
Abstract
Keywords
The number of people with dementia is increasing rapidly worldwide, with about 4.6 million new cases every year [1]. The results of early studies suggested that the risk factors for Alzheimer's disease were largely non-modifiable, such as increasing age [2] and family history of dementia [3], but more recently it has become apparent that modifiable factors including education, physical activity, diabetes, brain injury, smoking and alcohol use, may also play a role [4–9].
Australian Aboriginal and Torres Strait Islander peoples experience high levels of co-morbid health conditions and are exposed to a disproportionally high number of health hazards during the course of their lives [10]. This may contribute to the observed discrepancy in life expectancy of Indigenous and non-Indigenous Australians [11], as well as to the high prevalence of dementia observed in Aboriginal communities. A recent prevalence study conducted in remote Western Australia found that 12.4% of Aboriginal people aged over 45 years have dementia (and 26.8% aged over 65 years), a prevalence rate that is five times greater than in the remainder of the Australian population [12].
This study was designed to investigate the demographic, lifestyle and clinical factors associated with dementia in Aboriginal people living in the Kimberley region. We were particularly interested in the role of potentially modifiable factors that may be amenable to interventions to decrease the burden of dementia amongst Aboriginal and Torres Strait Islander peoples.
Materials and methods
Setting
The vast Kimberley region (421/451 km2), is the sparsely populated northern-most region of Western Australia. Kimberley has the highest proportion of Aboriginal and Torres Strait Islander peoples in Western Australia at 42% [13], with Aboriginal communities in Kimberley being comprised primarily of Aboriginal Australians. Approximately 30 Aboriginal languages are spoken in the Kimberley region.
In this cross-sectional study we used semi-purposeful sampling techniques to identify six remote Aboriginal communities and one town in the Kimberley region. No comprehensive sampling frame exists for this region with the Aboriginal and Torres Strait Islander population being under-represented in the electoral roll [14], and completing a comprehensive survey of the vast and often inaccessible region would not have been feasible. A sampling frame was developed to ensure effective coverage of all language families in the region.
Participants
A target sample size of 400 was based on an expected prevalence rate of dementia of 10% to achieve a standard error of 1.5%. All Aboriginal community members aged over 45 years living in the communities at least six months of the year were eligible to take part in the study. As a large number of people living with dementia are placed from the community into residential care, people living in residential care that were originally from these communities and town were also eligible. One third of the town's eligible population was randomly sampled. A nominated family member or carer for each participant took part in the assessment. People who were acutely unwell were excluded from the study. Lists of community members were provided by the local health services and community office, combined and then updated by Aboriginal community workers.
Procedures
Following the community consultation and approval phase, Aboriginal community members were employed and trained in the use of the Kimberley Indigenous Cognitive Assessment (KICA). The KICA is a locally developed valid cognitive tool for the Kimberley Aboriginal population freely available on www.wacha.org.au/kica.html [15]. It is also used to collect information from the participant and their caregiver on past medical history, smoking and alcohol, emotional well-being and activities of daily living.
Aboriginal community workers used the KICA to screen participants. Interpreters were employed as required. Participants completed the cognitive assessment (KICA-Cog) and participants and informants reported on their demographic, lifestyle and clinical factors. Within 3 months of assessment all participants scoring less than 37 on the KICA-Cog and a random sample of those scoring 37 or more were reviewed by specialist clinicians (geriatrician or psychogeriatrician) who, blinded to the KICA results, performed a clinical examination, collected history from the informant and reviewed participants’ medical records. With consent, this information was fed back to the participant's doctor and local health clinic. The specialist assessment was also forwarded for DSM-IV and ICD-10 dementia consensus diagnoses to two other specialists.
At the conclusion of the study, details on the prevalence of health conditions in each community sample were reported back to community councils (remote community governing body) and approval was gained from council members to disseminate results. Aged care education was provided to interested community members and other key stakeholders.
Measured exposures
The key factors analysed for association with dementia were demographic features: age, sex, education; lifestyle factors: smoking, alcohol and chewing tobacco; and clinical: head injury, heart disease, hypertension, diabetes, previous stroke, epilepsy, falls, mobility, incontinence, urinary problems, vision and hearing.
