
Abstract
Atypical depression (AD) has been a subject of nosological debate since its conception in the late 1950s. It was found to be associated with diverse conditions such as phobic anxiety, ‘hysteroid dysphoria’, reversed vegetative shift, chronic pain, bipolar disorder, post-psychotic and non-endogenous depression [1–3]. Since the 1960s and especially after the publication of the DSM-IV [4,5], the concept of AD has been based increasingly on reversed neurovegetative symptoms such as increased appetite/weight and hypersomnia.
Most recent studies that examined the nosological status of AD were based on clinical samples of outpatients with major depressive episodes (MDE) and the DSM-IV criteria of AD [6–9]. They showed that 31.0–61.9% of those with MDE had AD [6–8]. Compared to those with non-atypical depression (non-AD), individuals with AD were characterized by higher rates of female gender, younger age, younger age of onset, more depressive mixed state, comorbidity, hypomanic symptoms, family history of bipolar disorders, higher suicidality and rate of bipolar II disorder (BP-II). The findings on impairment were less conclusive [6–8,10]. These overall findings suggested that AD may be clinically related to bipolar spectrum disorders. In fact, clinical studies showed that as many as 64.2-72.0% of those with AD had BP-II and soft (subthreshold) bipolar II disorder (soft BP-II) [9,11]. Sánchez-Gistau et al. also found that among outpatients with bipolar disorder and AD, proportions of bipolar I disorder (BP-I; 54.7%) and BP-II (42.6%) were comparably high [12]. There is evidence that, like depression in bipolar disorder, AD does not respond satisfactorily to conventional antidepressant monotherapy. This claim for a specific response to monoamine oxidase inhibitors [13], however, remains to be substantiated because recent studies did report some efficacy of selective serotonin re-uptake inhibitors and cognitive therapy [2,5,14]. All in all, clinical studies suggested that AD may be a valid affective variant that occupies an intermediate nosological position in the unipolar–bipolar spectrum of mood disorders. Whether the findings hold true in community settings, however, is less clear.
Community-based studies of AD are less common than clinical studies but are vital for clarifying the validity of AD because of the selection bias that might accompany the latter. They usually defined AD by the presence of reversed neurovegetative symptoms instead of using combinations of mood reactivity and the four other DSM-IV symptoms of AD [2,15–18]. This could partly be because the other three symptoms (i.e. mood reactivity, oversensitivity to rejection, and leaden paralysis) are hard to operationalize in community surveys conducted by lay interviewers. Moreover, the diagnostic value of mood reactivity and rejection oversensitivity has been questioned by many researchers [2,5,19]. The commonly used epidemiological definition of AD, based on increased appetite/weight and hypersomnia, exhibited high specificity (90.5%), positive predictive value (86.1%) and adequate receiver operating characteristic area (0.85) for predicting DSM-IV AD [10]. Some studies have even suggested that hypersomnia alone was more strongly associated with BP-II [20,21]. Overall, the lifetime prevalence of AD in the community was found to range from 0.7 to 2.8% [15,16,18,19]. Because increased appetite and hypersomnia have been shown to be more sensitive for identifying the external validating characteristics of AD than other DSM-IV atypical symptoms [20], it is not surprising that community studies that used reversed neurovegetative symptoms produced similar epidemiological findings as clinical studies using DSM-IV criteria in defining AD [6–8,10,11]. They confirmed clinical studies regarding higher rates of female gender and younger age of onset in individuals with AD than non-AD. A higher rate of help-seeking among those with AD than non-AD was found in some [22] but not other studies [16,17]. The findings on impairment in AD versus non-AD were mixed [16,22]. Regarding relationship with bipolar disorders, some studies found that AD was not significantly associated with BP-I [16,18], while others showed that AD was associated with subthreshold bipolar II disorder [20,22]. It is worthy of note that BP-I, BP-II, and soft BP-II have not previously been simultaneously examined in the same community study of AD.
