
Abstract
Objective:
This study aimed to provide a picture of who uses Better Access treatment services, how they do so and what the benefits are.
Methods:
We conducted an observational prospective study involving independent cohorts from the Australian Longitudinal Study on Male Health (Ten to Men [TTM]) and the Australian Longitudinal Study of Women’s Health (ALSWH). We used data from two pairs of baseline (T0) and follow-up (T1) waves for those aged ⩾ 18 in TTM and those in the 1989–1995, 1973–1978 and 1946–1951 cohorts in ALSWH. Using survey data and linked Medicare Benefits Schedule (MBS) claims data, we identified participants with ‘mental health need’ at T0 who had and had not used Better Access treatment services between T0 and T1.
Results:
Proportions of Better Access users varied across study cohorts and analyses, with 45% being the highest. Those who used Better Access treatment services typically accessed 5–6 sessions, usually from clinical psychologists and/or psychologists. Between half and three-quarters paid out-of-pocket costs (usually $80–$100/session). Typically, around half of those who used Better Access had better mental health at T1 than T0. Severity of mental health problems at baseline was strongly predictive of both Better Access use and improvements in mental health.
Conclusion:
Australian adults with mental health need make varying use of Better Access treatment services, but the programme appears to serve those with high levels of need relatively well.
Keywords
Introduction
Introduced in 2006, Australia’s Better Access initiative enables consumers with diagnosed mental disorders to receive psychological therapy services from clinical psychologists and focussed psychological strategies from psychologists, social workers, occupational therapists (OTs) and general practitioners (GPs) or prescribed medical practitioners (PMPs). Consumers need a mental health treatment plan from a GP/PMP to access these services. Each service is listed as a Medicare Benefit Schedule (MBS) item with a schedule fee. A percentage of this fee is provided to consumers as a rebate, and they pay the residual, except where the provider accepts the Medicare benefit as the full payment (i.e. bulk-bills).
The number of individual treatment sessions available through Better Access has varied. Initially, consumers could receive up to 18 sessions per year (six, plus two further sets of six following GP/PMP reviews). The number of sessions was reduced to 10 from November 2011, but transitional arrangements introduced in March 2012 enabled an additional six sessions to be provided in exceptional circumstances (i.e. a maximum of 16). From January 2013 until March 2020, the maximum was 10 sessions. At that point, an additional 10 sessions were introduced to counter the mental health impacts of the COVID-19 pandemic (i.e. a maximum of 20); these ceased in December 2022. Additional group sessions are available alongside individual sessions.
We have undertaken two evaluations of Better Access, one in 2009–2011 and one in 2021–2022 (Pirkis et al., 2011, 2022). This paper reports on one of 10 studies comprising the second evaluation; eight of the others are reported in this issue of the Australian and New Zealand Journal of Psychiatry (Chilver et al., 2026; Currier et al., 2026; Harris et al., 2026; Newton et al., 2026; Pirkis et al., 2026a, 2026b; Tapp et al., 2026a, 2026b). This study drew on data from the Australian Longitudinal Study on Male Health (Ten to Men [TTM]) and the Australian Longitudinal Study of Women’s Health (ALSWH) to provide a picture of who uses Better Access treatment services, how they do so and what the benefits are.
Methods
Design and data sources
We conducted an observational prospective study involving independent cohorts from TTM and ALSWH. TTM used a stratified random household sampling strategy to recruit a single cohort of 16,021 males (13,896 aged 18–55, and 2125 aged 10–17) in 2013/2014 (Pirkis et al., 2017). ALSWH recruited three cohorts based on birth-year by randomly sampling from the Medicare database in 1996 and a fourth by online and offline methods (e.g. social media posts, printed materials) in 2013: 1973–1978 cohort (14,247 aged 18–23); 1946–1951 cohort (13,714 aged 45–50); 1921–1926 cohort (12,432 aged 70–75); and 1989–1995 cohort (17,010 aged 18–23) (Brown et al., 1998; Loxton et al., 2015). When we conducted the current study (mid-2022), the TTM cohort had been followed for three waves and the ALSWH cohorts for 6–9 waves. Both TTM and ALSWH have linked participants’ survey data to their MBS and Pharmaceutical Benefits Scheme (PBS) claims data (https://tentomen.org.au/ and https://alswh.org.au/).
The longitudinal, linked data from TTM and ALSWH enabled us to identify participants with ‘mental health need’ at a given wave and determine whether they used Better Access treatment services between that and a subsequent wave. We were able to compare those who did and did not use these services, look at patterns of Better Access care, and gauge whether Better Access use was associated with mental health improvements.
Sampling frame and participant selection
We restricted the samples to those aged ⩾ 18 in TTM and those in the 1989–1995, 1973–1978 and 1946–1951 cohorts in ALSWH (we excluded the ALSWH 1921–1926 cohort due to significant attrition by the periods of interest). We took all three waves of data from TTM and the three waves for each cohort in ALSWH that were conducted at the closest time points to these. This gave us a study timeframe that, at the earliest, began in 2012 (ALSWH 1973–1978 cohort) and, at the latest, ended in 2020/21 (TTM).
For each cohort, we conducted two separate analyses to examine outcomes across pairs of survey waves (Figure 1). The first wave in any pair constituted the baseline wave (T0), and the second the follow-up wave (T1). For example, for the ALSWH 1946–1951 cohort, the first pair (Analysis 1) comprised Wave 7 (T0) and Wave 8 (T1) and the second pair (Analysis 2) comprised Wave 8 (T0) and Wave 9 (T1).
