
Abstract
Considerable scepticism greeted the first estimates of mental disorder prevalences from fully structured lay interviews in the Epidemiological Catchment Area study (ECA) [1]. This scepticism did not diminish when a decade later the National Comorbidity Survey (NCS) published even higher estimates [2]. Concern was expressed around the possibility that these community surveys were classifying too many mild episodes of psychological or emotional distress as depressive disorder [3,4]. As a consequence, the requirement for classification of disorder to encompass not just symptom criteria but impact of symptoms was incorporated into the DSM-IV classificatory system [5]. This system placed greater emphasis on the diagnostic requirement for symptoms to cause clinically significant distress or functional impairment. For depressive episodes, DSM-IV also includes a severity gradient of mild, moderate or severe episodes. However, these changes in the classification system have done nothing to allay concerns that depression is over-diagnosed, resulting in a medicalization of normal human experience and inappropriate treatment [6–9]. Indeed, the allowance of a severity gradient has been referred to as ‘dimensionalizing’ depression, blurring the distinction between clinical and normal mood states [6].
Data that can inform this debate, for example on the distribution of major depressive episode severity categories in the general population, have only recently become available. The ECA and NCS surveys were developed prior to the publication of the DSM-IV criteria, but the recent World Mental Health surveys [10], of which the New Zealand Mental Health Survey (NZMHS) is the largest single survey [11,12], use a revised structured interview (the Composite International Diagnostic Interview: CIDI 3.0 [13]) designed to correct for the possible over-diagnosis of depression. This is done through explicit probes for severity of dysphoria and anhedonia; by requiring clinically significant distress or impairment associated with these symptoms; and by asking separate questions about symptom duration (hours per day, days per week) and duration of depressive episodes [14]. Of particular relevance to the debate about the clinical significance of diagnosed depression, the NZMHS, along with other WMH sites, incorporated several measures of impairment (both disorder-specific and global) and of symptom severity for depressive episodes in the past 12 months.
Prior publications from the NZMHS have provided initial information on impairment associated with major depressive disorder [15,16], but we present here new and more detailed information on the symptom severity and disorder-specific impairment associated with 12-month major depressive episodes, treatment by severity, and the age and gender patterning of episodes and correlates.
Methods
Survey sample
Te Rau Hinengaro
Te Rau Hinengaro: the New Zealand Mental Health Survey 2003/4 (NZMHS) was a nationally representative community survey involving face-to face interviews with 12 992 adults aged 16 and over. Interviews were conducted by professional lay interviewers from October 2003 to December 2004 with a response rate of 73.3%. Written informed consent was obtained from all participants and ethics review and approval was obtained from the 14 New Zealand regional ethics committees. Internal sub-sampling was used to reduce respondent burden by dividing the interview into two parts. Part 1 included the core diagnostic assessment of mood disorders, substance use disorders and most of the anxiety disorders. Part 2 included assessment of post-traumatic stress disorder, obsessive–compulsive disorder and eating disorders, together with additional information relevant to a wide range of survey aims. All respondents completed Part 1. All Part 1 respondents who met criteria for an anxiety or depressive disorder, had a hospital admission for psychiatric disorders, or had made plans to suicide, plus a probability sample of other respondents were administered Part 2 (N = 7435). A more detailed description of the survey methods is provided elsewhere [11,12].
Measures
Mental disorders
The interview used to assess mental disorders was the World Mental Health Composite International Diagnostic Interview (WMH-CIDI), now the CIDI 3.0 [10,13]. This fully structured lay-administered interview ascertains lifetime prevalence of disorder (disorder occurring at any age up to the age at interview) plus recency of episodes or symptoms, which allows 12-month and 1-month prevalence to be derived. Major depressive episode (MDE) was assessed using the definitions and criteria of the DSM-IV [5]. CIDI organic exclusion rules were imposed which means that symptoms were not attributed to MDE if respondents attributed them to organic (physical) causes and this attribution was independently verified by a psychiatrist. MDE differs from major depressive disorder in including episodes that occur in individuals who also experience episodes of mania or hypomania.
Role impairment
Respondents with symptoms of MDE in the past 12 months were administered the disorder-specific Sheehan Disability Scale (SDS)[17] which assesses the degree of impairment in functioning due to depression in four domains: work, household, close relationships and social roles in the worst month of the past year. Responses were scored with a 0–10 visual analogue scale with response options labelled none (0), mild (1–3), moderate (4–6), severe (7–9) and very severe (10). If a domain was not applicable, the mean for a participant was the mean across all applicable domains.
