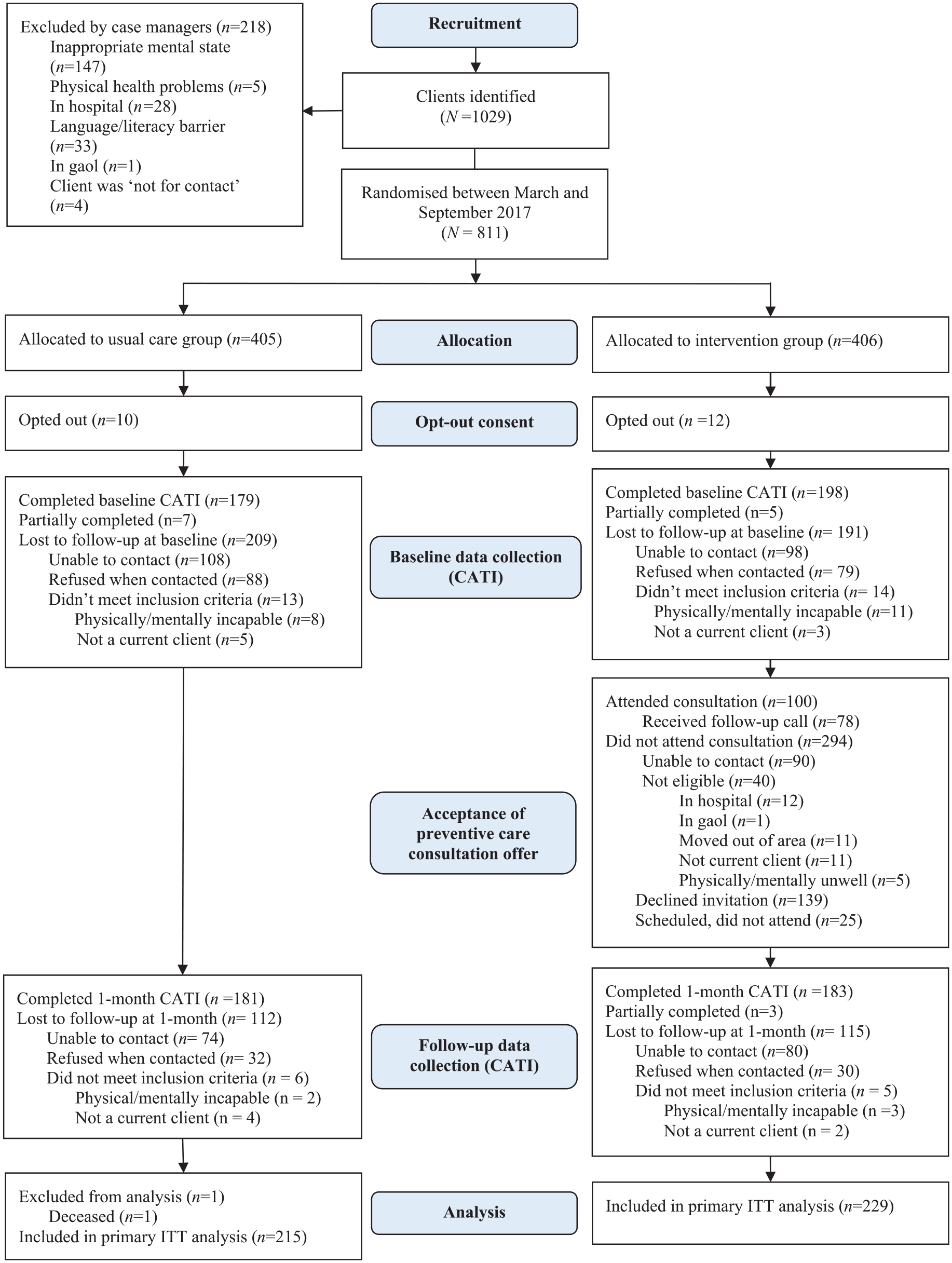
Participant flow diagram.
Characteristics of the sample.