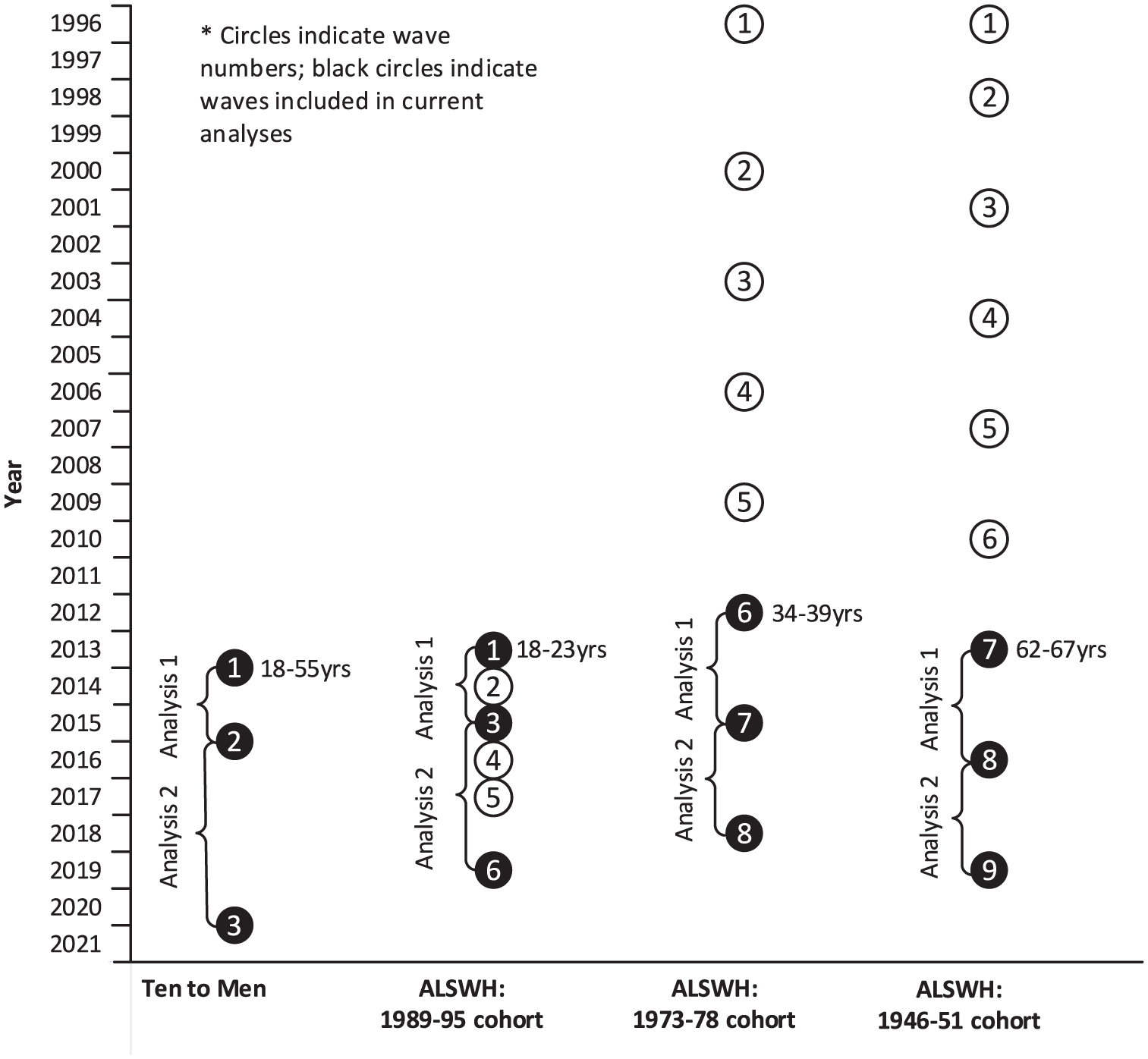
Waves included in each analysis for each cohort.
To be included in the analysis, participants had to satisfy the following criteria:
(1) aged ⩾ 18 at T0 (for TTM, they also had to have completed the survey for adult participants because some 18-year-olds completed one for younger participants);
(2) demonstrated ‘mental health need’ at T0 (see below);
(3) agreed to Medicare linkage for the T0–T1 period; and
(4) completed relevant survey waves.
Measures
Mental health need
Participants in each TTM and ALSWH wave completed standardised self-report mental health measures. In TTM, these were the Patient Health Questionnaire-9 (PHQ-9) (Kroenke et al., 2001) and PHQ-2 (Kroenke et al., 2003). In ALSWH, they were the Centre for Epidemiological Studies – Depression scale (CES-D-10) (Carpenter et al., 1998), Generalised Anxiety Disorder scale (GAD-7) (Spitzer et al., 2006) and Kessler 10 (K-10) (Kessler et al., 2002). These were used to assess ‘mental health need’ (Criterion 2, above). To be included in an analysis, TTM participants had to score ⩾ 2 on the PHQ-2, ALSWH 1973–1978 and 1946–1951 cohort participants had to score ⩾ 10 on the CES-D-10 or ⩾ 6 on the GAD-7, and ALSWH 1989–1995 cohort participants had to score ⩾ 16 on the K-10.
We classified those with ‘mental health need’ by prognostic severity using a similar approach to another study in the evaluation (Harris et al., 2026). We adapted algorithms developed for the Target-D and Link-me clinical trials to classify participants’ likely severity of depression (Target-D) or depression or anxiety (Link-me) in three months’ time: ‘minimal/mild’, ‘moderate’ or ‘severe’ (Chondros et al., 2018; Fletcher et al., 2021a, 2021b). These algorithms were based on baseline psychosocial factors (e.g. gender, mental health history, current symptoms, general health, living situation, financial security). TTM and ALSWH captured this information from participants at the various T0 points, and we conducted mapping exercises to ensure that the algorithms were based on information that was as similar as possible across studies. We used the Target-D algorithm for TTM and the Link-me algorithm for ALSWH because baseline anxiety information was unavailable in TTM.
Change in mental health
We assessed change in mental health from T0 to T1. For TTM participants, this was assessed with the PHQ-9. For ALSWH participants from the 1973–1978 and 1946–1951 cohorts, the CES-D-10 and GAD-7 were used to assess change; for ALSWH participants from 1989–1995 cohort, the K-10 was used. We used an effect size of 0.3 (small to medium (Cohen, 1988)) of a standard deviation of the baseline score of all participants who had used Better Access treatment services to calculate an absolute threshold for change score on each measure, and then used this to classify change as ‘significant improvement’, ‘no significant change’ or ‘significant deterioration’. We chose 0.3 as the effect size for this and other relevant studies in the evaluation (Harris et al., 2026; Pirkis et al., 2022a, 2026a, 2026b) because this was consistent with studies of the Minimum Clinically Important Difference (MCID) on the PHQ-9 and GAD-7 in comparable populations (Kounali et al., 2020; Kroenke et al., 2019) and other advice on effect sizes likely to reflect minimally important clinical or subjective benefit (Angst et al., 2017).
Use of Better Access treatment services
We used participants’ Medicare data to classify them into treatment groups, based on their use (or non-use) of Better Access treatment items in any T0–T1 period. Better Access treatment items were defined as all MBS items associated with psychological therapy services delivered by clinical psychologists and all MBS items associated with focussed psychological strategies delivered by psychologists, social workers, OTs and GPs/PMPs (Supplemental material).
For those who had used Better Access treatment services, we used information on the number of sessions, type of Better Access provider seen (clinical psychologist, psychologist, social worker, OT, GP/PMP) and out-of-pocket costs. Costs were converted to June 2022 dollars using Consumer Price Index (CPI) figures for Medical and Hospital Services from the Australian Bureau of Statistics (2022).
Other sociodemographic, clinical and treatment variables
We used the following additional sociodemographic, clinical, and treatment variables in our analyses: age (in years); First Nations (yes, no); highest education level (year 11 or less, year 12 or equivalent, certificate/diploma, bachelor’s degree or higher); country of birth (Australia, other); area of residence (metropolitan, regional, rural); lifetime history of depression (yes, no); lifetime history of anxiety (yes, no) and currently taking any medication for mental health (yes, no).
Analyses
We analysed data separately for each cohort and T0–T1 period. We identified participants who had and had not used Better Access treatment services and described them in terms of sociodemographic, clinical, and treatment characteristics using summary statistics (means and percentages). We conducted a multivariable logistic regression analysis to examine whether these characteristics were associated with Better Access use.
We described patterns of Better Access use for those who had used treatment services using summary statistics (medians and percentages). We conducted further multivariable logistic regression analyses to explore associations between individuals’ baseline characteristics and their treatment patterns and significant improvement (vs no significant change or significant deterioration) on each measure.
We conducted sensitivity analyses alongside each regression analysis, exploring coefficient correlation matrices and goodness-of-fit scores after fitting different models. We ultimately chose models that appeared stable and not impacted by multicollinearity.
