
Abstract
Australia's first National Survey of Mental Health and Wellbeing (NSMHWB), carried out in 1997, found that around one in four young people aged 18–24 years had a mental health problem, with affective, anxiety and substance use disorders being the most commonly reported conditions [1]. Despite the availability of effective interventions for these disorders, many young people either do not seek, or delay seeking, treatment [2]. This is particularly notable in the primary care sector, with few young people viewing general practitioners (GPs) as a source of help for mental health problems [3]. Such delays in accessing professional help can significantly affect social, educational and vocational outcomes, and may even have lifelong consequences [4].
Young people are more likely to access services when they recognize that they have a mental health problem and know how to seek help [5]. Supportive social influences also play a key role [6]. However, available data do not inform us as to whether help-seeking behaviours among young people differ across disorders, which is critical in terms of planning suitable service responses, with particular implications for primary care.
In 2007, a second NSMHWB was conducted, with the survey population extended to cover those over 16 years of age (as compared to 18 in the previous survey). More detailed data on service utilization was also collected. Initial findings from the survey indicate that young people aged 16–24 years have the highest prevalence of mental disorders, but the lowest rate of receiving services in the previous 12 months [7]. The rate of service use was particularly low for young men, with only 13.2% of those with a mental disorder receiving services despite a 12-month prevalence rate of 22.8%. The aim of this paper is to provide a more detailed analysis of the relationship between type and severity of mental disorders (depression, anxiety and substance misuse) and help-seeking in those aged 16–24 years compared to participants aged 25–44 and 45–85 years.
Methods
The 2007 NSMHWB data were obtained from the Australian Bureau of Statistics (ABS) in the form of a confidentialized unit record dataset. Survey interviews were conducted between August and December 2007 with participants randomly selected from a stratified, multi-stage area probability sample of households, excluding very remote regions. The population in scope were persons aged 16–85 years and usual residents of private dwellings, with those aged 16–24 and 65–85 having a higher probability of being selected to ensure the reliability of estimates for these age groups. Of 14 805 eligible participants, 8841 completed the interview, representing a response rate of 60% [8].
The survey instrument was based on the current version of the World Mental Health Composite International Diagnostic Interview (WMH-CIDI 3.0), which uses both DSM-IV and ICD-10 criteria to diagnose lifetime, 12-month and 30-day mental health disorders. The focus of data collection was on high prevalence mental disorders. These were anxiety disorders (i.e. panic disorder, agoraphobia, social phobia, generalized anxiety disorder, obsessive–compulsive disorder and post-traumatic disorder), affective disorders (i.e. depressive episode, dysthymia and bipolar affective disorder) and substance use disorders (i.e. alcohol harmful use, alcohol dependence, and drug harmful use and drug dependence for four drug classes: cannabinoids, opioids, sedatives and stimulants). The current paper focuses on the ICD-10 diagnoses and the 12-month prevalence of these three main classes of mental disorder.
For individuals diagnosed with a 12-month mental disorder, the severity of impairment was also classified into three categories: severe, moderate and mild. This severity measure provides an indication of the average impairment of individuals with specific mental disorders, and takes into account co-morbidity. Those individuals classified as severe, in addition to a 12-month mental disorder, must have had one of the following occur in the preceding 12 months: an episode of mania, a suicide attempt, at least two areas of severe role impairment on the Sheehan Disability Scales, or an overall functional impairment consistent with a Global Assessment of Functioning score of 50 or less. Individuals were classified as moderate if they had a 12-month mental disorder and were not classified as severe, and reported at least moderate interference on any Sheehan Disability Scale. The remaining individuals with a 12-month mental disorder were classified as mild. A more detailed description of the severity measure has been reported elsewhere [7,8]. For the analyses in this paper we used the Australian version of the ICD-10 severity measure.
Data collection on mental health service use was a major component of the 2007 NSMHWB. We used three overlapping categories of service use: (i) any mental health service use, which includes general practitioners (GPs), mental health professionals (MHPs) (i.e. psychiatrists, psychologists, mental health nurses, and other professionals that provide specialist mental health services, e.g. social workers, counsellors and occupational therapists), specialist doctors/surgeons and complementary/alternative therapists; (ii) consultations with GPs; and (iii) consultations with MHPs.