Statistical analyses
Data were entered and analysed on SPSS version 15. Associations between variables and the presence of dementia Cognitive impairment not fulfilling the criteria for dementia (CIND) and cognitive impairment (dementia and CIND diagnoses versus no cognitive impairment), were evaluated by univariate and multivariate logistic regression (results reported as odds ratio [OR] and 95% confidence interval [95%CI]). Multivariate logistic regression was used to adjust for the affect of confounding variables. As age, sex and education were strongly associated with dementia all other variables were adjusted for these factors. There is poor access to alcohol and cigarettes in residential care. Due to the high proportion of people residing in residential care with dementia these participants were excluded from analyses of associations of lifestyle factors with dementia.
Ethics approval
The study protocol was approved by the Western Australian Aboriginal Health Information and Ethics Committee (WAAHIEC) and the University of Western Australia Ethics Committee for Human Research. Community council and individual approval was sought and gained, with assistance from paid interpreters or Aboriginal community workers.
Results
Participants
A total of 363 people participated in the study. Refusal rates were low at 5.5%. Reasons given by the participants for not partaking in the study were being too busy, unwell or not interested in being involved.
The age range of the participants was 45 to 96 years, mean 60.7 years (SD 11.9). Fifty-five per cent of participants were female. Forty per cent of participants had never received any formal schooling and 20 Aboriginal languages were spoken. Study informants were primarily adult children of participants (36%), women (76%) and living with the participant (57%). Five per cent of informants were formal carers.