In addition, respondents were asked to estimate the number of days in the past 365 days when they were ‘totally unable to work or carry out normal activities’ because of depression.
Symptom severity
Respondents who met 12-month MDE criteria were administered a short (9 questions) version of the Quick Inventory of Depressive Symptomatology Self-Report (QIDS-SR) [18] to assess symptom severity in the worst month of the past year. The QIDS-SR is a fully structured rating scale based on DSM-IV diagnostic criteria that is highly correlated with both the clinician-administered full version (the Inventory of Depressive Symptomatology: IDS-C) [19] and the Hamilton Rating Scale of Depression (HAM-D) [20]. Transformation rules developed for the QIDS-SR were used to convert scores into clinical severity categories mapped to conventional HAM-D ranges of none (i.e. not clinically depressed), mild, moderate, severe and very severe [21].
12-month treatment
All Part 2 respondents were asked about receiving treatment for emotional problems in the past 12 months, the type of professional seen, and use of support groups, self-help groups and hotlines. Responses were used to classify 12-month treatment in the specialist mental health (SMH) sector (inpatient treatment or outpatient treatment with a psychiatrist, psychologist, social worker or counsellor in a mental health specialist setting, or use of a mental health hotline); the general medical (GM) sector (outpatient treatment with a primary care physician, other medical specialist, nurse or any other health professional); the human services (HS) sector (outpatient treatment with a religious or spiritual advisor or with a social worker or counsellor in any setting other than a specialist mental health setting), and the complementary–alternative medical (CAM) sector (outpatient treatment with any other type of healer, participation in an Internet support group or self-help group).
Statistical analysis
Estimates were weighted to take into account the probability of selection; to adjust for intentional oversampling of Maori and Pacific peoples; to adjust for non-response; and to post-stratify by age, sex and ethnicity to the 2001 census population. Additional weights were applied to adjust for the probability of selection into the Part 2 subsample. Age and gender differences in prevalence, impairment, symptom severity and treatment of MDE were examined using cross-tabulations and mean comparisons across groups. Chi-square values from Wald tests were used to assess significance when comparing means. Logistic regression analyses were used to study demographic correlates of treatment. Taylor series linearization [22] was used to approximate the variance of estimates using SUDAAN 9.0.1 statistical analysis package [23] to adjust for the complex sampling design. Associations were considered statistically significant at p <0.05.
Results
The total sample size was 12 992 with weighted proportions for males and females being 48% and 52% respectively, and 16.3% for 16–24 year olds, 39.3% for 25–44 year olds, 30.4% for 45–64 year olds and 14% for those aged 65 years and older. Full details on sample characteristics of the NZMHS have been published previously [11,12]. The prevalence of MDE in the past 12 months for all ages was 6.6%, and decreased with increasing age (Table 1); 12-month prevalence was higher in females (8.1% versus 4.9% in males).