Age was categorized into three groups: 16–24, 25–44, and 45–85. While the primary focus is on the 16–24-year-olds, these categories were used in order to capture some information about the age distribution of 12-month mental health disorders. For the analyses in this paper, a more detailed age category breakdown was not possible due to the relatively small number of cases in older age groups with 12-month CIDI-diagnosed mental disorders.
To take into account the complex sample design and weighting of the NSMHWB, the standard errors of prevalence estimates and odds ratios, along with their 95% confidence intervals, were calculated using the delete-a-group Jackknife method of replication in 60 replicate groups [8]. We calculated the prevalence of 12-month mental disorders and the severity of impairment. We also calculated the prevalence of any 12-month service use and consultations with GPs and MHPs for those with a 12-month mental disorder by age group and sex. Finally, three separate logistic regression models were generated for 12-month service use: 1) the use of any service, 2) the use of GP services, and 3) the use of MHP services as outcomes, with 12-month disorders by age category interactions as predictors of the use of these services, controlling for sex. All analyses were performed with Stata Release 10.
Results
Analysis of the data from the 2007 NSMHWB revealed that more than one in four Australians aged between 16 and 24 experienced a mental disorder in the preceding 12 months (26.4%, 95%CI = 23.6–29.1%) (see Table 1). This compared to one in five (20.0%, 95%CI = 18.9–21.1%) in those aged between 16 and 85 years, and was largely driven by the higher prevalence of substance use disorders in the 16–24 age group (16–24: 12.7% 95%CI = 10.7–14.7% vs 25–44: 5.9% 95%CI = 4.5–7.3% vs 45–85: 2% 95%CI = 1.3–2.7%). Harmful use of alcohol was the most common substance use disorder in those aged 16–24 years, with a prevalence of 8.6% (95%CI = 6.8–10.3%) (results not shown in the table). Prevalence rates for anxiety and affective disorders were not significantly different between the 16–24 and 25–44 age groups. Prevalence rates for anxiety disorders were higher in the 25–44 age group compared to the 45–85 age group (25–44: 17.3%, 95%CI = 15.1–19.4% vs 45–85: 11.8%, 95%CI = 10.5–13.2%), and this was also true for affective disorders (25–44: 8.1%, 95%CI = 6.8–9.4% vs 45–85: 4.7%, 95%CI = 3.7–5.7%).
The prevalence of CIDI diagnosed 12-month mental disorders by age and sex
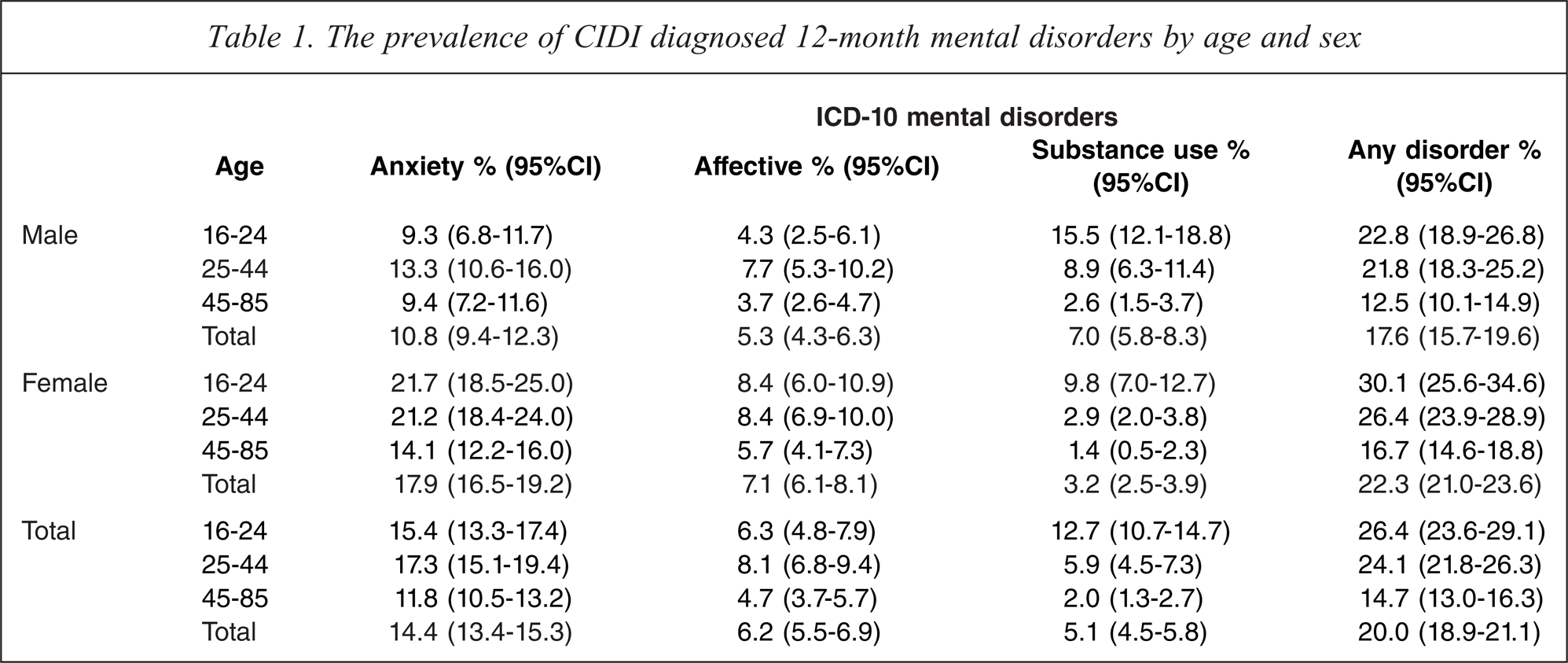