Nearly all previous studies of AD were conducted in Western societies. Consequently, it is worth exploring if Western findings on AD can be replicated in a non-Western population, thereby lending support to the cross-national validity of AD. Based on the extant literature and our clinical experience, we hypothesized that AD is as common in Hong Kong as in Western communities and is associated with female gender, higher rates of suicidality, family history of mental disorder, soft BP-II, and professional help-seeking behaviour. We studied the aforementioned hypotheses by examining the 12 month prevalence of AD and non-AD in the Chinese adult population of Hong Kong, and investigating the differences in demographic and clinical profiles between AD and non-AD. To examine the relationship between AD and bipolar disorder more thoroughly, we included a wide spectrum of bipolar disorders (BP-I, BP-II, and soft BP-II) in the present study.
Methods
Sampling
The present study was part of a survey on the prevalence and correlates of bipolar spectrum disorders [23]. It was approved by the research ethics committee of The Chinese University of Hong Kong. A random telephone survey of the general population aged between 18 and 65 years was conducted in Hong Kong between 16 January and 16 February 2007. Hong Kong has a population of 6.9 million and >99% of the domestic households have a telephone at home [24], with very few of them having more than one telephone line. Therefore, sampling telephone lines should generate a representative sample of households. By randomly selecting telephone numbers from the local telephone directory with the final two digits randomized, 7631 calls were made with initial contact established. Among them there were 1158 calls with no interviewees aged between 18 and 65 years, 1730 calls with respondents hanging up without acknowledging the actual content of the survey, 1727 calls in which respondents rejected interviews, and 3016 calls in which respondents successfully completed the interviews. Therefore, of the households that were successfully contacted and had interviewees within the age range, the participation rate was 63.6% (3016/[3016++1727] ×100%). Informed verbal consent was obtained in each successful contact. Each telephone interview took an average of 20 min to complete. The sample, which consisted of 1279 male and 1737 female respondents, was weighted according to the gender distribution of different age groups in Hong Kong as reported by the Census and Statistics Department of the Hong Kong Government in 2006. These distributions in the present sample (Table 1) were highly comparable to figures from the Census and Statistics Department [24]. At a 95% confidence level, the maximum sampling error was ±2.19%.
