
Abstract
The association between smoking and common mental disorders is well known. The National Comorbidity Survey conducted in the United States between 1990 and 1992 found that adults who met DSM-III-R criteria for mental illnesses in the month prior to the survey consumed an estimated 44% of cigarettes smoked by adults in the United States [1]. The 1997 Australian National Survey of Mental Health and Wellbeing found that adults with a 12-month mental disorder smoked at about twice the rate of adults without a mental disorder, and represented 30% of all adult smokers [2,3]. The 2007 Australian National Survey of Mental Health and Wellbeing (NSMHWB) found that adults who met the lifetime criteria for mental disorders and who experienced symptoms in the 12 months prior to the survey represented 32% of all adult smokers [4]. Overall, the 12-month prevalence of mental disorder was 20%, with anxiety disorders representing the most commonly occurring category of disorders with a prevalence of 14.4% [5,6].
Despite knowledge of this strong association, little attention has been paid to the role of common mental disorders in tobacco control policies and programmes. The draft national strategy prepared by the National Preventative Health Taskforce in 2008 [7] identified a number of groups requiring tailored messages and services including Aboriginal and Torres Strait Islander Australians, people from non-English speaking backgrounds, prisoners, patients of mental health services, and residents of highly disadvantaged neighbourhoods. However, the taskforce argued that people with common mental health problems (as distinct from severe mental illness) would benefit equally from broad population-based programmes. Leaders in tobacco control have argued that common mental disorders such as anxiety disorders and affective disorders do not warrant special strategies for several reasons: the majority of these disorders are mild and do not require hospital-based treatment or qualify the sufferer for a disability pension; the majority of these disorders are short-term and transient in nature and have little impact on long-term risk behaviours such as smoking; and apart from severe cases, people with common mental disorders are equally likely to benefit from population-based anti-smoking strategies such as price controls, sale and advertising restrictions, advertising of health risks, and denormalization of smoking behaviour [7–9].
To investigate if these contentions are supported by data, we set out to test the following null hypotheses using data from the 2007 NSMHWB:
People with anxiety disorders of mild or moderate severity smoke at the same rate as the general population. The majority of anxiety disorders will be of short duration and these disorders will not impact on smoking behavior. People with anxiety disorders of mild or moderate severity will quit smoking at the same rate as the general population.
Method
Data source
Data for this study were taken from the Australian National Survey of Mental Health and Wellbeing (NSMHWB). This survey was conducted by the Australian Bureau of Statistics (ABS) with funding from the Commonwealth Department of Health and Ageing. A confidentialized unit record file was obtained from the ABS. The survey comprised a nationally representative sample of 8841 participating adults aged 16–85 years living in private dwellings, representing a response rate of 60%. Fieldwork was conducted between August and December 2007. The survey sample was drawn using a stratified multi-stage area-based design. Data collection was undertaken by means of computer-assisted personal interviewing. Full details of the survey methodology have been published previously [10–12].
Measures
The NSMHWB measured the prevalence of three major groups of disorders — anxiety disorder, affective disorders and substance use disorders — using Version 3 of the Composite International Diagnostic Interview (CIDI) [13]. The CIDI assesses disorders using both ICD-10 and DSM-IV criteria. For this study, ICD-10 criteria have been used [14].
Anxiety disorders
We focused on adults with anxiety disorders because this is the most prevalent group of disorders in Australia. Six anxiety disorders were assessed in the NSMHWB using the CIDI: panic disorder, agoraphobia, social phobia, generalized anxiety disorder, obsessive-compulsive disorder and post-traumatic stress disorder. Adults were identified as having 12-month mental disorders if they met the criteria for the disorder within their lifetime, and experienced symptoms in the 12 months prior to the survey. To assess post-traumatic stress disorder, the respondent is questioned about a series of around 30 types of stressful events of threatening or catastrophic nature. Respondents who have experienced one or more such events are asked about distress, symptoms such as hypervigilance, hyperarousal, and insomnia, and avoidance behaviours to form a diagnosis. Respondents who experienced more than one event were asked to report which event caused them the most problems. This was used to identify the worst traumatic event experienced.