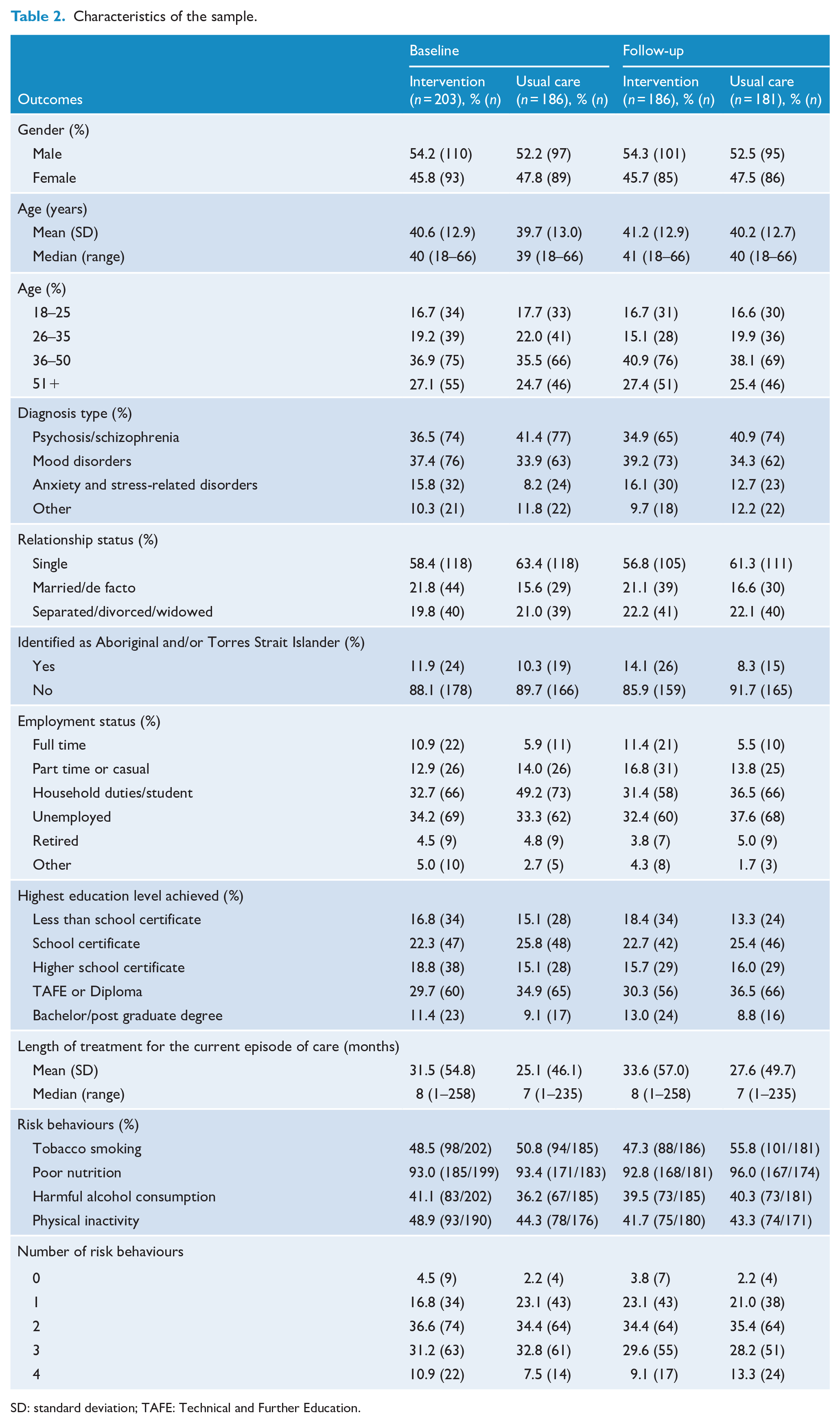
SD: standard deviation; TAFE: Technical and Further Education.