Sociodemographic correlates in atypical vs non-atypical depression
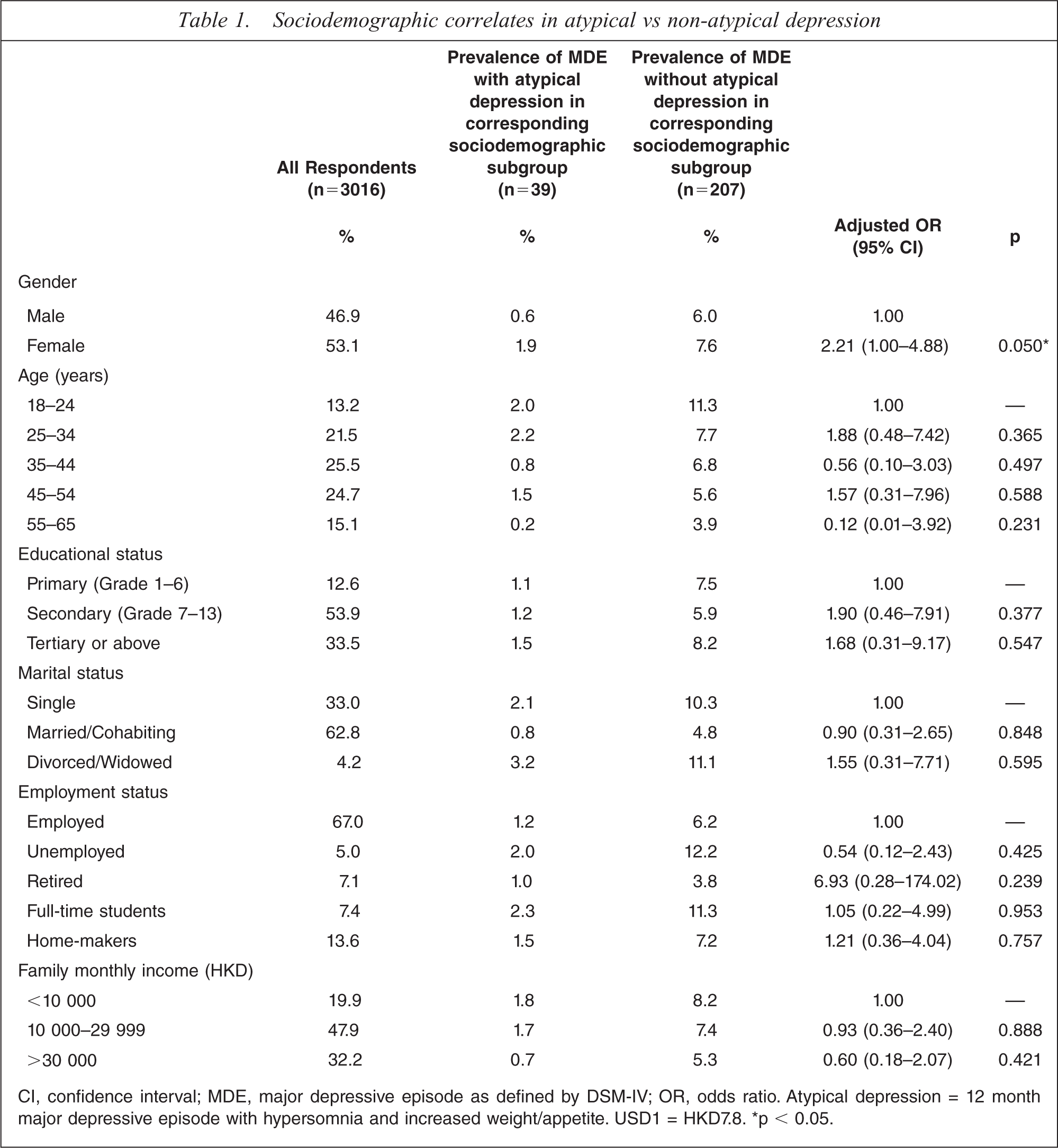
CI, confidence interval; MDE, major depressive episode as defined by DSM-IV; OR, odds ratio. Atypical depression = 12 month major depressive episode with hypersomnia and increased weight/appetite. USD1 = HKD7.8. ∗p < 0.05.
An independent survey research organization, the Hong Kong Institute of Asia-Pacific Studies of the Chinese University of Hong Kong, was commissioned to conduct the survey. The 54 interviewers were university students with 1–3 years of part-time experience in administering telephone survey interviews, including those on mental health. For the purpose of the present study they were given a briefing session to familiarize themselves with the questions and skills for eliciting the symptoms of mood disorders.
Instrument
The telephone questionnaire was devised by a psychiatrist (SL) specializing in mood disorders. It was in Cantonese Chinese, the predominant dialect used in Hong Kong. Its items covered demographic information (i.e. gender, age, educational level, marital status, family monthly income, and employment status), manic/hypomanic and depressive symptoms, family history of mental disorders, suicidal behaviours (i.e. suicidal ideation, plan, and attempt), distress, role impairment, and professional help-seeking behaviour. The symptom items were carefully adapted from the DSM-IV criteria for MDE as well as manic and hypomanic episodes [4]. Based on the same telephone survey, Lee et al. reported that blinded clinical reappraisal interviews using the enhanced version of the Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) [25,26] found generally good concordance between SCID diagnoses and telephone survey classification of 12 month MDE (area under the curve = 0.74) [23].
Fourteen dichotomous yes or no questions to assess the nine DSM-IV symptoms of MDE were asked (see Lee et al. [23] for the list of questions). Four of these nine symptoms are composite and were broken down into two or more questions. We deliberately separated the questions on increased and decreased weight/appetite as well as insomnia and hypersomnia. Increased weight/appetite and hypersomnia (hereafter labelled as atypical symptoms) were also asked of the respondents who endorsed decreased weight/appetite and insomnia. Respondents who answered ‘no’ to both questions on core depressive symptoms were asked to skip the subsequent questions related to the six associated symptoms of MDE except for the three questions on suicidal behaviours.