All cases with a 12-month mental disorder were classified as severe, moderate or mild. Overall, the highest prevalence of severe disorders was for those diagnosed with affective disorders, followed by anxiety and substance use disorders (51.5%, CI = 45.2–56.9%, 22.2%, CI = 18.5–25.9%, and 20.4%, CI = 14.8–26% respectively). The highest prevalence for mild disorders was for those diagnosed with substance use disorders, followed by anxiety and affective disorders (54.6%, CI = 47.5–61.7%, 43.8%, CI = 39.3–48.3%, and 10.2%, CI = 6.1–14.2% respectively). These patterns did not significantly vary by age and sex across the mental disorders, with the exception of substance use disorders for 16–24-year-old males, who had a significantly lower prevalence of severe disorders compared to 25–44-year-old males (8.7%, CI = 4.0–13.3% vs 28.9%, CI = 13.7–44.0%) (results not shown in the table).
Figures 1 to 3 show the 12-month prevalence of any service use, consultations with GPs and MHPs respectively for people with 12-month mental disorders by age category and sex. Figure 1 shows that, while there were no significant differences in the prevalence of any 12-month service use for 12-month anxiety or affective disorders across the age groups, the 16–24-year-old age group had a significantly lower prevalence of 12-month service use for 12-month substance use disorders compared to the 25–44-year-old age group (males: 7%, CI = 3.8–12.7% vs 27.4, CI = 15.8–43.3%, females: 18.1%, CI = 9.7–31.3% vs 52.4%, CI = 37–67.4% respectively), which also appears to have driven the significantly lower prevalence of any 12-month service use for any 12-month mental disorder in this age group compared to the older age groups (23.3%, CI = 18.4–29%. vs 36.9%, CI = 32.1–41.9% and 39.4%, CI = 32.8–46.5% respectively). Examination of Figures 2 and 3 reveals that, while there was no significant difference in the 12-month prevalence of service use for anxiety or affective disorders across the age groups for GP and MHP services, the figures show that the age group differences evident in Figure 1 were largely driven by the significantly lower prevalence of 12-month consultations with GPs for any 12-month mental disorder by the 16–24 year olds compared to the older age groups (males: 7.5%, CI = 4.2–13.1% vs 20.7%, CI = 14.6–28.5% and 21.3%, CI = 14.1–30.8% respectively; females: 20.2%, CI = 15–26.6% vs 33%, CI = 27.7–38.8%, Figure 2), and the significantly lower prevalence of 12-month consultations with MHPs for substance use disorders by 16–24-year-old males compared to 25–44-year-old males (4.4%%, CI = 1.8–10.4% vs 23%, CI = 12.4–38.8%, Figure 3).
