
Abstract
Background
Dementia is a growing global health concern, particularly among individuals with Posttraumatic Stress Disorder (PTSD), which may be a potential risk factor. However, the effects of moderating factors remain unclear.
Purpose
This study aims to assess the relationship between PTSD and dementia risk, including potential moderators.
Research design
A systematic literature review and meta-analysis were conducted in PubMed, CINAHL, PsycINFO, The Cochrane Library, and Scopus.
Data analysis
Random-effects meta-analyses were performed separately for unadjusted risk ratios (RRs) calculated from raw data and adjusted hazard ratios (HRs) reported from survival analyses. Subgroup and moderator analyses examined effects of population type, study quality, demographics, health and lifestyle factors on the PTSD-dementia association.
Study sample
Eighteen studies were included after screening 30,203 abstracts and 621 full-text articles.
Results
PTSD was associated with a 43% (unadjusted pooled RR = 1.43, 95% CI:1.09-1.89, I2 = 99.22%, P = 0.011) and 56% (adjusted pooled HR = 1.56, 95% CI:1.27-1.91, I2 = 95.50%, P < 0.001) increased dementia risk. Diabetes and hypertension strengthened the association, whereas depression, traumatic brain injury, and drinking alcohol might weaken it. However, post hoc analyses indicated that the moderation effects of depression and alcohol use were not significant after excluding one influential study. No moderating effects were found for age, gender, population type or race, and no evidence of publication bias was detected.
Conclusions
These findings confirm PTSD as a significant risk factor for dementia, with diabetes and hypertension potentially increasing vulnerability. Depression and alcohol use initially appeared to attenuate the association, but these effects were not robust in post-hoc analyses. Further research is needed to identify potential moderators and develop targeted interventions.
Introduction
Dementia is an umbrella term for disorders characterized by a decline in cognitive function beyond that expected from normal aging and is a growing public health concern globally. 1 All-cause dementia, or dementia of any type, currently affects 55 million people worldwide, a number projected to rise to 152 million by 2050 due to population aging. 1 Dementia leads to significant impairments in daily functioning and quality of life, and despite decades of research, no curative treatment is currently available, underscoring the urgency of preventive strategies and early detection.2,3 Among the various populations at risk, adults with post-traumatic stress disorder (PTSD) have emerged as a particularly vulnerable group.4,5 PTSD, a mental health condition that can develop after exposure to a potentially traumatic event, is marked by symptoms such as intrusive memories, avoidance behaviors, negative changes in thinking and mood, and heightened arousal. 6 The intersection of PTSD and dementia is an area of increasing interest and concern within the medical and psychological communities.7-9
Despite the growing interest in the relationship between PTSD and dementia, there remain significant gaps regarding the interplay of various risk and moderating factors. A previous systematic review from Günak et al 8 provided an in-depth exploration and meta-analysis of the available literature on this topic, describing the association between PTSD and all-cause dementia. Based on data from over 1.6 million individuals, results indicated that PTSD was associated with a 61% increased risk of developing dementia. This association remained after adjusting for key confounders, including depression and traumatic brain injury (TBI). Interestingly, the link between PTSD and dementia appeared to be stronger in community-based populations than among veterans, possibly reflecting differences in comorbidity profiles or healthcare access. Despite the robustness of these findings, substantial heterogeneity across studies was observed. The authors therefore emphasized the importance of longitudinal research and a more nuanced exploration of potential moderators, such as social support, lifestyle behaviors, and co-existing medical conditions like hypertension and diabetes. In the present meta-analysis, we build on and extend the work of Günak et al 8 by providing a substantial update, incorporating studies published through 2025. In contrast to Günak et al 8 who primarily focused on PTSD as a risk factor, our analysis systematically explores potential moderating variables that may influence the PTSD–dementia relationship. This approach aligns with recent developments in dementia prevention research, as highlighted in the 2024 update of the Lancet Commission report, 10 which emphasizes the importance of identifying modifiable risk factors. Moreover, we applied a broader and more rigorous screening process, and, where possible, calculated unadjusted risk ratios (RRs) from raw data in addition to extracting reported hazard ratios (HRs). This allowed for the inclusion of a greater number of studies, as some reported adjusted HRs from time-to-event models whereas others provided raw data enabling calculation of unadjusted RRs; these estimates were synthesized in separate meta-analyses rather than pooled together.
Many demographic factors and comorbid conditions are independently associated with an increased dementia risk.3,10,11 When combined with PTSD, they may strengthen this association through multiple biological and behavioral mechanisms. Several studies suggest that certain subgroups [e.g., females 12 and civilians 13 ] have an increased risk of developing dementia, highlighting potential differences in biological vulnerability or healthcare access.
Several studies have shown an association between (mid-life) diabetes mellitus and increased dementia risk, due to vascular changes that can impair cognitive function.10,14,15 And other studies highlighted the role of hypertension-related cerebrovascular dysfunction, which might contribute to dementia.3,16,17 PTSD has been associated with dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis; however, findings regarding cortisol levels are mixed, with reports of both elevated and reduced cortisol depending on sample characteristics and study design.18,19 The co-occurrence of PTSD with metabolic or vascular conditions may accelerate neurodegenerative processes and increase dementia risk beyond the effect of each condition alone. 20
Neurological and psychiatric factors commonly comorbid with PTSD might also be independently associated with dementia risk. For example, TBI has been strongly linked to neurodegenerative diseases, potentially due to blood-brain barrier disruption, neuroinflammation, and tau accumulation. 21 Additionally, depression has been associated with a 2-fold increased risk of developing dementia potentially due to its impact on brain structure and function, such as hippocampal atrophy, neuroinflammation, and disruption of stress-regulating systems.10,22,23 Conversely, depressive symptoms can be an early manifestation of dementia, particularly Alzheimer’s disease, suggesting that depression may be both a prodrome and a consequence of neurodegenerative processes.3,24-26 As both PTSD and depression are thought to share these pathways, their combination could intensify cognitive decline.
Additionally, behavioral risk factors associated with a diagnosis of PTSD such as alcohol consumption and smoking further contribute to neuronal damage and inflammation, which increases dementia risk. 27 For example, alcohol use and smoking are associated with an increased risk of vascular dementia,28,29 which highlights the role of modifiable lifestyle factors in dementia risk.
The present systematic literature review and meta-analysis aims to quantify the association between PTSD and dementia risk and identify moderators of this relationship.
Methods
Search Strategy
The literature search was conducted in PubMed, CINAHL, PsycINFO, The Cochrane Library and Scopus, and included all articles published between 1980 and December 2025. ProQuest Dissertations and Theses Global were searched for grey literature and unpublished studies. We also hand-searched the reference lists of related articles and secondary literature.
We utilized a comprehensive list of search terms (see Supplemental material) to carry out the systematic review. Titles and abstracts were independently screened by 2 reviewers (from a pool of DH, TF, ML, CR, CP, CH, SS, and KL). Reviewer pairs varied across records, and a third reviewer was available to resolve any disagreements. Full-text articles were also independently screened by 2 reviewers (from DH, TF, ML, CH, SS, and KL), with disagreements resolved by consensus or by a third reviewer. The search strategy adhered to the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) 2020 guidelines. 30 A full study protocol is available for this review and can be consulted on the PROSPERO international register of systematic reviews (Record number: CRD42019128553).
