
Abstract
Research studies of schizophrenia have focused mainly on its cardinal positive and negative symptomatology. However, recent attention to the early phases of this illness has generated a renewed interest in the subtle, self-experienced cognitive and emotional changes that have been described since the earliest articulation of dementia praecox [1,2]. Subjective experiences are subtle subjective disturbances in drive, affect, thinking, language, perception, motor action, vegetative functions, and stress tolerance [1–3], a thorough description of which is provided within the framework of the concept of basic symptoms [1,2,4,5]. These include various disturbances in the stream of consciousness (e.g. thought disturbance), perceptual aberrations, anomalous bodily experiences (e.g. somatic depersonalization), a lack of a sense of immersion in the world (e.g. diminished vitality), and various other disorders of self-consciousness [1,2,4–9]. These experiences, if present, can be assessed in most affected subjects with the help of guided questioning [1,10]. Recent studies have shown that subjective experiences have important implications for early recognition of schizophrenia and related disorders [1,11–14].
In recent years, Danish researchers have found that subjective experiences discriminate schizophrenia in remission from psychotic bipolar disorder in remission [15]. Further, in a prospective longitudinal study of first-admission cases, they demonstrated that subjective experiences selectively aggregate in schizophrenia-spectrum disorders but not in the diagnostic categories outside the spectrum [8,16]. They also reported that reliable measurements of subjective experiential anomalies can be obtained in patients with schizophrenia [7]. These results strongly support the notions that certain subjective experiences represent a specific disturbance underlying schizophrenia and that this disturbance may develop into positive symptoms under certain conditions [11,14,17–19]. However, there have been conflicting findings with regard to the relationship between subjective experiences and psychopathological dimensions in schizophrenia. Several studies reported that subjective experiences were associated with positive symptoms in acute schizophrenia [20–23] and in chronic schizophrenia [14], whereas other studies found no such correlation with positive symptoms in acute schizophrenia [24] or reported a significant relationship with negative symptoms in chronic schizophrenia [25]. Moreover, few studies have considered or made reference to the correlations between subjective experiences and extrapyramidal adverse effects. Previous studies have reported that drug-induced Parkinsonism and akathisia are significantly associated with a variety of subjective cognitive-perceptual deficits as assessed by the scale developed for evaluating subjective experiences [14,24,26], which has important implications for compliance with antipsychotic treatment.
Therefore, the relationship between subjective experiences and psychopathological dimensions in schizophrenia remains inconclusive. In the present study we investigated the relationship between subjective experiences and psychopathology in outpatients with schizophrenia by performing comprehensive assessments of subjective symptoms, objective psychopathology, and extrapyramidal adverse effects.
Materials and methods
Subjects
A total of 67 outpatients (38 men, 29 women) were enrolled in the study. All patients met the DSM-IV criteria for schizophrenia [27], and they were required to be clinically stable for at least 4 weeks on a constant dose of risperidone or haloperidol prior to study entry. Patients were not included if they had concurrent medical or neurological disorders. Written informed consent was obtained from all subjects after a full explanation of the study procedure. The subjects had a mean age of 36.1 ± 9.7 years and a mean duration of illness of 7.9 ± 6.2 years. The mean years of formal education were 11.0 ± 3.7. Thirty-eight subjects were receiving haloperidol with a mean dosage of 10.9 ± 8.8 mg/day. Twenty-nine subjects were taking risperidone with a mean dosage of 4.1 ± 2.2 mg/day. With respect to anticholinergics and benzodiazepines that were used for extrapyramidal side effects, akathisia (including subtle subjective akathisia) or agitation, 24 subjects were administered both anticholinergics and benzodiazepines, 25 subjects were administered anticholinergics alone, and 7 subjects were administered benzodiazepines only. The mean dosages of anticholinergics and benzodiazepines were 1.2 ± 1.2 mg/day (benzotropine equivalents) [28] and 2.7 ± 4.3 mg/day (diazepam equivalents) [29]. The study was approved by the local ethical committee, and all procedures used in the study were conducted in accordance with international ethical standards, Declaration of Helsinki.