12-month prevalence of major depressive episode (MDE) by age and sex
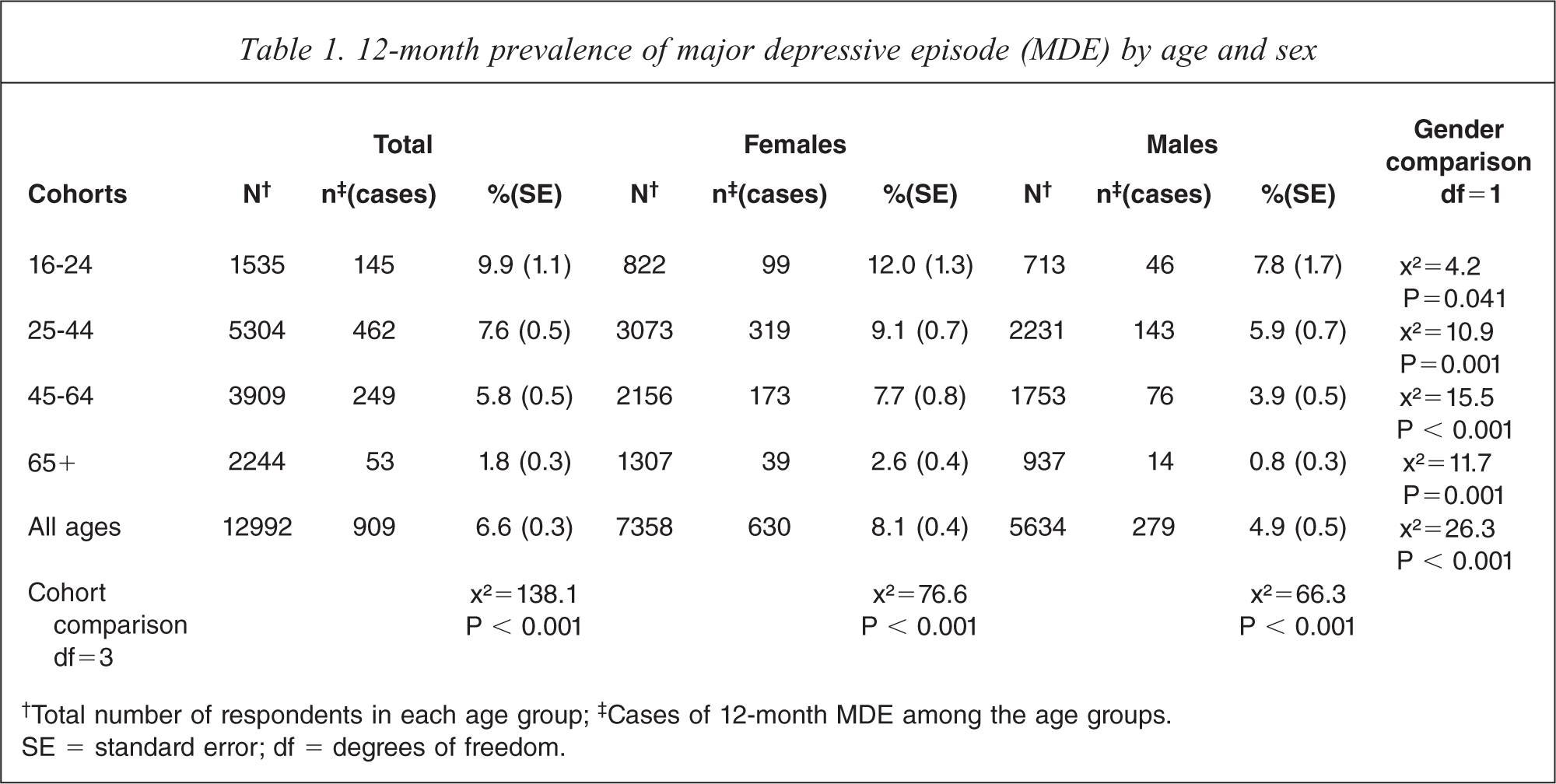
†Total number of respondents in each age group; ‡Cases of 12-month MDE among the age groups.
SE = standard error; df = degrees of freedom.
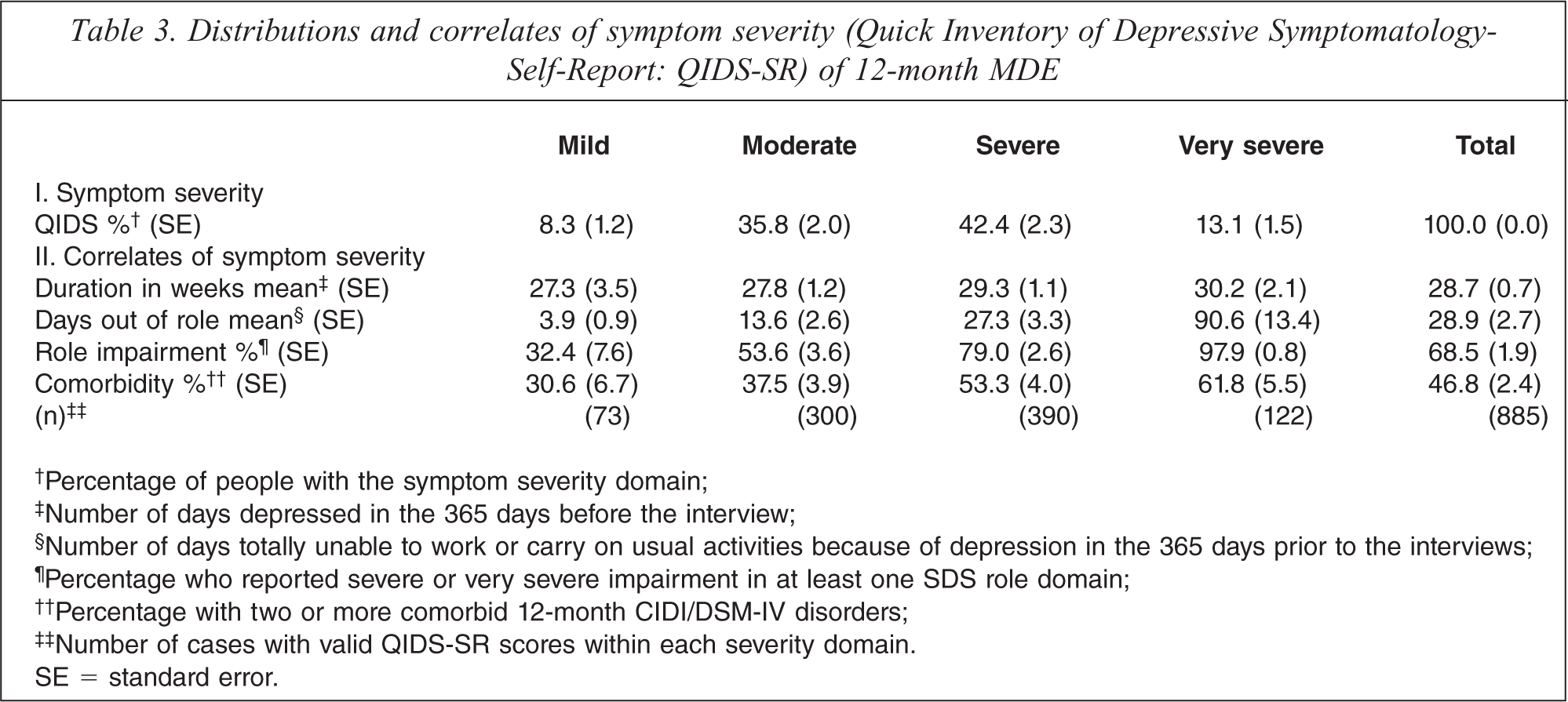
The degree of severe role impairment associated with 12-month MDE, as indicated by a Sheehan Disability Scale score of 7 or more, is shown in Table 2. For all ages, the percentage reporting severe impairment for particular domains ranged from a little over a third (36.4%) for impairment in home functioning to a half (49.9%) for impairment in social role functioning. Over two thirds (68.7%) of respondents (of all ages) reported severe impairment in at least one domain. The percentage reporting severe impairment did not differ significantly by age or by gender.