Study Selection
As the primary goal of this study was to identify possible moderators of dementia risk among adults with PTSD, we included all studies in which current PTSD symptoms in dementia cases were described. Additionally, we used the following inclusion criteria: (a) studies on adults, with an average age of ≥50 years at follow-up, who have been diagnosed with PTSD, given earlier onsets associated with some types of dementia; (b) observational longitudinal cohort studies (prospective and retrospective) with 300 or more participants; (c) randomized controlled trials (RCTs) with ≥50 participants; (d) studies published between 1980 and December 2025. We limited our search to publications in the English language and involving human subjects and excluded those that focused solely on symptoms of PTSD or dementia, rather than the full diagnosis. The study quality was evaluated using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) guidelines. 31
Data Extraction
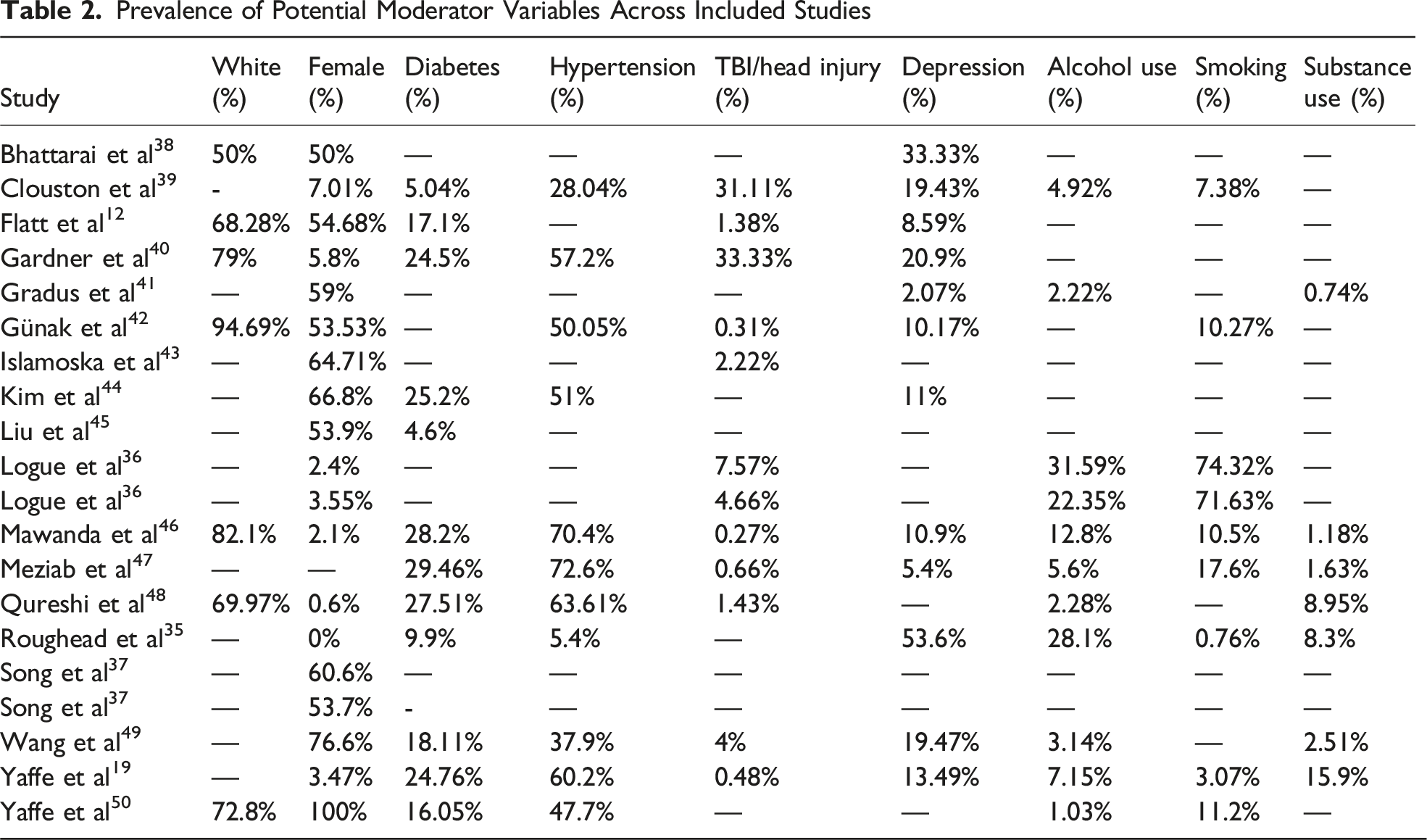
Data were extracted into evidence tables in Excel, independently by at least 2 reviewers (from DH, TF, KL). Disagreements between the 2 reviewers were resolved by consensus or by obtaining a third reviewer’s opinion should the 2 reviewers fail to reach consensus. Extracted data items included: (a) mild cognitive impairment (MCI) and dementia diagnoses; (b) assessment/diagnostic instruments used for PTSD and dementia; (c) PTSD total and symptom cluster severity scores; (d) participant characteristics such as average age, gender and race; (e) study methodology including sample size and study design; (f) potential predictor factors (e.g., diabetes, hypertension, TBI/head injury, depression, alcohol use, smoking and substance use) (g) study findings (e.g., RRs and HRs); and; (h) author conclusions. Moderator variables were extracted as study-level prevalence estimates (i.e., the percentage of participants with a given condition or reporting a given behaviour; e.g., the proportion reporting alcohol use), because more detailed operationalizations (e.g., frequency/volume/heavy use) were not consistently reported across studies.
Two reviewers (from DH, CR, or TF) independently assessed risk of bias following the recommendations from Grading of Recommendations, Assessment, Development and Evaluations. 32
Statistical Analysis
All statistical analyses were conducted using the metafor package in RStudio. 33 Two separate meta-analyses using random-effects meta-analysis with a restricted maximum-likelihood (REML) estimator were performed: one using unadjusted risk ratios (RR) based on raw data (crude associations) and one using adjusted hazard ratios (HR) as reported by studies (accounting for censoring and measured confounding). This approach was necessary as many studies reported only HRs without providing raw data for RR calculations, while others lacked time-to-event data required for HR estimation. Adjusted RRs and unadjusted HRs were not consistently available and could not be derived for most studies. Corresponding authors were contacted by email if information was missing (e.g., effect estimates or sample sizes), but either no response was received or the data were no longer available. For the RR meta-analysis, all RRs were calculated from raw event counts (a = dementia cases in the PTSD group; b = non-cases in the PTSD group; c = cases in the comparison group; d = non-cases in the comparison group), using: RR = (a/(a+b))/(c/(c+d)). All RR calculations were performed in R.”
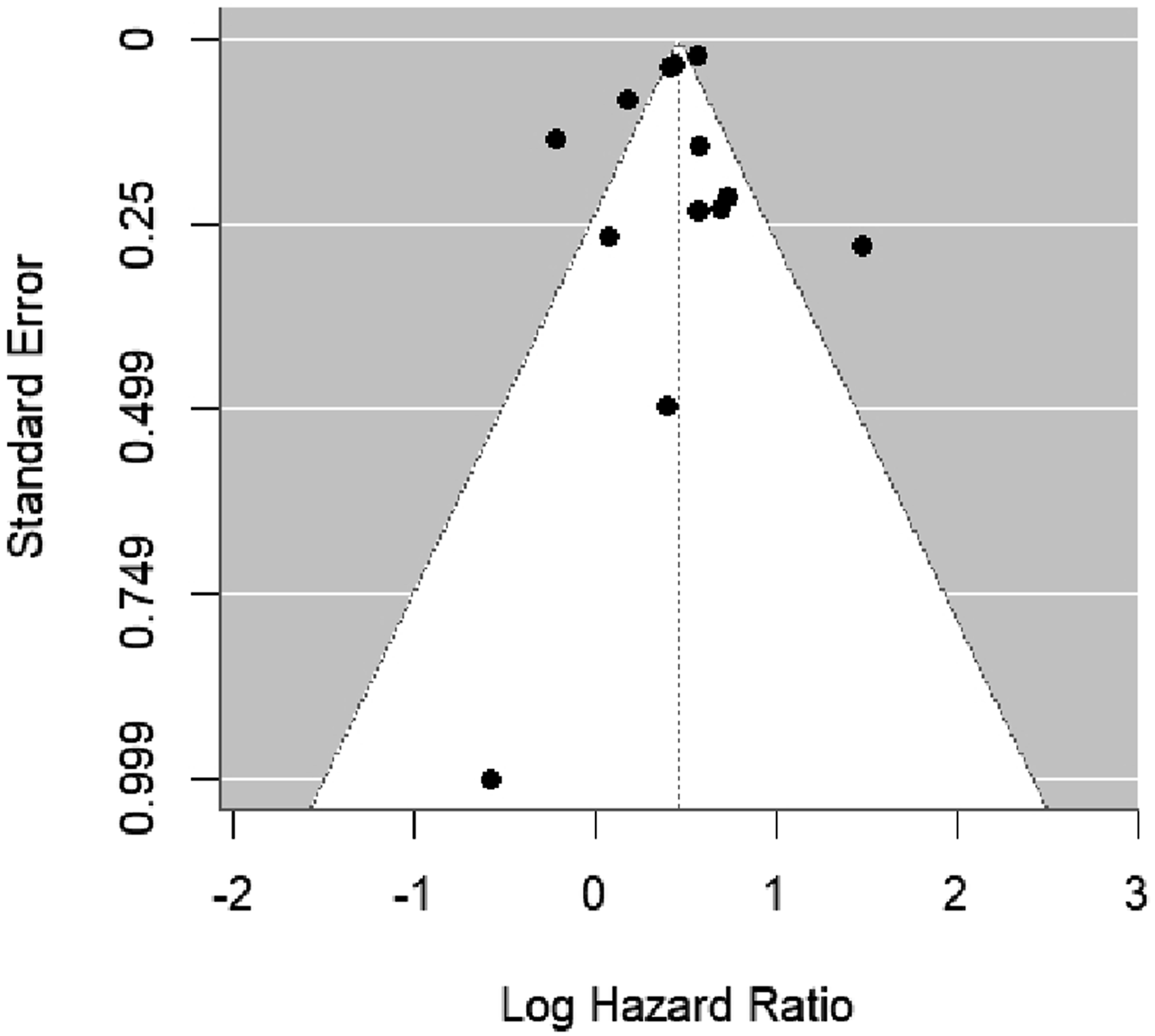
The pooled effect size with 95% confidence intervals (CI) and corresponding P-value were calculated for each analysis. Heterogeneity was assessed using Q-statistic (Q) with P-value, I2, and τ2. 34 Egger’s test was performed to evaluate publication bias (i.e., small study effects), and visual inspection of funnel plots was also conducted to assess asymmetry. Moderator analyses included regression coefficient (B) with standard error (SE), P-value, QM-statistic (df), I2, and R2 to quantify explained heterogeneity. Subgroup analyses were conducted based on population type (veterans vs general population), and a sensitivity analysis was performed to assess the impact of study quality. Meta-regression models were performed using the rma () function, testing each study-level characteristic (e.g, quality of study, age, race, gender, veteran or general population, diabetes, hypertension, TBI/head injury, depression, alcohol use, smoking and substance use) separately. For example by entering the proportion of female participants as a continuous moderator to examine its influence on the PTSD–dementia association.
