
Abstract
Keywords
Introduction
In the first Australian National Survey of Mental Health and Wellbeing (Andrews and Carter, 2001), 13.6% of the population met criteria for anxiety or depression; each associated with significant disability. More than 50% who met criteria for anxiety or depression received no treatment (Andrews and Carter, 2001). Since 2001, the Australian Federal Government has funded access to mental health services via Better Outcomes in Mental Health Care, a five-component program detailed elsewhere (Hickie and Groom, 2002; Pirkis et al., 2004). The Access to Allied Psychological Services (ATAPS) component (2003) enabled eligible patients to access Medicare rebates for psychological services from allied health professionals (McGarry et al., 2009; Pirkis et al., 2010)
ATAPS guidelines mandated services to be short term (6–12 sessions), low cost and aimed at mild to moderate, high prevalence mental illnesses, particularly anxiety and depression, as defined by the International Classification of Diseases (ICD-10) (Australian Government Department of Health and Aging, 2010). To refer to ATAPS, GPs conduct a Mental Health Treatment Plan, which includes a clinical diagnosis and another measure, most commonly the Kessler 10 (K-10) (Kessler et al., 2002) or the Depression, Anxiety and Stress Scale (DASS-21) (Lovibond and Lovibond, 1995), which are used in the assessment of national program effectiveness (Pirkis et al., 2010). GPs have keenly adopted the initiative, which has increased access to mental health services and evidence-based treatments (Hickie et al., 2004); 110 of 111 Divisions of General Practice generated 150,945 referrals for 113,107 patients in 2005–2010 (Pirkis et al., 2010).
National ATAPS evaluations showed 70% of patients met criteria for anxiety or depression (Pirkis et al., 2010) and K-10 or DASS-21 scores demonstrated improvements after treatment (Pirkis et al., 2010, 2011). Despite the frequency of anxiety and depression in the ATAPS population, anxiety and depression often go undetected in primary care, which may prevent eligible patients accessing ATAPS (Hickie et al., 2001a).
This study was designed to determine to what extent GP referrals of patients resulted in patient characteristics conforming to the ATAPS referral guidelines, and to explore what other variables mediated GPs’ selection of patients for referral to ATAPS.
Methods
Aims
Primary: Determine the likelihood of ATAPS cases meeting ICD-10 criteria for any mood or any anxiety disorder compared to GP controls.
Secondary: Determine the likelihood of ATAPS cases having higher psychological distress scores (K-10) and psychological symptom scores (DASS-21) compared to GP controls.
Develop a multivariable explanatory model of patient characteristics distinguishing ATAPS cases from GP controls.
Setting
GP Access is the trading name of the Hunter Urban Division of General Practice, which supports 450 GPs in 145 general practices (population 447,254). GP Access Psychology Service delivered the ATAPS program, employing 20 psychologists, clinical psychologists in training or clinical psychologists. From July 2005 to December 2010, approximately 6929 patients used 24,045 ATAPS sessions (GP Access, 2010).
Study design and participants
A case-control design was used. Cases and controls were aged 18–65 years and drawn from the underlying population of patients attending a GP in the Hunter Division.
Cases were drawn from patients who were referred by their GP and subsequently attended GP Access Psychology Service for ATAPS January 2009 to March 2010. Cases came from North/Westlakes (n = 7), Eastlakes (n = 6), Newcastle (n = 16), Newcastle West (n = 29) and Maitland networks (n = 5). Cases were ‘incident’ (first referral to ATAPS). There was no random selection of cases. Hunter New England Human Research Ethics Committee (HNEHREC) required the initial approach to be made by GP Access reception staff on the patient’s second or subsequent attendance. We have no data on number of eligible patients, invitations by reception staff or subsequent acceptance of contact with the researcher. We have no data on referrals to ATAPS who never attended at all or who only attended for a single appointment.
Controls were drawn from patients who attended their GP for any reason in the period January to February 2010 and had never been referred to any GP Access ATAPS program. There was no random selection of controls. Controls were recruited from participating GPs, who had responded to a written invitation; 20 GPs in five practices, from four of the five GP Access networks. Two practices were located in the North/Westlakes (n = 25) and one each in Eastlakes (n = 15), Newcastle (n = 12) and Newcastle West (n = 12) networks. A maximum of four patients for each GP were recruited from any one GP practice and recruitment in each network was spread across multiple days of the week. Consecutive patients were initially approached by GP reception staff and invited to speak with the research psychologist. We have no data on number of eligible patients, approaches by reception staff or acceptance of contact with the researcher.
Sample size
We estimated 30% of controls would have an ICD-10 diagnosis (mood or anxiety disorder). To detect the least extreme odds ratio of 2.8 for cases, power 0.8 and alpha ≤ 0.05 required 64 cases and 64 controls.
Instruments
Demographics (age, gender, relationship, education, employment, household income), GP network, and GP treatment (mental health visit past month, current antidepressant treatment).