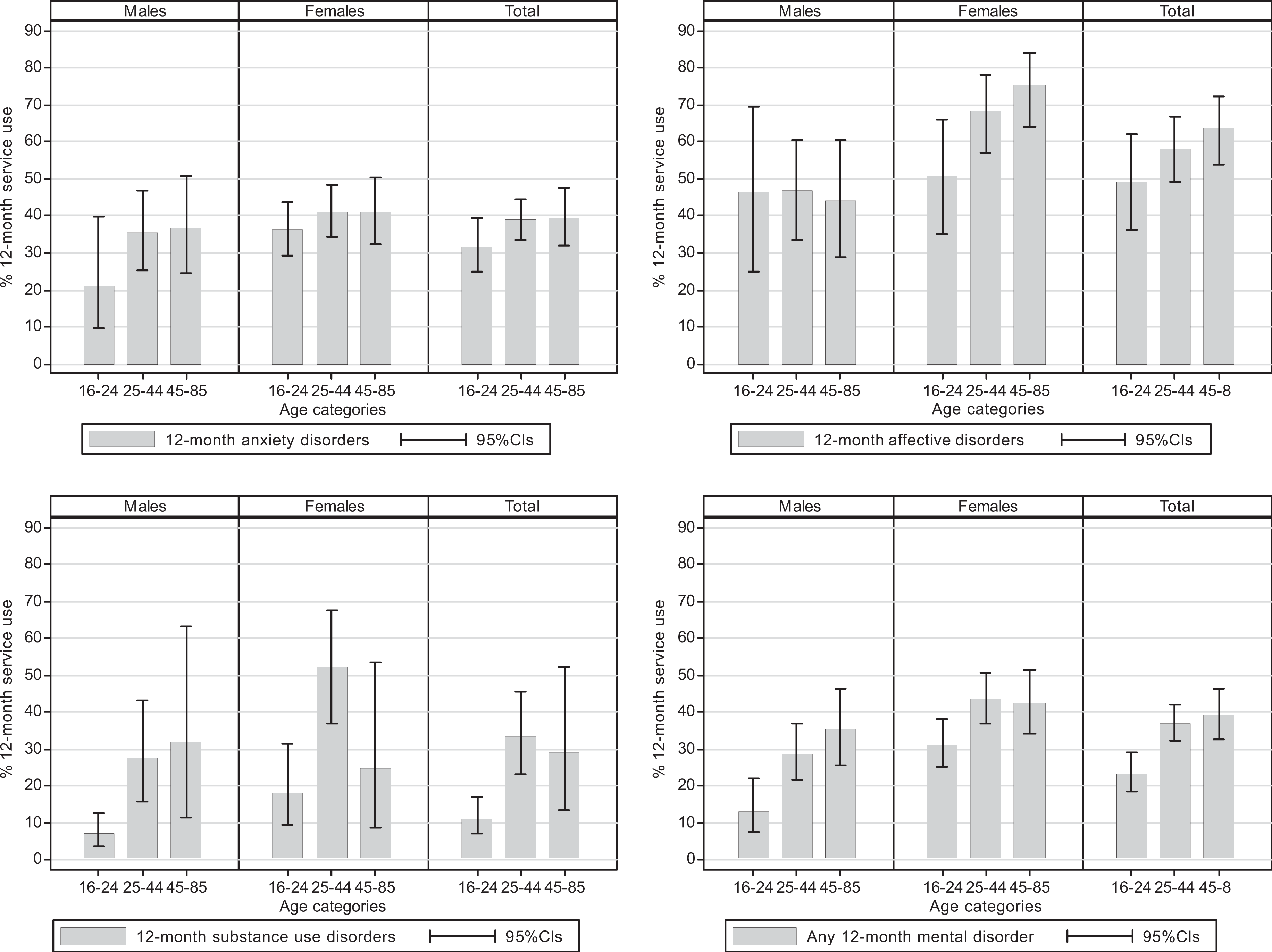
Any mental health service use in the past 12-months for 12-month CIDI diagnosed mental disorders by age and sex.