Assessments
Subjective experiences were comprehensively assessed using the Frankfurt Complaint Questionnaire (FCQ) [10], which was standardized for the Korean population [30]. The FCQ is one of the most widely used rating scales for subjective experiences [10] and its metric properties have been well established [30–33]. It rates the current level of subjective experiences [10,30]. The FCQ is a well-constructed instrument for self-assessment and is easy to administer [11,30]. The FCQ scores have been found to be strongly correlated with the objective neuropsychological test results [34]. The Korean version of the FCQ consists of 103 items concerning a wide range of subjective cognitive, emotional and perceptual experiences [30]. The items are subdivided into 10 phenomenological subscales, i.e. anxiety (e.g. ‘I frequently feel anxious without any reason’), disorder of selective attention (e.g. ‘Noise, which was nothing before, now irritates me and hinders me from concentration’, ‘If several people talk together, all are mixed up and I am unable to concentrate on one person’, ‘Sometimes it is hard to keep concentrating on one thing’), deterioration of discrimination (e.g. ‘Sometimes when I see something, it is confusing whether it is what I actually see or just an imagination’), psychomotor disorder (e.g. ‘My body occasionally moves quite differently from my intention’), perceptual disorder (e.g. ‘Sometimes people look distorted’), cognitive floating (e.g. ‘Sometimes I am confused because too many thoughts come into my mind’), blocking symptoms (e.g. ‘Sometimes my thoughts stop and I have to wait in silence’), language disorder (e.g. ‘Recently it is hard for me to speak or write logically’), automatic behaviour disorder (e.g. ‘When doing daily routine work, I have to think for a long time about how to do it’), and disorder of coping responses (e.g. ‘I avoid stressful things’, ‘I try to escape from the situation that may confuse my mind’, ‘I have to be very careful because I may make a mistake in everyday life’) [30].
The current severity of symptoms of schizophrenia was evaluated using the Manchester Scale (MS) [35], from which positive and negative symptom scores were derived. The positive symptom score was the total sum score of the delusion, hallucination, and incoherence subscales, and the negative symptom score was the total sum score of the flattened affect, poverty of speech, and psychomotor retardation subscales.
Extrapyramidal adverse effects were assessed in the domains of drug-induced Parkinsonism (DIP), akathisia, and tardive dyskinesia (TD). DIP was assessed using the Simpson-Angus Scale (SAS) [36], and TD was assessed using the Abnormal Involuntary Movement Scale (AIMS) [37]. Drug-induced akathisia was assessed using the Barnes Akathisia Rating Scale (BARS) [38], which was developed to evaluate both the mental symptoms and motor signs of akathisia.
Each patient underwent a thorough assessment of schizophrenic symptoms and extrapyramidal adverse effects by an investigator (J.H.K.), who had been sufficiently trained in the use of the scales and was familiar with the assessment of psychotic symptoms and drug-induced movement disorders [39,40], and was assessed using the FCQ in the presence of a research assistant who monitored whether or not the questions were completely understood.
Statistical analysis
To examine the association between subjective experiences and psychopathological dimensions, Pearson's partial correlation analysis was performed between the FCQ and the MS scores, controlling for the severity of extrapyramidal adverse effects. For all analyses, the level of statistical significance was defined as p < 0.05 (two-tailed). All statistical analyses were performed using SPSS 14.0 for windows (SPSS, Chicago, IL).
Results
The FCQ score had no significant correlations with age (r = −0.07, p = 0.55), gender (r = −0.07, p = 0.59), duration of illness (r = 0.09, p = 0.49), years of education (r = −0.15, p = 0.23), or antipsychotic dose (r = 0.01, p = 0.95). The scores of the FCQ correlated significantly with those obtained from the extrapyramidal adverse effects assessment scales (p < 0.05) (Table 1). The global score of the BARS had significant positive correlations with the FCQ total score and subscales scores (anxiety, disorder of selective attention, deterioration of discrimination, psychomotor disorder, cognitive floating, blocking symptoms, automatic behaviour disorder, and disorder of coping responses) (p < 0.05) (Table 1). The AIMS total score had significant positive correlations with the FCQ total and subscale scores (psychomotor disorder, cognitive floating, blocking symptoms, automatic behaviour disorder, and disorder of coping responses) (p < 0.05) (Table 1). The FCQ total score tended to have a positive correlation with the SAS total score (p = 0.06) (Table 1).