Outcome analysis
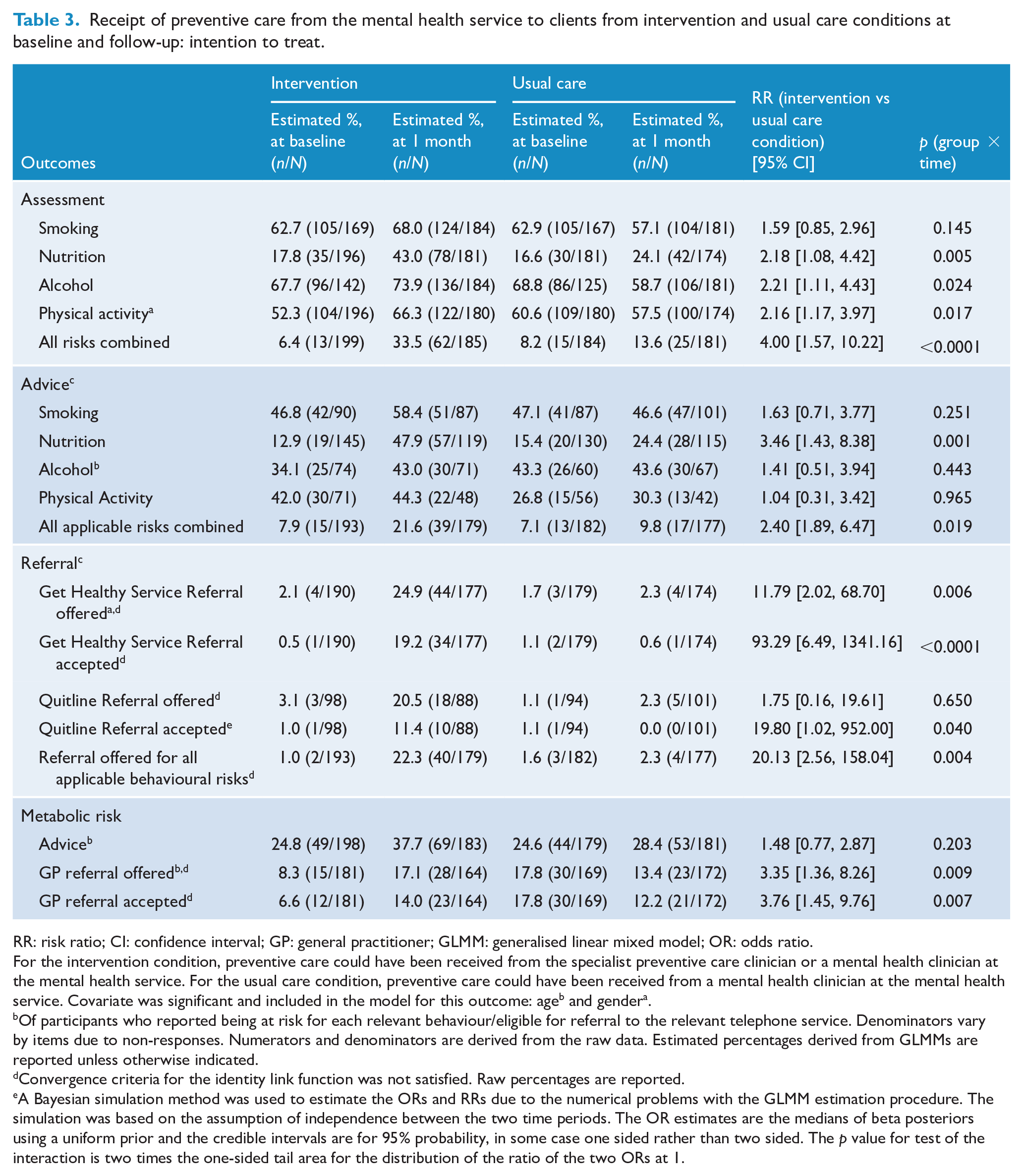
In the primary analysis, for assessment outcomes, from baseline to follow-up, there was a significantly greater absolute increase in clients reporting assessment in favour of the intervention group for four of five outcomes: nutrition (+25.2), alcohol (+6.2), physical activity (+14.0) and all four risks combined (+27.1) compared to the usual care condition (+7.5, –10.1, –3.1 and +5.4, respectively) (Table 3). The intervention effect (RR) was 2.18, 2.21, 2.16 and 4.00 times that of the usual care condition for assessment of nutrition, alcohol, physical activity and all risks combined, respectively. There was no significant differential change between groups for assessment of tobacco smoking.
Receipt of preventive care from the mental health service to clients from intervention and usual care conditions at baseline and follow-up: intention to treat.
RR: risk ratio; CI: confidence interval; GP: general practitioner; GLMM: generalised linear mixed model; OR: odds ratio.
For the intervention condition, preventive care could have been received from the specialist preventive care clinician or a mental health clinician at the mental health service. For the usual care condition, preventive care could have been received from a mental health clinician at the mental health service. Covariate was significant and included in the model for this outcome: ageb and gendera.
