
Abstract
The importance of maintenance therapy in schizophrenia has been well established and long-term maintenance treatment with antipsychotic medication appears critical in preventing relapse [1,2]. Non-adherence to medication has a serious impact on the course of the illness in patients with schizophrenia. The risk of relapse increases almost 5-fold when antipsychotic drug therapy is discontinued [3]. It also affects worsening of symptoms, suicidal attempts and, consequently, repeated emergency room visits or re-hospitalization [3,4].
Given the devastating effect of psychotic relapse on the course of the illness, relapse prevention strategies should encourage greater awareness of the impact of non-adherence and should incorporate appropriate steps to minimize or eliminate this problem [5]. Identifying the risk factors associated with non-adherence is an important initial step because modifiable risk factors might become targets for future interventions. Non-adherence to medication among patients with schizophrenia has a wide range of courses [6]. There is general agreement that adherence is mediated by several factors broadly categorized as either patient-, environment-, or treatment-related [5,6]. Symptomatology, cognitive functions, disease insight, and presence of substance abuse are considered as the most important features [5]. However, few studies have adequately identified the relative importance of the different risk factors. Most studies have tended to examine the impact of each risk factor in isolation [5,7]. Furthermore, the lack of economic access to health care, which is an important factor influencing non-adherence [8], has rarely been explored. It is generally acknowledged that subjects with severe mental illness have inadequate access to mental health services [9,10]. People suffering from schizophrenia face numerous barriers to receiving appropriate health care and a lack of health insurance is an important factor influencing the utilization of mental health services. McCann et al. [11] found that many patients with schizophrenia reported dissatisfaction with the level of access to their mental health care providers, especially psychiatrists, and that the lack of access significantly predicted medication omission. As such, the French health system may offer an interesting approach by controlling this factor as its universal access to care guarantees totally free health care and access to the most appropriate treatment, regardless of cost.
The aim of this study was to quantify the factors associated with non-adherence to medication among stable patients suffering from schizophrenia in the context of universal access to care.
Patients and methods
Study population
This cross-sectional, naturalistic, multicenter study was conducted in 15 French public hospitals in a region of south-eastern France during a 1 week period in 2008. All consecutive outpatients who met the following criteria were recruited and included in the study: diagnosis of schizophrenia or schizoaffective disorder according to DSM-IV criteria confirmed through administration of a Structured Clinical Interview (SCID) [12], stable schizophrenia or schizoaffective disorder (no need for hospitalization at inclusion and no major change in the patients condition for 2 months prior to inclusion [13]), 15–75 years of age, written informed consent to participate in the study, and French as native language. The project was conducted in accordance with the Declaration of Helsinki [14] and French Good Clinical Practice. The French National Commission for Data Protection (CNIL) approved this study [15]. Founded on January 6, 1978, the CNIL is an independent administrative authority protecting privacy and personal data.
Procedure
All outpatients who met the diagnostic criteria were asked to take part in the study. The following information was collected at the same time using either self-rating questionnaires completed by the patients (attitude toward medication measure and therapeutic alliance) or through a routine clinical interview by a psychiatrist (psychiatric assessment and insight measure). These assessments were chosen on the basis of proven reliability and validity.
Attitude toward medication measure
The patients’ attitudes towards treatment were assessed with the 10-item Drug Attitude Inventory (DAI) [16,17]. This self-report instrument includes 10 questions on the subjective response to neuroleptic medication, including both positive drug effects (e.g. prevention of relapses) and negative ones (e.g. dysphoric reactions). The DAI correlates with both clinician-rated adherence and biochemical measures of adherence. In addition, the scale has good internal consistency and high test–retest reliability, indicating good validity and reliability. Scores range between −10 and +10: scores ≥ 0 suggest adherence and < 0 suggest non-adherence.
Psychiatric assessment
The following data were recorded:
Socio-demographic characteristics: gender, age, marital status (single or divorced/separated versus married/stable partnership), educational level (primary school, high school, university), employment status (employed/unemployed), living situation (living independently versus living with family members/in an assisted living facility), income, family and friend support (presence versus absence).