Degree of role impairment associated with MDE: % severe impairment (Sheehan Disability Scale score >= 7) by age and sex
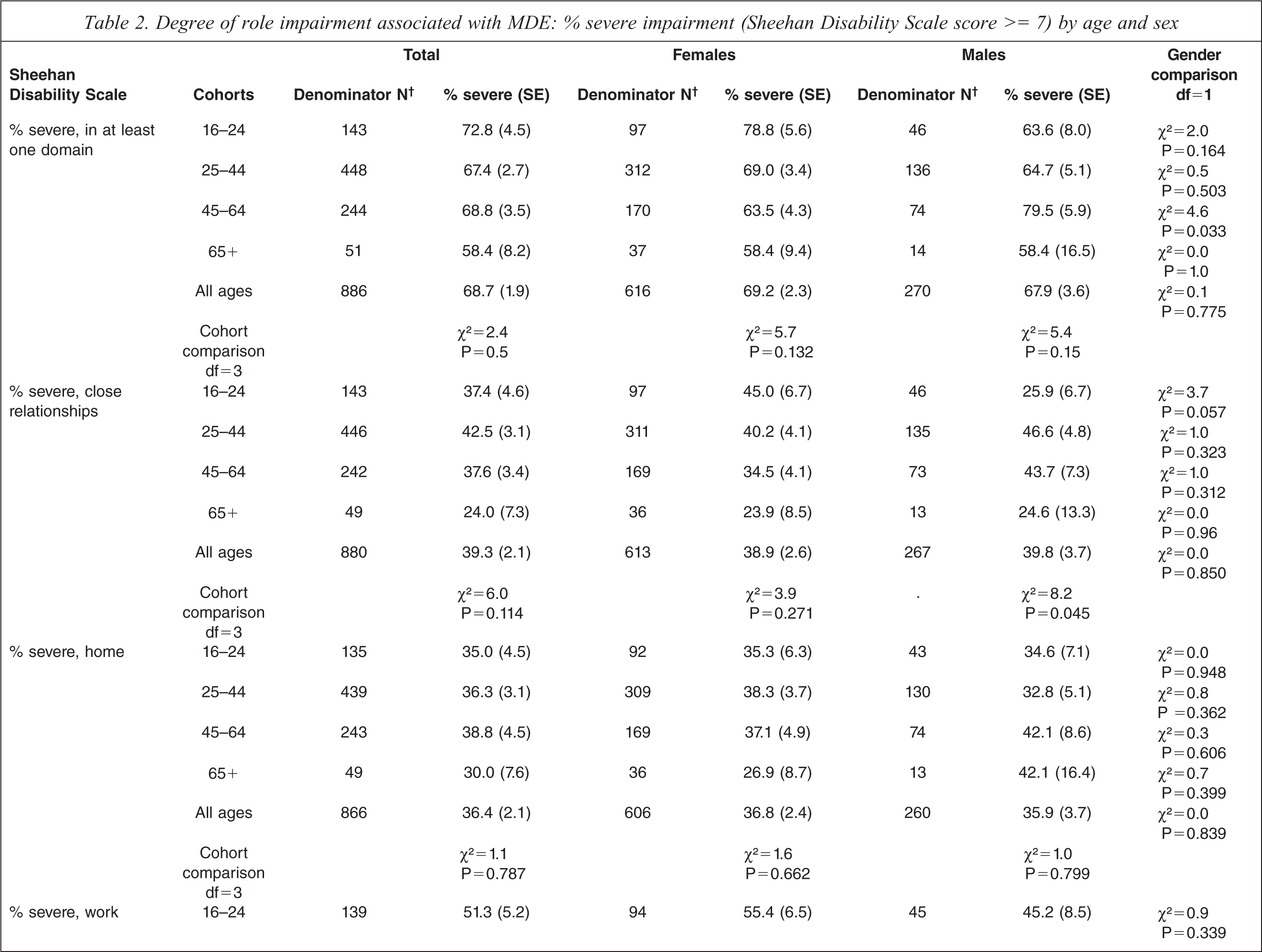
†Total number of cases with 12-month MDE among each age group; not all that have 12-momth MDE have valid Sheehan scores, therefore the Ns may be inconsistent with Table 1.;
SE = standard error; df = degrees of freedom.
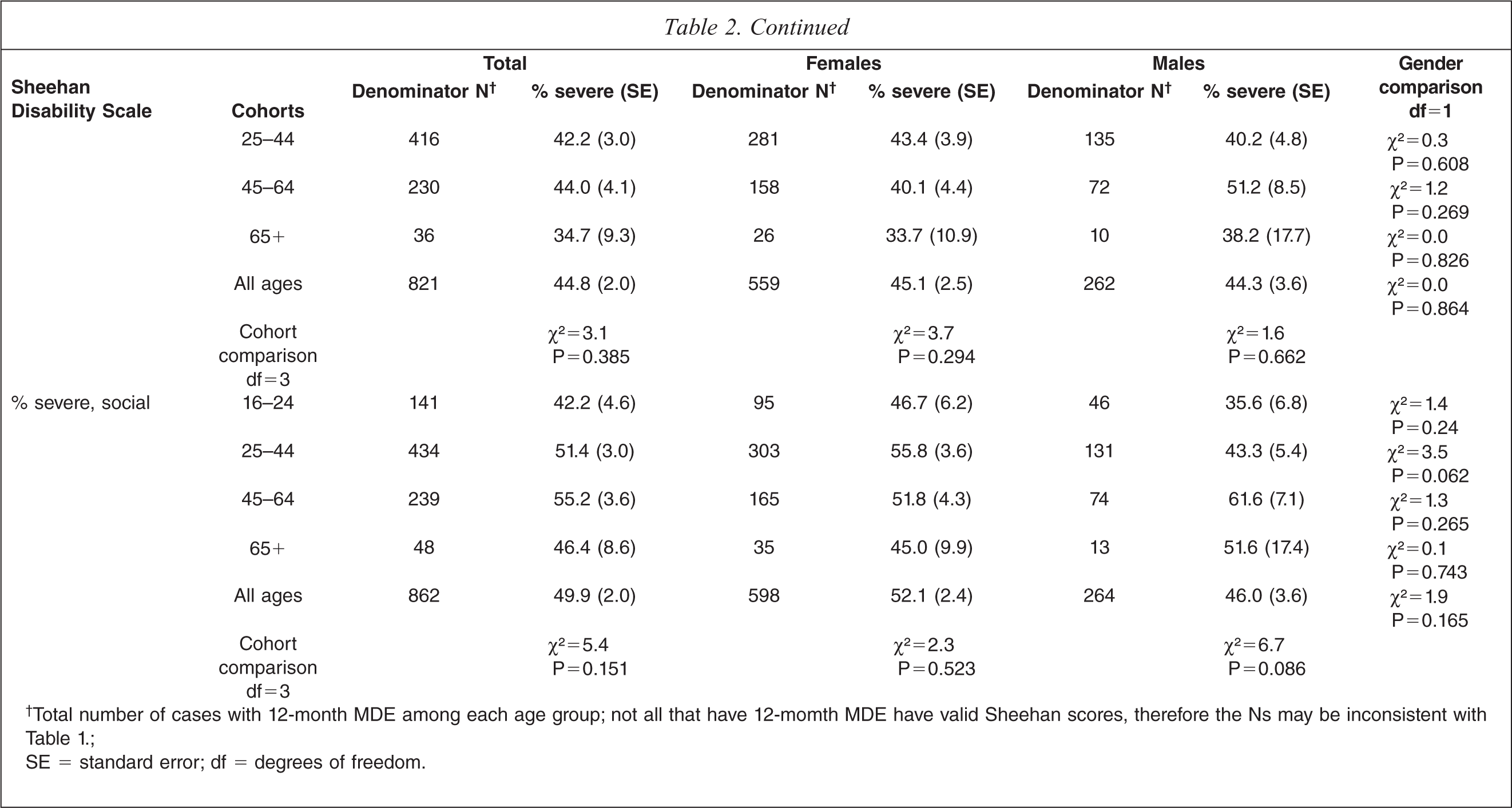
Table 3 shows the symptom severity associated with 12-month MDE, as measured by the QIDS-SR, and on correlates of severity. All MDE episodes were classified as clinically depressed, with fewer than 10% rated as mild episodes and over half of episodes (55.5%) rated as severe or very severe on the