Smoking status
Respondents were asked “do you currently smoke every day, at least weekly, less than weekly, or not at all?” While the wording of the question is not specifically limited to cigarettes, the interviewers’ instructions and further questions in the series specifically refer to cigarette smoking. Respondents were classified as current smokers if they smoked daily or less than daily, and classified as daily smokers if they smoked daily. Daily smokers were asked “at what age did you start smoking every day?”. Respondents who were not daily smokers were asked “Have you ever smoked every day?”. All respondents who had ever smoked daily were asked “At what age did you start smoking every day?”. Respondents who were not current daily smokers were asked “at what age did you stop smoking every day?”. These data were used to calculate number of years that the respondent had smoked daily.
Severity of mental illness
Severity was measured using the World Mental Health Survey Initiative severity measure, which summarizes the impact of mental disorders experienced in the previous 12 months as mild, moderate or severe [11,13]. Mental illness was classified as severe if during the 12 months prior to the survey there was either an attempted suicide, an episode of mania, severe role impairment experienced in at least two domains on the Sheehan disability scales or overall functional impairment was assessed as equivalent to a Global Assessment of Functioning score of 50 or less.
Time since first onset of symptoms
The time since first onset of symptoms was derived from the reported age of onset of relevant symptoms.
Use of services
Respondents were given the definition “The next few questions are about problems with your mental health. This includes but is not restricted to such things as stress, anxiety, depression or dependence on alcohol or drugs.” Respondents were then asked how often they accessed the following health services for problems with their mental health in the 12 months prior to the survey: general practitioner, psychiatrist, psychologist, mental health nurse or other professional providing specialist mental health services, or other health professional including medical specialist, other professional providing general services or complementary and alternative therapist.
Data analysis
Weighted estimates and confidence intervals
Survey weights were applied to calculate estimates of totals and proportions. As the survey used a complex sampling design including stratification and area-based clustering, the sample design needed to be accounted for to calculate correct confidence intervals for estimates from the survey data. Standard errors and confidence intervals for the NSMHWB were calculated using the jack-knife method of replicate weighting [15]. Prevalence of anxiety disorders were calculated by disorder type, severity, years since onset of symptoms, and use of services. Within each category estimated proportions of current and daily smokers were calculated. For comparison, a control group consisting of those adults who have no lifetime history of mental disorder was used.
Smoking cessation
The reported ages of first and last daily smoking and current daily smoking were used to estimate relative risk of smoking cessation comparing adults with 12-month anxiety disorders to adults who have no lifetime history of mental disorder. As these data take the form of censored time-to-event data, from time first smoked, survival analysis methods were employed. Time to smoking cessation was calculated from age of first and last daily smoking for ex-smokers, and was censored at time of the survey for current smokers. Kaplan-Meier life table methods were used to estimate survival curves for smoking cessation status for the two groups, and to calculate median duration of daily smoking. We used proportional hazards regression to test for statistical significance between the two groups. Four additional models were fit to examine relative risk for smoking cessation by type, severity and duration of anxiety disorder and service use. Each model also adjusted for sex and age of the respondent at the time of the survey. As the association with age will not necessarily be linear, especially as proportional hazards regression models the log of the hazard ratio, we fitted a fractional polynomial in age [16].
Because this cohort is retrospectively determined from a cross-sectional survey rather than obtained from longitudinal follow-up, there is no chance for people who have died to be represented in the cohort, as they could not be selected in the survey. To avoid bias due to differential rate of deaths caused by smoking, the survival analyses have been limited to adults aged 45 years or less at the time of the survey. As reported by Doll et al. [17], almost all smoking related deaths occur after 45 years of age and there is no observable difference in mortality curves between smokers and non-smokers before age 45 years. This also has the advantage of limiting response bias that may be caused by older respondents not reporting shorter periods of daily smoking many years prior to the survey.
All analyses were undertaken using SAS software version 9.2 [18].