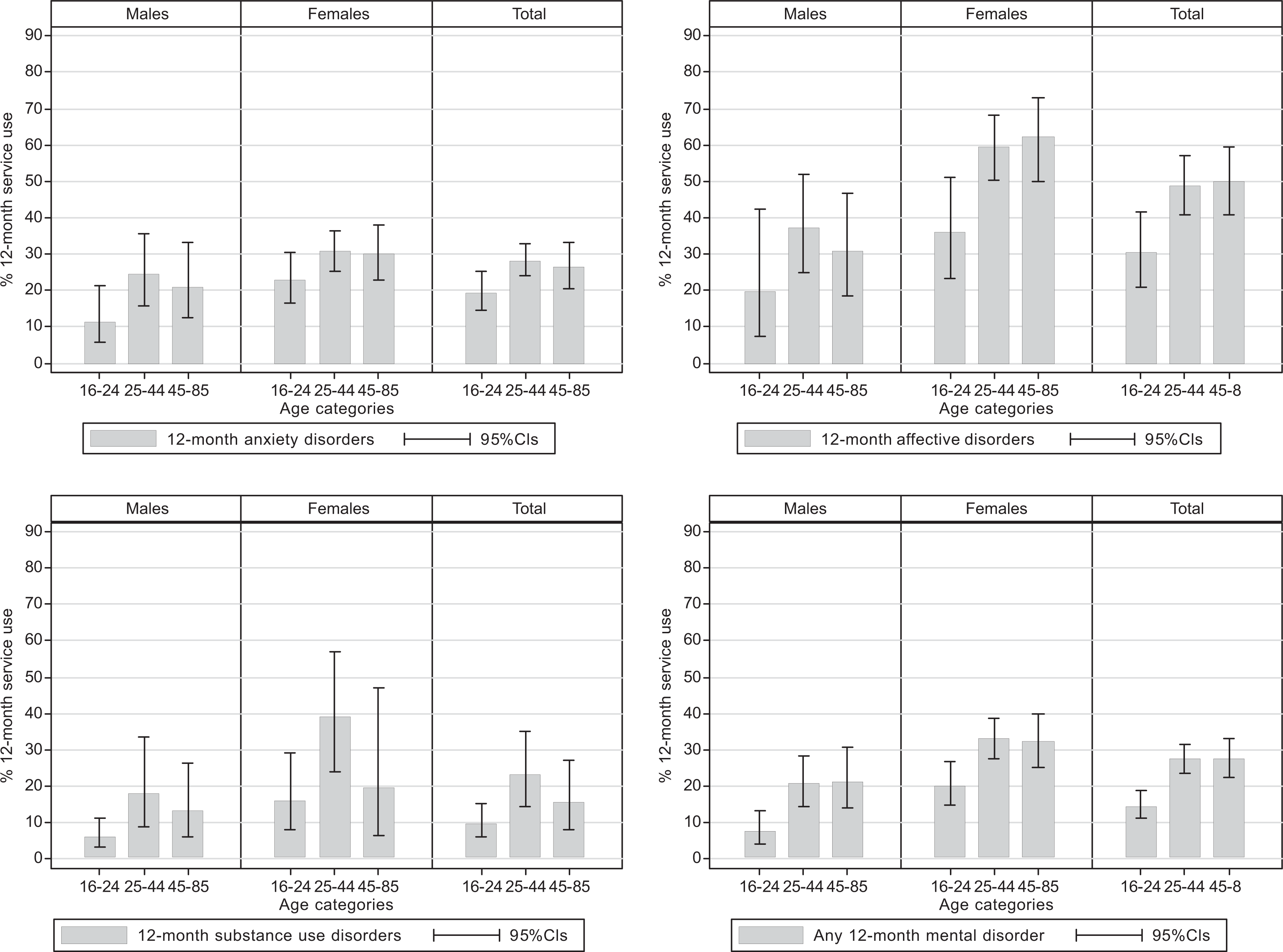
Consultations with GPs in the past 12 months for 12-month CIDI-diagnosed mental disorders by age and sex.