Clinical characteristics: type of schizophrenia according to DSM-IV, age at onset of illness, duration of illness, duration of untreated psychosis (DUP) defined as the time between the appearance of at least one psychotic symptom until initiation of adequate treatment [18]. Psychotic symptoms were assessed using the Clinical Global Impression (CGI) of severity and global functioning was investigated with the Global Assessment of Functioning (GAF) scale [19].
Current substance use disorder: tobacco, alcohol, opioids, cannabinoids, and cocaine.
Current antipsychotic medication: first generation (or typical) antipsychotics (FGAs), second generation (or atypical) antipsychotics (SGAs) or antipsychotic polypharmacy.
Current antipsychotic medication: oral versus depot formulation.
Psychotherapeutic activity (presence versus absence).
Number of hospitalizations since the onset of schizophrenia.
Insight measure
Insight was measured by the psychiatrist using the Scale to assess Unawareness of Mental Disease (SUMD) [20]. The following three global insight dimensions were used: (i) ‘having a mental disorder’, (ii) ‘effects of medication’, (iii) ‘consequences of the mental disorder’. Each of these dimensions is rated on a 5 point rating scale: 0 ‘not applicable’, 1 ‘aware’, 3 ‘somewhat aware/unaware’, and 5 ‘severely unaware’. Following the criteria of Amador and Strauss [21,22], a score ≥ 3 was indicative of a poor individual level of insight.
Therapeutic alliance measure
Therapeutic alliance was assessed using the Patient Session Questionnaire (PSQ) [23]. This self-report questionnaire covers the therapeutic alliance as perceived by the patient: (i) the therapist and I understand each other, (ii) ‘today I felt at ease with the therapist’, and (iii) ‘I think the therapist is really interested in my well-being’. The statements are rated on a 7 point Likert scale ranging from −3, ‘absolutely not true’, 0, ‘neither nor’, and +3, ‘absolutely true’. Only the composite alliance score is presented here. The final score ranges from −3 to +3, with higher scores reflecting a better therapeutic alliance.
Statistical analysis
Patients were grouped as adherent or non-adherent according to positive (≥ 0) or negative (< 0) scores on the 10-item DAI. The socio-demographic and clinical characteristics, presence of substance use disorder, antipsychotic medication and psychotherapeutic activities, and the scores for insight and therapeutic alliance were compared between the two groups using the Student's t-test for continuous variables and Chi-squared test for categorical variables. A logistic regression analysis was used to estimate the odds ratio (OR) for risk factors associated with non-adherence, after adjusting for confounding factors. Models were developed with a backward selection procedure. Variables relevant to the model were selected based on their clinical interest and/or a threshold p value (≤ 0.02) in univariate analysis. The following variables were included in the analysis, with the respective reference groups listed in parentheses: age, gender (female), education level (university), income (≥ $1000), family support (absence), DUP, CGI, GAF, current substance use disorder: cannabinoids (absence), current antipsychotic medication (typical), current antipsychotic medication (oral), insight (SUMD < 3), therapeutic alliance (PSQ), and the number of hospitalizations since the onset of schizophrenia. The statistical significance level was set at P = 0.05 in a two-sided test. Data were analysed using SPSS 15.0 software.
Results
Of the 383 patients who were eligible in the study, 29 refused and 53 were not evaluated by the psychiatrists (Figure 1). Of the 301 patients who were enrolled, 10 were excluded from this study because they did not respond to the DAI. Our sample analysis consisted of 291 patients (75.9%). The socio-demographic variables were similar for the included (n = 291) and non-included patients (n = 92) (all p values >0.05).