Results
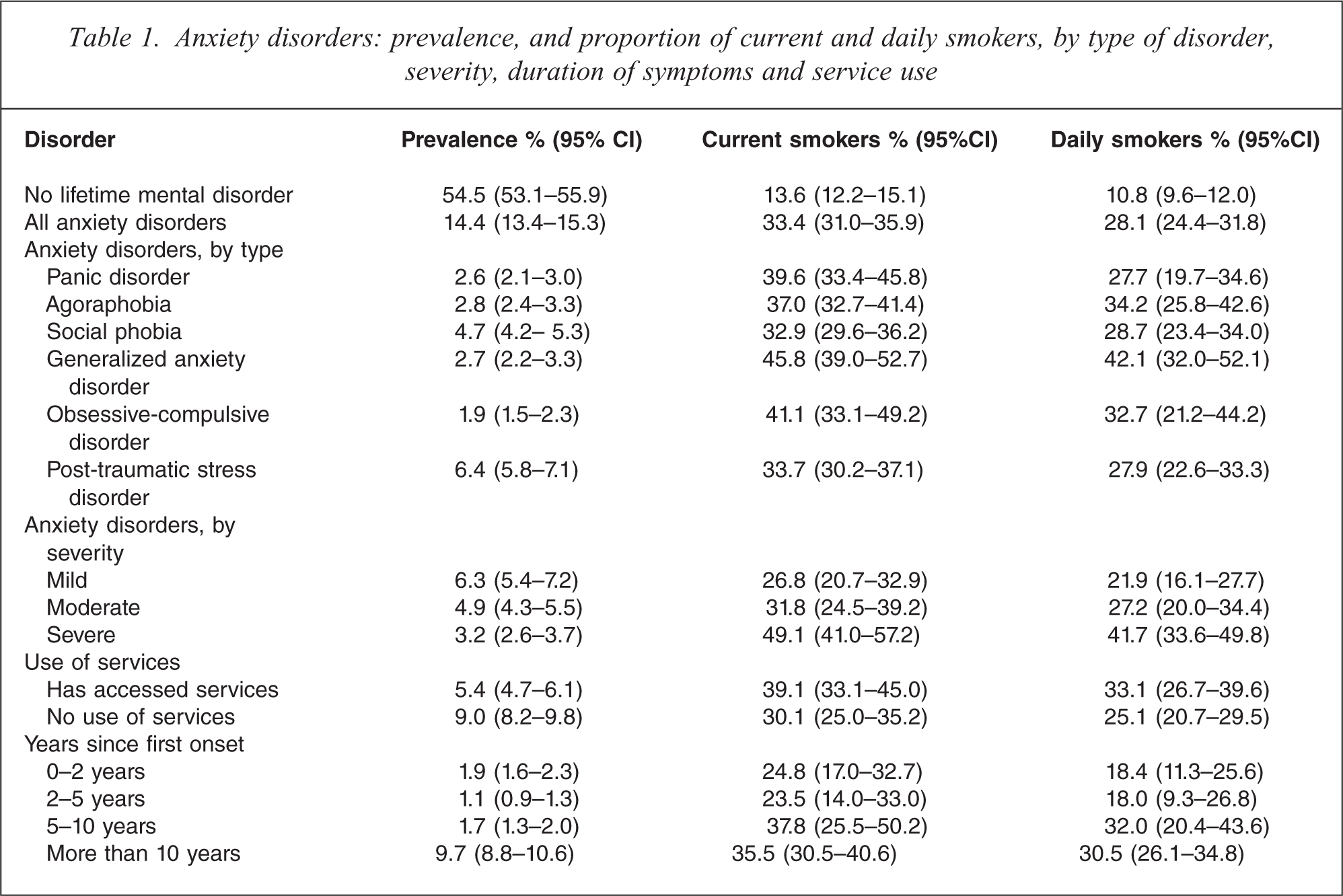
An estimated 14.4% of adult Australians have a 12-month anxiety disorder. Of these adults 33.4% are current smokers and 28.1% are daily smokers, compared with 13.6% current smokers and 10.8% daily smokers among the 54.5% of Australian adults who have no lifetime mental disorder. By type of anxiety disorder, adults with generalized anxiety disorder had a higher rate of current smoking (45.8% current smokers) than adults with social phobia and post-traumatic stress disorder, although smoking rates in these groups were still two and a half times greater than in adults with no lifetime history of mental disorder (Table 1). Note that in Table 1, a person may have more than one anxiety disorder. Rates of current smoking increased with increasing severity of disorder (χ2 5 18.2; p < 0.001), and with increasing time since first onset of symptoms (χ2 5 8.02; p < 0.043). Again, however, adults with mild anxiety disorders had smoking rates twice as high as adults with no lifetime mental disorder (Table 1). Because of their higher rate of smoking, adults with anxiety disorders make up 21.6% of all adult smokers in Australia (95% CI: 18.7–24.5%). Very similar patterns were observed for current daily smoking.
Anxiety disorders: prevalence, and proportion of current and daily smokers, by type of disorder, severity, duration of symptoms and service use
Post-traumatic stress disorder is the most commonly occurring anxiety disorder in Australian adults, with an estimated 1 000 000 adults with this disorder (Table 2). Respondents were asked to report the traumatic event that caused their worst trauma. About 6% of adults did not wish to discuss the details of the traumatic event. Most commonly reported traumatic events included the unexpected death of a loved one, rape or sexual assault, being beaten by their spouse, romantic partner or caregiver, having witnessed physical fighting at home when they were a child, or experiencing life-threatening illnesses or accidents (Table 2).