Thirty-five participants (10%) were living in residential care, of whom 5 (14%) were aged 45–59 years, 7 (20%) were 60–69 years, 10 (29%) were 70–79 years and 13 (37%) were aged over 80 years. Twenty-six people (74%) living in residential care had dementia, 6 (17%) had cognitive impairment not dementia and 3 (8.6%) had no cognitive impairment.
Prevalence of lifestyle, demographic and clinical factors
The prevalence of demographic, medical, lifestyle, ageing and sensory factors are presented in Table 1 within dementia diagnosis and total sample. Further details on the prevalence of these factors within CIND and no cognitive impairment diagnoses are presented in Smith et al. 2008 [12]. The most common cause of head injuries was fighting/violence at n = 86 (46.5%), followed by horse riding accidents n = 27 (14.6%), motor vehicle accidents n = 19 (10.3%), falls n = 13 (7%), sorry time (hit head with hard object when family member died) n = 11 (5.9%), a sporting accident and lightning strike (both n = 1, 0.5%). For 24 participants (13%) the reason for head injury was not recorded.
Characteristics of 363 subjects aged over 45 years
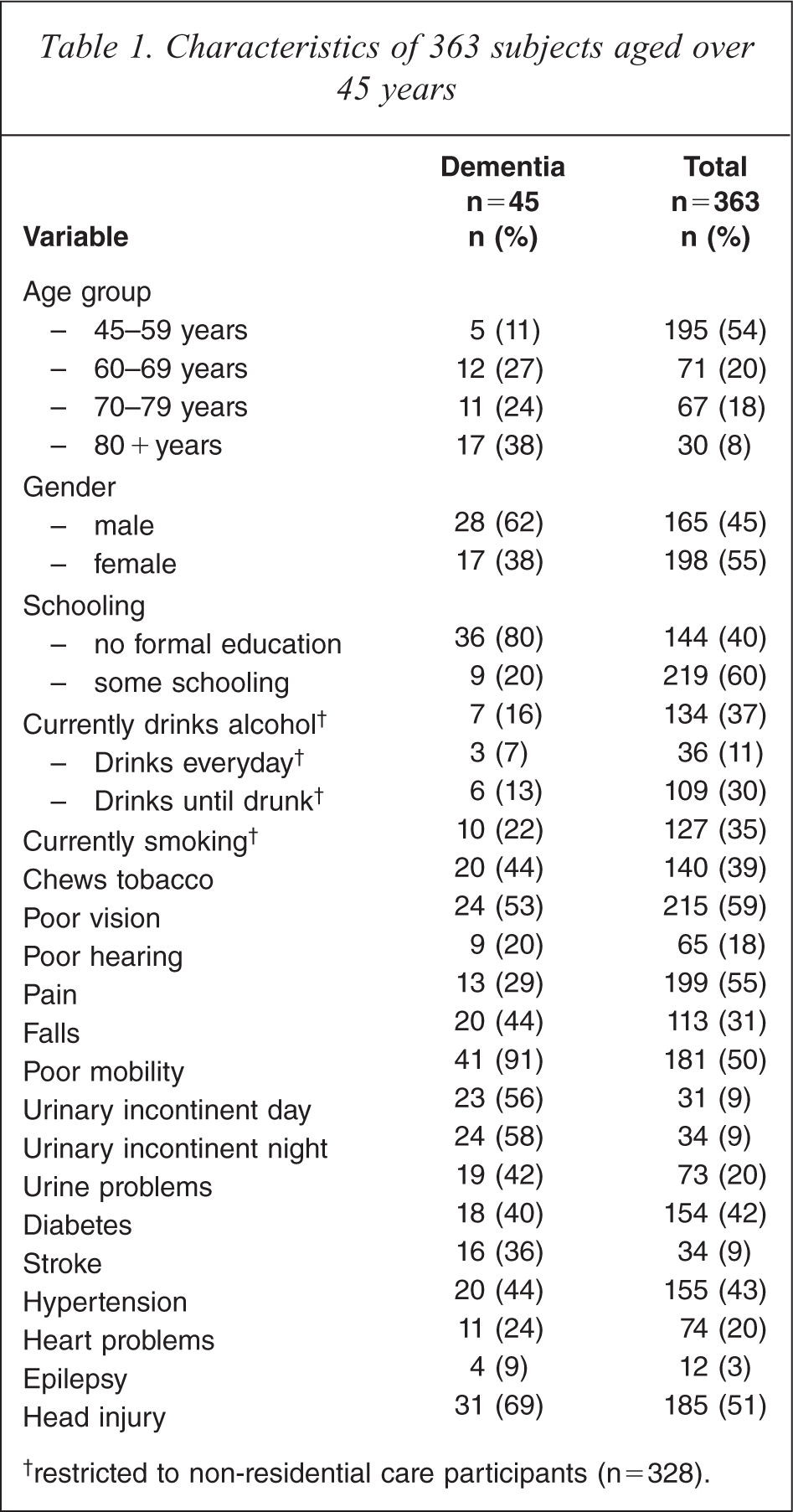
† restricted to non-residential care participants (n=328).
Demographic factors associated with dementia
Older age, male gender (OR 3.1, 95%CI 1.4, 6.8) and no formal education (OR 2.7, 95%CI 1.1, 6.7) were associated with dementia after adjusting for the other two variables (see Table 2).