To assess the robustness of significant moderator effects, post-hoc analyses were conducted in which the study by Roughead et al, 35 which reported particularly high prevalence rates of depression and alcohol use, was excluded. This allowed us to explore whether the observed moderation effects were driven by this single influential study.
Results
Study Selection and Characteristics
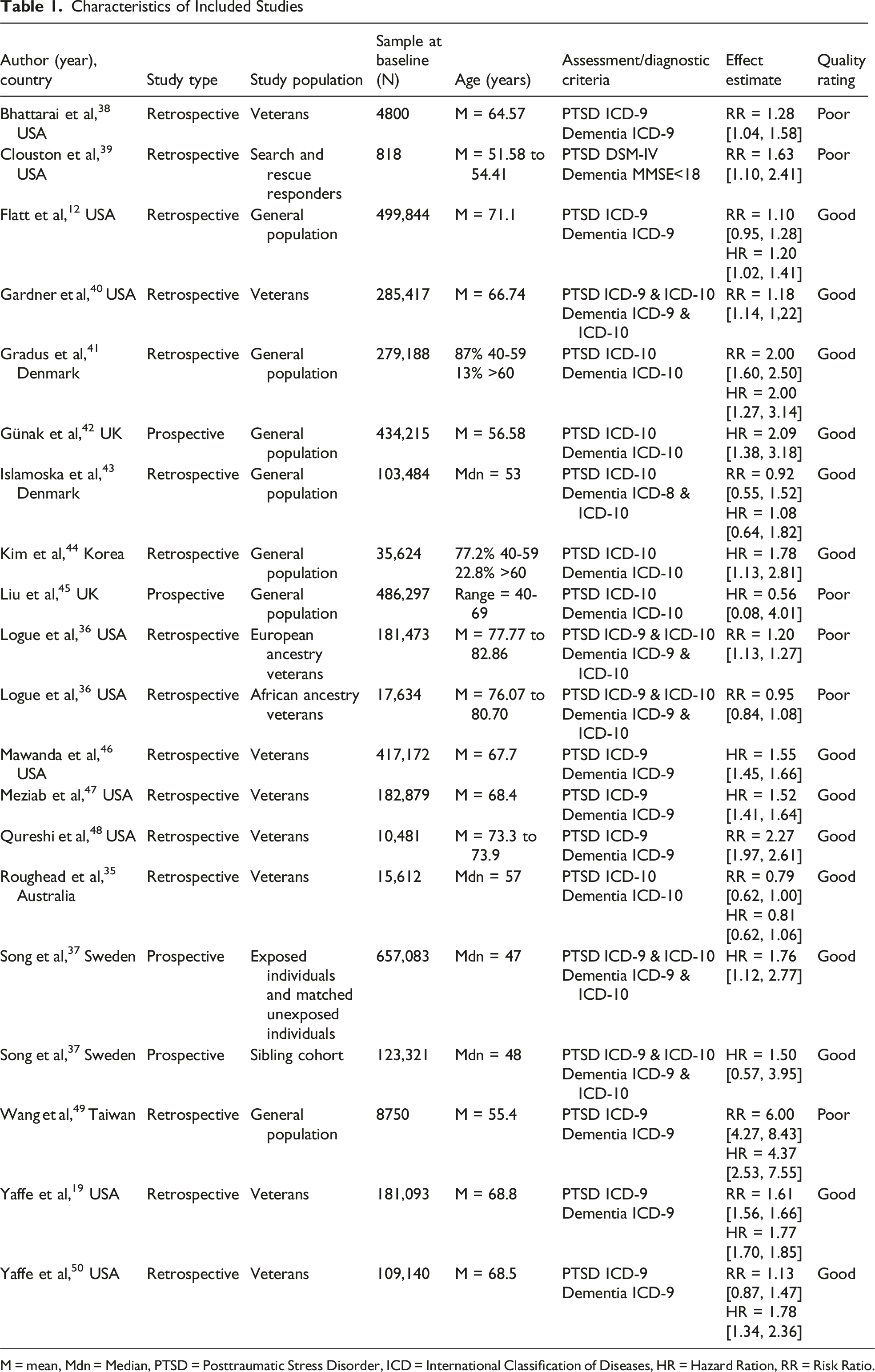
We initially identified 37,040 abstracts. After removing duplicates, we screened 30,203 records based on title and/or abstract, resulting in 621 articles eligible for full-text review. Of these, 593 records were excluded due to different reasons based on the exclusion criteria (see Figure 1), resulting in 28 studies that met inclusion criteria. All included studies were observational cohort studies; no RCT’s were identified. Of the studies that met inclusion criteria, 10 were excluded in the meta-analyses due to missing data required to calculate either a RR or a HR. Thus, a total of 18 studies that met the