Adults with post-traumatic stress disorder: stressor event that caused the most problems
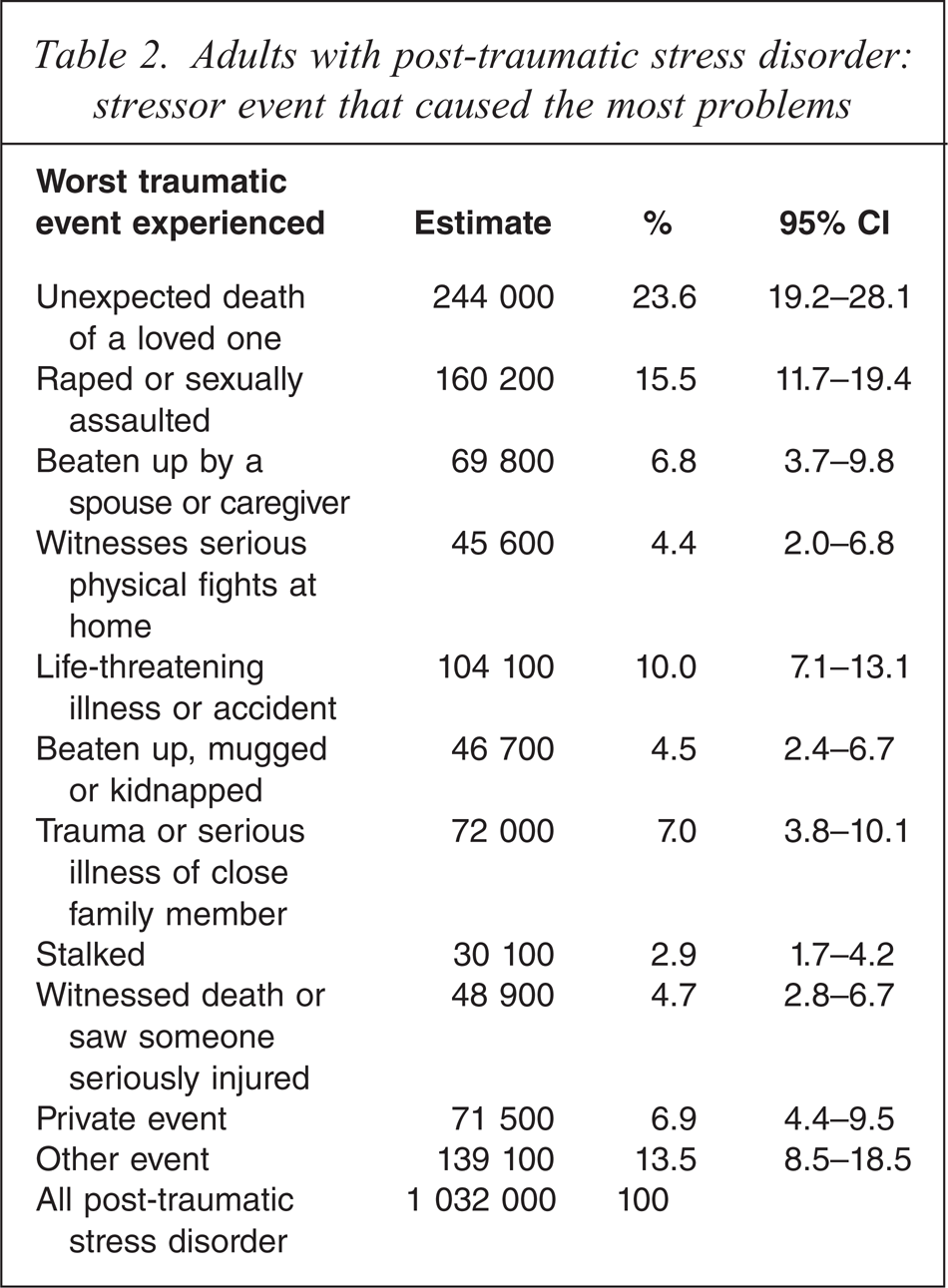
Figure 1 shows the Kaplan-Meier survival curve estimate of the proportion of smokers who no longer smoke daily, by years since they first started smoking every day. Adults with anxiety disorders are compared with adults with no lifetime history of mental disorder. Smoking cessation rates are higher in those who have no lifetime history of mental disorder. The median duration of daily smoking among adults with no lifetime history of mental disorder was 14 years (95% CI: 12–16 years), while the median duration of daily smoking was 22 years (95% CI: 20–26 years) among adults who have anxiety disorders. We tested for the significance of the difference between these two smoking cessation curves using proportional hazards regression (Table 3). The hazard ratio for smoking cessation was 0.57 comparing adults with anxiety disorders with adults with no lifetime history of mental disorder. This model adjusted for sex and age of the survey respondent. There was no difference in smoking cessation rate by sex. There was a trend for a modest decrease in cessation rates with age, consistent with the overall trend for reduced smoking rates nationally over the last 20 years. Analysis of smoking cessation rates was conducted on adults aged 45 years or less at the time of the survey to limit the possible effect of bias due to smoking-related deaths.