QIDS-SR. Severe or very severe QIDS-SR episodes were typically lasting 29–30 weeks and were characterized by substantial role impairment and psychiatric comorbidity. When role impairment was measured by days totally unable to work or carry out usual activities in the past year, those classified as very severe on the QIDS reported around three months (91 days) totally out of role.
Distributions and correlates of symptom severity (Quick Inventory of Depressive Symptomatology-Self-Report: QIDS-SR) of 12-month MDE
†Percentage of people with the symptom severity domain;
‡Number of days depressed in the 365 days before the interview;
§Number of days totally unable to work or carry on usual activities because of depression in the 365 days prior to the interviews;
¶Percentage who reported severe or very severe impairment in at least one SDS role domain;
††Percentage with two or more comorbid 12-month CIDI/DSM-IV disorders;
‡‡Number of cases with valid QIDS-SR scores within each severity domain.
SE = standard error.
Table 4 provides information on who sought treatment within each treatment sector for their depressive episode in the past 12 months, stratified by age and Sheehan role impairment. The percentage receiving any treatment was greater for those with severe role impairment (64.6% for all ages) versus those without severe impairment (51.4%). Only a third (33%) of those with severe role impairment received treatment from mental health services, and a little under half of those with severe role impairment (48.5%) had a consultation with a general practitioner.