List of threatening experiences (LTE) (Brugha et al., 1985): 12 experiences (past 6 months), scored by summation for a score 0–12. Question 1 (LTE Q1) asked has there been a ‘serious accident, illness or injury’, used as a binary variable for current physical illness.
12-item short-form health survey version 2 (SF-12) (Ware et al., 1996): 12 items measuring physical disability (SF-12 PCS) and mental disability (SF-12 MCS), scored as a continuous variable using the brief rounded integer scorer (Andrews, 2002), yielding mean scores of 50 (SD 10), with higher scores indicating lower disability.
Alcohol, Smoking and Substance Involvement Screening Test V3.0 (Humeniuk and Ali, 2006): 8-item screener for problem use of alcohol and other drugs in primary care. Total number used (past 3 months) as continuous variable.
Depression, Anxiety and Stress Scale 21-item version (DASS-21) (Henry and Crawford, 2005): three subscales of seven items rating mental health symptoms (depression, anxiety and stress), summation for continuous ‘composite negative affect score’ 0–62 (Sheehan et al., 1998).
Kessler 10 (K-10) (Kessler et al., 2002): 10-item measure of distress associated with mental illness, scored 10–50, higher scores indicating greater distress.
The Mini International Neuropsychiatric Interview (MINI) (Sheehan et al., 1998): standardised diagnostic interview for ICD-10 mental disorders. Any anxiety disorder included agoraphobia, panic disorder, social phobias, obsessive-compulsive disorder, post-traumatic stress disorder and generalised anxiety disorder. Any mood disorder included depressive episode, manic or hypomanic episode, dysthymia and cyclothymia.
Analyses
The dependent variable for all comparative analyses was ATAPS case versus GP control.
Descriptive statistics used for socio-demographic, clinical and GP treatment characteristics of participants. Comparisons used two-tailed t-tests, chi square test and Fisher’s exact test.
Four unadjusted logistic regression analyses were used to test the two categorical (any mood or any anxiety disorder (Table 2) and two continuous variables (K-10 and DASS-21) (Table 3), expressed as odds ratio (OR) and 95% confidence intervals (CIs), for the association with ATAPS caseness. Initial unadjusted models were adjusted for several potential confounders (and effect modifiers) to examine the change in magnitude on the effect for each of the four main predictor variables. Standard errors and interaction terms were used to test for multi-collinearity.
Specifically, regression models for any mood or any anxiety disorder as main predictors were adjusted in separate analyses for: demographics, number of threatening experiences, physical illness and physical disability, mental disability, psychological distress, GP treatment (mental health visit in past month, current antidepressant treatment), and comorbidity of mental illness including: any mood disorder, substance misuse and substance misuse or any mood disorder (for any anxiety disorder), and any anxiety disorder and substance misuse or any anxiety disorder (for any mood disorder). Results were expressed as ORs with 95% CIs in predicting case versus control with the referent group being no mood and no anxiety disorders, respectively (Table 2).
Similarly, regression models for K-10 and DASS-21 as main predictors were adjusted for: demographics, number of threatening experiences, physical illness and disability, comorbidity of mental illness and GP mental health treatment (mental health visit in the last month, current antidepressant treatment, substance misuse, any anxiety disorder), any mood disorder and mental disability. Results were expressed as ORs with 95% CIs for each rise of one point on K-10 or DASS-21 in predicting case versus control (Table 3).
To develop an explanatory multivariable model a forward stepwise logistic regression analysis used the predictor variables: relationship status, household income, any mood disorder, any anxiety disorder (categorical), age, number of threatening experiences, mental disability, physical disability and total number of substances misused (continuous). Variables with significant multi-collinearity were excluded (e.g. DASS-21, K10) and no interaction terms were included in any models. Variables were retained in the model with p < 0.05 and removed if p > 0.10. The Hosmer-Lemeshow test examined ‘goodness of fit’ for all logistic regression models. Model summary statistics are reported for the final iteration: –2 log likelihood and Nagelkerke R2 statistic.
The multivariable logistic regression model yielded three continuous predictors. Because the sample size was relatively small and non-linear distributions of continuous variables may produce a number of ‘cells’ with zero or low counts, a post hoc confirmatory forward stepwise regression model was tested. This model included income level, any mood disorder, any anxiety disorder, and continuous predictor variables were transformed into quartiles based on distributions of scores (mental disability, physical disability) or a three-level categorical variable, none, one, two or more (number of threatening experiences and substances misused), with the model limited to seven predictor variables to avoid over-fitting.
In order to explore the relatively high proportion of GP controls having any anxiety disorder, a post hoc analysis was conducted, reporting number and percentage with recent mental health visits, current antidepressant treatment or both.
Predictive Analytic Software (PASW statistics 18, copyright 1993–2007 Polar Engineering and Consulting, IBM, New York, USA, www.winwrap.com) was used for analyses.
Ethics
The HNEHREC approved the project. Each participant’s results were provided to the GPs with consent. Five cases and one control declined to have results reported to their GP.