Multivariate logistic regression of age group, schooling and sex against the diagnosis of dementia versus normal cognition
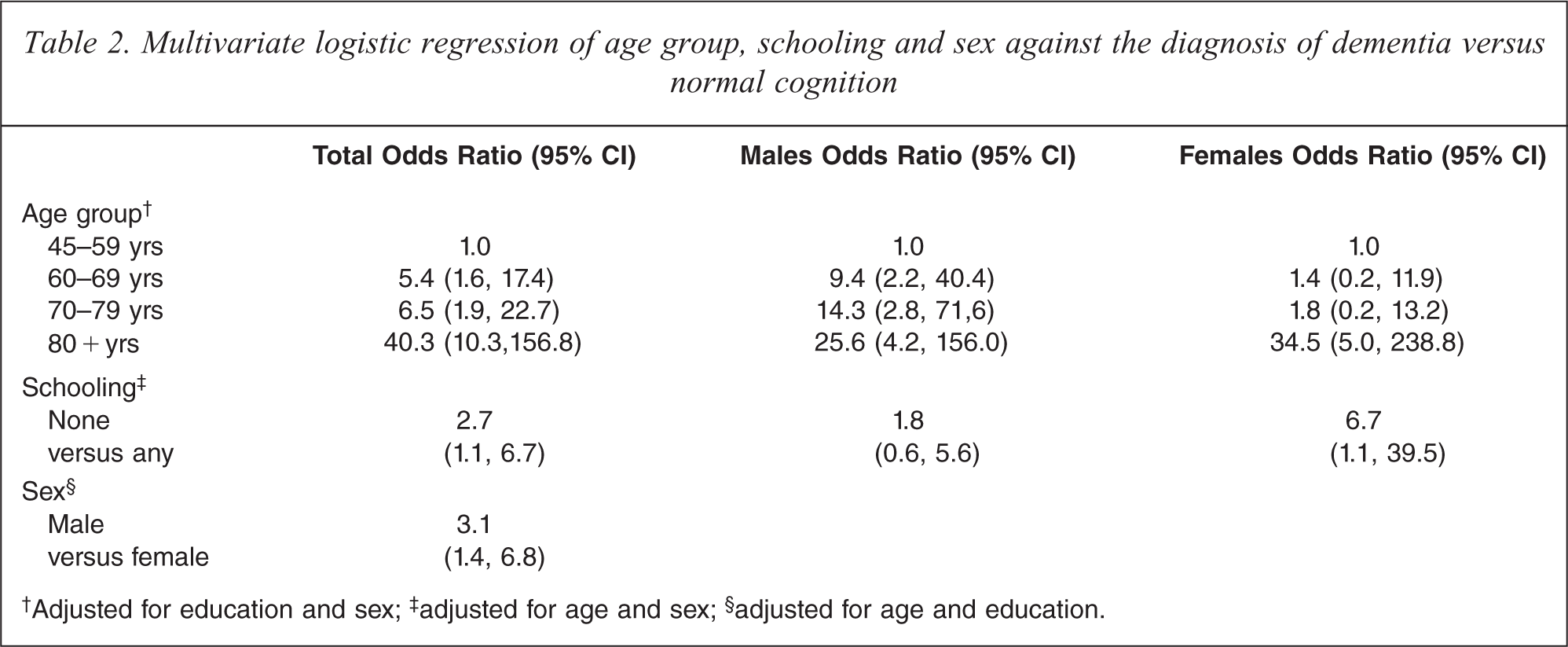
†Adjusted for education and sex; ‡ adjusted for age and sex; § adjusted for age and education.
Lifestyle and clinical factors associated with dementia
Current smoking (OR 4.5, 95%CI 1.1, 18.6), previous stroke (OR 17.9, 95%CI 5.9, 49.7), epilepsy (OR 33.5, 95%CI 4.8, 232.3) and head injury (OR 4.0, 95%CI 1.7, 9.4) were associated with dementia after adjusting for age, sex and education (see Table 3). Not surprisingly various geriatric conditions were also associated with dementia including poor mobility (OR 13.4, 95%CI 4.1, 43.9), daytime incontinence (OR 116.8, 95 %CI 21.9, 622.8), incontinence at night (OR 87.4, 95%CI 18.4, 415.7), any urinary problems (eg. urinary tract infections, incontinence) (OR 4.2, 95%CI 1.8, 10.2) and falls (OR 2.7, 95%CI 1.2, 6.1).
Factors analysed against the presence of dementia versus normal cognition (OR 95% CI) adjusted for age, sex and education
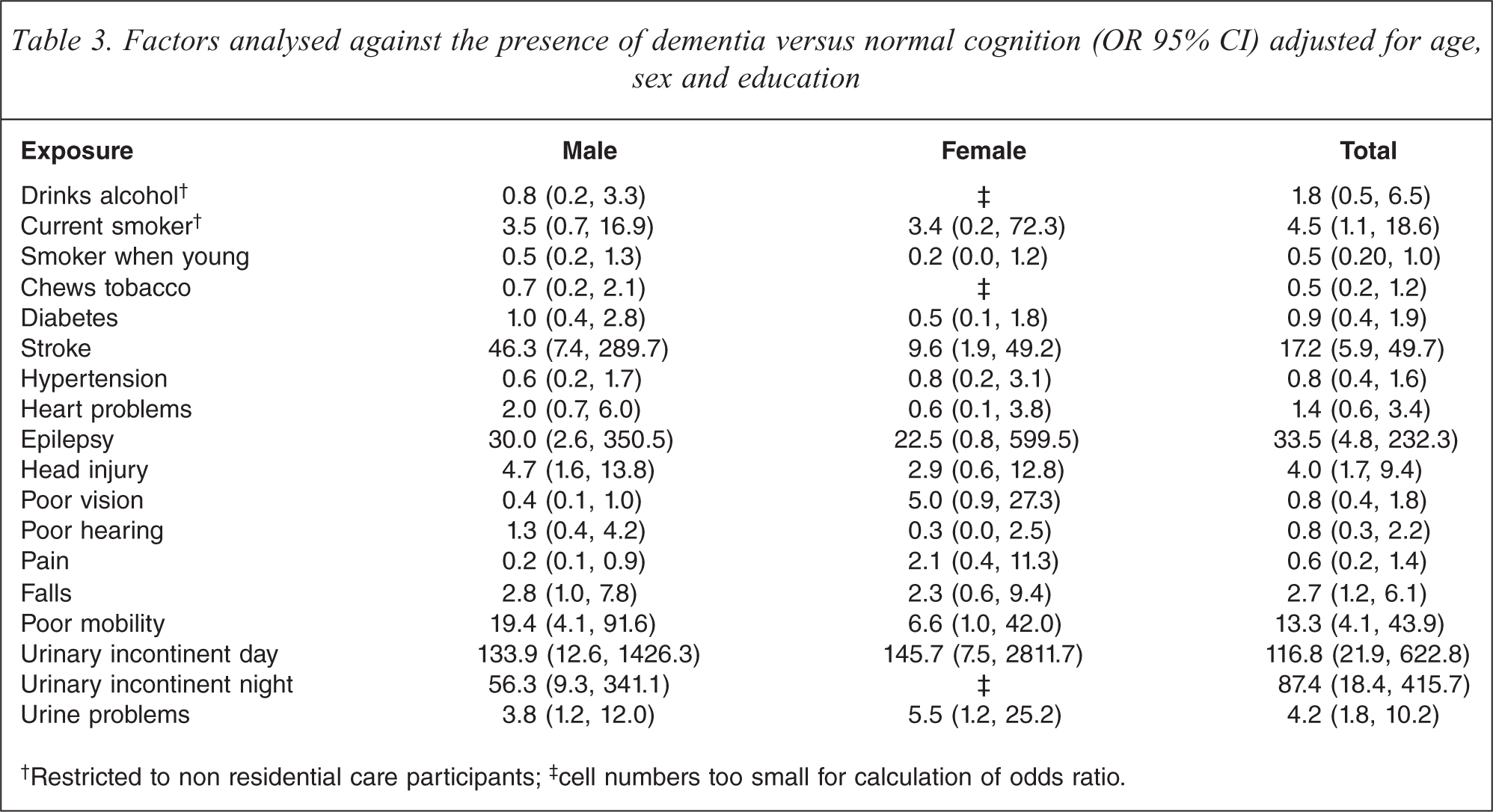
†Restricted to non residential care participants; ‡ cell numbers too small for calculation of odds ratio.
Conclusions
This study determined that older age, male gender, no formal schooling, head injury, smoking, stroke and epilepsy are associated with high rates of dementia in the Aboriginal population. Other factors that were associated with dementia include the geriatric conditions of falls, poor mobility and urinary incontinence.
No formal schooling, head injury and smoking are all potentially modifiable risk factors, where poor access to quality education, health care and employment in Aboriginal communities is resulting in this population being at substantial risk of chronic debilitating health conditions such as dementia.
The risk factors for chronic disease such as stroke are relatively poorly controlled in Aboriginal populations. Aboriginal Western Australians are 50% more likely to have a stroke recurrence than their non-Aboriginal counterparts [16]. Early management of identified stroke can reduce ongoing brain injury and potentially reduce cognitive deficits [17].
The study had some limitations. While data were collected from a number of sources, including medical records and participant and informant reports, these data only present part of the picture. Brain imaging was not accessible at the time of the study, with CT scanning not becoming available in the Kimberley region until after its completion. Medical records were only utilized as a data source for participants who qualified for the specialist review (37%). Twenty-nine potentially eligible people were not traceable at the time of specialist review. In addition, one person died prior to specialist review. The level of education was only measured as yes or no, whereas a more accurate measure of this, without relying on number use, such as whether the participant completed primary, secondary or adult education or traditional Aboriginal education would have been beneficial. The cross-sectional design made it difficult to determine whether some variables were risk factors for dementia or result from the presence of dementia. Due to a relatively limited sample size (n = 363), exposures associated with small effects could not be reliably investigated in this study.