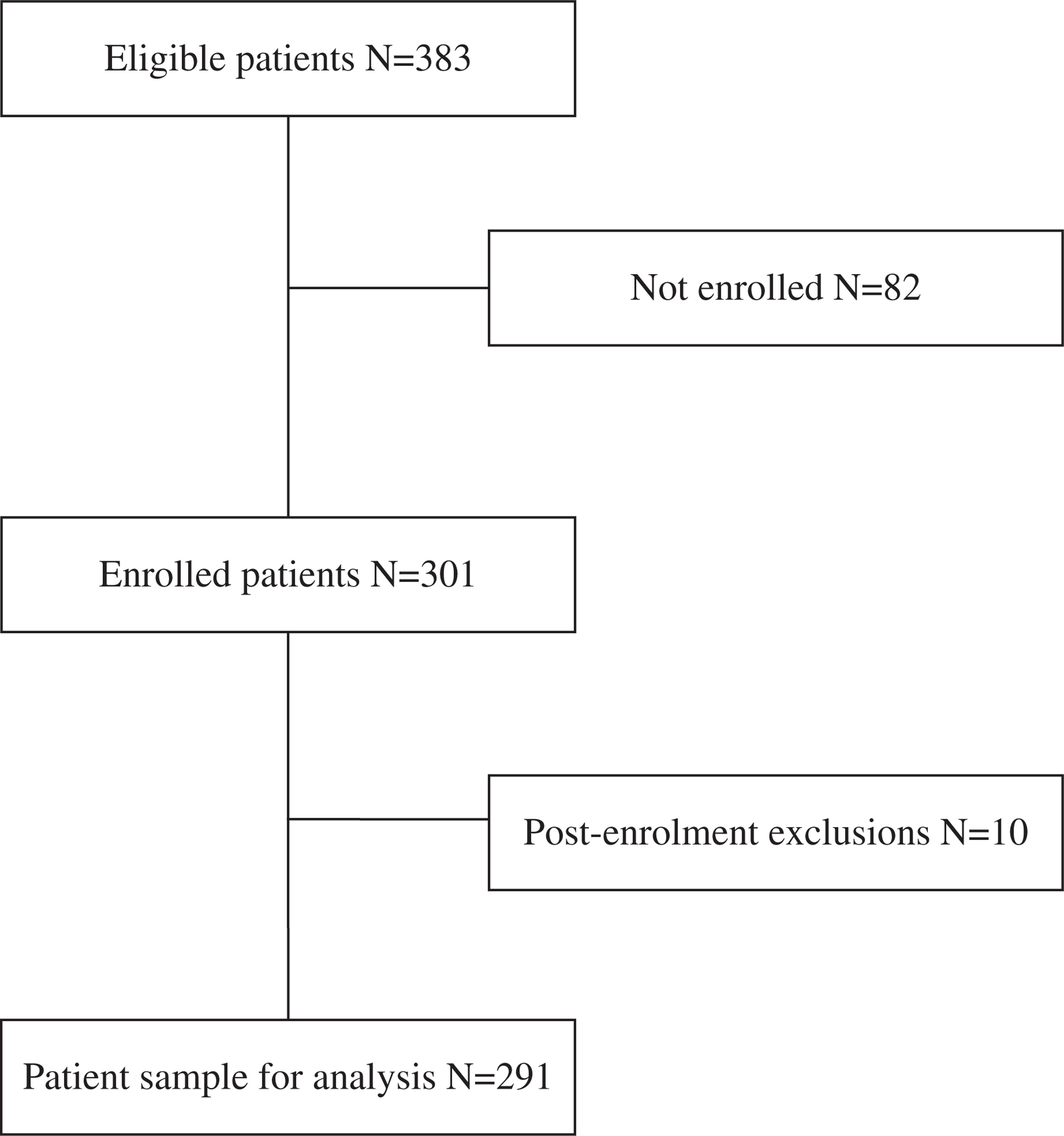
Patient enrolment. The analytical sample consisted of patients with diagnosis of schizophrenia or schizoaffective disorder, stable schizophrenia or schizoaffective disorder, 15–75 years of age, informed consent to participate in the study, and French as native language.
