
Abstract
Objectives:
Timely and accurate assessments of disease burden are essential for developing effective national health policies. We used the Global Burden of Disease Study 2015 to examine burden due to mental and substance use disorders in Australia.
Methods:
For each of the 20 mental and substance use disorders included in Global Burden of Disease Study 2015, systematic reviews of epidemiological data were conducted, and data modelled using a Bayesian meta-regression tool to produce prevalence estimates by age, sex, geography and year. Prevalence for each disorder was then combined with a disorder-specific disability weight to give years lived with disability, as a measure of non-fatal burden. Fatal burden was measured as years of life lost due to premature mortality which were calculated by combining the number of deaths due to a disorder with the life expectancy remaining at the time of death. Disability-adjusted life years were calculated by summing years lived with disability and years of life lost to give a measure of total burden. Uncertainty was calculated around all burden estimates.
Results:
Mental and substance use disorders were the leading cause of non-fatal burden in Australia in 2015, explaining 24.3% of total years lived with disability, and were the second leading cause of total burden, accounting for 14.6% of total disability-adjusted life years. There was no significant change in the age-standardised disability-adjusted life year rates for mental and substance use disorders from 1990 to 2015.
Conclusion:
Global Burden of Disease Study 2015 found that mental and substance use disorders were leading contributors to disease burden in Australia. Despite several decades of national reform, the burden of mental and substance use disorders remained largely unchanged between 1990 and 2015. To reduce this burden, effective population-level preventions strategies are required in addition to effective interventions of sufficient duration and coverage.
Introduction
Mental and substance use disorders (MSDs) are a major public health concern, both in across the globe (Whiteford et al., 2013) and in Australia. Australia has experienced a major transition in the public health response to MSDs since the 1993 National Mental Health Strategy and the 1985 Campaign Against Drug Abuse with a focus on prevention (including supply and demand reduction for drug use disorders), promotion of mental health, partnerships between health and other agencies (including welfare and housing agencies) and improvement of services and harm reduction. However, while services have been expanded and reorganised in response to ongoing policy reform, previous research failed to find evidence of diminishing prevalence for most MSDs in Australia (Jorm et al., 2017).
Timely and accurate data on the epidemiology and population-level impact of MSDs are necessary for the successful implementation of the upcoming Fifth National Mental Health Plan (Department of Health, 2016) and National Drug Strategy 2016–2025 (Australian Government, 2015). For example AIHW (2016) and the Australian Burden of Disease Study (2011) estimated the burden of 188 causes (including MSDs) for 2003 and 2011, further disaggregated into subnational estimates by state and territories, indigenous status, remoteness and socioeconomic status. However, policy changes and initiatives generally take several years to have an impact, and burden estimates, generated using consistent methodology, are needed across an extended period to detect change. Furthermore, country-level burden of disease studies do not provide a platform on which to benchmark Australia against other countries in terms of health or improvement over time due to confounding variations in methodology.
Historically, the Global Burden of Disease Study (GBD) played an important role in highlighting the disability burden of mental health disorders through their use of disability-adjusted life years (DALYs) rather than just life years lost/deaths, which previously was largely unrecognised in debates about public health priorities (Lopez and Murray, 1998). To date, the GBD 2015 is the largest and most comprehensive effort conducted to quantify the burden of 315 diseases and injuries across 195 countries, age group of 20 years, both sexes and 5-year intervals beginning in 1990 (Kassebaum et al., 2016). Consistent methodology is applied across GBD, and findings are re-estimated with every new iteration to ensure comparability across time and location. As such, the study enables the investigation of trends over time as well as comparisons between and within countries. In this paper, we use the methodology and the findings of GBD 2015 to report on the burden of MSDs in Australia in 2015 with reference to changes since 1990. We analyse the relative contributions of different MSDs to total burden and explore variations by age and sex.
Methods
GBD 2015 measured burden in terms of DALYs, years lived with disability (YLDs), and years of life lost (YLLs) due to premature mortality. Burden was estimated for 195 countries, age group of 20 years, both sexes and at 5-year intervals beginning in 1990. Corresponding 95% uncertainty intervals (UIs), which is a composite measure to compound uncertainty at different stages of the analysis, were calculated for all estimates. The methodology has been described comprehensively elsewhere (Kassebaum et al., 2016; Vos et al., 2016; Wang et al., 2016) and is summarised below.
Case definitions
The definitions of MSDs followed the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text revision; DSM-IV-TR; American Psychiatric Association, 2000) and the International Classification of Diseases (ICD-10; World Health Organization, 1993). The MSDs included in GBD 2015 were depressive disorders (major depressive disorder [MDD], dysthymia), anxiety disorders, drug dependence (opioid dependence, amphetamine dependence, cocaine dependence, cannabis dependence, other drug dependence), schizophrenia, bipolar disorder, alcohol use disorders (alcohol dependence and fetal alcohol syndrome [FAS]), autism spectrum disorders (ASDs; autism, Asperger’s syndrome and other ASDs), conduct disorder, eating disorders (anorexia nervosa and bulimia nervosa), attention-deficit/hyperactivity disorder (ADHD), idiopathic developmental intellectual disability (a residual category capturing intellectual disability not attributable to any other cause) and a residual group of other MSDs. Neurological disorders were not included in the analyses.