Another set of 14 dichotomous questions were used to assess the eight symptoms (including the two core symptoms of elevated and irritable mood) listed in the DSM-IV for manic/hypomanic episode because four of these eight symptoms are composite (see Lee et al. [23] for the list of questions). Respondents were asked all of these 14 questions that covered the core and associated symptoms of manic/hypomanic episode. One question on co-occurrence of symptoms (‘Had two or more of the above experiences ever occurred in the same period of time?’) and one on duration of hypomanic symptoms (‘How many days did the longest of these experiences last?’) were then asked.
A question on level of distress associated with the symptoms of MDE was asked at the end of the MDE section with the choices of ‘none’, ‘mild’, ‘moderately severe’, and ‘very severe’. Role impairment was assessed with the Sheehan Disability Scale (SDS) after the MDE section. The SDS measured the degree of interference with four domains of life when MDE symptoms were the most severe. The four domains include household responsibilities, work/school, close relationships, and social life, all of which were rated on a scale of 0–10 (none = 0, mild=1–3, moderate=4–6, severe=7–9 and very severe=10) [27]. The SDS has been widely used in both Western and Chinese community psychiatric surveys [23,28].
Three separate questions were asked to determine whether respondents had sought help for any of the mood symptoms examined or other mood problems from general practitioners, psychiatrists, and clinical psychologists, respectively. The question ‘to the best of your knowledge, had any of your parents, siblings, or relatives been diagnosed with emotional or psychotic illnesses?’ was asked at the end of the survey as a general indicator of family history of mental disorders.
According to the DSM-IV, respondents were classified as having 12 month MDE if he/she (i) reported five or more symptoms in the past 12 months for at least 2 weeks, of which one of them must either be persistently depressed mood or persistent loss of interest/motivation; and (ii) either reported the level of distress as ‘very severe’ or scored ≥7 (severe) on one of the four SDS domain-specific scores.
Respondents who fulfilled the 12 month MDE criteria and endorsed both atypical symptoms (i.e. hypersomnia and increased appetite/weight) were classified as having AD while those who endorsed 0 or 1 atypical symptom were classified as having non-AD. The classifications of lifetime manic and hypomanic episodes were based on DSM-IV criteria. For lifetime soft hypomanic episode, the DSM-IV symptoms of hypomanic episode were present but lasted 2–3 days only. Respondents who fulfilled both lifetime manic episode and 12 month MDE criteria were classified as having 12 month BP-I. Those who fulfilled both lifetime hypomanic episode and 12 month MDE criteria were classified as having 12 month BP-II, while those who fulfilled both lifetime soft hypomanic episode and 12 month MDE criteria were classified as having 12 month soft BP-II [23].
Statistical analysis
The statistical package SPSS 15.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for analyses. Associations between sociodemographic variables and AD were examined using multivariate logistic regression based on a backward stepwise model. Differences in level of distress, level of impairment, number of manic/hypomanic and depressive symptoms, associations with bipolar disorders (i.e. BP-I, BP-II, and soft BP-II), family history of mental disorders, suicidal behaviours (i.e. suicidal ideation, plan, and attempt), and help-seeking behaviour were also examined using logistic regression, ordinal regression, or linear regression while controlling for the demographic variables. Cross-tabulations were used to estimate the percentage of the demographic and clinical variables within AD and non-AD groups. The results were evaluated based on an alpha level of 0.05 of a two-tailed test.
Results
Twelve month prevalence and sociodemographic characteristics
Of the 246 respondents with 12 month MDE (prevalence 5 8.2%) in the whole sample, hypersomnia and increased weight/appetite were reported by 36.2% and 30.1%, respectively. A total of 34.6% of respondents had only one atypical symptom while 15.9% of respondents had both atypical symptoms. The 12 month prevalence of AD was 1.3%.
On multivariate logistic regression it was found that respondents with AD, versus non-AD, were more likely to be female (Table 1). No statistically significant differences between those with AD and non-AD were found in age, education, marital status, employment status, or family monthly income.