Of participants who reported being at risk for each relevant behaviour/eligible for referral to the relevant telephone service. Denominators vary by items due to non-responses. Numerators and denominators are derived from the raw data. Estimated percentages derived from GLMMs are reported unless otherwise indicated.
Convergence criteria for the identity link function was not satisfied. Raw percentages are reported.
A Bayesian simulation method was used to estimate the ORs and RRs due to the numerical problems with the GLMM estimation procedure. The simulation was based on the assumption of independence between the two time periods. The OR estimates are the medians of beta posteriors using a uniform prior and the credible intervals are for 95% probability, in some case one sided rather than two sided. The p value for test of the interaction is two times the one-sided tail area for the distribution of the ratio of the two ORs at 1.
For advice outcomes, there were significantly greater absolute increases in favour of the intervention condition for two of the five outcomes: nutrition (+35.0%) and all applicable risks combined (+13.7), compared to the usual care condition (+9.0 and +2.7, respectively) (Table 3). The intervention effect was 3.46 and 2.40 times that of the usual care condition for nutrition and all applicable risks combined, respectively. There was no significant differential change between groups for the remaining advice outcomes (smoking, alcohol and physical activity).
For referral outcomes, there were significant absolute increases from baseline to follow-up in favour of the intervention group for offer of a referral to Get Healthy (+22.8), all applicable behaviour change telephone services (+21.3) and to a GP for metabolic risk assessment (+8.8) compared to the usual care condition (+0.6, +0.7 and –4.4 respectively) (Table 3). The intervention effect was 11.79, 20.13 and 3.35 times greater than the usual care condition for offer of a referral to Get Healthy, all applicable telephone services and a GP, respectively. The differential change between groups regarding offer of referral to the Quitline was not significant.
A positive intervention effect was evident for all three outcomes pertaining to acceptance of a referral. Participants in the intervention condition were significantly more likely report an increase in acceptance of a referral to Get Healthy (+18.7), the Quitline (+10.4) and to a GP (+7.4) compared to usual care (–0.5, –1.1 and –5.6, respectively). The intervention effect (RR) was 93.29, 19.80 and 3.76 times greater compared to usual care for acceptance of a referral to Get Healthy, Quitline and a GP, respectively.
Sensitivity analysis
In the sensitivity analysis, outcomes were similar to the primary analysis, with the exception of assessment for alcohol and assessment for physical activity, which were no longer significant (Supplementary Table S2).
Per-protocol analysis
In the per-protocol analysis, similar effects to the primary analysis were found, with two additional significant outcomes obtained: assessment for smoking (RR = 3.58; 95% CI = [1.42, 9.04]) and advice regarding metabolic risk (RR = 3.31; 95% CI = [1.37, 8.00]) (Supplementary Table S3).
Preventive care consultation uptake
Of participants who were eligible and able to be contacted by the specialist clinician, 37.8% (n = 100) attended the consultation (Figure 1). Of those who attended, 78% (n = 78) received the follow-up call. Of the intervention participants who completed the baseline interview (n = 196), 35.2% (n = 69) attended the consultation, and, of those who completed the follow-up interview (n = 183), 38.8% (n = 71) attended.
Satisfaction with preventive care
Outcomes regarding satisfaction with preventive care received from the community mental health service at follow-up are reported in Table 4. Overall, the majority of the participants reported high levels of satisfaction, with more than 66% reporting being ‘mostly’ or ‘very’ satisfied across the outcomes. No significant differences were identified between the two conditions.
Satisfaction with the receipt of preventive care received from the mental health service at follow-up.