Results
Characteristics of cases and controls
ATAPS cases were predominately female, mean age 40 years, married, year 12 or tertiary qualified, employed, with annual household income < $50,000, attending a Newcastle area GP. Relationship status, income level, GP network and employment were significantly different for cases and controls. Employment was non-significant when tested post hoc as employed versus unemployed or support benefits.
ATAPS cases had significantly more life events, mental disability, psychological distress and psychological symptoms, and were more likely to have antidepressant treatment and recent GP mental health care. Cases were more likely to have any anxiety or any mood disorder, although these disorders were also common in controls. Any anxiety or any mood disorder occurred in 52 (82.5%) cases and 33 (51.6%) controls.
There was no difference for current physical illness, although physical disability was significantly lower in ATAPS cases (Table 1).
Characteristics of ATAPS cases and GP controls.
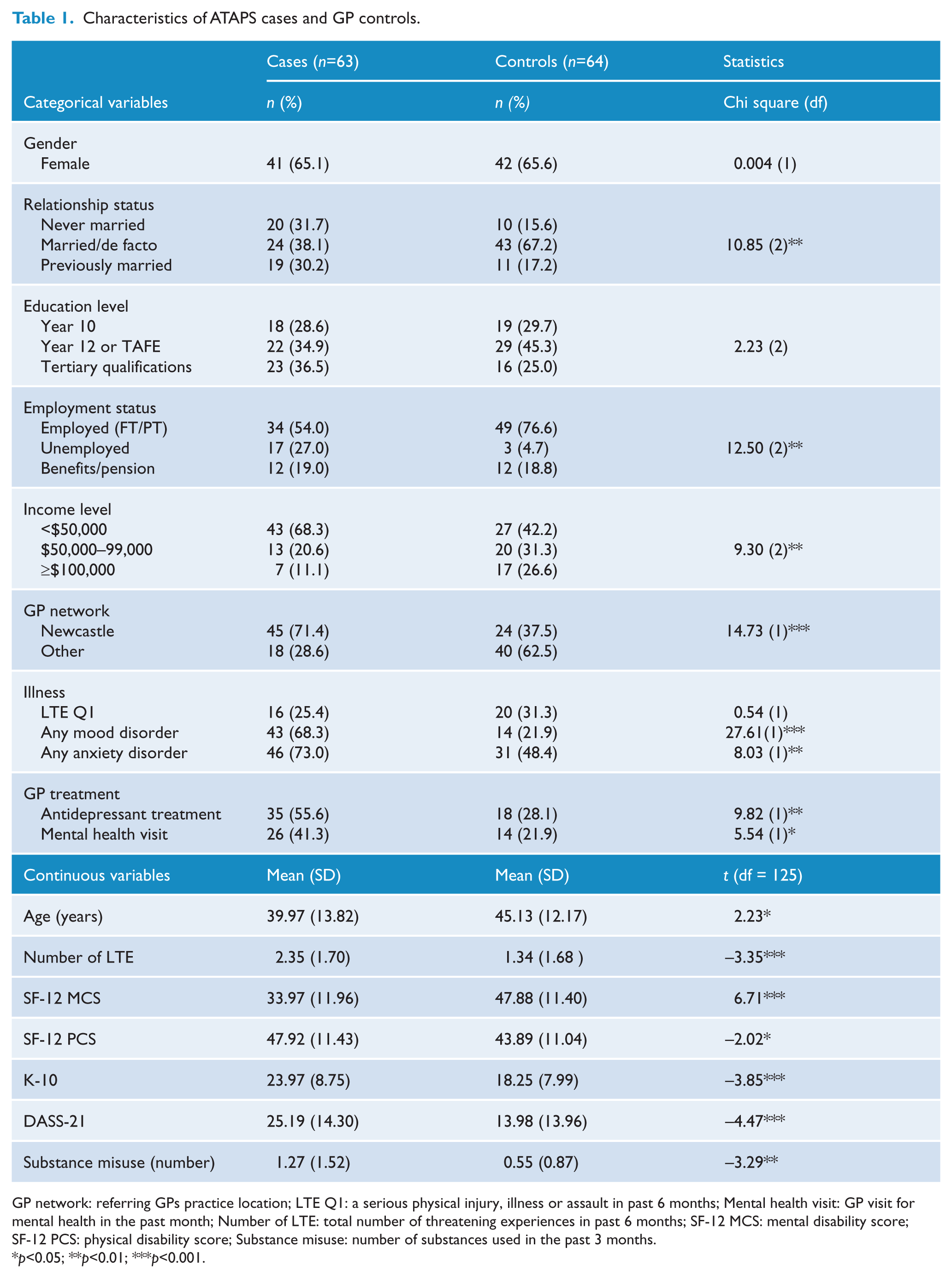
GP network: referring GPs practice location; LTE Q1: a serious physical injury, illness or assault in past 6 months; Mental health visit: GP visit for mental health in the past month; Number of LTE: total number of threatening experiences in past 6 months; SF-12 MCS: mental disability score; SF-12 PCS: physical disability score; Substance misuse: number of substances used in the past 3 months.
p<0.05; **p<0.01; ***p<0.001.