criteria. Additionally, 2 studies reported on 2 independent samples,36,37 which were treated as separate datasets in the analyses. In total, 13 studies provided sufficient data to be included in the unadjusted RR meta-analysis and 14 in the adjusted HR meta-analysis. Some studies contributed to both analyses, while others could only be included in one due to limitations in the reported data—such as the absence of raw data for RR calculation or a lack of time-to-event information for HR estimation. Characteristics of the included studies are presented in Tables 1 and 2. PRISMA flowchart of included studies. Characteristics of Included Studies M = mean, Mdn = Median, PTSD = Posttraumatic Stress Disorder, ICD = International Classification of Diseases, HR = Hazard Ration, RR = Risk Ratio. Prevalence of Potential Moderator Variables Across Included Studies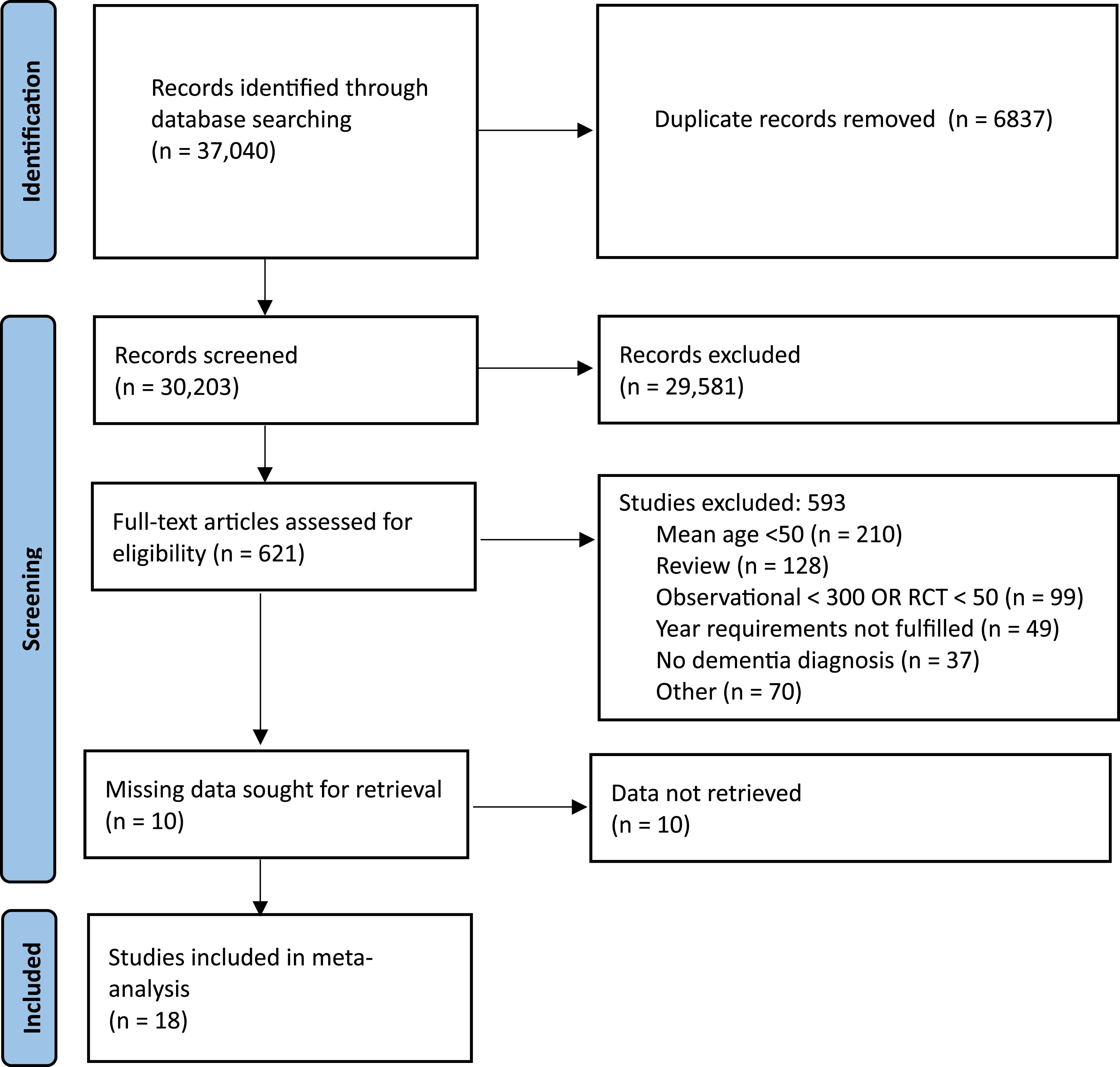
Primary Meta-Analysis of PTSD and Dementia Risk
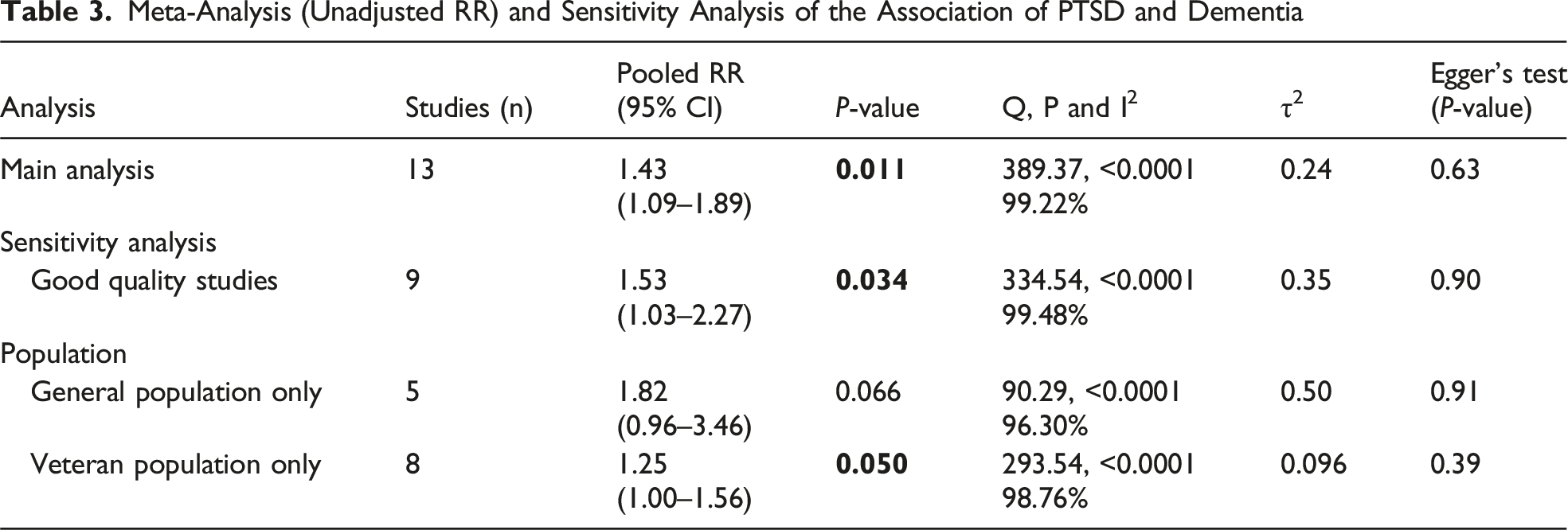
Meta-Analysis (Unadjusted RR) and Sensitivity Analysis of the Association of PTSD and Dementia