All analyses were conducted using Stata version 17 (StataCorp, 2021). The ALSWH analyses were conducted within the Secured Unified Research Environment (SURE), administered by the Sax Institute. We suppressed numbers ⩽ 10 in all outputs.
Approvals
Both TTM and ALSWH received initial ethics approvals from the responsible organisations’ ethics committees. All participants provided informed consent. For both TTM and ALSWH it is not necessary to obtain separate ethical approval for data use as the existing Australian Institute of Family Studies and ALSWH Data Access Committee approvals provide coverage. The TTM and ALSWH analyses for this study were granted an exemption from Human Research Ethics Review under the National Statement on Ethical Conduct in Human Research and relevant University of Queensland policy (PPL 4.20.07).
Results
Figure 2 shows the number of participants who met inclusion criteria for each analysis. The highest number of participants in any analysis was 6979 (ALSWH 1989–1995 cohort, Analysis 1) and the lowest was 1550 (TTM, Analysis 2). In general, around one-third of participants demonstrated ‘mental health need’ at baseline (the exception was the ALSWH 1989–1995 cohort, three-quarters of whom did so). Typically, half to three-quarters of those who demonstrated ‘mental health need’ agreed to Medicare linkage and completed relevant surveys.
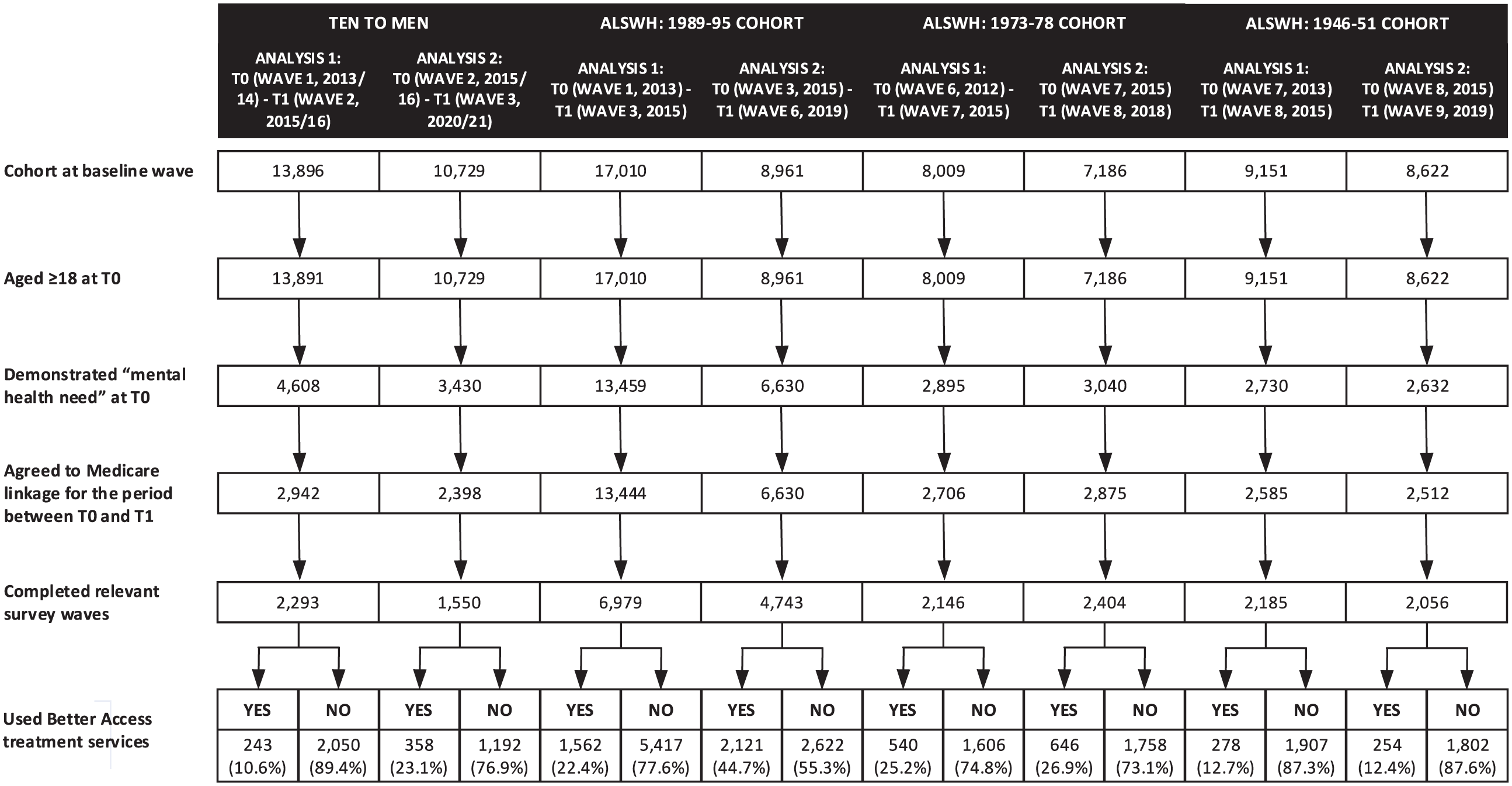
Participants selection and use of Better Access treatment services by study, cohort.
Figure 2 shows the proportion of participants in each analysis who used and did not use Better Access treatment services between the relevant survey waves. Proportions varied across study cohorts and analyses, with the lowest proportion being 10.6% in (TTM, Analysis 1), and the highest being 44.7% (ALSWH 1989–1995 cohort, Analysis 2). For these cohorts, the proportions of participants using Better Access increased over time, doubling from Analysis 1 to Analysis 2. For the other two cohorts, the proportions remained the same at around one-quarter (ALSWH 1973–1978 cohort) and one-tenth (ALSWH 1946–1951 cohort).
Characteristics of participants who used Better Access treatment services
Table 1 profiles the participants who used Better Access treatment services. Although there were some between-cohort differences, Better Access users tended to be relatively well educated, born in Australia, and living in cities. Their prognostic severity levels varied, but often relatively high proportions could be classified as ‘severe’. High proportions had lifetime histories of depression. Smaller, but often still substantial, proportions had lifetime histories of anxiety. A minority (usually well under half) were taking medication for their mental health.