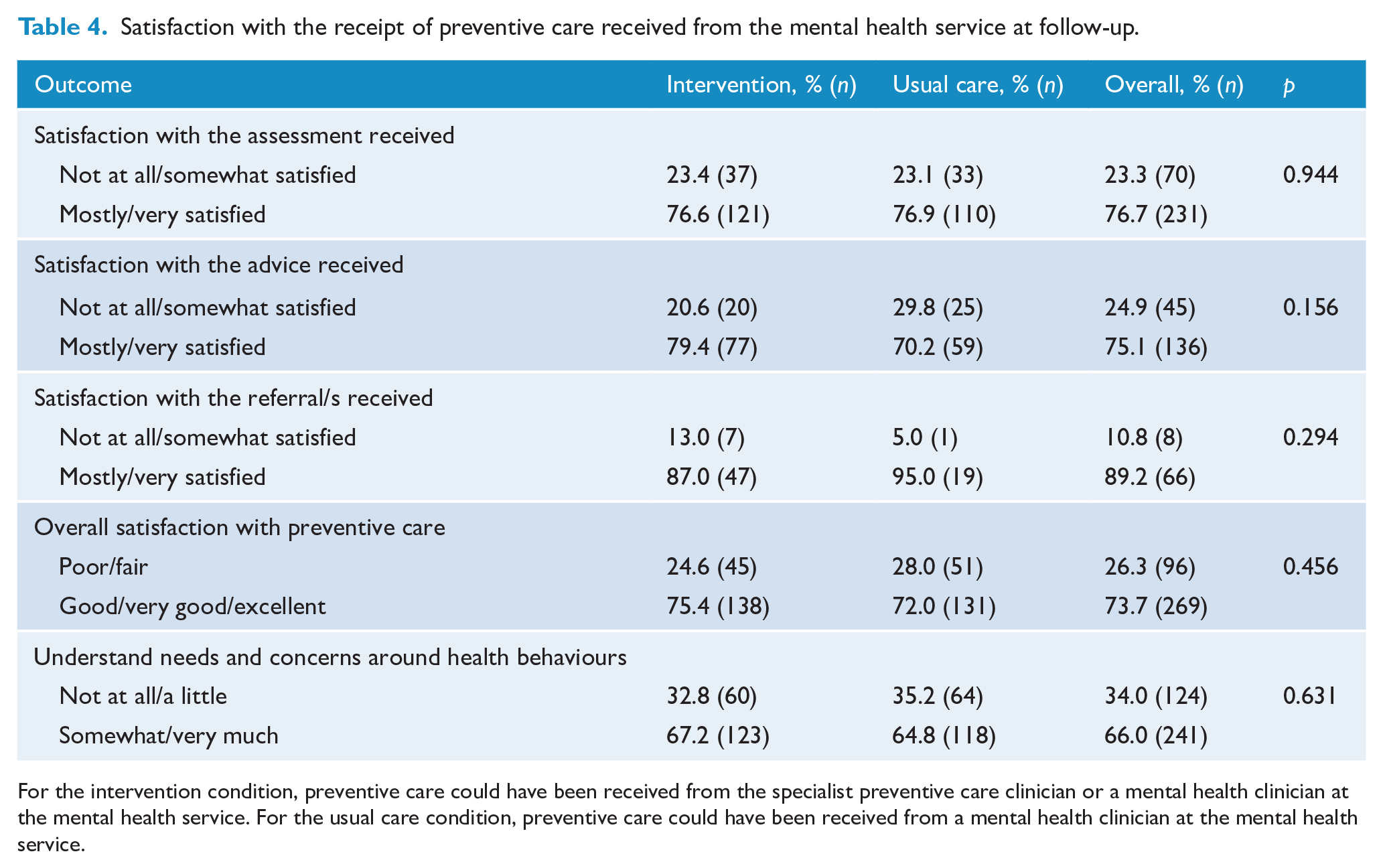
For the intervention condition, preventive care could have been received from the specialist preventive care clinician or a mental health clinician at the mental health service. For the usual care condition, preventive care could have been received from a mental health clinician at the mental health service.
Discussion
This paper is the first to rigorously and comprehensively examine the effects of an additional preventive care consultation with a specialist clinician on the provision of specific elements of preventive care addressing multiple risk behaviours to clients of a community mental health service. The primary analysis found that participants in the intervention condition were significantly more likely, relative to preventive care provision in routine consultations only, to have received assessment, advice and referral for all risk behaviours combined, with a significant effect being observed for at least one of the individual risk behaviours for each element of care. These findings suggest that offering clients an additional consultation with a specialist preventive care clinician represents an effective approach for increasing the delivery of preventive care to people with a mental illness, a currently underserved population group with a particular need for such care.