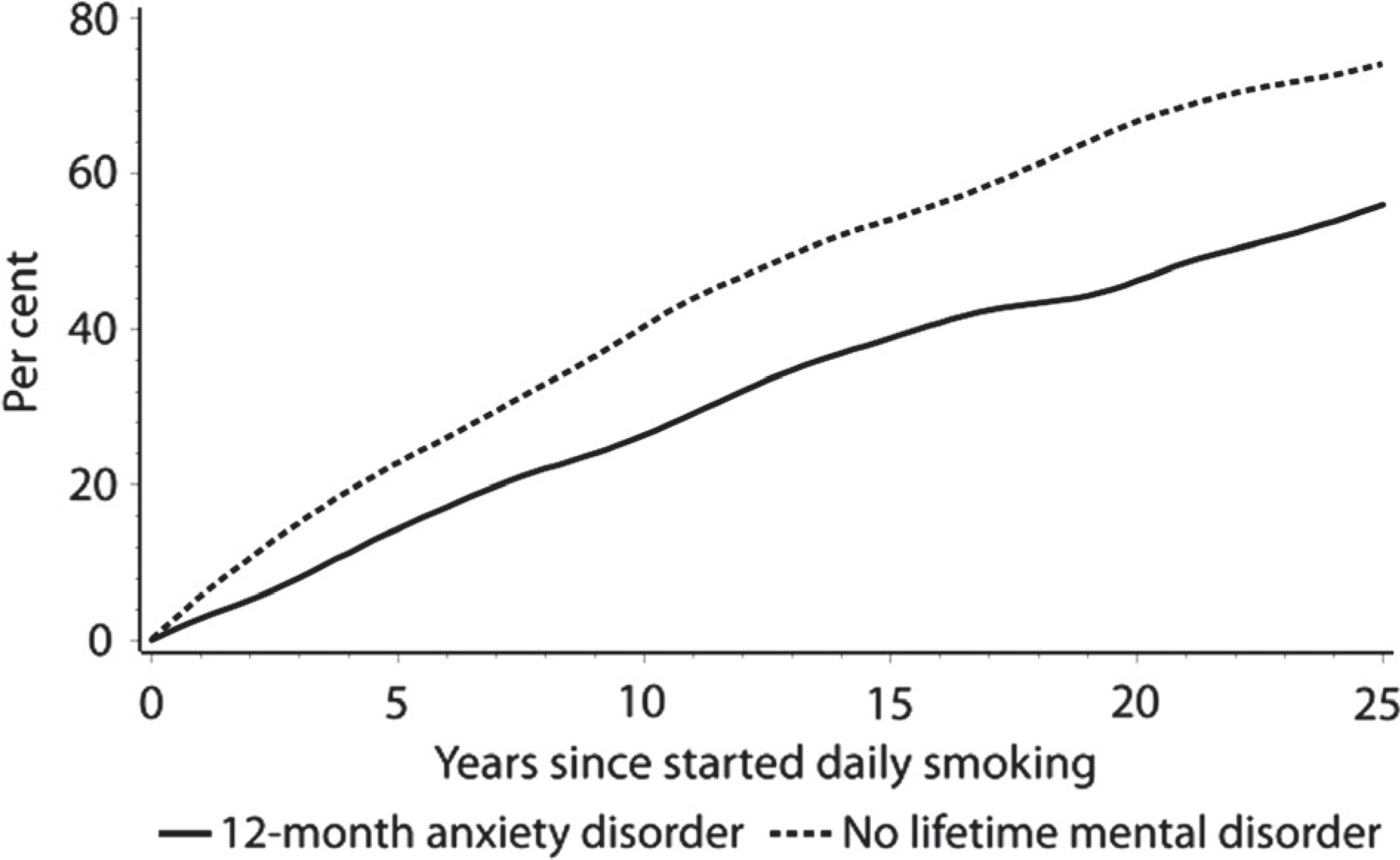
Kaplan-Meier survival curve: proportion of daily smokers who have quit smoking.