Clinical characteristics of AD and non-AD
In a multivariate model adjusting for the aforementioned demographic variables, respondents with AD had a significantly greater number of manic/hypomanic symptoms (5.43) than those with non-AD (4.61; β = 0.883, 95% confidence interval (CI) = 0.322–1.444, p < 0.001). AD respondents also had a significantly greater number of MDE symptoms (7.94) than non-AD respondents (7.09; β = 0.749, 95%CI = 0.303–1.194, p < 0.001).
Respondents with AD (32.9%) were more likely to have soft BP-II than those with non-AD (19.8%) at a trend level (p = 0.08) while similar proportions of BP-I and BP-II were found in the two groups (Table 2).
Clinical correlates in atypical vs non-atypical depression
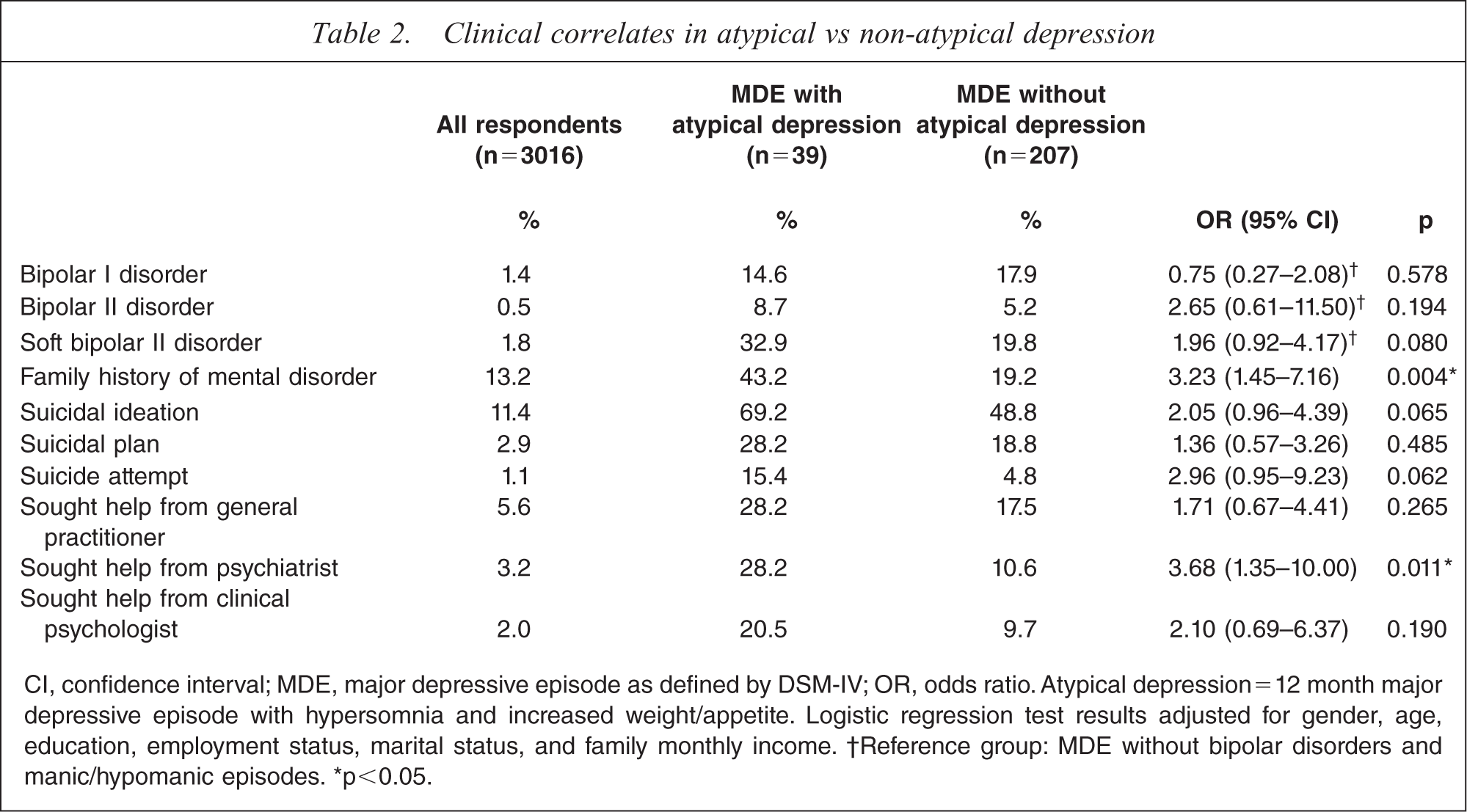
CI, confidence interval; MDE, major depressive episode as defined by DSM-IV; OR, odds ratio. Atypical depression = 12 month major depressive episode with hypersomnia and increased weight/appetite. Logistic regression test results adjusted for gender, age, education, employment status, marital status, and family monthly income.