For the preventive care elements of assessment and referral, the study found a significant effect for almost all (10 of 12) outcomes. However, only one significant outcome was found with regard to ‘advice’ for individual risk behaviours (nutrition). The latter finding could be due to measurement factors such as the limitations of self-report, including participants’ knowledge of what constitutes ‘advice’, and recall. This observed lack of effect is in contrast with the significant increases for ‘referral’ outcomes. The latter finding is of particular importance as ‘referral’ has been suggested to be the most critical element of preventive care to ensure successful long-term behaviour change (Glasgow et al., 2004) and has been the least likely to have been positively affected in previous trials of interventions to increase the provision of preventive care in routine health consultations (Bartlem et al., 2016; McElwaine et al., 2014). However, the overall proportion of intervention participants who accepted referrals to the Quitline (11%), Get Healthy Service (19%) and GPs (14%) could be improved. While not possible in this study, future research with sufficient statistical power may determine factors associated with accepting such referrals, to inform strategies to increase acceptance and ensure that clients receive extended, specialist behaviour change support.
The intervention effect in this study varied across the risk behaviours, being least effective for smoking, with only one significant effect being observed (i.e. Quitline referral acceptance). This lack of effect for smoking outcomes may be attributable to the high baseline levels of provision of assessment’ and ‘advice’ for smoking (above 45%). Post hoc power analyses indicated that the study may have been underpowered to detect an intervention effect for smoking assessment (detectable: 14% vs observed: 11% difference) and advice (detectable: 20% vs observed: 12% difference). A previous RCT of this model of care (Osborn et al., 2010), as well as previous trials of interventions to increase preventive care provision in routine consultations in both community general health (McElwaine et al., 2014) and mental health (Bartlem et al., 2016) settings, have been ineffective in increasing provision of assessment, advice and referral for smoking. Further research is required to identify the determinants of smoking cessation care provision as a basis for developing relevant practice change strategies.
Approximately a third of the eligible participants who were offered the additional preventive care consultation attended. In line with clinical guidelines (Fiore et al., 2008), the consultation was offered on a universal basis, i.e., to all clients regardless of their demographic or risk characteristics. The observed level of attendance is less than a previous trial of this model of care (75%) (Rogers et al., 2016). However, this previous trial employed narrower eligibility criteria, including only clients who expressed willingness to attend such an additional consult. A need exists for further research to identify the barriers to and facilitators of client acceptance of an offer for the additional consultation, particularly when such an offer is made universally. Such information is required to inform the inclusion of strategies to increase client motivation and interest in taking up the additional consultation (Rogers et al., 2016). In addition, alternative approaches to the delivery of such a consultation should be considered. One potential approach involves the consultation being provided by a person with a lived experience of mental illness (‘peer worker’), given their ability to provide advice and role modelling informed by their lived experiences (Gillard et al., 2013). Previous research suggests that receiving healthy lifestyle support from a peer worker may be perceived by people with a mental illness as more acceptable than a mental health professional (Williams et al., 2011).
A further opportunity for enhancing the uptake of the model of care assessed in this study, and its overall effectiveness, involves identifying strategies for increasing the provision of preventive care in routine consultations. Such care provision has been reported by community mental health service clients to be highly acceptable (Bartlem et al., 2015b). However, improving its delivery in this clinical context has been found to be challenging. For example, a previous Australian study examining the effectiveness of an evidence-based practice change intervention in increasing the provision of preventive care in routine mental health consultations found a significant effect in only 1 of 16 preventive care outcomes (Bartlem et al., 2016). Tailoring the practice change strategies to the particular circumstances, context and culture of community mental health services may enhance their effectiveness. To date, such tailoring has not been reported.
The findings suggest that there is potential for the specialist clinician model and warrants consideration of its feasibility to be implemented. A key component of such an assessment involves its feasibility in terms of the additional resources required and benefits accrued. To address this issue, analysis is required of its cost-effectiveness and budget impact (Bilinski et al., 2017). Only one previous study, undertaken in the United States, has assessed the cost-effectiveness of this model of care (Druss et al., 2011). The study reported that, from the perspective of the health system, it was more cost-effective than usual care in increasing the quality of preventive care services received: physical examinations, screening tests, vaccinations and health education. No economic analyses for this model have been conducted in Australia, nor have analyses been reported where the focus of the additional consultation was specifically preventive care for risk behaviours.