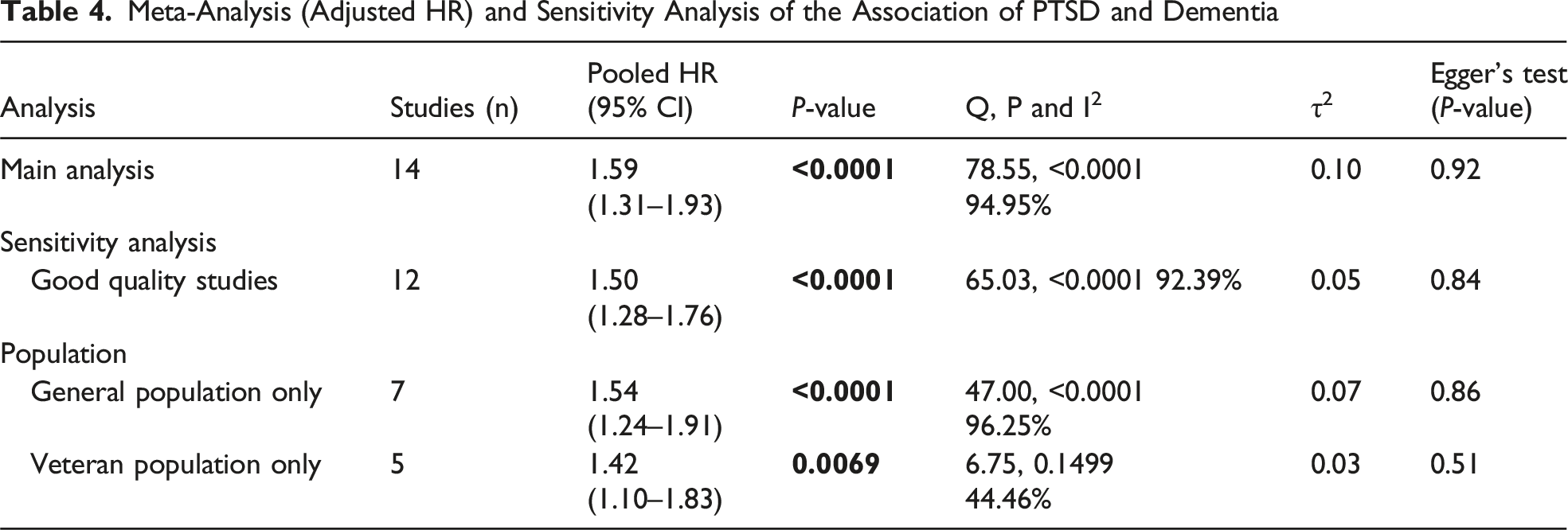
Meta-Analysis (Adjusted HR) and Sensitivity Analysis of the Association of PTSD and Dementia
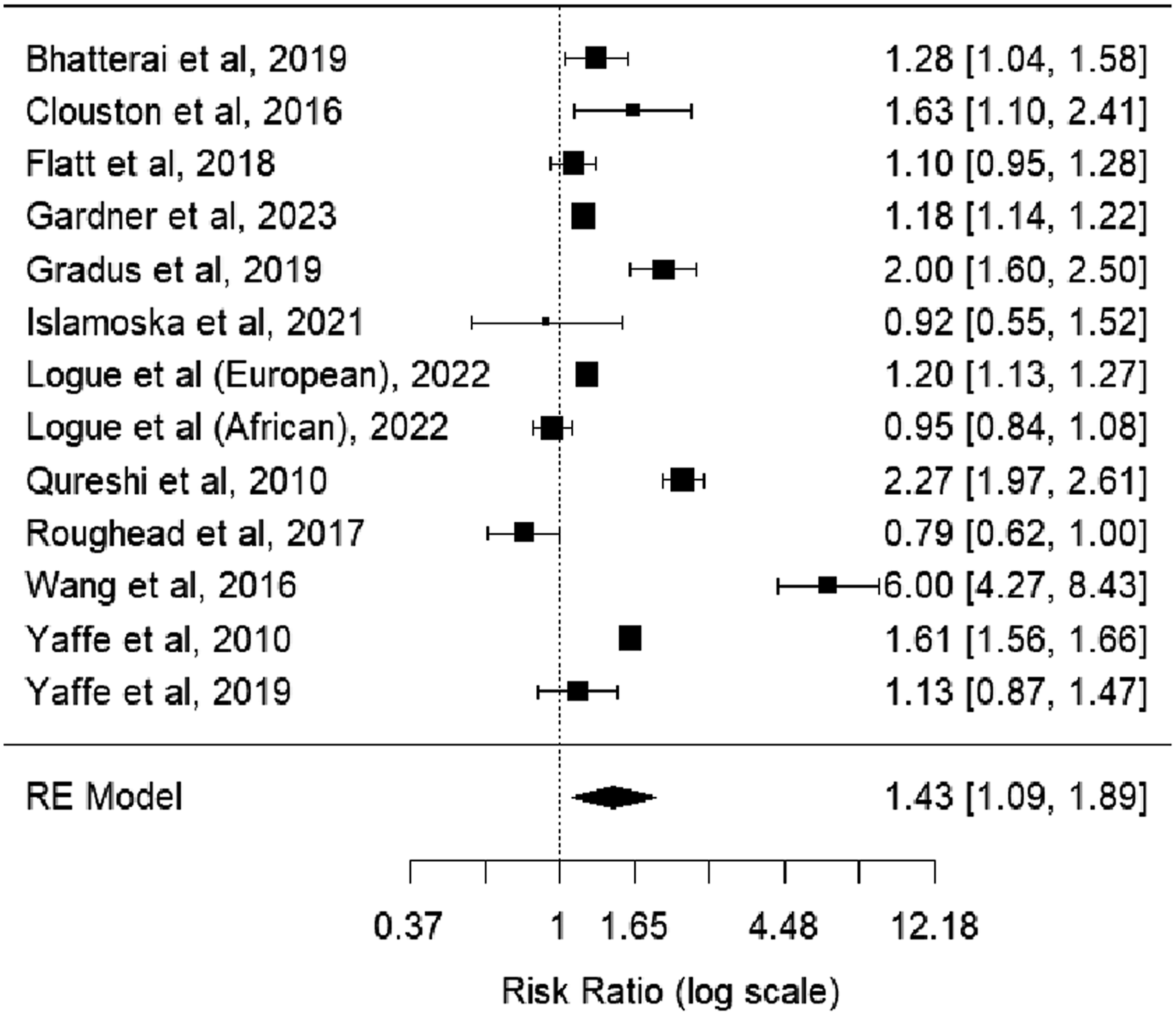
Meta-analysis of RRs of PTSD compared with no PTSD on dementia risk
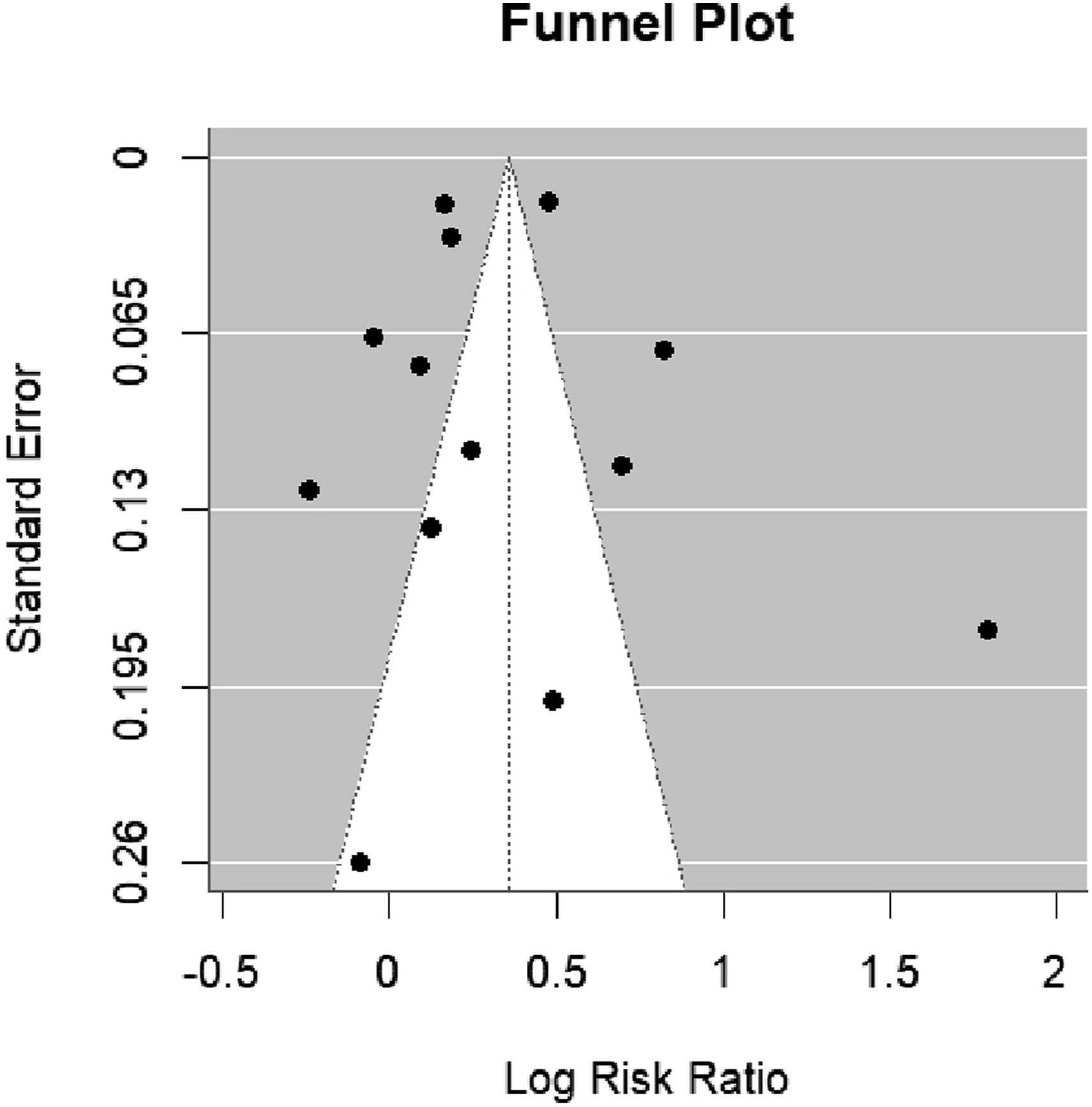
Funnel plot with pseudo 95% confidence limits to inspect publication bias
The second forest plot (Figure 4) presents a pooled adjusted HR of 1.56 (95% CI: 1.27-1.91, I2 = 95.50%, P < 0.001) for the association between PTSD and dementia. This finding suggests that individuals with PTSD have a 56% increased risk of developing dementia compared to those without PTSD. A visual inspection of the funnel plot (Figure 5) did not indicate signs of publication bias, which was further confirmed by Egger’s test (z = −0.0010, P = 0.99). Meta-analysis of HRs of PTSD compared with no PTSD on dementia risk Funnel plot with pseudo 95% confidence limits to inspect publication bias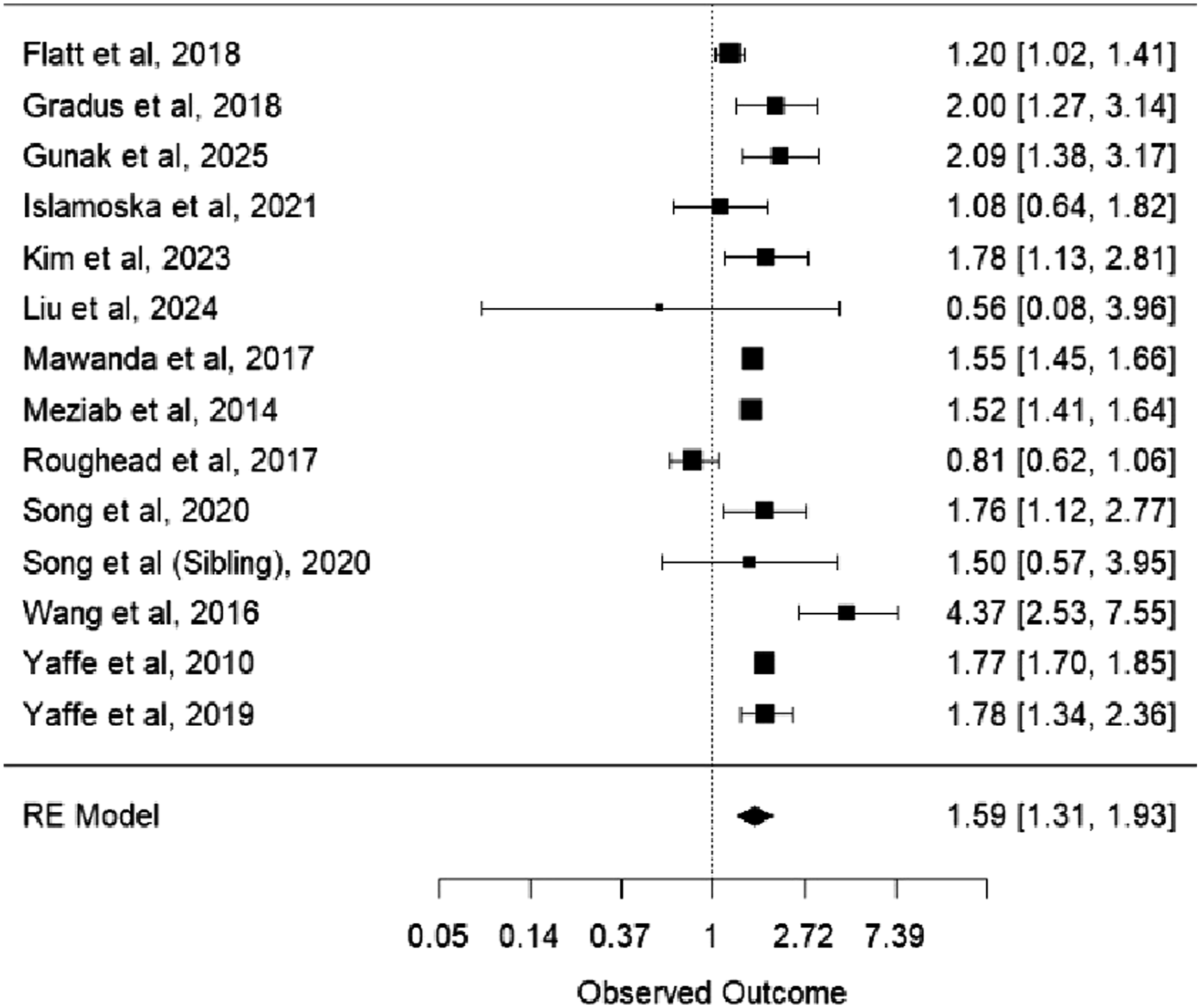