Based on the adherence measure, 30% of patients were considered to be non-adherent. The results of univariate analysis, summarized in Table 1, showed that only two of the socio-demographic characteristics were statistically associated with non-adherence: non-adherent patients had a lower level of education and less family support compared to adherent patients. There was no significant difference in clinical characteristics between the two groups according to the different subtypes of schizophrenia or in terms of the duration of the illness or DUP. In contrast, the severity of psychosis (CGI) was higher in non-adherent patients than in adherent patients (p = 0.008), and the global functioning (GAF) of non-adherent patients was lower than for adherent patients (p = 0.001). Substance use disorders, type of antipsychotic medication, and presence of a psychotherapeutic activity did not differ significantly between the two groups. As expected, the number of psychiatric hospitalizations was higher for non-adherent patients than for adherent patients (6.2 ± 7.0 versus 4.5 ± 4.4, respectively; p = 0.04). Non-adherent patients also presented a lower level of insight than adherent patients for the three dimensions of the SUMD: having a mental disorder, effect of medication, and consequences of the mental disorder (p < 0.001). The level of therapeutic alliance was significantly lower for non-adherent patients than for adherent patients (p<0.001).
Socio-demographic and clinical characteristics of non-adherent and adherent patients (N = 291)
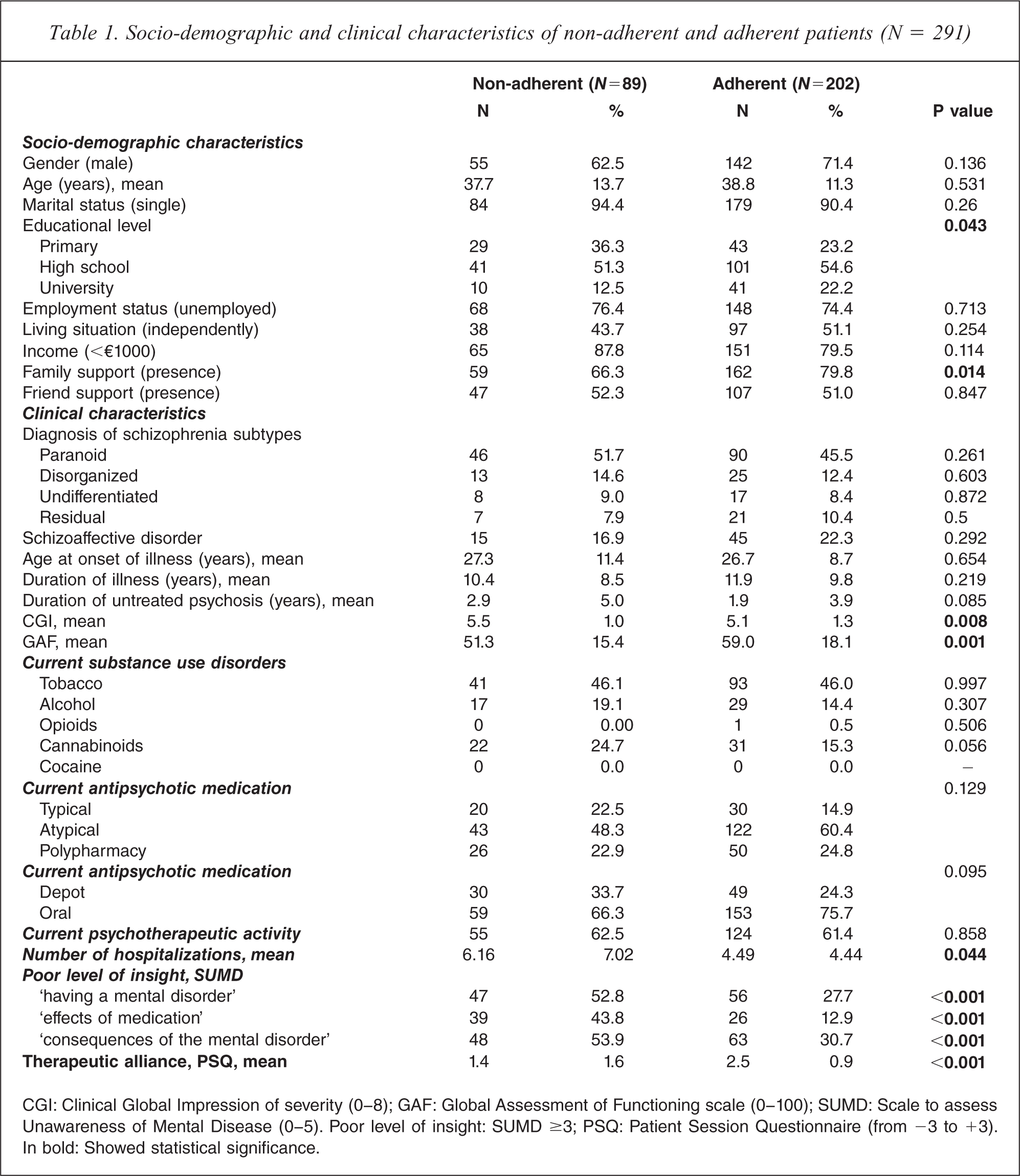
CGI: Clinical Global Impression of severity (0–8); GAF: Global Assessment of Functioning scale (0–100); SUMD: Scale to assess Unawareness of Mental Disease (0–5). Poor level of insight: SUMD ≥3; PSQ: Patient Session Questionnaire (from −3 to +3). In bold: Showed statistical significance.