Results from this study suggest that the intervention and usual care condition did not significantly differ in terms of clients’ reported satisfaction with their receipt of preventive care, with over two thirds of participants in both groups reporting high levels of satisfaction for all care elements. Previous research has also found that clients receiving preventive care in routine consultations and clients receiving a specialist clinician–delivered intervention both reported similar, high levels of satisfaction (Osborn et al., 2010).
Limitations
With regard to limitations, there were significant differences between those who did and did not consent to participate in terms of psychiatric diagnosis and length of time in treatment. To address the risk of this potential bias influencing the study findings, these characteristics were entered into all models. These factors should be considered in the development of future interventions, suggesting a need for specific strategies to target these hard-to-reach individuals. Second, although specified in the study protocol, data regarding the number of appointments with the mental health service were unable to be obtained. In lieu of this information, length of time in treatment was utilised as an alternative. As the number of appointments has been reported to be associated with receipt of preventive care (Bartlem et al., 2015b), future studies may wish to include this as a covariate. Third, a large proportion of clients were unable to be contacted for both the offer of the preventive care consultation (by the specialist clinician) and data collection (by telephone interviewers). The difficulty in contacting, recruiting and retaining people with a mental illness has previously been acknowledged as particularly challenging in both research (Kanuch et al., 2016) and clinical settings (Olfson et al., 2009). Further qualitative research is required to investigate the factors from a client perspective that may limit their participation in such research and in the uptake of such care. Finally, data regarding ethnicity (other than Aboriginal or Torres Strait Islander status) and language were not collected. While this trial was undertaken within the context of real-world mental health service delivery, replication of the study with a more rigorous trial design and in multiple mental health service sites is warranted. Furthermore, given the acknowledged role of GPs in providing preventive care to people with a mental illness, research is needed to explore strategies to additionally support provision of preventive care in this setting (Royal Australian College of General Practitioners, 2015).
Conclusion
Mental health services face significant challenges in providing comprehensive preventive care. This study suggests that offering clients preventive care via an additional consultation with a specialist preventive care clinician embedded in a community mental health service may be an effective model for increasing the provision of comprehensive multi-risk preventive care. It provides evidence to support such care being provided systematically, regardless of characteristics such as psychiatric diagnosis or interest in change. Further research examining the feasibility of implementing this model of care as well as strategies for enhancing its effectiveness is required.
Supplemental Material
Supplementary_tables – Supplemental material for Effectiveness of embedding a specialist preventive care clinician in a community mental health service in increasing preventive care provision: A randomised controlled trial
Supplemental material, Supplementary_tables for Effectiveness of embedding a specialist preventive care clinician in a community mental health service in increasing preventive care provision: A randomised controlled trial by Caitlin MC Fehily, Kate M Bartlem, John H Wiggers, Paula M Wye, Richard V Clancy, David J Castle, Andrew Wilson, Chris E Rissel, Sonia Wutzke, Rebecca K Hodder, Kim Colyvas, Fionna Murphy and Jenny A Bowman in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors would like to acknowledge the staff and clients of the community mental health service and the CATI interviewers for their support and contribution to the project. They would like to thank Christophe Lecathelinais and Frank Tuyl for their statistical assistance. They would also like to acknowledge Rhonda Patrick for her contribution as the specialist preventive care clinician. The authors dedicate this work to their colleague, mentor and, above all, friend Associate Professor Sonia Wutzke (1970–2017).
Author Contributions
All authors provided substantial contribution to the conception and design of the study. C.M.C.F. led the manuscript development. C.M.C.F., K.M.B. and K.C. contributed to the analysis of the data. C.M.C.F., K.M.B., J.H.W., P.M.W., R.V.C., D.J.C., A.W., C.E.R., R.K.H., K.C., F.M. and J.A.B. provided substantial contribution to editing and critical revision of the manuscript, and read and approved the final manuscript to be published.
Availability of Support Data
The datasets generated and analysed during the current study are not publicly available to preserve the privacy of participants; however, they are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was supported by The Australian Prevention Partnership Centre through the NHMRC partnership centre grant scheme (Grant ID: GNT9100001) with the Australian Government Department of Health, NSW Ministry of Health, Australian Capital Territory (ACT) Health, The Hospitals Contribution Fund of Australia (HCF) and the HCF Research Foundation and by Hunter New England Population Health. The study funders had no role in the study design, data collection, data analysis, interpretation or manuscript preparation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.