Characteristics of participants who did and did not use Better Access treatment services, by study, cohort and analysis. a
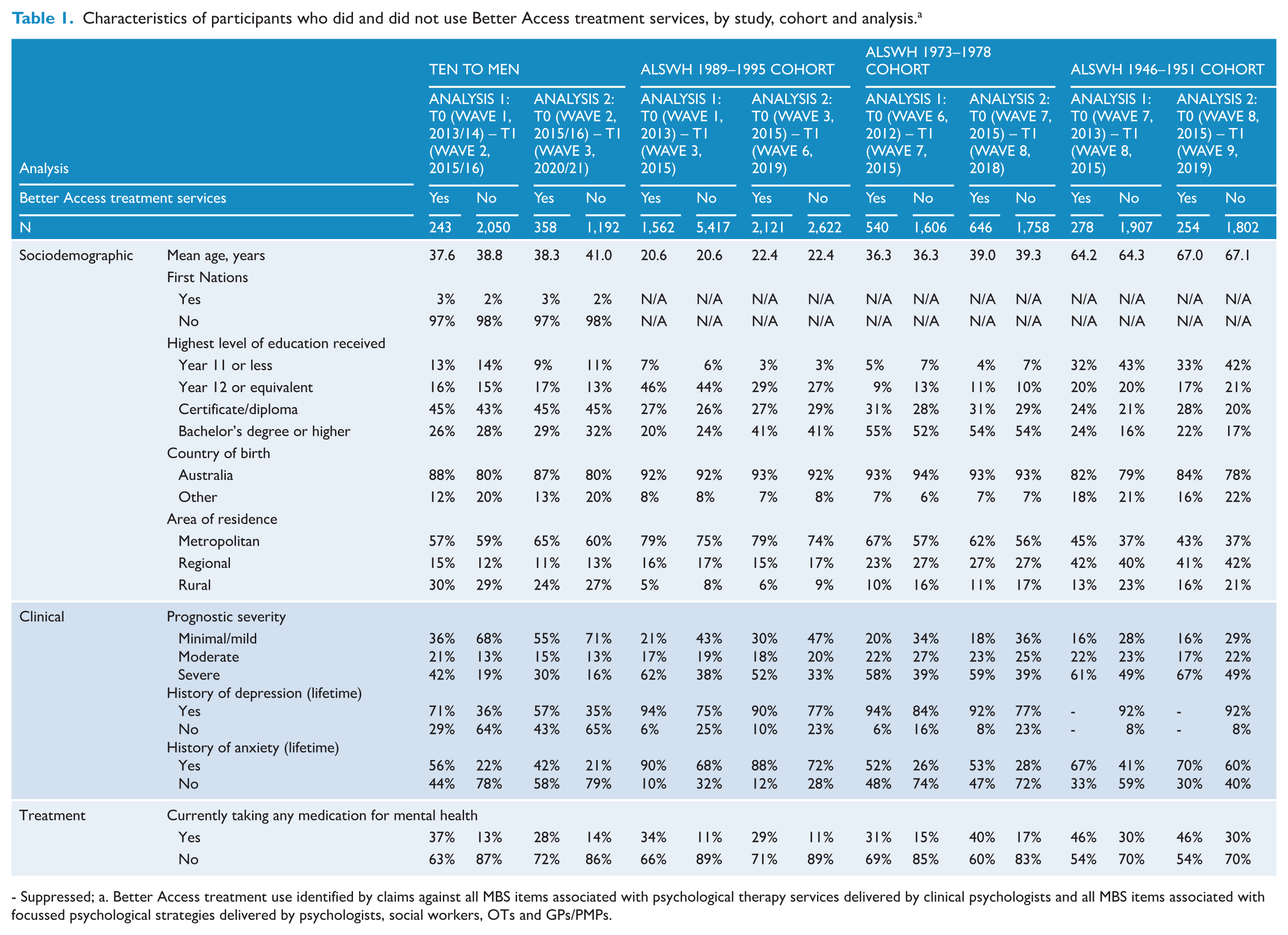
- Suppressed; a. Better Access treatment use identified by claims against all MBS items associated with psychological therapy services delivered by clinical psychologists and all MBS items associated with focussed psychological strategies delivered by psychologists, social workers, OTs and GPs/PMPs.
The multivariable logistic regression compares the users of Better Access treatment services with non-users of these services (Table 2). Several clinical factors were consistently associated with higher odds of using Better Access (statistical evidence of an association in most analyses across most cohorts): worse prognostic severity, lifetime history of depression or anxiety, and current use of mental health medication. Living in a rural area was consistently associated with lower odds of using Better Access. Some other factors – notably age and education level – were associated with differential odds of using Better Access (statistical evidence of an association in some analyses with some cohorts, but not others). Older age was associated with lower odds of using Better Access in one analysis for TTM, the ALSWH 1973–1978 cohort, and the ALSWH 1946–1951 cohort, but not in either analysis for the ALSWH 1989–1995 cohort (noting that age ranges differed across cohorts). Higher education levels were consistently associated with greater odds of using Better Access for most analyses with the three ALSWH cohorts, but there was no effect of education for the TTM cohort.
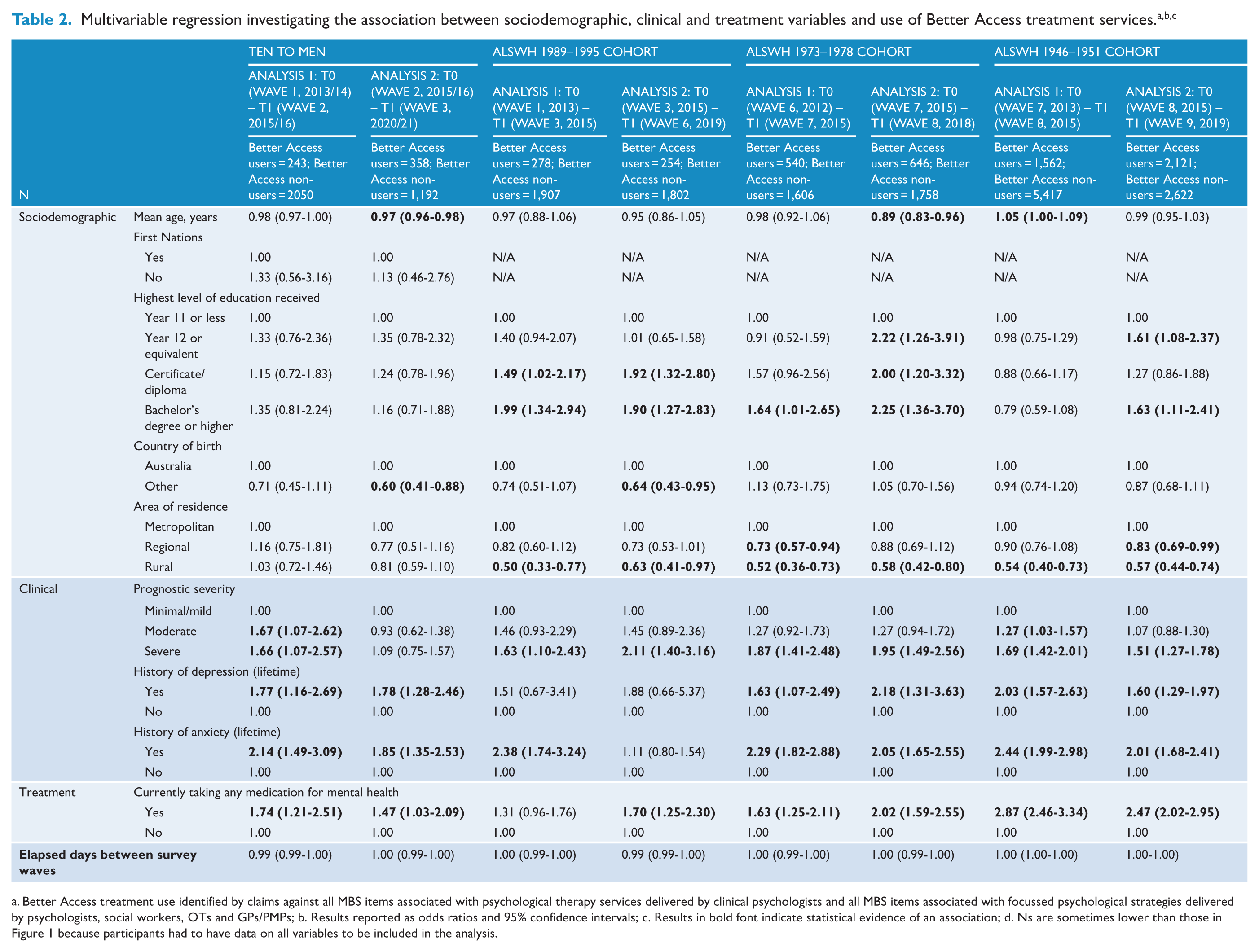
a. Better Access treatment use identified by claims against all MBS items associated with psychological therapy services delivered by clinical psychologists and all MBS items associated with focussed psychological strategies delivered by psychologists, social workers, OTs and GPs/PMPs; b. Results reported as odds ratios and 95% confidence intervals; c. Results in bold font indicate statistical evidence of an association; d. Ns are sometimes lower than those in Figure 1 because participants had to have data on all variables to be included in the analysis.