PTSD was associated with increased dementia risk in both analyses. The pooled unadjusted RR reflects crude relative risk, whereas the pooled adjusted HR reflects relative rate over follow-up time adjusted for covariates; these estimates are presented as complementary summaries and should not be interpreted as directly equivalent in magnitude.
Subgroup, Moderator, and Sensitivity Analyses
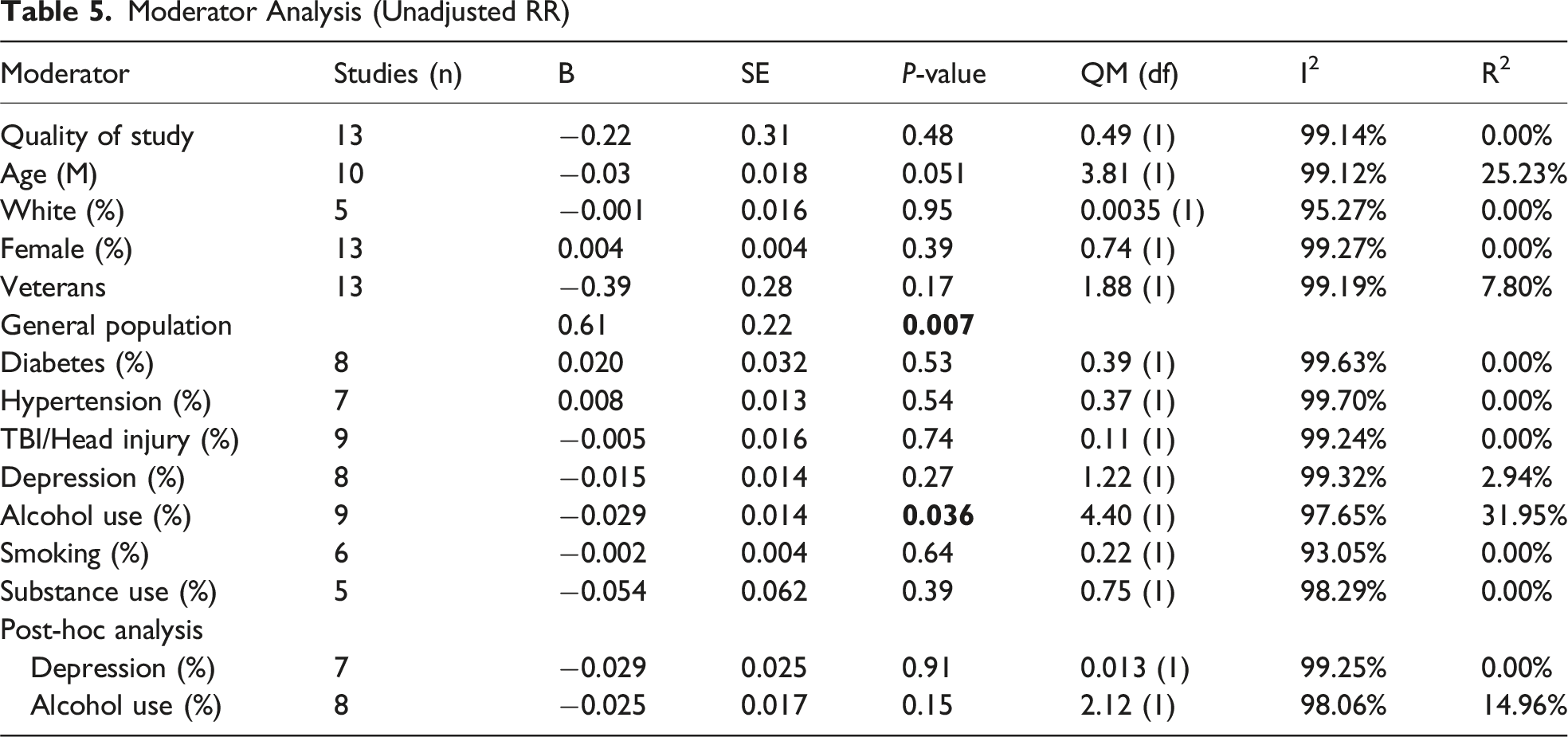
Moderator Analysis (Unadjusted RR)
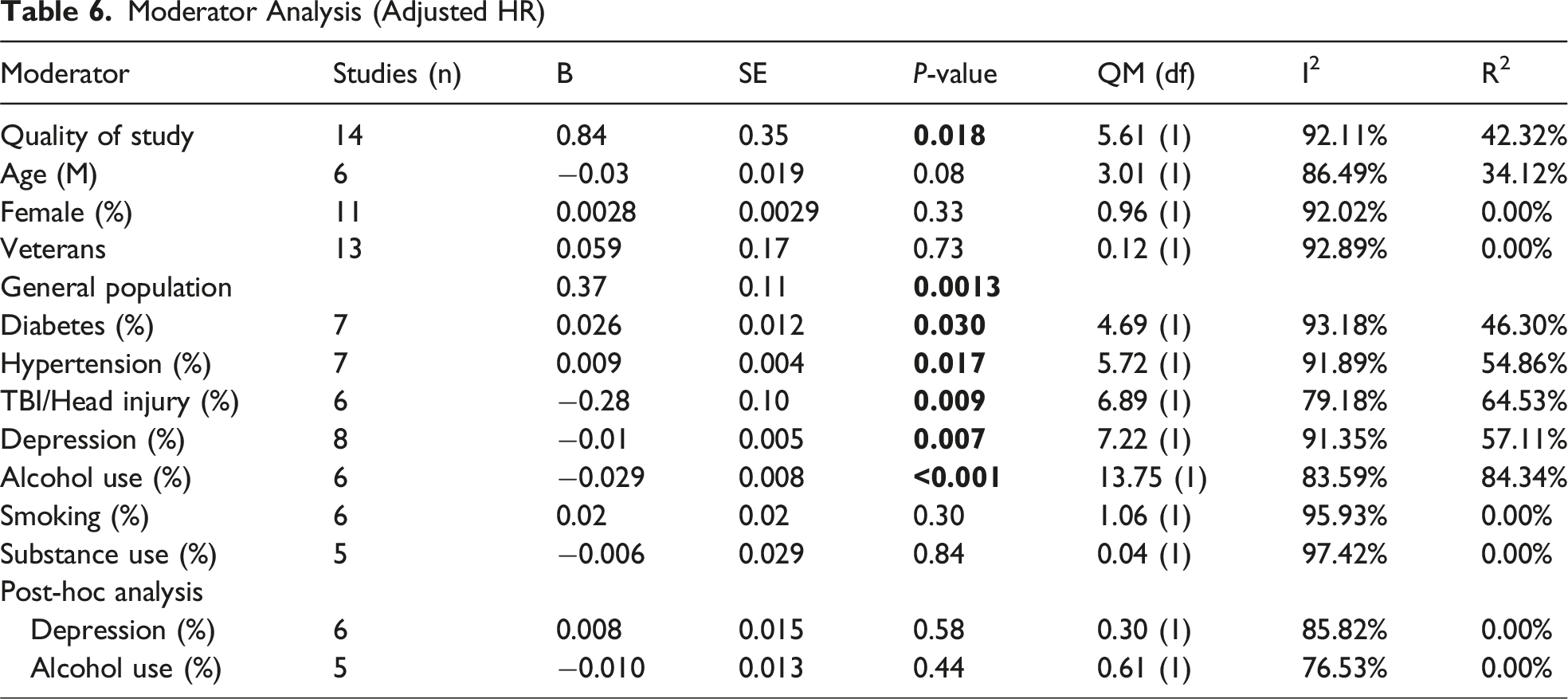
Moderator Analysis (Adjusted HR)
Study Quality
A moderator analysis was performed to formally assess whether study quality influenced effect size. The results for unadjusted RR were non-significant (B = −0.22, SE = 0.31, P = 0.483), indicating that study quality did not systematically impact the effect size. However, for adjusted HR, study quality was a significant moderator (QM(1) = 8.87, P = 0.003). We found that higher study quality was related to a stronger association between dementia and PTSD (B = 1.10, SE = 0.37, P = 0.003, I2 = 92.13%, R2 = 48.90%).