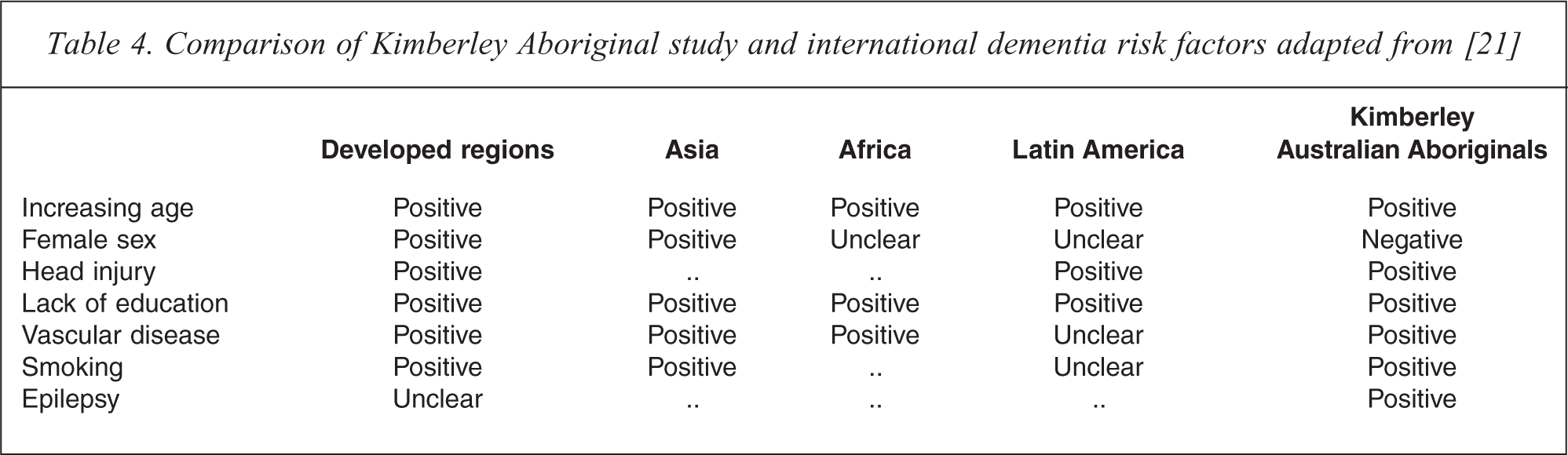
Some developing countries have a similarly high prevalence of dementia, notably Venezuela (10.3% over 65 years) [18], Argentina (12.2% over 65 years) [19] and an Arab community in Israel (21.1% over 65 years) [20]. Kalaria et al. [21] have collated a number of international studies on risk factors for dementia including these countries. The results from this Australian study have been compared to the international studies in Table 4. The factors that are associated with dementia in both this study and studies in other regions are increasing age, gender, head injury, lack of education, vascular disease and smoking. The hypothesis whereby exposure to conditions related to poverty in utero (such as poor nutrition) may lead to chronic disease in later life [22], is likely to be an underlying factor in developing countries and Aboriginal populations.
Comparison of Kimberley Aboriginal study and international dementia risk factors adapted from [21]
The burden of dementia in Aboriginal populations is substantial. Although reducing the level of morbidity to that of the general population will take multiple holistic interventions over long periods, directing services towards the prevention or better management of these known risk factors could reduce the rate of dementia in vulnerable populations.
Footnotes
Acknowledgements
Sincere thanks are extended to Kimberley Aged and Community Services, Kimberley Aboriginal Medical Services Council and the interpreters of the Kimberley Interpreting Service. Grateful assistance is acknowledged from Gordon Oscar, Edward Mungulu (named with permission from family) and Judith Brooking, Darryl Isaac, Gabriella Dolby, Brenda Green, Wayne Milgin, Kevin Nungatcha, Charlene Carrington, Laurie Churnside, Lorna Hudson, Ronald Mosquito and Melissa Sunfly who assisted with data collection, and acknowledgement of the traditional owners of Derby, Ardyaloon, Mowanjum, Looma, Junjuwa, Balgo and Warmun communities.