In multivariable analysis (Table 2), non-adherence increased with the DUP (OR = 1.12, 95%CI = 1.03–1.22), lack of insight only for the effect of medication (second dimension of the SUMD) (OR = 3.23, 95%CI = 1.05–9.89), and low level of therapeutic alliance (OR = 0.45, 95%CI = 0.32–0.64). Individuals prescribed atypical antipsychotic drugs were more likely to be adherent than those prescribed typical antipsychotics (OR = 0.37, 95%CI = 0.13–1.00). The number of psychiatric hospitalizations was higher for non-adherent patients than for adherent patients (OR = 1.09, 95%CI = 1.00–1.19).
Factors associated with non-adherence (N = 291)
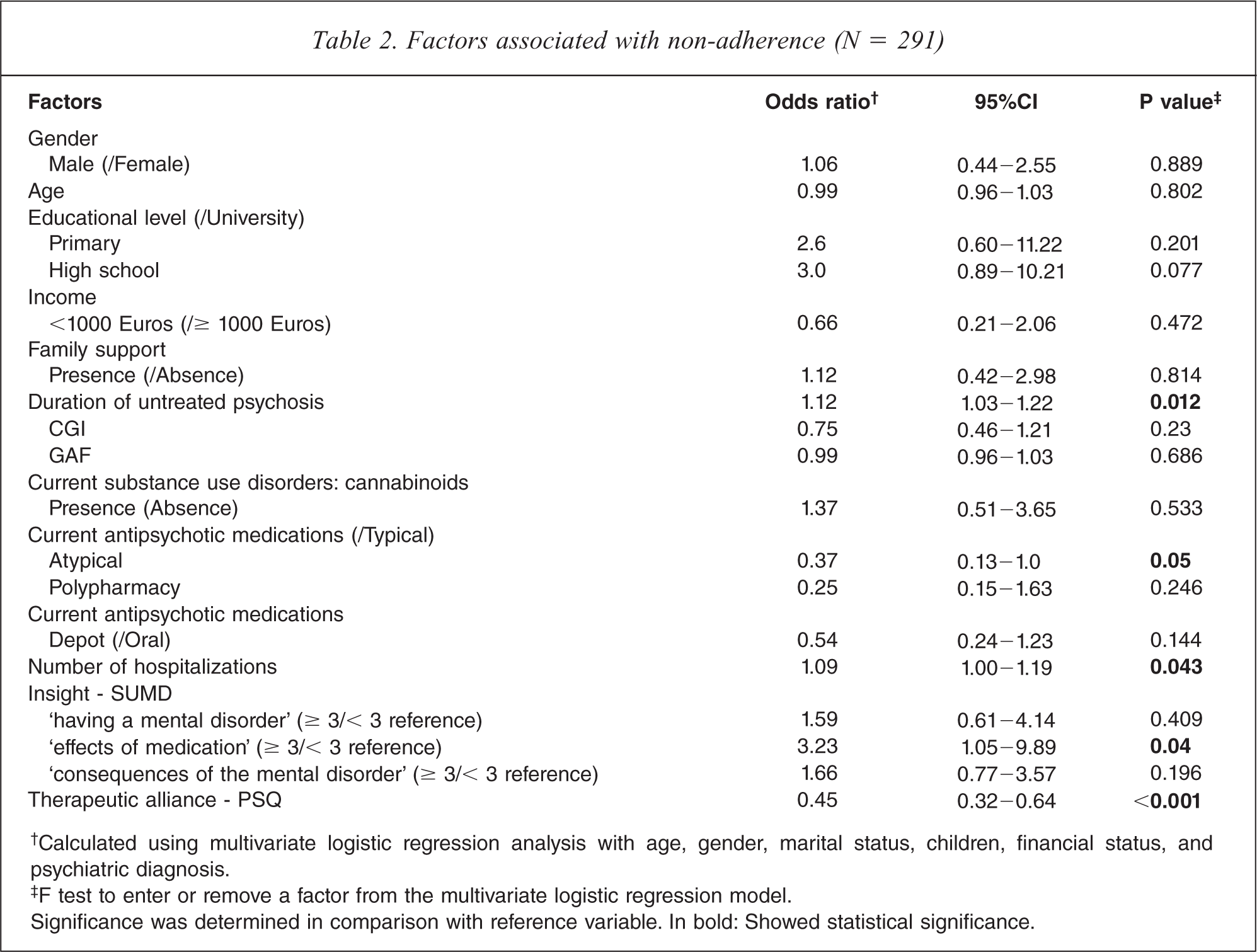
†Calculated using multivariate logistic regression analysis with age, gender, marital status, children, financial status, and psychiatric diagnosis.
‡F test to enter or remove a factor from the multivariate logistic regression model.
Significance was determined in comparison with reference variable. In bold: Showed statistical significance.
Discussion
This study explored the relative importance of different risks factors associated with non-adherence to medication among patients suffering from schizophrenia. DUP, prescription of SGAs in comparison to FGAs, therapeutic alliance, and poor insight were the most important features associated with non-adherence. These findings differ substantially from those found in previous studies for several reasons. First, previous studies have varied in design, potential predictors, and sample examined, and manner in which adherence was defined and measured [6,24]. Given this variability, it is rare that consistent predictors of adherence have emerged. Second, one of the strengths of our study is that the French health care system is characterized by near-universal access, which allowed us to quantify the risk factors independently of economic barriers. Considering this last characteristic, several hypotheses must be discussed and clarified.
Socio-demographic factors