Hazard ratio for smoking cessation, people with anxiety disorders compared with people with no lifetime mental disorder, by type and nature of anxiety disordera
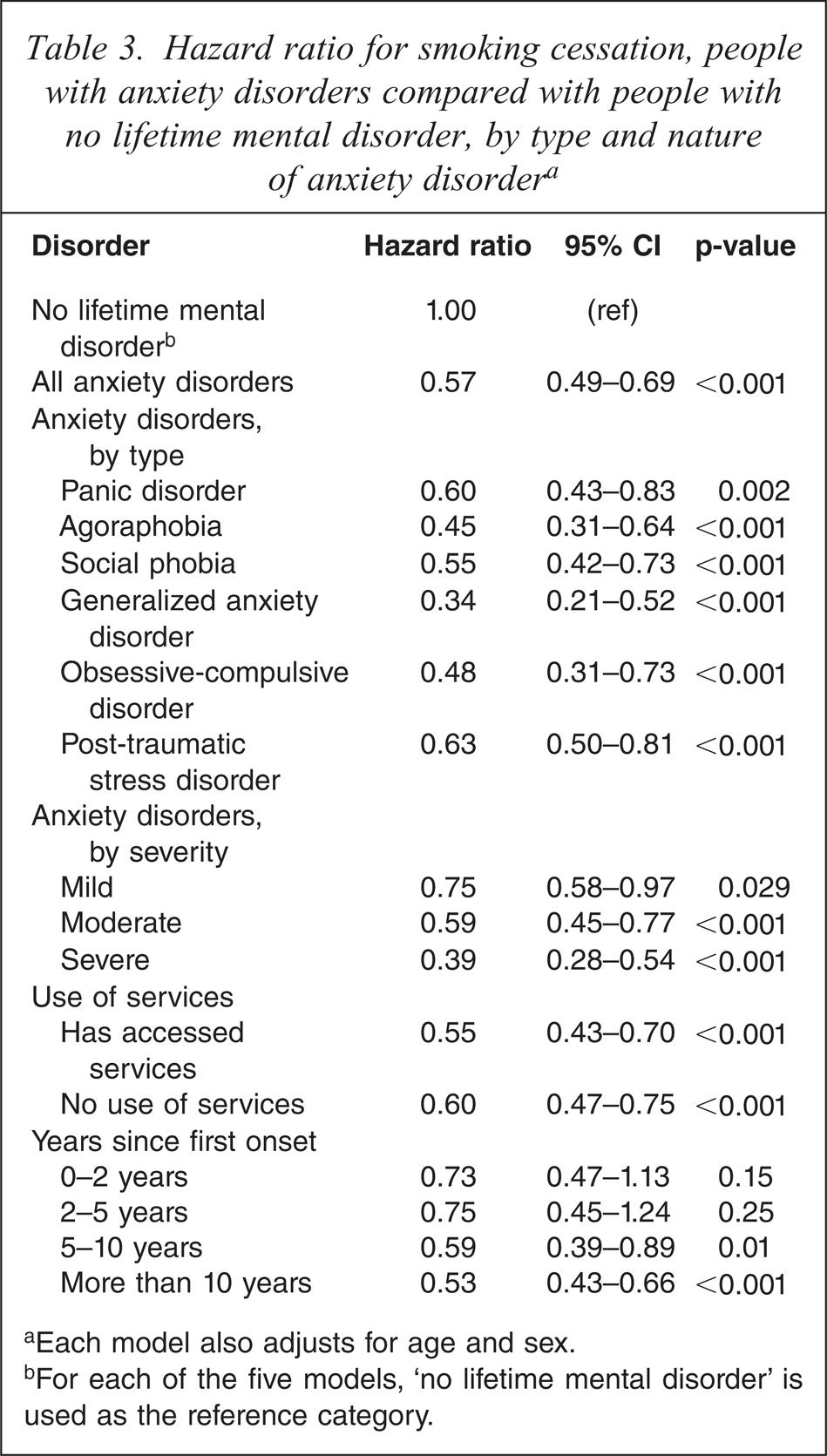
aEach model also adjusts for age and sex.
bFor each of the five models, ‘no lifetime mental disorder’ is used as the reference category.