† Reference group: MDE without bipolar disorders and manic/hypomanic episodes. ∗p<0.05.
Respondents with AD had approximately threefold the odds of reporting a family history of mental disorder (43.2%) than those with non-AD (19.2%; odds ratio (OR) = 3.23, p = 0.004). There is a trend for respondents with AD to exhibit higher odds of suicidal ideation (69.2% vs 48.8%; OR=2.05, p = 0.065) and suicide attempt (15.4% vs 4.8%; OR=2.96, p = 0.062) than those with non-AD.
Respondents with AD were significantly more likely to have sought help from psychiatrists for depressive or manic/hypomanic symptoms or other mood problems (28.2%) than those without AD (10.6%; OR=3.42, p = 0.026). By contrast, the two groups did not show significant difference in help-seeking from general practitioners and clinical psychologists (Table 2).
Among those with non-AD, 36.7% and 48.8% reported severe and moderate distress attributed to MDE symptoms, respectively. For those with AD, 35.9% and 38.5% reported severe and moderate distress attributed to MDE symptoms, respectively. In a multivariate ordinal regression model adjusting for the demographic variables, level of distress was not significantly associated with AD (OR=−0.369, 95%CI = −1.056–0.318, p = 0.293).
Table 3 lists the mean total scores and domain-specific scores of the SDS. After adjusting for demographic variables, all of the role impairment scores were not significantly different between the AD and non-AD groups.
Role impairment in atypical vs non-atypical depression
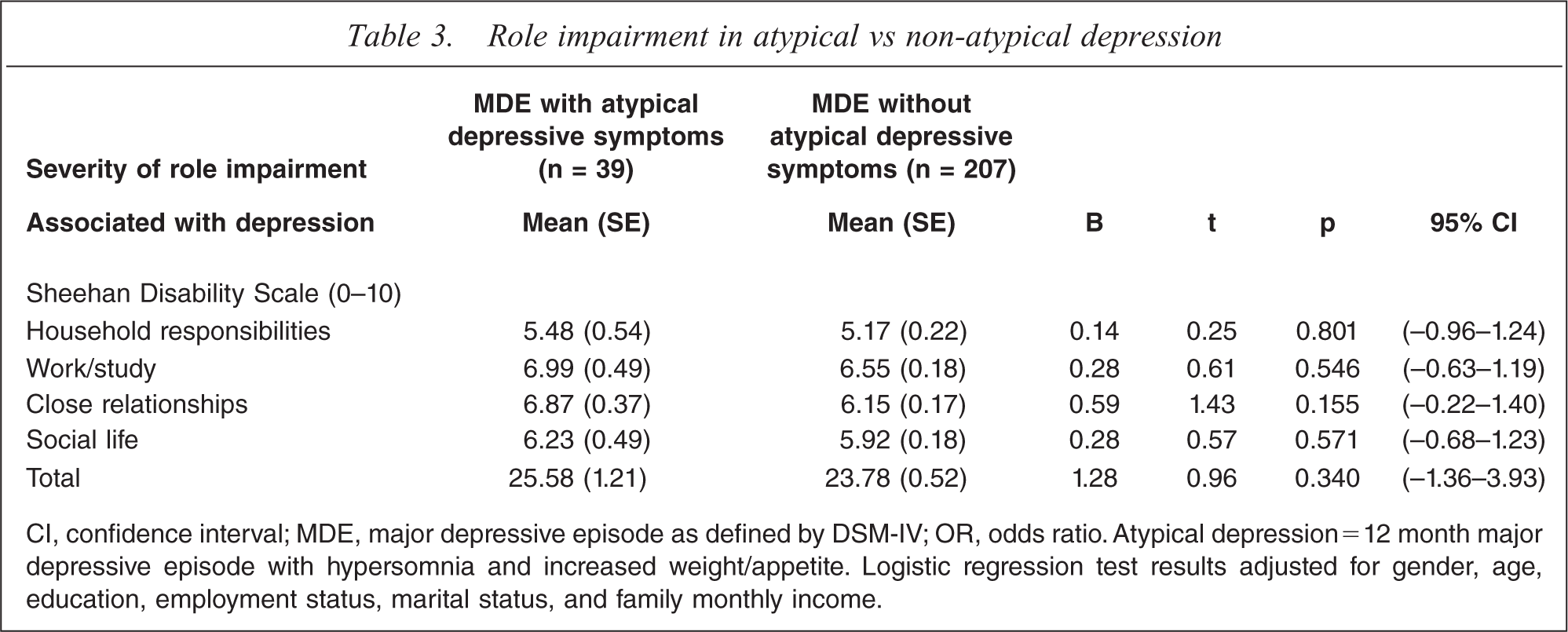
CI, confidence interval; MDE, major depressive episode as defined by DSM-IV; OR, odds ratio. Atypical depression = 12 month major depressive episode with hypersomnia and increased weight/appetite. Logistic regression test results adjusted for gender, age, education, employment status, marital status, and family monthly income.
Discussion
Prevalence estimates of AD
Consistent with previous Western community studies that used the same definition of AD [15,16], approximately half of the respondents with 12 month MDE endorsed one or both of the atypical depressive symptoms. This suggested that it is cross-nationally common for these symptoms to co-occur among those having MDE. The present finding of a 12 month prevalence of 1.3% for AD is also consistent with estimates of lifetime prevalence of AD in other studies using the same definition (0.7–2.0%) [15,16,18]. It confirmed that AD was less common than non-AD in the community. The prevalence reported here is lower than those found in community studies that used a broader definition of AD [20,22]. This is more likely to reflect our failure to measure the other three DSM-IV characteristics of AD than substantive cross-cultural differences because our prevalence estimate is consistent with other studies using the same definition of AD.