Correlation coefficients between subjective experiences and extrapyramidal adverse effects
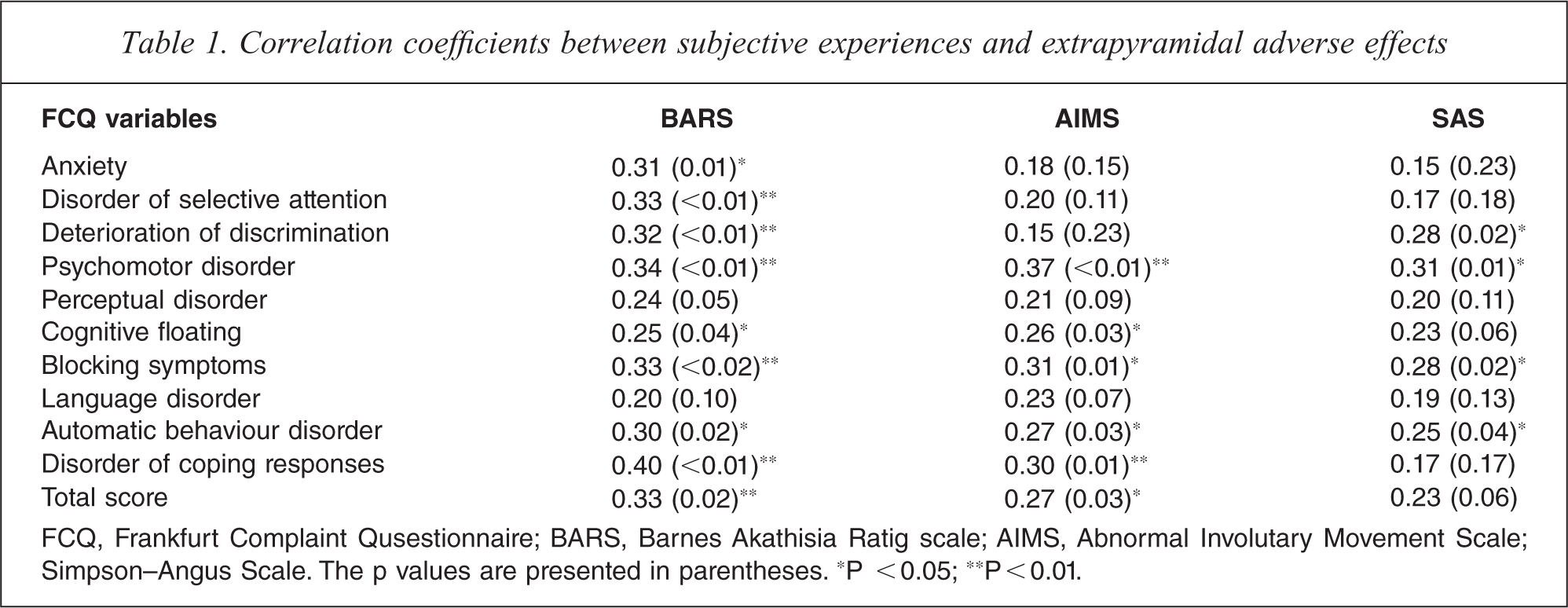
FCQ, Frankfurt Complaint Qusestionnaire; BARS, Barnes Akathisia Ratig scale; AIMS, Abnormal Involutary Movement Scale; Simpson–Angus Scale. The p values are presented in parentheses. ∗P < 0.05; ∗∗P <0.01.
The correlations between subjective experiences and psychopathology are presented in Table 2. Correlation analysis controlling for the BARS, AIMS, and SAS scores revealed that the MS positive symptom score had significant positive correlations with the FCQ total score and subscales scores (anxiety, disorder of selective attention, deterioration of discrimination, perceptual disorder, cognitive floating, blocking symptoms, language disorder, automatic behaviour disorder, and disorder of coping responses) (p < 0.05) (Table 2). The MS negative symptom score did not have significant correlations with the FCQ scores (p > 0.05), except for the psychomotor disorder subscale score (p = 0.03) (Table 2).