Regression models
Any mood disorder was significant in the unadjusted model (OR 7.68, 95% CI: 3.47, 17.01), and remained significant after adjustment in all nine models. Any anxiety disorder was significant in the unadjusted model (OR 2.88, 95% CI: 1.37, 6.05), but became non-significant in models adjusted for demographics, mental disability, psychological distress, and any mood disorder (Table 2). Higher (incremental) K-10 and DASS-21 scores predicted case versus control and these models became non-significant only when adjusted for any mood disorder or mental disability (Table 3).
Unadjusted and adjusted models for any mood and any anxiety disorder associated with being an ATAPS case.
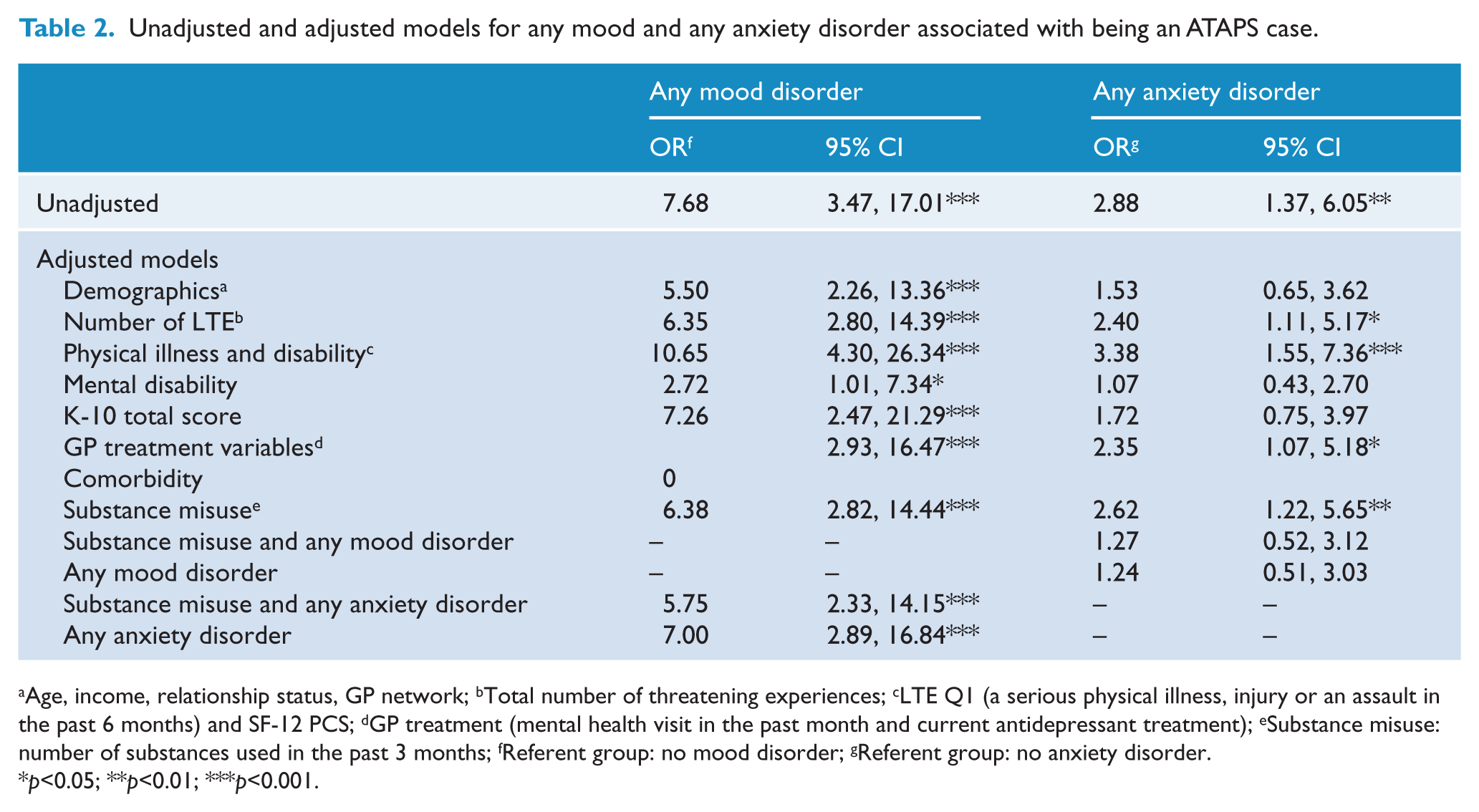
Age, income, relationship status, GP network; bTotal number of threatening experiences; cLTE Q1 (a serious physical illness, injury or an assault in the past 6 months) and SF-12 PCS; dGP treatment (mental health visit in the past month and current antidepressant treatment); eSubstance misuse: number of substances used in the past 3 months; fReferent group: no mood disorder; gReferent group: no anxiety disorder.
p<0.05; **p<0.01; ***p<0.001.