A sensitivity analysis including only high-quality studies was conducted to assess the robustness of the findings. The pooled unadjusted RR was 1.53 (95% CI: 1.03-2.27, P = 0.034), indicating a significant association. Despite this, substantial heterogeneity remained (Q (7) = 334.54, P < 0.0001, I2 = 99.48%). Similarly, the corresponding adjusted HR analysis also confirmed a significant relationship, with a pooled HR of 1.47 (95% CI: 1.25-1.73, P < 0.0001, I2 = 92.80%), suggesting that PTSD remains a significant risk factor for dementia even when lower-quality studies are excluded.
Demographic characteristics as well as several metabolic, neurological, and psychiatric conditions were assessed as potential moderators of the association between PTSD and dementia.
Demographic Factors
A moderator analysis was conducted to assess whether the mean age of study participants influenced the association between PTSD and dementia. The results were not statistically significant for either unadjusted RR (B = −0.034, SE = 0.018, P = 0.051, I2 = 99.12%, R2 = 25.23%) or adjusted HR (B = −0.083, SE = 0.052, P = 0.11, I2 = 88.64%, R2 = 25.52%). These findings suggest that age does not significantly impact effect sizes, although a trend toward weaker associations in older samples was observed.
The percentage of white participants did not significantly moderate the association between PTSD and dementia. For unadjusted RR, studies with a higher percentage of white individuals did not report significantly different effect sizes (B = −0.001, SE = 0.016, P = 0.95, I2 = 95.27%, R2 = 0.00%). Due to insufficient reporting of relevant data, this moderator could not be assessed for the adjusted HR meta-analysis.
Similarly, the percentage of female participants was not a significant moderator according to both the unadjusted RR (B = 0.004, SE = 0.004, P = 0.39) and adjusted HR (B = 0.003, SE = 0.003, P = 0.38). Therefore, study-level differences in the proportion of female participants or racial composition were not associated with differences in the strength of the PTSD–dementia association.
Finally, veteran status did not significantly influence the pooled unadjusted RR (B = −0.39, SE = 0.28, P = 0.17, I2 = 99.19%, R2 = 7.80%) or the pooled adjusted HR (QM(1) = 0.037, P = 0.84), suggesting that the effect of PTSD on dementia does not significantly differ between the veteran population or the population that are not veterans. When examining adjusted HR, veteran status was included as a moderator. The results did not significantly influence the pooled adjusted HR (QM(1) = 0.037, P = 0.84), indicating that PTSD is a significant risk factor in both populations, but the effect does not significantly differ between veterans and the general population.
Metabolic Factors
Neither diabetes nor hypertension significantly influenced the pooled unadjusted RR. However, the percentage of individuals with diabetes significantly influenced the pooled adjusted HR. Studies with a higher prevalence of diabetes reported a larger adjusted HR (B = 0.026, SE = 0.012, P = 0.03, I2 = 93.18%, R2 = 46.30%). Similarly, studies with a higher prevalence of hypertension showed a stronger relationship between PTSD and dementia (B = 0.009, SE = 0.004, P = 0.008, I2 = 91.81%, R2 = 64.33%), influencing the adjusted HR. Therefore, PTSD may have a greater impact on dementia risk among individuals with diabetes and hypertension.
Neurological and Psychiatric Factors
Neither TBI nor depression significantly influenced the pooled unadjusted RR. In contrast, studies with a higher percentage of participants with TBI or head injury reported a lower adjusted HR (B = −0.26, SE = 0.11, P = 0.015, I2 = 99.02%, R2 = 0.00%), suggesting a weaker association between PTSD and dementia in these populations.
Additionally, a higher proportion of individuals with depression was associated with a weaker relationship between PTSD and dementia (B = −0.01, SE = 0.005, P = 0.009, I2 = 92.28%, R2 = 58.08%). To assess the robustness of this finding, a post-hoc analysis was conducted, excluding the study by Roughead et al, which reported a particularly high prevalence of depression. For the RR analysis, the moderating effect of depression was already non-significant after removing Roughead et al (B = −0.015, SE = 0.014, P = 0.27). Excluding the same study from the full dataset yielded similarly non-significant results (B = −0.029, SE = 0.025, P = 0.91, I2 = 99.25%, R2 = 0.00%), suggesting that the initially observed association may have been driven largely by this single study. Similarly, the moderating effect was no longer significant for adjusted HR (B = 0.008, SE = 0.015, P = 0.58, I2 = 85.82%, R2 = 0.00%).
A moderator analysis of alcohol use revealed significant moderation effects for both unadjusted RR and adjusted HR. Alcohol use significantly influenced the pooled unadjusted RR, with studies including a higher percentage of participants consuming alcohol reporting lower RRs (B = −0.0293, SE = 0.010, P = 0.036). Similarly, for adjusted HR, studies including a higher percentage of participants consuming alcohol reporting lower HRs (B = −0.029, SE = 0.008, P < 0.001, I2 = 97.65%, R2 = 31.95%). To further explore the robustness of this finding, a post-hoc analysis was conducted in which the study by Roughead et al was excluded due to its relatively high alcohol use prevalence and potential influence on the model. After exclusion, the moderating effect of alcohol use was no longer statistically significant for either unadjusted RR (B = −0.025, SE = 0.017, P = 0.15, I2 = 98.06%, R2 = 14.96%) or adjusted HR (B = −0.010, SE = 0.013, P = 0.44, I2 = 76.53%, R2 = 0.00%). This suggests that the initial effect may have been partially driven by the inclusion of this single study and should be interpreted with caution.
For smoking and substance use, neither RR nor HR analyses revealed a significant moderation effect, indicating that these factors did not contribute to heterogeneity in effect sizes across studies.
Discussion
The present meta-analysis provides further insights into the association between PTSD and dementia, highlighting the role of potential moderators of this relationship. Consistent with a previous meta-analysis, 8 our findings confirm that PTSD is a significant risk factor for dementia, with individuals showing a 43% increased risk based on unadjusted RRs and a 59% increased risk based on adjusted HRs. However, the strength of this association appears to be influenced by various metabolic, neurological, and psychiatric comorbidities. Some reported health conditions, such as diabetes and hypertension, intensified the observed association between PTSD and dementia; others, such as TBI, depression and alcohol use, weakened the association. Post hoc analyses further revealed that these moderation effects were not always consistent across studies. Specifically, the significant moderating effects of depression and alcohol use on the adjusted HRs became non-significant when one particular study was removed, 35 suggesting that the strength of these associations may be driven by one individual study. This highlights the need for cautious interpretation and replication in future research.
Compared with the previous meta-analysis by Günak et al, 8 which reported an overall increased dementia risk among individuals with PTSD (pooled estimate approximately HR = 1.61), our updated analyses likewise indicate an elevated risk (adjusted pooled HR = 1.59; unadjusted pooled RR = 1.43). While the direction and magnitude are broadly consistent, the present review extends prior work by incorporating newly published cohorts and by systematically exploring a wider range of potential study-level moderators and sensitivity analyses. These moderator findings should be interpreted cautiously, as they reflect between-study differences in reported prevalences rather than individual-level effect modification.