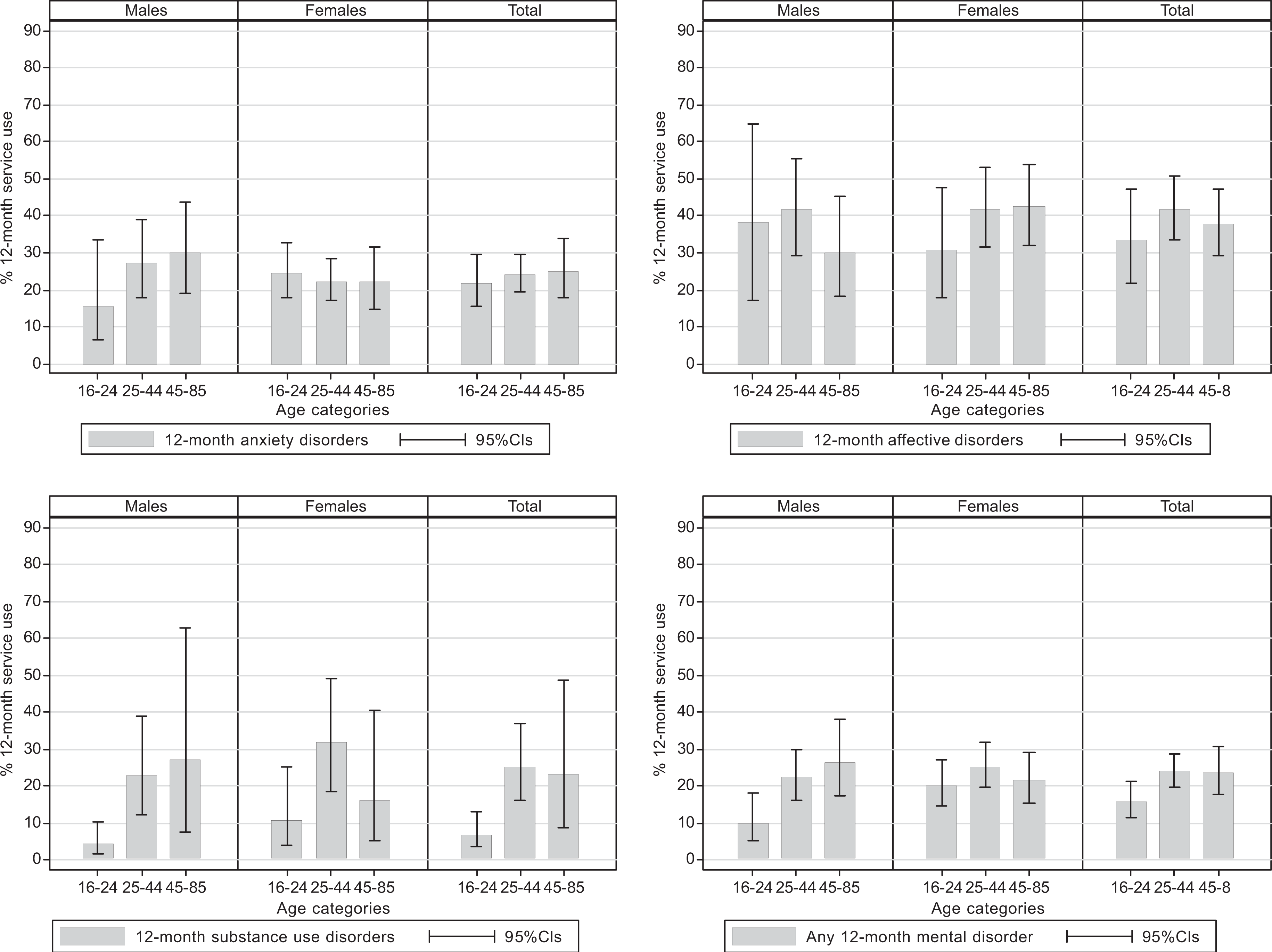
Consultations with mental health professionals in the past 12 months for 12-month CIDI-diagnosed mental disorders by age and sex.