Treatment for MDE by Sheehan role impairment
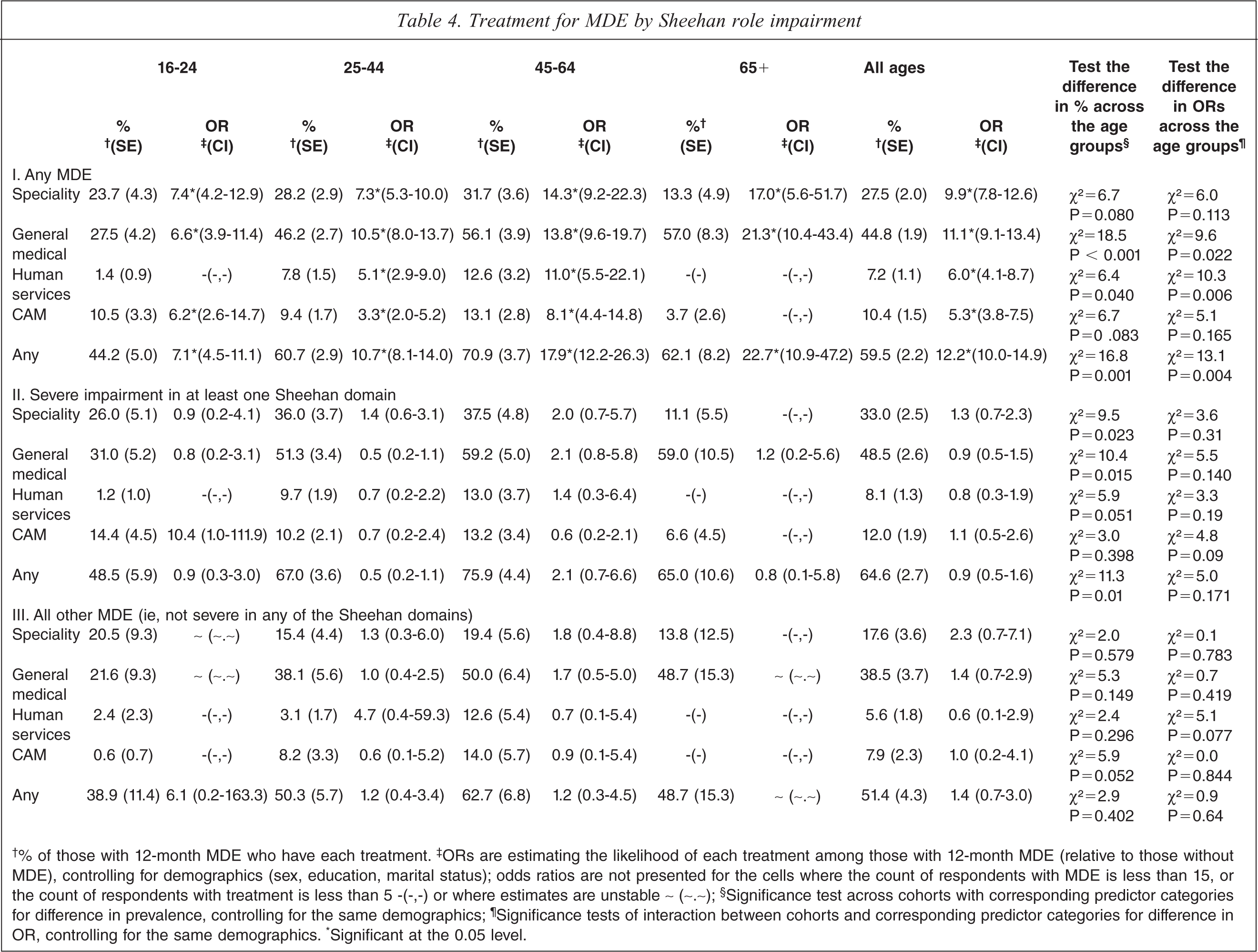
†% of those with 12-month MDE who have each treatment. ‡ORs are estimating the likelihood of each treatment among those with 12-month MDE (relative to those without MDE), controlling for demographics (sex, education, marital status); odds ratios are not presented for the cells where the count of respondents with MDE is less than 15, or the count of respondents with treatment is less than 5 -(−,−) or where estimates are unstable ∼ (∼.∼); §Significance test across cohorts with corresponding predictor categories for difference in prevalence, controlling for the same demographics; ¶Significance tests of interaction between cohorts and corresponding predictor categories for difference in OR, controlling for the same demographics. ∗Significant at the 0.05 level.