Our results showed that the association between PTSD and dementia was stronger in studies with a higher prevalence of comorbid diabetes, suggesting that metabolic dysfunction may amplify neurodegenerative risk. 51 Diabetes is well-established as a risk factor for both vascular dementia and Alzheimer’s disease due to its role in promoting insulin resistance, microvascular damage, and neuroinflammation.10,14,15 However, PTSD may also be a risk factor for diabetes. PTSD has been linked to chronic dysregulation of the HPA axis and altered cortisol regulation; however, the direction of cortisol changes is not uniform across studies. 52 HPA-axis dysregulation has been associated with immune and inflammatory changes, 53 which may increase the risk of diabetes. 54 From this perspective, physiological abnormalities in the HPA axis, changes in metabolic hormones, and lifestyle factors may help explain associations between PTSD and diabetes. 55 Thus, PTSD and diabetes may co-occur and contribute to increased metabolic burden, which could be relevant for dementia risk.
Similarly, hypertension is known to increase the risk of cognitive decline by making blood vessels stiffer, reducing blood flow to the brain, and weakening the blood-brain barrier.3,16,17 PTSD might further contribute to this problem by causing an overactive stress response, which raises blood pressure and puts extra strain on the brain’s blood vessels. 56 Over time, stress-related high blood pressure can lead to small, unnoticed strokes, damage to brain tissue, and reduced oxygen supply to certain areas of the brain, which increase the dementia risk. 57 Indeed, a diagnosis of PTSD is associated with a 94% increased risk of hypertension incidence. 56 The combination of PTSD and hypertension may amplify vascular damage, speeding up cognitive decline that could lead to dementia.
Although metabolic conditions strengthened the association between PTSD and dementia, TBI or head injury appeared to weaken the association despite TBI on its own increases dementia risk. 21 One possible reason is that some symptoms of PTSD after a brain injury may actually be caused by TBI-related cognitive issues rather than PTSD itself. This overlap makes it more difficult to distinguish the specific effects of PTSD and TBI in dementia research.
Likewise, moderation by depression was associated with a weaker association between PTSD and dementia. This finding is particularly intriguing given that depression itself is a well-documented risk factor for dementia.10,22,23,58 Both PTSD and depression are linked to overlapping neurobiological mechanisms, including chronic stress, inflammation, hippocampal atrophy, and HPA-axis dysregulation, that have all been implicated in cognitive decline and dementia development.3,26 It is possible that when these pathways are already activated by depression, the additional impact of PTSD may be less detectable, effectively “tapping” the same vulnerability pathways.
Importantly, post hoc analyses suggested that this moderation effect may have been driven by a single study with unusually high depression rates. The influence of this study highlights how variability in study populations—such as clinical vs community samples—can shape pooled outcomes and suggests that future research should carefully consider the context and measurement of comorbid conditions. Additionally, our analysis did not distinguish between early-and late-onset depression. Prior literature indicates that late-onset depression, often linked to vascular pathology or prodromal dementia, may carry different implications for dementia risk than early-onset forms.3,24,25 Without detailed onset data or survival analyses, we are limited in interpreting these trajectories. As such, while our findings point to a potentially attenuating role of depression, this observation should be interpreted with caution and warrants further investigation in more finely stratified samples.
The finding that a higher prevalence of people who drink alcohol was associated with a weaker PTSD-dementia relationship appears counterintuitive. An extensive body of literature links alcohol consumption, regardless of amount, to adverse health outcomes, including neurodegeneration and increased dementia risk.28,29,59,60 Recent studies have challenged earlier suggestions of a protective effect of light-to-moderate alcohol intake, instead emphasizing that even low levels of consumption are associated with increased risks of cancer, cognitive decline, and dementia.61-64
Since we used aggregated study data rather than individual-level data, the results reflect group-level trends. Thus, moderation effects do not show direct causal links but suggest that the strength of the PTSD–dementia association may vary depending on background levels of certain characteristics. Nonetheless, the association observed in our data warrants further exploration. One possible explanation may lie in the role of alcohol as a form of self-medication among individuals with PTSD. 65 Alcohol and other substances are often used to manage hyperarousal and emotional distress, core symptoms of PTSD, which could confound the observed relationship between trauma exposure, substance use, and cognitive outcomes.66,67 Indeed, research has shown that reductions in PTSD symptoms are frequently accompanied by declines in substance and alcohol use, suggesting a dynamic, bidirectional interplay between trauma-related distress and coping behavior. 66
Another explanation may relate to sample composition. Post-hoc analyses indicated that the found moderation effect was largely driven by one particular study with notably high alcohol use prevalence. 35 It is possible that in such populations, higher rates of severe alcohol use may lead to increased early mortality, thereby reducing the number of individuals surviving to old age when dementia risk becomes apparent. 68 This form of survivor bias could partially account for the observed decrease in dementia risk in studies with higher alcohol use.
Taken together, while our findings suggest a statistically significant moderating effect of alcohol use on the PTSD–dementia association, this should be interpreted with caution. It is important to underscore that these results do not support any protective effect of alcohol. Rather, they point to the complex and potentially confounded nature of alcohol use within PTSD populations and the need for further research to disentangle potential moderators and underlying mechanisms.
Limitations
This review has several limitations. A key limitation is that available studies reported different effect measures and adjustment sets; therefore, we synthesized unadjusted RRs and adjusted HRs in separate meta-analyses. Differences in confounder control and time-to-event modelling may contribute to heterogeneity, and direct comparability of effect magnitude across RR and HR analyses is limited. Another limitation is that the second meta-analysis relied on unadjusted RRs. This is problematic because unadjusted estimates do not account for confounding factors such as age, sex, comorbidities, or lifestyle behaviors. As a result, the associations between several moderators, PTSD and dementia may be overestimated or underestimated, reducing the reliability of the conclusions. Besides, although we assessed small-study effects using funnel plots and Egger’s test, these methods have limited power when the number of included studies is small. As a result, absence of evidence for small-study effects should not be interpreted as evidence of absence. Another limitation is the substantial statistical heterogeneity among studies, which persisted even after conducting multiple subgroup and sensitivity analyses. While efforts were made to explore potential sources of heterogeneity, it remained high, suggesting that unmeasured differences between studies, such as variations in sample characteristics or study methodologies, may have influenced the findings. Additionally, most included studies were observational cohort studies, with many using a retrospective design. Since observational studies cannot establish causality, and retrospective designs are prone to biases and incomplete data, the findings should be interpreted with caution. Another potential limitation is the variability in PTSD assessment across studies, with many instruments lacking validated diagnostic accuracy in older adults or those with cognitive impairment. As shown by Havermans et al, 69 this may have led to misclassification, affecting the observed associations. Finally, several moderator analyses were based on a limited number of studies, which may compromise the statistical power and increase the likelihood of false-positive or false-negative results. Larger and more diverse samples should be used to confirm these findings to strengthen future research.
Conclusion
This meta-analysis confirm that PTSD significantly increases dementia risk, with affected individuals having approximately one and a half times the risk compared to those without PTSD. These findings support previous research and add new insights by identifying factors that may influence this relationship. Diabetes and hypertension appear to be associated with increased dementia risk in the context of PTSD. In contrast, TBI, depression and alcohol use initially appeared to attenuate the link between PTSD and dementia. Post hoc analyses further suggested that these moderation effects were largely driven by a single influential study. This may reflect overlapping mechanisms with PTSD, sample-specific factors, or measurement issues. More long-term studies, biomarker research, and clinical trials are needed to understand how PTSD leads to dementia. From a clincial perspective, these findings highlight the importance of early screening and managing PTSD and related health conditions. Future research is needed to determine whether interventions targeting metabolic or cardiovascular health, and/or evidence-based treatment of PTSD, may reduce dementia risk among individuals with PTSD.
Supplemental Material
Supplemental Material - The Role of Posttraumatic Stress Disorder as a Risk Factor for Dementia: A Meta-Analysis
Supplemental Material for The Role of Posttraumatic Stress Disorder as a Risk Factor for Dementia: A Meta-Analysis by D. C. D. Havermans, C. M. Hoeboer, T. M. Farrell, C. S. Rippey, C. N. Pinheiro, S. Sobczak, M. Olff, S. Henderson, K. Deckers, K. A. Lawrence in Journal of Geriatric Psychiatry and Neurology.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is partially sponsored by a K01AG070279 awarded to K.A. Lawrence from the National Institute on Aging (NIA) at the National Institutes of Health (NIH). This content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH’s NIA. The data have not been previously presented orally or by poster at scientific meetings.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.