Patterns of use of Better Access treatment services
We explored the patterns of use of Better Access treatment services for those who used them (Tables 3 and 4). These findings should be considered in the context of the ‘window of opportunity’ that participants had to do this. The periods between T0 and T1 varied by cohort and analysis; the shortest was 1.87 years (TTM, Analysis 1) and the longest was 4.65 years (TTM, Analysis 2).
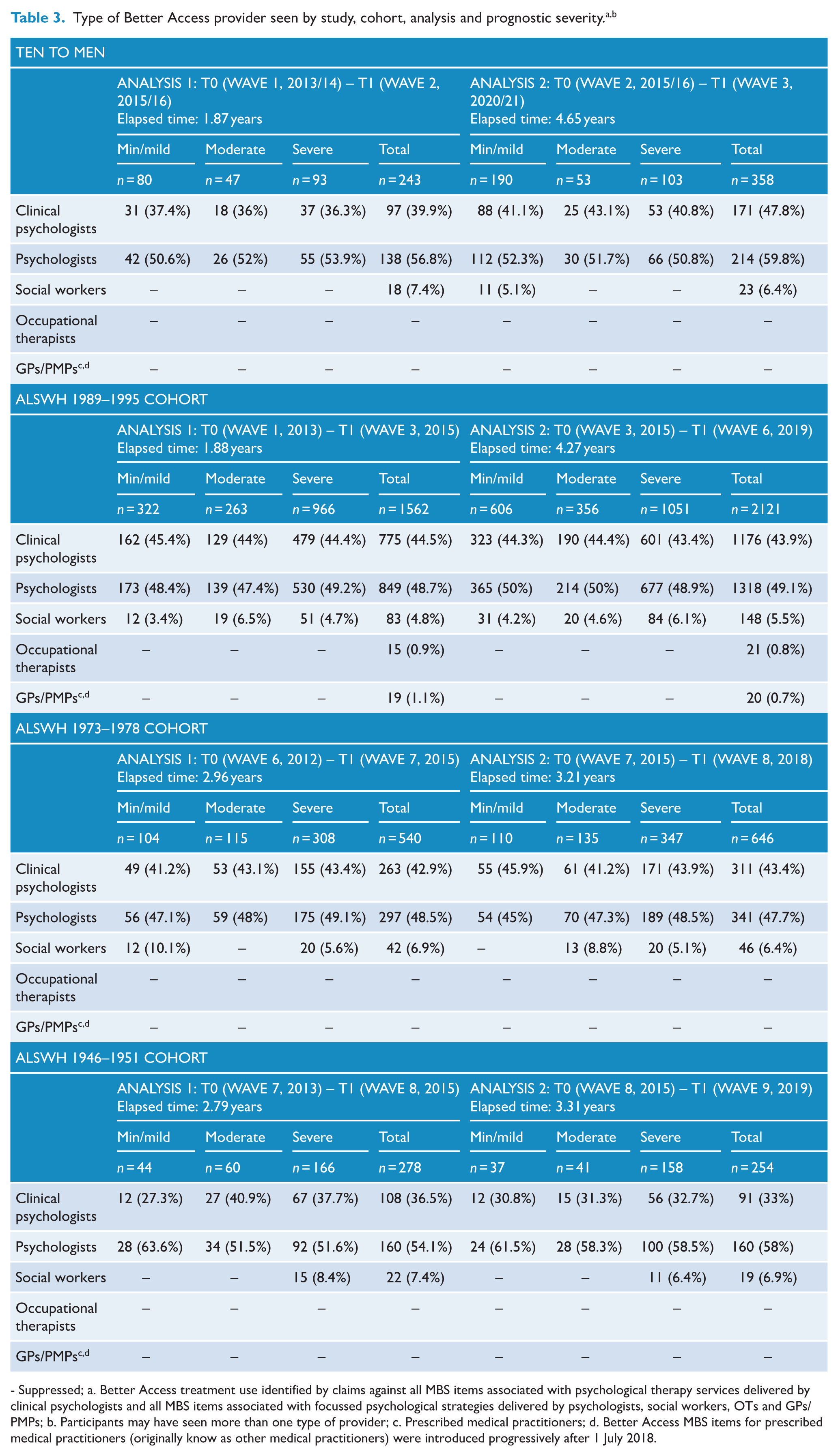
- Suppressed; a. Better Access treatment use identified by claims against all MBS items associated with psychological therapy services delivered by clinical psychologists and all MBS items associated with focussed psychological strategies delivered by psychologists, social workers, OTs and GPs/PMPs; b. Participants may have seen more than one type of provider; c. Prescribed medical practitioners; d. Better Access MBS items for prescribed medical practitioners (originally know as other medical practitioners) were introduced progressively after 1 July 2018.