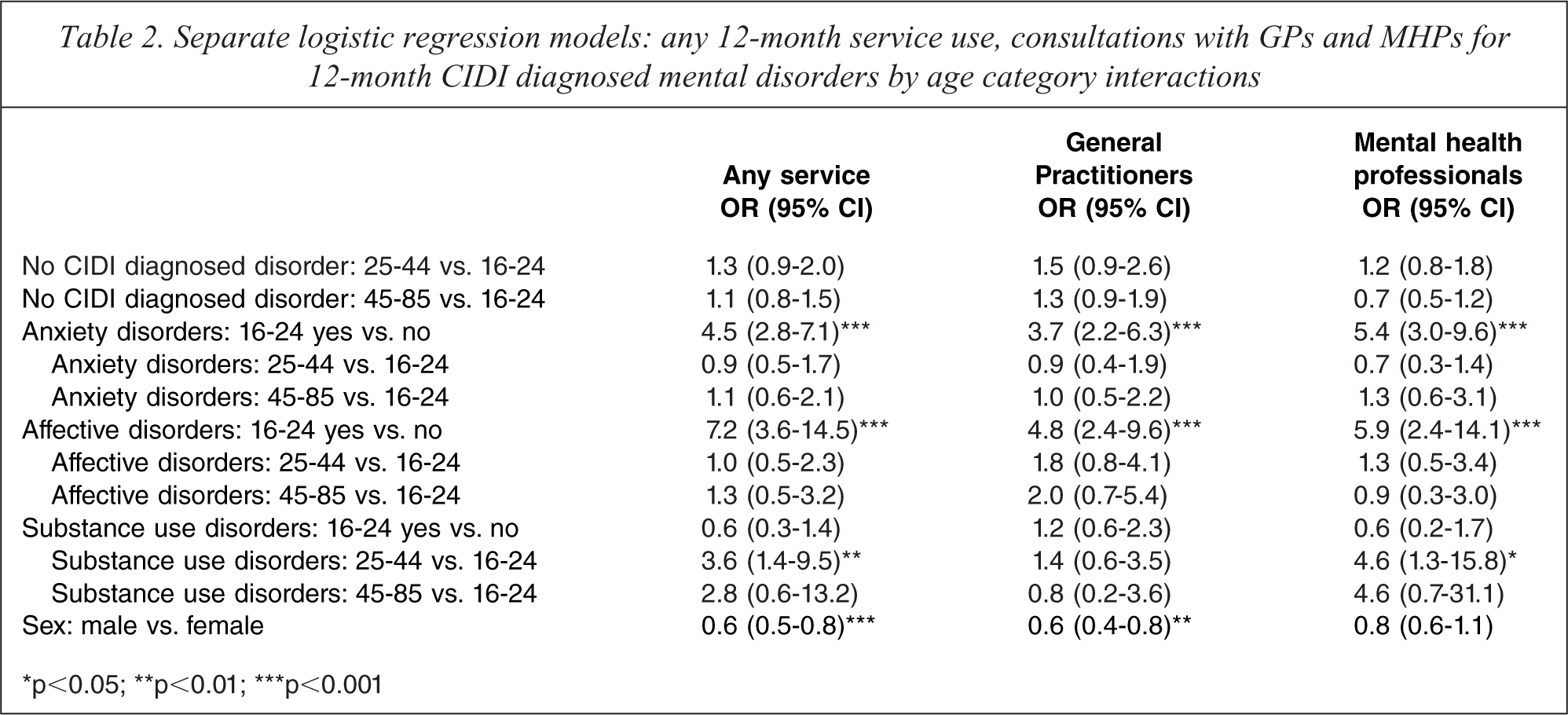
The lower prevalence of service use by the 16–24-year-old age group for substance use disorders may have been the result of a lower level of co-morbidity and, therefore, severity compared to the 25–44-year-old age group. To adjust for the potential confounding effect of co-morbidity on the relative level of service use by the age groups, three logistic regression models were generated: 1) the use of any 12-month service, 2) the use of GP services, and 3) the use of MHP services as outcomes, with 12-month disorder by age category interactions as predictors of the use of these services, controlling for sex (Table 2). The results show that 16–24 year olds with an anxiety or affective disorder had significantly higher odds of service use across the service types than 16–24 year olds without these disorders (any mental health service use: OR = 4.5, 95%CI = 2.8–7.1 and OR = 7.2, 95%CI = 3.6–14.5; consultations with GPs: OR = 3.7, 95%CI = 2.2–6.3 and OR = 4.8, 95%CI = 2.4–9.6; and consultations with MHPs: OR = 5.4, 95%CI = 3.0–9.6 and OR = 5.9, 95%CI = 2.4–14.1 respectively). However, there was no statistically significant difference in the odds of service use for the 16–24-year-old age group between those with and those without a substance use disorder. Comparisons with the older age groups revealed that, while there was no statistically significant difference in service use across the service types for anxiety or affective disorders between the 16–24-year-old age group and the older age groups, the 25–44-year-old age group had significantly higher odds of consulting MHPs or using any mental health service generally for substance use disorders compared to the 16–24-year-old age group (OR = 4.6, 95%CI = 1.3–15.8 and OR = 3.6, 95%CI = 1.4–9.5 respectively).