The 12 month prevalence of MDE found in the present study (8.2%) was relatively high but within the range found in Western community surveys [29–31]. A remarkably similar estimate (8.4%) was found in a previous local survey based on an identical methodology [32]. These estimates were much higher than those found in Hong Kong more than two decades ago [33] but tallied with recent epidemiological evidence that depression in Chinese communities is considerably more common than previously thought [34]. Although concordance studies using clinician-administered semi-structured interviews and rating scales generally supported the telephone-based methodology [23,35–38], methodological differences in addition to substantive factors almost certainly contributed to the increase in prevalence estimates of depression in Chinese communities [39].
Sociodemographic profile of AD versus non-AD
Consistent with most previous studies [6,7,10,17,20,22], female gender was found to be proportionately higher among respondents with AD. Some [7,15,17] but not all [19] studies reported that younger age was associated with AD. Although we did not find age to be significantly associated with AD, there appeared to be a decrease in the older age group. Future research should examine whether there is a curvilinear relationship that prevents a single associational relationship with age from being identified. The lack of significant differences between AD and non-AD regarding educational level, marital status and socioeconomic status was consistent with other studies [6,15,17,19].
Clinical profile of AD versus non-AD
Previous studies suggested a connection between bipolar disorders and AD in several ways. They found a significantly higher proportion of AD in BP-II compared to major depressive disorder (MDD) [21,40], a greater number of AD symptoms in bipolar disorders versus MDD [21,41–43], a moderately high positive predictive value of AD for BP-II (71.7%), a dose–response relationship between the number of AD symptoms and bipolar family history, and a significant relationship between depressive mixed states and AD [7,21,40].