Number of Better Access treatment sessions and out-of-pocket costs by study, cohort, analysis and prognostic severity. a
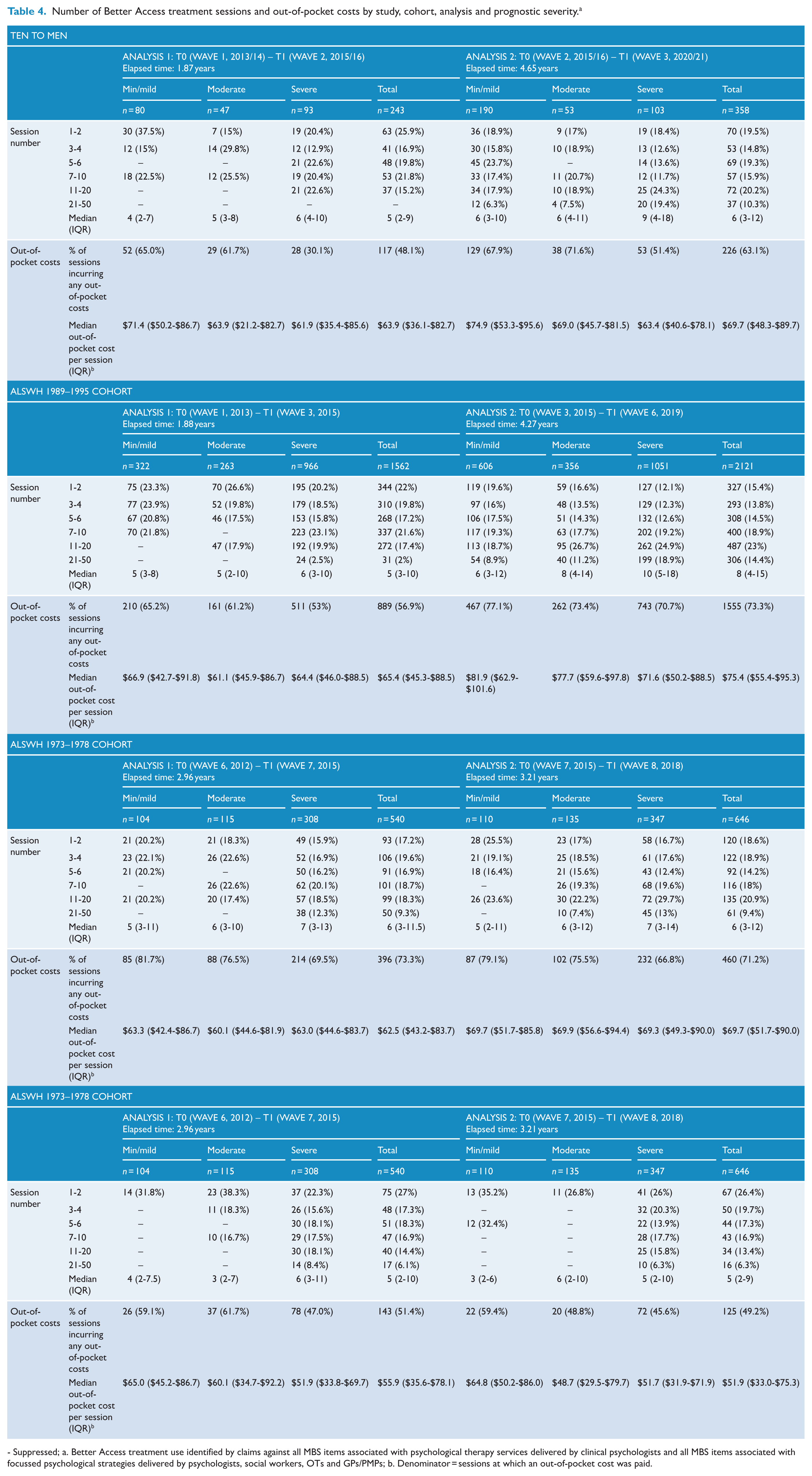
- Suppressed; a. Better Access treatment use identified by claims against all MBS items associated with psychological therapy services delivered by clinical psychologists and all MBS items associated with focussed psychological strategies delivered by psychologists, social workers, OTs and GPs/PMPs; b. Denominator = sessions at which an out-of-pocket cost was paid.
Type of Better Access provider seen
Table 3 shows the types of Better Access providers who delivered participants’ treatment (noting that participants may have seen more than one type of provider). In general, around 40% of participants received treatment from a clinical psychologist and around 50% did so from a psychologist. Smaller proportions (typically less than 10%) received treatment from a social worker. Smaller proportions still received treatment from OTs and GPs/PMPs, as evidenced by the number of cells with suppressed data. In the main, participants’ provider-based service use patterns did not differ by their prognostic severity.
Number of sessions of Better Access treatment and out-of-pocket costs
Table 4 summarises the number of sessions received by those who used Better Access treatment services in each T0–T1 period. Across cohorts and analyses, participants typically accessed a median of 5–6 sessions. There was a dose-response effect, whereby the median number of sessions increased as a function of prognostic severity. This was also apparent when the number of sessions was categorised; relatively higher proportions of those in the ‘minimal/mild’ group tended to have 1–2 sessions, and, conversely, relatively higher proportions of those in the ‘severe’ group had 7–10 sessions or more.
Table 4 also shows the out-of-pocket costs for participants who received Better Access treatment services. Across the board, between half and three-quarters paid at least some out-of-pocket costs (usually $80–$100/session). For the TTM cohort and the ALSWH 1989–1995 cohort, the proportion increased over time, with more paying out-of-pocket costs in Analysis 2 than in Analysis 1. This pattern did not hold for the ALSWH 1973–1978 and 1946–1951 cohorts, however; their proportions remained more consistent across analyses. There was some evidence of a relationship between out-of-pocket costs and prognostic severity. In general, participants in the ‘minimal/mild’ group were more likely to pay out-of-pocket costs than those in the ‘severe’ group.
Changes in mental health for users of Better Access treatment services
Figure 3 shows the T0–T1 change in mental health for participants who used Better Access treatment services. Typically, 45%–55% of these participants had better mental health at T1 than at T0.
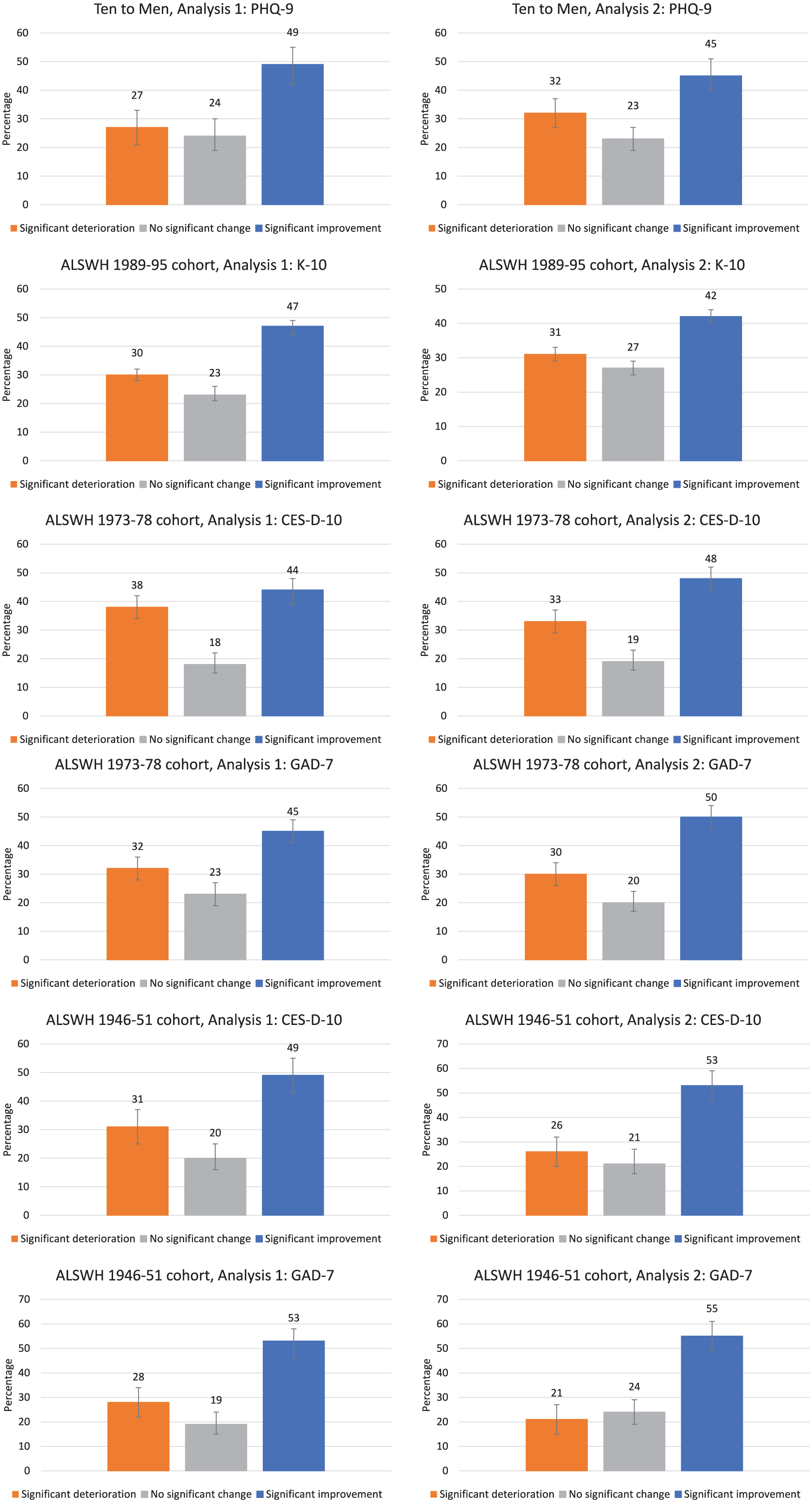
Changes in mental health over time, by study, cohort, analysis and measure (cont.).