Separate logistic regression models: any 12-month service use, consultations with GPs and MHPs for 12-month CIDI diagnosed mental disorders by age category interactions
∗p<0.05; ∗∗p<0.01; ∗∗∗p<0.001
Discussion
Findings from the 2007 NSMHWB demonstrate that young people aged 16–24 years are disproportionately affected by mental disorders, with more than one in four experiencing symptoms of an anxiety, affective or substance use disorder in the past 12 months. Service use was also lower in those aged 16–24 years compared with other age groups, with less than one in four of those with a mental disorder accessing health services in the previous 12 months. This gap in general help-seeking was primarily related to higher rates of substance use disorders and a lower level of severity in this age group. In young men, the prevalence of substance use disorders, particularly harmful use of alcohol, was higher than other disorders, and rates of service use were particularly low. In contrast, we found no evidence of lower rates of help-seeking for anxiety and affective disorders among those aged 16–24 years.
Australian National Health Surveys have shown that levels of risky drinking in those aged 18–24 have increased since 1995 [9]. There is also evidence that rates of alcohol-related harm in young people have increased significantly over recent years [10]. However, despite higher rates of harmful use, young people are less likely to be concerned about alcohol misuse, with 26% of those aged 14–19 nominating alcohol as the form of drug use of most serious concern, compared to 32% of the general population. Many young people consider that the benefits of drinking alcohol outweigh the risks and often view excessive alcohol consumption as part of the rite of passage into adulthood [11,12]. Young people commonly underestimate the harms associated with high-risk drinking. For example, the 2007 National Drug Strategy Household Survey found that around 23% of males (aged 14 or over) who drank at risky levels thought that an adult male could drink seven or more standard drinks without putting his health at risk [13]. Such views may go some way to explaining the relatively low levels of help-seeking for alcohol disorders in 16–24 year olds.
While there has been a greater emphasis on early, effective intervention for young people in recent years, this has largely focused on the treatment of mental health problems, such as anxiety and depression. Although there is good evidence that brief interventions delivered within primary care are effective in reducing excessive drinking [14], use of such interventions is not widespread, and a number of barriers to their implementation have been identified. These include time, cost and lack of knowledge about early phase heavy drinking and how to implement such interventions [15–17].
Given that young people with 12-month affective disorders are almost five times more likely than those without these disorders to visit a GP, there is an opportunity to identify co-occurring alcohol problems in this particularly vulnerable population [18]. However, one recent study found that GPs do not readily identify co-occurring alcohol misuse in young people with depression [19]. Such findings highlight the need for better coordination and integration of mental health and alcohol and drug services within primary care settings.
While improvement in the identification and treatment of harmful drinking within primary care may be beneficial for young people who access such services, less than 10% of all GP visits are by those aged between 15 and 24 [20]. Thus, a large number of young people who drink at risky levels do not engage with health services for any health problems. Consideration should therefore be given to policies and programmes that might improve help-seeking for substance use disorders, particularly among young men. Research suggests that attention should be focused on interventions that limit the supply of alcohol, tackle erroneous beliefs about alcohol and related harms, improve overall mental health literacy, facilitate emotional competence (particularly in young men) and improve supportive social influences [6,21].
Help-seeking for affective disorders is more common than for other mental disorders in both young men and women, likely reflecting the greater numbers reporting severe disorders and possibly the effects of health promotion campaigns such as those run by ‘beyondblue: the national depression initiative’ [22]. Given the relatively large number of those with mild anxiety and substance use disorders, health promotion campaigns could play a role in tackling the large unmet need for treatment without overly burdening clinical resources [23]. Online interventions for harmful drinking may also have a role to play [24].
Conclusions
Findings from the 2007 NSMHWB show that the gap in help-seeking in young people with mental health problems is largely due to high rates of substance use disorders and the low rates of help-seeking associated with these. In order to address this gap, there is a need for better coordination and integration of mental health and alcohol and drug services within primary care settings. Further, given that over half of those with substance use disorders in the 16–24-year-old age group were classified as having mild disorders, population health approaches are also needed, including those that tackle erroneous beliefs about alcohol consumption and related harms, and improve overall mental health literacy.
Footnotes
Acknowledgements