Unadjusted and adjusted models for K-10 and DASS scores associated with being an ATAPS case.
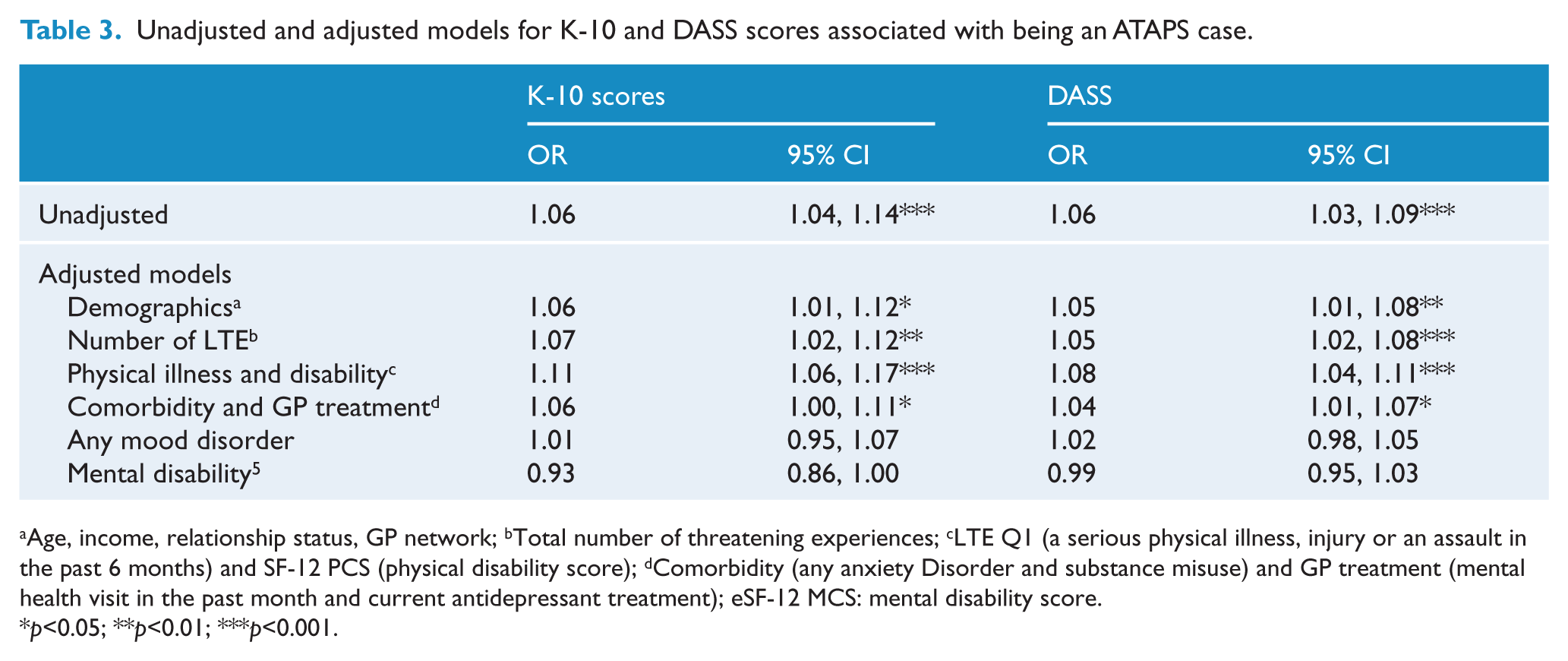
Age, income, relationship status, GP network; bTotal number of threatening experiences; cLTE Q1 (a serious physical illness, injury or an assault in the past 6 months) and SF-12 PCS (physical disability score); dComorbidity (any anxiety Disorder and substance misuse) and GP treatment (mental health visit in the past month and current antidepressant treatment); eSF-12 MCS: mental disability score.
p<0.05; **p<0.01; ***p<0.001.
Overall, any mood disorder was a strong independent categorical predictor for being a case. Adjustment for mental disability reduced the ORs for all four main predictor variables whilst current physical illness combined with higher scores SF12 physical disability (indicating less physical disability) increased the ORs for all four main predictors.
The forward stepwise regression model yielded three predictive variables: greater mental disability had higher likelihood of ATAPS caseness (OR 0.90, 95% CI: 0.87, 0.94 for each unit increase on SF12 MCS), greater physical disability had lower likelihood of ATAPS caseness (OR 1.07, 95% CI: 1.02, 1.11 for each unit increase on SF12 PCS) and more substances misused had higher likelihood of ATAPS caseness (OR 1.63; 95% CI: 1.08, 2.46 for each additional substance misused). The –2 log likelihood for the model was 124.04 and R2 = 0.45. The post hoc confirmatory stepwise regression model yielded four predictive variables (see Table 4): Any mood disorder, two or more threatening experiences and greater mental disability (higher likelihood of ATAPS caseness); and greater physical disability (lower likelihood of ATAPS caseness). This model had R2 = 0.61 and –2 log likelihood was 112.31.