Partial correlation coefficients between subjective experiences and psychological dimensions, controlled for the severity of extrapyraidal advmerse effects
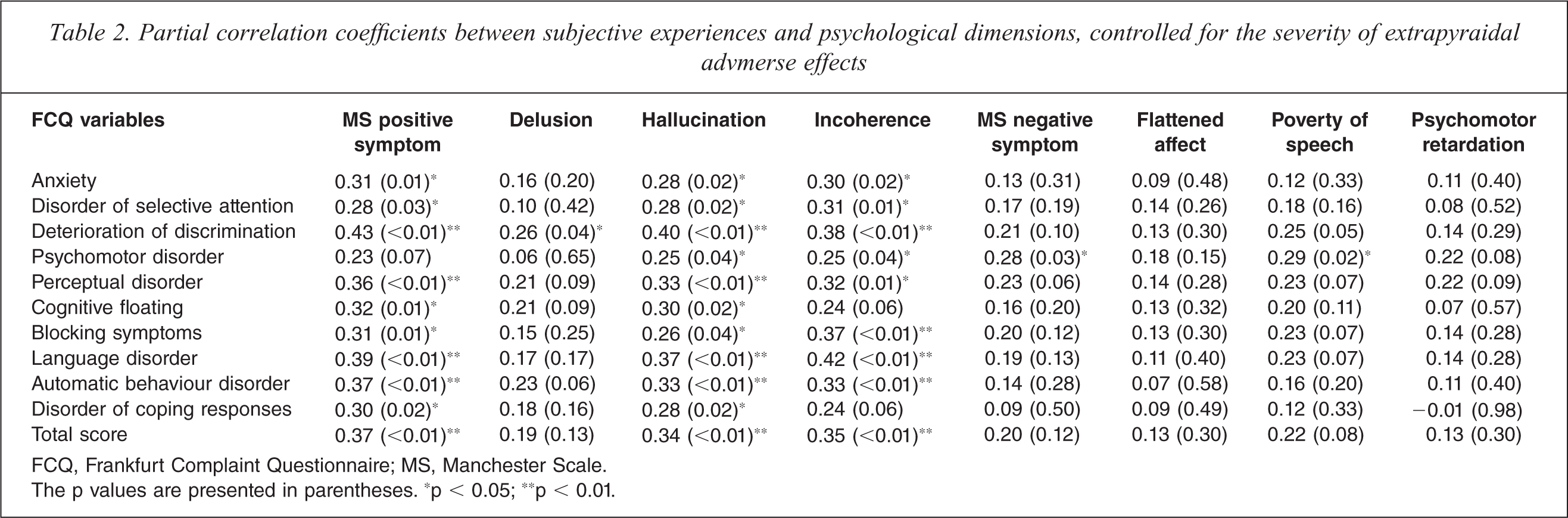
FCQ, Frankfurt Complaint Questionnaire; MS, Manchester Scale.
The p values are presented in parentheses. ∗p < 0.05; ∗∗p < 0.01.
Discussion
Unlike objective psychopathology, subjective experiences have been a neglected area of research in schizophrenia [12]. In particular, assessing the patient's subjectivity has been limited, because of concerns about its reliability. However, the self-perceived cognitive-perceptual dysfunction has been increasingly acknowledged for the assessment of both functional and symptomatic outcome in schizophrenia [41,42]. In recent years, the importance of subjective measures has been repeatedly addressed in the studies on schizophrenia [43–45]. In addition, there has been a suggestion that subjective complaints may represent a truer assessment of the well-being of schizophrenic patients than measures of manifest psychopathology [46].