The multivariable logistic regression analyses highlight key predictors of improvement (Table 5). The most consistent predictor was prognostic severity at T0; across most cohorts and analyses, and irrespective of the measure chosen to assess change in mental health, those in the ‘severe’ group at baseline were the most likely to demonstrate significant improvement.
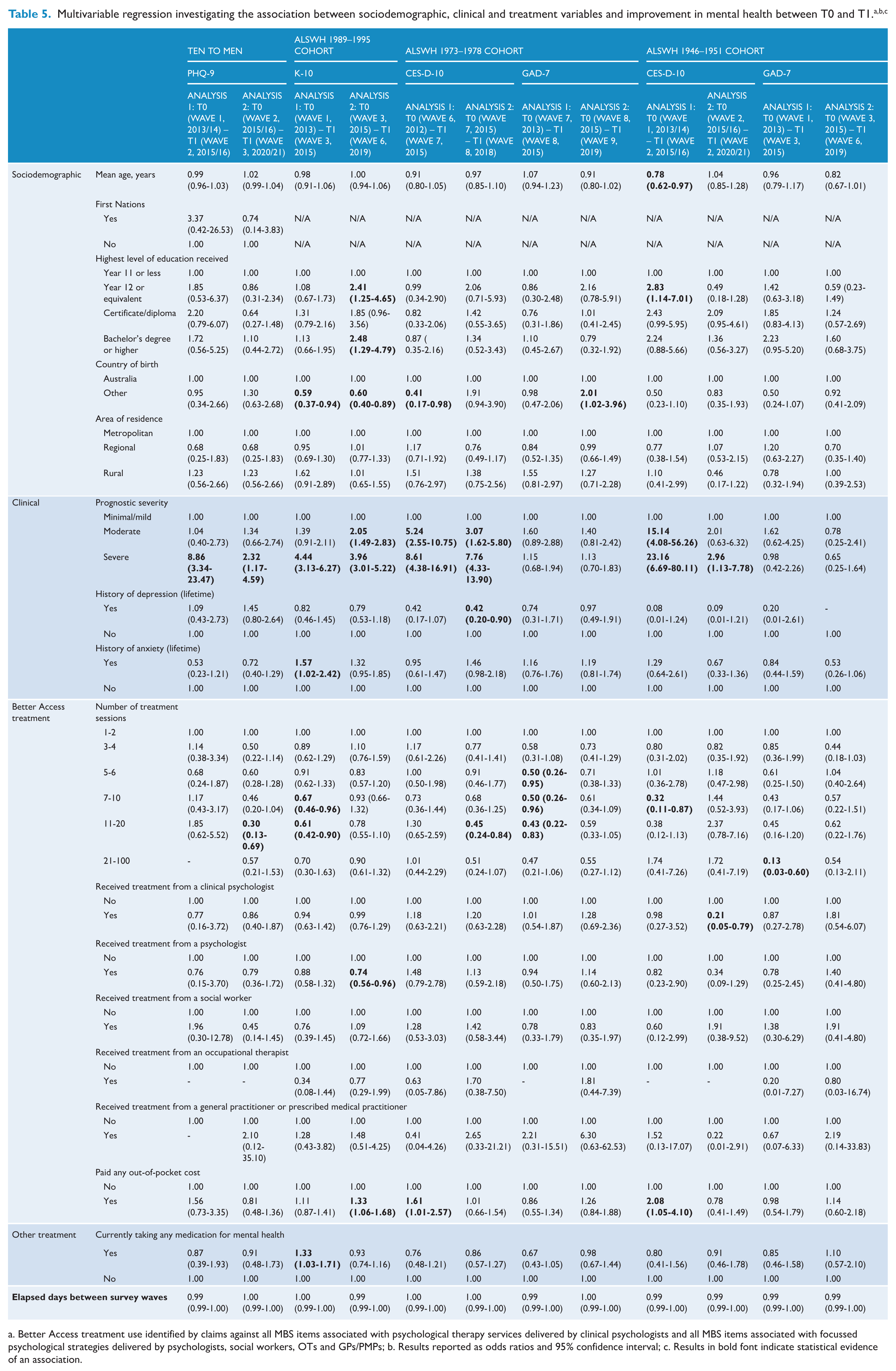
a. Better Access treatment use identified by claims against all MBS items associated with psychological therapy services delivered by clinical psychologists and all MBS items associated with focussed psychological strategies delivered by psychologists, social workers, OTs and GPs/PMPs; b. Results reported as odds ratios and 95% confidence interval; c. Results in bold font indicate statistical evidence of an association.
The number of sessions was also related to improvement in some analyses for some cohorts, but not in the direction that might have been expected based on other studies in our evaluation (Harris et al., 2026; Pirkis et al., 2026a, 2026b). In the current study, compared with participants who had 1-2 sessions, those who had more sessions had lower odds of showing improvement within one follow-up wave.
Other variables were either not associated with improvement in any analyses or associated with improvement in a small number of analyses only.
Discussion
This study examined use of Better Access treatment services by TTM and ALSWH participants identified as having mental health need. In the more recent analysis period for each cohort, the proportion of those with mental health need who used Better Access ranged from around 13% in the ALSWH 1946–1951 cohort to around 45% in the ALSWH 1989–1995 cohort, with the proportion in the other cohorts around 25%. These findings can be compared with the National Study of Mental Health and Wellbeing which suggests that in 2020–2022 around one-quarter of Australians with a mental disorder saw a psychologist (Australian Bureau of Statistics, 2023). There are suggestions that the proportions accessing care increased over time in the TTM cohort and the ALSWH 1989–1995 cohort, but the fact that the Analysis 2 period was typically longer than the Analysis 1 period may have influenced this. In the case of the TTM cohort, Analysis 2 included the pandemic period which may be atypical.