The present findings were supportive of the association between AD and bipolar disorders. First, the average number of manic/hypomanic symptoms and MDE symptoms was significantly higher among respondents with AD when compared to those with non-AD [20,22]. This not only indicated that those with AD might be associated with a greater severity of mood episodes but also suggested a connection between AD and bipolar spectrum disorders [7]. Second, although only at a trend level, a larger proportion of respondents with AD than non-AD had soft BP-II(AD, 32.9%vsnon-AD, 19.8%) [7,10,20,22]. We also confirmed that BP-I and BP-II were similarly common among the AD and non-AD groups [17,18]. Third, respondents with AD were more likely to report a family history of mental disorder than those with non-AD [7,10,17,20].
Respondents with AD had a tendency to report more suicidality. Previous community studies on AD and suicidal behaviours were, unlike those on bipolar disorders [44], inconclusive [17,20,22]. To our knowledge no study has examined the relationship between AD and all three kinds of suicidal behaviours. Our finding of suicidal ideation and suicide attempt being correlated with AD at a trend level should motivate further studies using more sophisticated ways of assessing suicidality and AD [45].
Although the overall lack of difference in help-seeking behavior between respondents with AD and non-AD was consistent with previous studies [8,10,16,20], Angst et al. found increased treatment rates among those with AD [22]. In the present study respondents with AD were more likely to have sought help from psychiatrists but not general practitioners or clinical psychologists. This might be because of the greater severity of AD, which called for specialist psychiatric treatment.
Limitations
Several limitations should be considered when interpreting the present findings. Our definition of AD was the same as those used in most Western community surveys [4,23,24]. It is, however, strictly speaking, an epidemiological proxy of atypical depression diagnosed by clinicians in accordance with the DSM-IV, which describes other characteristics of AD, including the multi-dimensional trait construct of interpersonal rejection sensitivity [4]. Comparison between community studies such as the present one and those in which AD was diagnosed by clinicians using DSM-IV criteria should therefore be made with this discrepancy in mind [6–8,10,11]. Because the validity of AD and different combinations of atypical symptoms has not been fully established [22], we believe that both community and clinical studies with somewhat different definitions of AD are useful at this stage of research. Future community surveys may devise ways of operationalizing other atypical symptoms so that they can be validly assessed by lay interviewers and be convergently analysed with regard to a comprehensive set of external validators. Another limitation to note is that in order to lower the refusal rate, telephone interviews had to be brief. Consequently, we did not collect detailed information on comorbidity, frequency and persistence of MDE, age of onset, or family psychiatric history. Future studies should assess the presence of the specific types of mental disorders among family members in order to identify any dose–response relationships between atypical symptoms and bipolar family history or other patterns of familial associations [7]. We examined only 12 month MDE, which might not reflect other syndromal presentations of depression throughout life. Thus, the present estimate of the prevalence of AD might be conservative. Finally, we did not obtain drug treatment data that might shed light on how psychotropics affected the symptoms of hypersomnia and increased weight/appetite.
Conclusion
The present findings confirmed our a priori hypotheses and most Western research findings on AD. They also suggested that AD might be closer to bipolar spectrum disorders than non-AD. AD, however, still resembled non-AD in terms of its overall syndromal structure, levels of distress, impairment and possibly response to treatment. As postulated by Akiskal and Benazzi, BP-I and MDD, which lie on the opposite ends of a spectrum, are more likely to exhibit differences while disorders in between are more likely to resemble one another [40]. The view that unipolar and bipolar depressions lie on a spectrum of polarity bridged by AD was also supported by a lack of bimodal distribution of the number of AD symptoms between patients with BP-II and MDD in clinical studies [7,40]. These findings and the intriguing ideas they raise need to be further examined in community samples in which disorders are more representative and likely to distribute dimensionally than in clinical samples. Family aggregation, risk factors and treatment response studies are also needed to further examine the disease validity of depression with reference to a spectrum of atypical symptoms [14].