In the present study, by using the FCQ, one of the most frequently used scales for assessing subjective experiences and one which covers a wide range of domains, we examined the correlation between subjective experiences and objective psychopathology, controlling for the confounding factor of extrapyramidal adverse effects. Out results show a significant correlation between subjective experiences and positive psychopathology, suggesting that they may share a common underlying neural basis. These results are in line with previous studies that have suggested that subjective experiences represent an underlying disturbance of schizophrenia and they may also produce positive psychopathology [11,20,47]. Negative symptoms, on the other hand, may be associated with less subjective experiences or alternatively patients suffering from them may not be capable of identifying subjective experiences as a consequence of the general blunting of mental process [48,49].
It should be noted that previous studies suggested that subjective experiences are associated with positive symptoms mainly in the acute phase of the illness, and may be related to negative symptoms in the chronic phase [50]. In the present study, the subjects had a mean duration of illness of more than 5 years, indicating post-acute phase of their illness. According to our study, the relationship between subjective experiences and positive symptoms may not depend on the phase of the illness, suggesting that patients are aware of some subjective disturbance associated with positive psychotic phenomena throughout the illness [47]. Our results and those of the previous studies suggest that anomalous subjective experiences may be fundamental or core subjective clinical manifestations of schizophrenia. Thus, subjective disturbances may represent a potentially important trait phenotype for the clinical characterization of the schizophrenia spectrum [6]. This aspect has important implications for the issues of early identification and intervention strategies for subjects at risk of psychosis, in that the subjective experiences may serve as useful clinical features for early detection, supplementing and enriching current prodromal and high risk models, which provide a prodromal set of symptoms that lead to schizophrenia and could be specific and accurate enough to warrant early treatment intervention before the onset of the disorder [51–53], with a potential phenotype associated with schizophrenia-spectrum disorders [6,7,9,54]. However, it is possible that the subjective experience of schizophrenia is heterogeneous and that the phase of the illness and the severity of symptoms may influence the specific factor structure of subjective experiences [14]. Future studies are required to compare the relationships between subjective experiences and objective psychopathology for patients with first-episode and chronic schizophrenia to clarify the issue.
Although the relationship between subjective experiences and positive psychopathology was found to be significant, the magnitudes of the correlations were moderate, accounting for a small portion of the variance. The results indicate that the majority of subjective experiences may constitute a unique dimension distinct from the classical objective psychopathology, as previously proposed [12]. The results are also in line with previous suggestions that subjective experiences in schizophrenia may be heterogeneous and may fall into two groups, one relatively independent of objective psychopathology and the other associated with positive symptoms [14].
In the present study, we found a significant association between subjective experiences and extrapyramidal adverse effects, suggesting a variety of cognitive complaints associated with neurological side effects [26]. The results have important implications for early therapeutic interventions for extrapyramidal adverse effects considering their significant association with the subjective cognitive dysfunction. In addition, given the phenomenological overlap between motor features and negative symptomatology and the complex nature of drug-induced movement disorders [40,55], the influence of the severity of extrapyramidal adverse effects should be considered in the analysis of the relationship between subjective experiences and psychopathology.
The interpretation of the results of the present study, however, should be considered in light of some limitations. Several factor analyses of the FCQ have reported a one-factor solution, suggesting a unidimensionality of the scale [31–33]. The unidimensionality could be explained by the fact that the FCQ comprises a small number of items rating negative dimensions of subjective experiences [11], which may account for the absence of significant correlations between the FCQ and the negative symptomatology in the present study. Therefore, the results need to be replicated using other rating scales for subjective experiences, such as the Bonn Scale for the Assessment of Basic Symptoms (BSABS), the reliability of which has been previously established [7,13]. In addition, the study was a cross-sectional one and the sample size was small. Further prospective study with a larger sample is warranted to confirm the stability of the relationships. The subjects were all outpatients receiving stable doses of antipsychotics, and as such, the findings may not be generalized to a more diverse group of patients. Further studies with a large sample of subjects at different stages of the illness are required to obtain valuable insight and understanding into the complex nature of subjective experiences in schizophrenia.
In conclusion, the results of our study suggest that subjective experiences are significantly associated with positive symptomatology in schizophrenia, suggesting that they may share a common underlying neural basis. Future prospective studies are necessary to confirm the stability of the relationships observed and to explore the diagnostic and therapeutic implications of subjective experiences in a diverse group of patients with schizophrenia.
Footnotes
Acknowledgements