The survey asked respondents who were no longer daily smokers at what age they stopped smoking daily. Not all of these adults will have given up smoking completely. An estimated 6.6% (95% CI: 5.2–8.1%) of former daily smokers currently smoke on a weekly basis, and 2.9% (95% CI: 2.0–3.9%) of former daily smokers were currently smoking less than weekly. The remaining 90.5% of ex-daily smokers reported no longer smoking at all (95% CI: 88.7–92.2%).
We fit four further proportional hazards models to examine smoking cessation rates classifying adults with anxiety disorders by type of disorder, severity, duration, and use of services (Table 3). Each model adjusted for age and sex. Across all types of anxiety disorders, and all levels of severity, adults with anxiety disorders were significantly less likely to stop daily smoking than adults with no history of mental disorder. Cessation rates were lowest for adults with generalized anxiety disorder, who were only one-third as likely as adults with no mental illness to cease daily smoking. There was little difference in smoking cessation rates between those who accessed services for their mental health problem in the 12 months before the survey and those who did not. The two-thirds of adults whose anxiety disorder had first onset more than 10 years prior to the survey had substantially lower hazard rate for smoking cessation.
Discussion
Anxiety disorders are the most common class of mental disorders among Australian adults [10,11]. Smoking rates among adults with anxiety disorders are substantially higher than among adults with no mental disorders, and more than one-fifth of adult smokers in Australia have a current anxiety disorder.
The strong association between anxiety disorders and current smoking has been reported from previous surveys, and has also been observed in other countries [1,3,19,20]. However, there has been little effort to account for anxiety disorders in anti-smoking programmes in Australia or internationally. Australian tobacco control experts have argued that there is no need to take specific account of anxiety disorders for several reasons: (i) the majority of disorders are not serious (i.e. do not require hospital treatment and sufferers do not qualify for a disability pension), (ii) the majority of anxiety disorders are transient in nature and are thus not relevant to long-term behaviours such as cigarette smoking, and (iii) people with anxiety disorders have the same rates of smoking cessation as anyone else and respond equally well to broad population preventive measures [7–9].
Data from the NSMHWB do not support these contentions. First, while many adults with anxiety disorders only experience mild functional impairment, these adults have current smoking rates double that of adults with no mental disorder, and are significantly less likely to quit smoking. While there is a gradient in both increasing smoking rates and decreasing likelihood of quitting smoking with increasing severity of disorder, these data strongly suggest that all anxiety disorders, including those of mild severity have an impact on smoking initiation and smoking cessation.
Second, the contention that most anxiety disorders are of short duration is not strongly supported by the survey. While the survey does not distinguish between constant and remitting recurring symptoms, the majority of anxiety disorders have onset during childhood and adolescence. As a result, most people with anxiety disorders report first onset of symptoms many years prior to the survey, with two-thirds having first onset more than 10 years prior.
Third, data from the survey show that people with anxiety disorders are significantly less likely to cease daily smoking once they have started, and thus are exposed on average to a longer duration of daily smoking. This would be expected to impact on the proportion of smokers with anxiety disorders who will ultimately suffer from smoking-related morbidity and mortality.
It has been suggested that money spent on targeted anti-smoking efforts is money wasted as it is money taken away from the most successful broad population-based approaches [21]. Our results from the NSMHWB suggest that not all groups within the population respond equally to these broad population-based efforts. Only investing in strategies that focus solely on smoking without regard to other issues that smokers may be dealing with is likely to contribute to inequality of health outcomes between those with and without mental disorders. The contention that investment in anti-smoking programmes should be concentrated on broad programmes is based on the assumption that all members of the population are equally likely to respond to these programmes. Where a substantial proportion of the population is less likely to respond to a population programme a case is supported that more nuanced approaches are required. As the evidence suggests that people with anxiety disorders are more likely to smoke and less likely to quit smoking, and are thus less likely to have benefited from the long-running efforts to reduce smoking prevalence in Australia, it could well be argued that anxiety disorders and life circumstances surrounding them justify a higher rather than lower level of support to achieve equitable outcomes.