Univariate and confirmatory multivariable forward stepwise logistic regression model associated with being an ATAPS case.
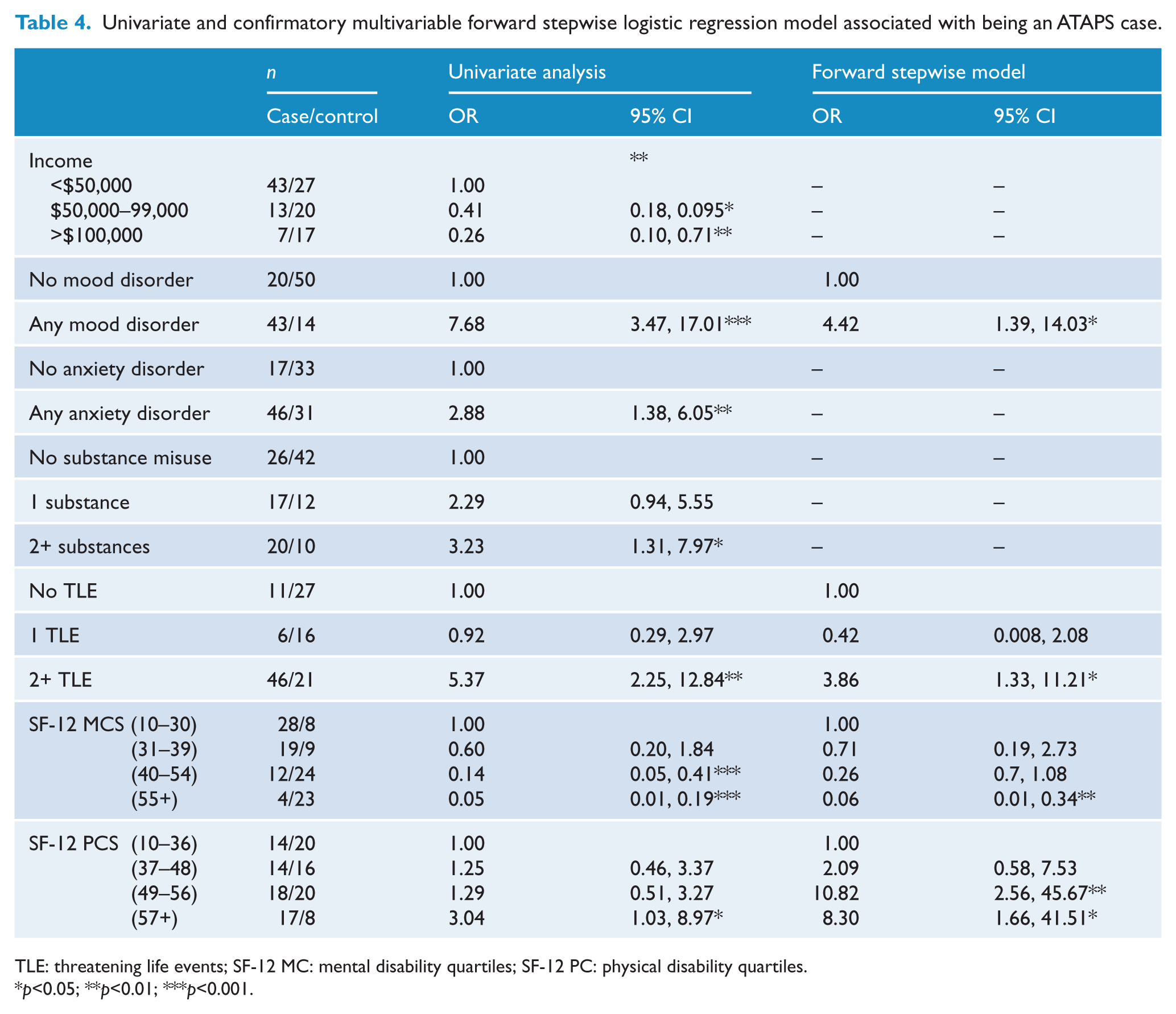
TLE: threatening life events; SF-12 MC: mental disability quartiles; SF-12 PC: physical disability quartiles.
p<0.05; **p<0.01; ***p<0.001.
In the post hoc analysis of controls 31 (48.4%) met criteria for any anxiety disorder. Of these 14 (45.2%) were not receiving any mental health care, whereas 5 (16.1%) were only receiving antidepressant treatment, 4 (12.9%) only GP mental health care and 8 (25.8%) were receiving both.