In contrast to previous studies, the socio-demographic factors considered here failed to account for the differences in attitude towards medication. Previous studies have generally found that younger age, lower level of education, and lack of a family member with an involvement in the treatment plan were associated with adherence problems [25–27]. These factors generally reflect a relationship between poorer socioeconomic status and a failure to prioritize mental health or levels of engagement with health services [5]. Our results can confirm this hypothesis. Economic factors pertinent to medication adherence include whether patients have insurance or another financial resource to pay for the medication, but this is not required in the French health care system. As such, the importance of economic factors should not be neglected in public policies or strategies to address adherence problems in non-universal coverage systems. Non-adherence is not just a patient-related phenomenon [6]. The majority of patients who have difficulty paying for medication report skipping medication some of the time [28,29].
Diagnosis and medication
Unlike previous studies [7,30,31], age at onset of the illness, severity of symptoms, and illicit drug or alcohol use were not associated to non-adherence. It can also be hypothesized that these factors may be linked to lower socio-economic status, which can have an impact on financial resources to pay for medication.
An interesting result in our study concerns the DUP, which is strongly associated with non-adherence. This result has rarely been reported previously in the literature but seems coherent with the concept of DUP. It has been suggested that a longer DUP may be associated with poorer treatment outcome as a result of the toxic effects of the psychosis experience [32]. Perkins et al. [33] demonstrated the importance of DUP influencing response to treatment, reflecting a potentially malleable progressive pathological process. However, several studies have not identified a relationship between DUP and non-adherence to medication [34,35]. Our findings must be analysed with caution and need to be confirmed. One major difficulty is definition and measurement of DUP, for which there are no reliable measures. If the relationship between DUP and adherence is confirmed, it will be important to alert clinicians to this critical period.