While many of those with current anxiety disorders had their first onset of symptoms many years before the survey, our results do not inform whether the anxiety disorder was a cause of smoking, the reverse, or whether both are related to some other factor. Studies of teenagers suggest that both anxiety and depressive symptoms predict both experimenting with smoking and later daily smoking [22,23]. While the start of daily smoking most commonly occurs in the mid- to late teenage years, the majority of anxiety disorders have their first onset during childhood or adolescence. Results from prospective studies suggest that anxiety disorder is a risk factor for nicotine dependence [24], and the reverse may also be true for some anxiety disorders, such as panic attacks [25]. People with anxiety disorders may smoke to regulate their symptoms and to cope with emotional distress [24]. Whether the association between anxiety disorders and smoking is causal in either direction, or whether shared common risk factors underlie both smoking behaviours and anxiety disorders is the subject of ongoing research [24]. Nonetheless, it would seem logical that attention to both the emotional and psychological wellbeing of young people and risk-taking behaviour would benefit both the mental health and wellbeing and smoking status of young people.
It is common marketing practice to create variants of products or brands and promotional messages that are targeted towards population sub-groups. These population groups may be defined based on demographic or psychosocial characteristics. This approach was used historically in the tobacco industry where a significant number of brand variants were brought to market with their own promotional strategies and targeted demographics, even though the products predominantly differed in style and packaging with little substantive functional difference. Thus different cigarette brands would be targeted to different personality traits and marketed based on differing motivations for smoking [1,26–29]. Targeted approaches have been largely rejected in the field of tobacco control in the belief that while population groups may have very different rates of smoking initiation, cessation rates and responses to population campaigns are equal across groups [21]. This approach pays little attention to the contexts in which people smoke, and does not acknowledge that promotional messages that resonate with some people alienate others. In the trend to denormalize or stigmatize smoking an underlying message is put forward that smokers smell, are selfish and thoughtless, throw their rubbish in the streets and are generally undesirable for non-smokers to associate with. By establishing that smoking is outside the bounds of normally accepted social behaviour the hope is that people will be sufficiently motivated by the desire to be part of normal society that they will abstain from smoking [30,31]. However, many people with mental disorders including anxiety disorders already face or perceive stigmatization as a result of the symptoms and consequences of their disorders [32]. For such people who struggle to overcome the real and perceived stigmas associated with their mental illness, there would seem to be less motivation to choose to not smoke to avoid the stigma associated with smoking. The benefits of a stigmatizing strategy must be balanced against the harm it may cause [33].
The National Preventative Health Taskforce has responded to submissions in this area in the recently released National Preventative Health Strategy [34], which has acknowledged that people living with mental illness are an under-addressed group in tobacco control. We hope this is a first step towards addressing smoking behaviours in all people with mental illness, not just those in contact with mental health services.
Limitations
The survey was a cross-sectional survey relying on respondent recall. Trained lay interviewers administered fully structured questionnaires in the households of the respondents. While the CIDI has been validated in several countries and is strongly related to diagnosis by trained professionals, diagnosis via the CIDI is not the same as would be produced by examination of all respondents by qualified psychiatrists. Data on mental illnesses and smoking were obtained by respondent recall. There may be cases where respondents are reluctant to admit behaviours that are potentially stigmatizing, although it would be anticipated that this would occur less often in a lengthy face to face survey interview than it would in telephone and mail-based surveys. The surveys that track smoking prevalence in Australia are predominantly shorter surveys administered via telephone, and these surveys are subject to high non-response and non-contact rates. The estimates of smoking prevalence obtained from the NSMHWB and other face-to-face surveys such as the recent National Health Survey tend to be higher than those reported by the telephone-based tracking surveys. Response and participation biases may account for some of the differences.
As it was household-based, the NSMHWB did not include people in psychiatric institutions, prisons or other institutional care, and thus may underestimate the prevalence of some disorders, though the proportion of the population not covered by the survey is small.
Survival analysis of smoking cessation has been based on respondent recall of start and end ages of smoking. These data may not be as reliable as data collected in a prospective longitudinal study. However, we are not aware of any such study ever undertaken that has a robust assessment of mental health status. We sought to limit exposure to recall and early death bias by limiting this part of the analysis to respondents aged 45 years or less.
Footnotes
Acknowledgements
The NSMHWB was conducted by the Australian Bureau of Statistics and funded by the Australian Government Department of Health and Ageing. The views expressed in this paper are those of the authors and not those of the Australian Bureau of Statistics or the Australian Government Department of Health and Ageing.