Discussion
Strengths and limitations
The study was adequately powered for the primary predictors but caution should be used in interpreting the specific estimates in the multivariable models. An unmatched case control design was appropriate for the study questions. The internal validity of studies of this type depends on the degree of bias (especially selection and information biases) and confounding. There may have been substantial selection bias for several reasons. ATAPS cases were recruited from within the ATAPS service and across the five GP Access networks, while controls were recruited from 20 participating GP practices in four of the five networks. There was no random selection of cases or controls and the underlying populations are very large compared to the number selected. There was a different time frame for sampling the cases and controls and a differential non- participation rate was possible.
Instruments were validated for Australian primary care, with the same administration for cases and controls. However, administration was by a single rater, not masked to group status. Study results were usually reported to the GP, which may have affected responses, however results were only communicated with consent, which may then limit response bias. There may be unknown confounders not included in our study.
Patient characteristics
The National Survey of Mental Health and Wellbeing (Andrews and Carter, 2001) reported a community prevalence of 13.6% for anxiety or depression, much lower than GP controls (52%) and ATAPS cases (83%) in our study. However, GP controls (52%) were similar to Australian general practice populations (Wilhelm et al., 2008) (49% anxiety or depression), while ATAPS cases (65% female, 68% low income and 83% anxiety or depression), were similar to national ATAPS patients (70% female, 66% low income and 70% anxiety or depression) (Pirkis et al., 2010).
ATAPS guidelines
ATAPS cases were generally suitable for the ATAPS program and this must in part represent successful selection and referral by GPs. The majority of ATAPS cases had anxiety or depression and had low household income in keeping with the ATAPS guidelines. We did not explore the issue of mild to moderate severity.
To the extent that the pattern of results might indirectly indicate GP decision making in selecting patients for referral to ATAPS we offer some speculative explanations. There are other ‘filters’ that affect referral and attendance at ATAPS; patient, family and social factors, data which were unavailable. Patients with anxiety or depression might decline referral or fail to attend an ATAPS appointment for fear of stigma or believe treatment is not useful. Patients with mild or self-limiting depression or anxiety might not attend because they no longer require treatment, while more severe enduring cases might not attend because of negative cognitions and difficulties with the motivational requirements for making and attending appointments.
Any mood disorder was the stronger categorical main predictor. Any anxiety disorder had a smaller odds ratio as a predictor of ATAPS caseness due to the relatively high frequency of anxiety in controls and was more likely to be made non-significant by adjustment.
Anxiety was common in GP controls. GPs might differentially under-recognise anxiety or consider anxiety to be a chronic condition not requiring specific treatment (Kartal et al., 2010), may prefer to manage anxiety in primary care (Comino et al., 2003), or consider anxiety to be transient or an ‘understandable’ response to life circumstances that will resolve without intervention (Wilhelm et al., 2008). Patient factors might include a lower perceived need for care or a preference to manage anxiety themselves (Andrews and Carter, 2001; Issakidis and Andrews, 2002), believe treatment will not help (Andrews et al., 2001; Jorm and Griffiths, 2006) or that the very symptoms of anxiety are an obstacle to help-seeking (Jorm and Griffiths, 2006).
The post hoc analysis showed that around half of the controls with any anxiety disorder were not accessing any mental health treatment, suggesting these were not recognised by GPs or considered unresponsive to treatment. Conversely, half had recent GP treatment suggesting a preference for GP treatment of anxiety, perhaps by both patients and GPs.
GPs are asked to provide one other measure for referral to ATAPS; the K-10 and some form of the DASS most commonly used nationally (Pirkis et al., 2010). K-10 and DASS-21 scores were significantly higher for cases, suggesting that GPs may have used these continuous measures in addition to their clinical diagnosis, to determine referral. Both measures showed similar results for all adjusted models, with an unadjusted relative increase in the likelihood of referral to ATAPS of 6% for each increased point on either scale. For practical use, the K10 has the advantage of fewer items while the DASS-21 has the advantage of greater coverage of psychological symptoms and stress.
The ATAPS guidelines (Australian Government Department of Health and Aging, 2010) also say services should be prioritised for patients for ‘whom Medicare based services are not affordable or appropriate’, that is, patients who are financially disadvantaged. There were significant differences in terms of income, suggesting GPs were selecting financially disadvantaged patients. Most cases (68%) had annual household incomes of < $50,000, with a substantial minority either unemployed or on other benefits (46%).
We suspect GPs may be influenced by additional factors in the selection of patients for referral.
Other factors potentially affecting GP referral decisions
Given that 17% of cases did not have either anxiety or depression while 52% of controls did, GP referrals to ATAPS were influenced by factors in addition to the presence of anxiety or depression. Only speculative inferences can be made from the pattern of patient characteristics that differentiate cases from controls.
Demographic variables (combined) substantially reduced the ORs for any mood and any anxiety disorder as predictors. Specifically, cases were younger, had lower proportions in a relationship (38%) and had less distance to travel to the ATAPS service.