Another interesting result in our study concerns the global functioning (GAF) and the severity of psychopathology (CGI). We found a significant statistical difference between non-adherent and adherent patients in the univariate analysis, but this result was not confirmed in the multivariate analysis. This finding seems to confirm the importance of not examining the impact of each risk factor in isolation as in several previous studies. However, this result has to be confirmed in future studies.
Finally, patients treated with SGAs were found to have a better global attitude towards medication than FGA-treated patients. This result seems coherent as SGAs have been shown to be superior to FGAs in terms of treatment of negative symptoms, cognitive enhancement, fewer extrapyramidal symptoms, tolerability, and higher levels of subjective well-being [36]. The burden of side-effects has been extensively explored as a predictor of poor medication adherence [37]. However, while reports have revealed the advantages of SGAs in terms of efficacy and tolerability, the superiority of SGAs in terms of adherence is still controversial [25,38]. One hypothesis is that SGAs have metabolic and weight gain side-effects that may negatively affect adherence [39], and this may explain the small clinical differences in adherence rates between FGAs and SGAs. Our results suggest another hypothesis that the absence of a difference in the literature might be due to the higher cost of SGAs compared to FGAs, which can constitute an important barrier to adherence. This hypothesis needs to be confirmed in future studies.
Insight
Surprisingly, only one aspect of insight, ‘effect of medication’, was associated to drug attitude: patients who were aware of the effect of medication had a more favorable view of medication and adherence. This result contradicts the study of Rocca et al. [29], who found that only awareness of the illness was associated with DAI score. Our result is interesting, however, because it suggests that consciousness of the impact of medication seems to be more important to adherence than awareness of the illness. This result seems to indicate that the patient's subjective satisfaction with medication and its impact on well-being or quality of life is crucial from the perspective of medical adherence [40].
Therapeutic alliance
Our findings for therapeutic alliance confirm the results of earlier studies and reviews concerning the importance of therapeutic alliance in promoting adherence to treatment in patients with schizophrenia [35,41,42]. A good patient–physician relationship is essential to developing individualized treatment approaches which address issues interfering with adherence. Kikkert et al. [43] reported a positive influence on adherence if professionals focus on positive aspects of medication, an enhancing insight, and on fostering a positive therapeutic relationship with patients and carers.
Limitations
Several limitations should be considered in our study.
Adherence behavior is not easy to detect and quantify, and all methods of detection have some drawbacks. As such, the use of the DAI may be criticized. First, this is a subjective method of assessing adherence in comparison with objective methods such as pill counts, pharmacy records, electronic monitor and plasma concentrations. However, as suggested by Velligan et al., even the use of more objective measures can be associated with significant errors [22]. Second, while the 10-item DAI is easy to administer and is widely used, the scale is old and was only validated before the development of new antipsychotics. However, this scale has good psychometric properties, has been shown to predict compliance [15] and is still largely used [7,44,45].
The study is also limited by the fact that it is cross-sectional rather than prospective in design, the study period was only 1 week, and the site of the study was not based on random assignment. As such, the results may not be representative of schizophrenic patients and should be generalized with care. However, the naturalistic, multicentric approach, and high response rate can limit this bias.
Another limitation of our study is the absence of assessment of side effects considering this is likely to be an important determinant of adherence to treatment. The assessment of side effects should be addressed in future studies.
Finally, the use of CGI to measure the severity of psychopathology instead of other scales as the Positive and Negative Syndrome Scale (PANSS [46]) can be criticized. While the CGI is easier to use and understand, the PANSS may be preferred due to its strong psychometric properties of reliability and validity. However, several studies support the extrapolation between the PANSS and CGI [47].
Conclusion
The true non-adherence rate is difficult to assess and there is no agreement regarding the gold standard for this measurement. In this cross-national study we chose to investigate self-reported non-adherent behaviour in a naturalistic manner. The challenge was to explore and quantify the relative importance of the different risk factors. In our patient sample it can be concluded that DUP, prescription of SGAs, therapeutic alliance, and insight were the most important features associated with non-adherence. This study also suggests that economic factors such as the service delivery system should not be neglected in public strategies to address the problem of non-adherence.
Footnotes
Acknowledgements