Among those with any MDE, increasing age predicted increasing treatment-seeking in the general medical, human services and ‘any’ sectors, relative to help-seeking among those without MDE. This was also seen for the actual percentage with MDE seeking treatment except that this was highest in the 45–64 age group for ‘any’ service contact. The age comparisons among the adjusted percentages of those with MDE seeking treatment are shown in the column second from the right of Table 4 beside the significant interactions with age in the adjusted odds of treatment seeking among those with MDE (relative to those without MDE). These significant age × MDE interactions indicate that the age differences in treatment-seeking among those with MDE are not simply a function of age differences in treatment-seeking in the general population.
Discussion
How should these results be interpreted in the context of concerns that diagnostic thresholds are set too low by current classificatory systems and that lay administered community surveys using the CIDI may aggravate this further by including too many mild cases? The finding of 6.6% with 12-month MDE is not consistent with the claim that the ‘dimensionalizing’ of clinical depression in the DSM system has made it ‘almost a ubiquitous human experience’ ([6] p 841). Nor is there evidence that the CIDI 3.0 over-diagnoses relative to clinician-administered interviews. Blinded clinical reappraisal surveys using the Structured Clinical Interview for DSM-IV (SCID) administered by clinicians as the validation standard have been conducted in a number of the WMH surveys (not including New Zealand) and have found moderate to good concordance between CIDI and SCID estimates [24].
In relation to the concern that community surveys count too many mild episodes as cases, this survey found that fewer than 10% of MDE cases were classified as mild in terms of symptom severity on the QIDS-SR, using standard Hamilton symptom severity thresholds. The Hamilton severity thresholds have been criticized [8], but they seem validated by other aspects of these results: for example, by the fact that the vast majority of the MDE episodes rated on the QIDS-SR as severe or very severe were accompanied by severe functional impairment in at least one Sheehan Disability Scale domain, and by a period of 1–3 months when those experiencing episodes were totally unable to carry out usual activities.
Of course, it is still possible to remain sceptical about these findings since doubts have been raised about the validity of self-reported impairment in depressed individuals [25,26]. For example, these results show that social functioning is one of the domains most affected by depression, and some researchers, observing that the degree of self-reported social disability by depressed individuals improves once depressive symptoms have been relieved, have concluded that depressed individuals ‘over-report’ their degree of disability [27]. We suggest that such views reflect an unrealistic expectation of objectivity in the depressed individual's self-report that overlooks a central feature of clinical depression: its impact on psychological functioning, resulting in distorted perception, judgement, motivation and cognition. This psychological dysfunction, temporary or enduring, is as real an impairment as any other [16,28].
These results also provide little indication of over-treatment of MDE, with only a third of those experiencing severe impairment in at least one Sheehan domain receiving treatment in the mental health sector, and only a half of these same individuals receiving treatment in the general medical sector. These data merely indicate that a consultation took place; they do not necessarily indicate that effective treatment was received by the person. It has been argued that although there may be a significant group of severely depressed patients not receiving treatment there is a much larger group with mild symptoms who are being treated inappropriately, particularly with anti-depressant medication, and that this is an indication of the dangers of depression awareness campaigns [8]. This study does not provide data that can evaluate that argument empirically, but even if it were true, we must remain concerned about the proportion of under-treated severe episodes due to the significant suicide risk they pose [29].
This study is limited by sample selection bias, in that although this survey has a reasonably good response rate for a survey of this nature, it is likely that people with severe mental disorders were less likely to agree to take part. Additionally, the sampling frame was the non-institutionalized population, so again those with severe disorders may be under-represented. This sample selection bias means that the estimates reported here of those with more severe depression should probably be considered conservative.
In summary, we find that symptoms classified by the CIDI as DSM-IV major depressive episodes in the non-institutionalized adult New Zealand population are typically self-rated as of moderate to severe severity and are accompanied by substantial functional impairment. Of concern is that a substantial proportion of those with severe and moderate depressive episodes have not received treatment. These results do not support the contention that major depressive episodes are over-diagnosed and over-treated and that current diagnostic systems are capturing too many mild episodes.
Footnotes
Acknowledgements
The survey was carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. WMH publications are listed at ![]() .
.
Other members of the NZMHS research team are: Magnus McGee, Joanne Baxter, Jesse Kokaua, Te Kani Kingi, Rees Tapsell, Siale Foliaki, David Schaaf, Mason Durie, Colin Tukuitonga and Chris Gale.
We thank the Kaitiaki Group and Pacific Advisory Group for their input and support for this survey and we thank all the participants.