Mental disability for cases was in the moderate (30–40) and controls in the mild range (40–50), with substantial effects in all adjusted models. Conversely, cases had lower levels of physical disability than controls (both mild range 40–50), which also affected all adjusted models. The multivariable regression model results were consistent with the adjusted models; cases had significantly higher mental disability and lower physical disability compared with controls. This suggests GPs might be differentially selecting patients with psychological symptoms plus substantial mental disability, which seems appropriate. However, it also suggests that GPs tend not to refer those with psychological symptoms if they have associated higher levels of physical disability, which needs explanation and future exploration.
There are several possible explanations. GPs may not easily recognise mental illness in the presence of physical disability (Simon and Von Korff, 2006), or feel that physically disabled patients might reject psychological treatments (Jorm and Griffiths, 2006) or believe psychological treatment is ineffective with higher physical disability. They may also consider that physical disorders take treatment priority over mental disorders and psychological distress. However, physical and mental disorders are not mutually exclusive and response to treatment is good (Peverler et al., 2002).
Substance misuse is also a valid mental disorder for referral to ATAPS. Locally, patients with primary drug or alcohol dependence are referred to specialist services. Despite this, the greater number of substances currently misused affected the risk in the four predictors in adjusted models and was a significant independent predictor of caseness in the first multivariable model (OR 1.63, 95% CI: 1.08, 2.46). This suggests that substance misuse might be a more important reason for referral to ATAPS than previously thought.
Clinical utility of standardised measures and screening instruments
Short, standardised instruments have been successfully used in primary care in Australia to detect common mental illnesses and problematic drug and alcohol use (Hickie et al., 2001b). This study has demonstrated the potential utility of measures like K10 or DASS in helping GPs make referral decisions to ATAPS. Similarly, the SF-12 is a short instrument that could be used in GP settings to provide information about mental and physical disability levels, in the presence of common mental illness (Sanderson and Andrews, 2002).
The US Preventive Services Task Force recommended screening adults for depression in primary care only when professional supports are in place to assure accurate diagnosis, effective treatment and follow-up (O’Connor et al., 2009). The availability, general acceptability and effectiveness of the ATAPS program (Pirkis et al., 2011) means that this level of support is now widely available, especially to the financially disadvantaged. So the development of effective screening for common mental illness, distress and disability at the primary care level, integrated with ATAPS referral, could become a reality for future patients.
Policy implications for the ATAPS program
To the extent that results of this study are generalisable to the national population, several issues may have an impact on the policy development and review of the ATAPS program.
The presence of current physical illness and lesser physical disability increased the ORs for any mood disorder or any anxiety disorder to predict ATAPS caseness in the adjusted models. ATAPS cases had lower levels of physical disability even when controlling for any anxiety and any mood disorder in the multivariable model. GP patients with depression or anxiety but with higher levels of physical disability might be differentially excluded from access to the ATAPS program, which is probably not intended in current ATAPS policy.
The Chronic Disease Management program is delivered by GPs. It was designed to improve prevention, early identification and best practice management of chronic illnesses that have been ‘present for at least six months including asthma, cancer, cardiovascular disease, diabetes, musculoskeletal conditions and stroke’; conditions associated with considerable physical and mental disability (Department of Health and Aging, 2011). Identifying mental and physical disability could be potentially addressed by use of the SF-12 in addition to K-10 or DASS-21 with complementary referral pathways to ATAPS and Chronic Disease Management programs.
ATAPS cases misused more substances than controls. Further investigation of the nature and extent of substance misuse in ATAPS patients and appropriate treatment availability is warranted. Seventeen per cent of cases did not meet diagnostic criteria for anxiety or depression, similar to 30% in the national ATAPS population (Pirkis et al., 2010). Further investigation of the symptoms these patients have and whether the ATAPS approved treatments are suitable for them is warranted.
Conclusions
The ATAPS program has made psychological treatments available to many more patients (Hickie and Groom, 2002). This study shows that GPs make referrals which are consistent with the ATAPS referral guidelines. In particular, GPs appropriately refer patients with low incomes, anxiety and depression, especially when associated with substantial mental disability. However, patients with higher levels of physical disability are less likely to be referred, even when they meet criteria for anxiety and depression, a result that warrants further exploration. GPs also refer to ATAPS those with greater substance misuse, which may have relevance for service delivery within the ATAPS program.
Because depression and anxiety are common in chronic physical illness and are generally responsive to psychological treatments, limitations on access of these patients for psychological treatment may not be optimal. The potential for using standardised instruments in primary care, combined with an integrated referral pathway to ATAPS and Chronic Disease Programs should be explored.
Footnotes
Acknowledgements
We would like to thank several people for their support of this project: the staff of the GP Psychology Service, Ms Katrina Delamothe, Service Manager, and Dr Mark Foster, CEO of GP Access, and all participating general practitioners and their staff. We also thank Dr Andrew Page and Professor Nick Glozier for helpful comments on the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
Professor Carter and Professor Startup have no competing interests in relation to this manuscript. Ms Maddock is employed as a Psychologist in the GP Access Psychology Service in Newcastle to provide ATAPS services.