When we compared those who had used Better Access treatment services with those who had not, certain characteristics stood out. These largely related to clinical need, which would appear to be appropriate. Better Access users were more likely to be classified in the ‘severe’ prognostic severity group, have a history of depression or anxiety, and be taking mental health medication. However, those in rural areas were less likely to use Better Access treatment services. This issue has been identified in previous studies of Better Access use that have used ALSWH data (Dolja-Gore et al., 2014), and is likely to relate to provider availability in rural areas.
Those who used Better Access treatment services typically accessed 5–6 sessions, usually from clinical psychologists and/or psychologists. This finding is consistent with a previous analysis of data from the ALSWH 1973–1978 cohort (Dolja-Gore et al., 2022). Again, these results should be considered in the context of the analysis periods which ranged from 1.87 to 4.65 years. Given this, it might have been anticipated that median numbers of sessions would have been higher, although we know from elsewhere that relatively few people make intensive use of Better Access on a continuous basis (Dolja-Gore et al., 2022). For most of the time covered by the study, participants would have been eligible for 10 sessions of Better Access treatment per year. Half to three-quarters of participants paid at least some out-of-pocket costs (usually $80-$100/session). Prognostic severity was associated with these service use patterns: those in the ‘severe’ group tended to use more sessions, and those in the ‘minimal/mild’ group were generally more likely to pay out-of-pocket costs. This suggests that those with the greatest levels of need were not only more likely to access Better Access, but also likely to access more sessions and to pay less for them. Again, this would seem to be appropriate. However, an alternative explanation is that those in the ‘minimal/mild’ group may hesitate to seek treatment because of high out-of-pocket costs (potentially seeking other services initially), and that their symptoms may worsen before they use Better Access. It should also be noted that the level of co-payment may still act as a barrier to people with limited financial resources, regardless of their mental health needs. Other studies have shown that there are economic barriers to accessing Better Access services (Dolja-Gore et al., 2023), including several in our evaluation (Currier et al., 2026; Newton et al., 2026; Pirkis et al., 2026a; Tapp et al., 2026a). Equity of access to mental health care is paramount.
Many participants who used Better Access treatment services experienced improvements in their mental health. Typically, around 45–55% had better mental health at the end of any analysis period than at the beginning. Caution must be exercised in attributing improvement (or indeed lack of change or deterioration) to their Better Access use, particularly given the length of the analysis periods; we were not able to conduct pre-/post-analyses of discrete episodes of care, and we do not know the treatment stage participants were at or what else happened between survey waves. Nonetheless, this degree of improvement is reasonably consistent with the findings from other studies in our evaluation, which used similar standardised mental health measures to assess change over time (Harris et al., 2026; Pirkis et al., 2026a).
The key predictor of improvement was prognostic severity; those in the ‘severe’ prognostic severity group at baseline were the most likely to show improvement. This makes sense; those with higher levels of symptomatology and poorer levels of functioning have a greater opportunity for improvement. Again, this is consistent with other studies in our evaluation (Harris et al., 2026; Pirkis et al., 2026a; 2026b).
More surprisingly, however, in some analyses, greater numbers of sessions were associated with a lower likelihood of improvement. This may relate to the long periods between waves, and the fact that participants’ levels of symptoms and functioning and consequent needs for treatment may have varied over time. Some participants may have had a single treatment episode, whereas others may have had multiple episodes. In this context, the number of sessions may have acted more like a proxy for greater fluctuations in mental health, more intractable difficulties and unresolved treatment needs than as an indicator of treatment ‘dose’. The findings may also have been influenced by uncontrolled confounders like difficult life circumstances. In addition, some people – particularly those with high baseline severity levels – may need more comprehensive care than Better Access is able to provide in isolation, and we could not determine whether they received this (see below). An alternative explanation is that reverse causality may be operating, and those who make substantial improvements quite quickly may require fewer sessions. The fact that the finding was not consistent across all analyses in all cohorts and is at odds with the other studies in our evaluation (Harris et al., 2026; Pirkis et al., 2026a, 2026b) suggests that further investigation is warranted.
Strengths and limitations
We used two large longitudinal studies involving representative samples of Australian men and women from across the age spectrum; previous studies have considered women only (Byles et al., 2011) or men and women aged ⩾ 45 only (Dolja-Gore et al., 2018). TTM and ALSWH were designed for purposes other than evaluating Better Access, reducing biases associated with recruiting participants for mental health studies. Linkage between survey data and MBS records allowed us to reliably determine whether participants had used Better Access treatment services and, if so, how much and what they paid.
Limitations include that the variables that were used in the original Target-D and Link-me algorithms were not always available, so we used proxies to determine prognostic severity. Due to variable availability, we used the Target-D algorithm for TTM and the Link-me algorithm for ALSWH, which may explain why higher proportions of women than men were in the ‘severe’ prognostic severity group. Those who were lost-to-follow-up in TTM and ALSWH may have differed from those who were retained (Loxton et al., 2019). The mental health measures were completed at survey waves, not at the beginning and end of Better Access episodes; the between-wave duration was often lengthy, and multiple factors may have influenced participants’ mental health. We could not determine what non-Better Access mental health services participants accessed. Most of the study periods did not extend beyond 2019, limiting our ability to examine recent Better Access use.
Conclusions
This study provides valuable insights into who uses Better Access and how they use it. It suggests that Australian adults with mental health need make varying use of Better Access treatment services, but the programme appears to serve those with high levels of need relatively well.
Supplemental Material
sj-docx-1-anp-10.1177_00048674251409017 – Supplemental material for Examining Better Access use by Australian adults using data from two longitudinal studies (Ten to Men and the Australian Longitudinal Study on Women’s Health)
Supplemental material, sj-docx-1-anp-10.1177_00048674251409017 for Examining Better Access use by Australian adults using data from two longitudinal studies (Ten to Men and the Australian Longitudinal Study on Women’s Health) by Vikas Arya, Caley Tapp, Dianne Currier, Philip Burgess, Julie Byles, Xenia Dolja-Gore, Meredith Harris, Long Khanh-Dao Le, Cathrine Mihalopoulos, Katrina Scurrah, Matthew J Spittal and Jane Pirkis in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
This study was funded by the Australian Government Department of Health, Disability and Ageing, as part of the broader evaluation of Better Access. We would like to thank the two groups that were constituted to advise on the evaluation, the Clinical Advisory Group and the Stakeholder Engagement Group.
The research on which this study is based was conducted as part of TTM by the University of Melbourne and the Australian Institute of Family Studies and as part of the ALSWH by the University of Queensland and the University of Newcastle. We are grateful to the Department of Health, Disability and Ageing for funding these longitudinal studies. We also acknowledge the boys and men who provided the survey data for TTM and the women who provided the survey data for ALSWH. We also acknowledge the Department of Health, Disability and Ageing for providing MBS and PBS data, and, for the ALSWH, the Australian Institute of Health and Welfare as the Integrating Authority.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclose receipt the following financial support for the research, authorship, and/or publication of this article: The evaluation of Better Access was funded by the Australian Government Department of Health, Disability and Ageing.
ORCID iDs
Data accessibility statement
The TTM and ALSWH datasets used in this analysis are available from the respective custodians. The specific analytic datasets derived for the current study are not available.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.