Estimation of non-fatal burden
Non-fatal burden was measured in YLDs where one YLD equates to one year lived in less than ideal health. YLDs were calculated by multiplying the prevalence of a disorder by a disorder-specific disability weight (Vos et al., 2016).
Systematic reviews
For each MSD, epidemiological data were obtained from systematic reviews of electronic databases (MEDLINE, EMBASE and PubMed) conducted up to 31 October 2015. Grey literature searches for unpublished sources, which included government reports, international collaborative research projects and other mental health research groups were also conducted. Included studies were published during or after 1980, adhered to DSM or ICD criteria and were representative of the general population. A comprehensive list of data sources can be found at http://ghdx.healthdata.org/gbd-2015/data-input-sources.
Epidemiological modelling
Data from the systematic reviews were modelled in DisMod-MR 2.1, a publicly available Bayesian meta-regression tool designed specifically for GBD (Flaxman et al., 2013). DisMod-MR 2.1 uses the available epidemiological data to estimate point prevalence by age, sex and year for all countries (regardless of data availability) with corresponding 95% UIs.
Estimation of severity distribution
Severity proportions were estimated to better reflect the varying levels of disability within disorders. GBD 2015 followed the same approach for estimating the distribution of severity (Burstein et al., 2015; in GBD 2013). For most disorders, individual-level survey data from the Medical Expenditure Panel Survey (MEPS), the National Epidemiological Survey on Alcohol and Related Conditions (NESARC) and the 1997 Australian National Survey of Mental Health and Wellbeing were used to estimate the proportion of persons experiencing each level of severity. For schizophrenia and bipolar disorder, severity distributions were estimated from a meta-analysis of survey data. For residual group of MSDs, we used prevalence of personality disorders not comorbid with MSD categories and severity distribution from NESARC and the 1997 Australian National Survey of Mental Health and Wellbeing. The prevalence estimates generated by DisMod-MR 2.1 were then split by severity using these proportions. More details on the severity distributions for MSDs are available elsewhere (Vos et al., 2016).
Disability weights
Disability weight is a numerical representation of the severity of health loss associated with a health state. For all disorders, each level of severity had a corresponding disability weight (Salomon et al., 2012). Disability weights were obtained from surveys of over 30,000 participants from Hungary, Italy, the Netherlands and Sweden, conducted face-to-face, via telephone, or online (an open-access web-based survey; Salomon et al., 2015). As described in the original study, participants were presented with pairs of lay health state descriptions and asked to select which of the two was ‘healthier’. Responses were anchored on a scale ranging from 0 and 1 (with 0 equivalent to full health and 1 equivalent to death) using additional questions comparing the benefits of lifesaving and disease prevention programmes for selected health states.
Comorbidity adjustment
As individuals may suffer from more than one disease at a given point in time, YLD estimates were adjusted for comorbidity. Microsimulations were conducted to estimate independent comorbidity. Hypothetical populations for each age group, sex, year and location were exposed to the independent probably of having each disorder (where the probability was set as the prevalence of the disorder). The multiplicative function was then used to calculate the combined disability experienced for people with multiple disorders (Vos et al., 2016). The comorbidity correction estimated the difference between the average disability weight in individuals suffering from only one disorder and combined disability weight in those suffering from two or more disorders.
Estimating fatal burden
Cause-specific YLLs were calculated by multiplying the number of deaths by the life expectancy at the age of death (Wang et al., 2016). Data on causes of death were derived from vital registration, verbal autopsy and maternal and child mortality surveillance databases. For MSDs, the Cause of Death Ensemble modelling (CODEm) strategy was used to model cause of death data by location, age, sex and year (Vos et al., 2016). CODEm algorithm was necessary to reassign inaccurate causes of death and enhance the validity of cause of death estimations. Normative life tables were generated based on the lowest observed death rates for any age group within all GBD locations with a total population greater than 5 million. The GBD world population age standards were used to calculate age-standardised mortality rates and YLL rates. Death records used in GBD 2015 followed the ICD-10 definition of attribution of cause of death to a single underlying cause (World Health Organization, 1993), and as such, YLLs were calculated for drug use disorders, alcohol use disorders, schizophrenia and eating disorders. Deaths due to suicide were not included in the YLL estimations.
Aggregation of non-fatal and fatal burden
DALYs were calculated by summing YLDs and YLLs for each disorder. One DALY equates to one lost year of healthy life.
Results
Prevalence
Figure 1 shows the prevalent cases of MSDs in Australia in 2015. Anxiety and depressive disorders were the most prevalent, followed by other MSDs and substance use disorders. MSDs were prevalent across all ages and both sexes. Females had significantly higher prevalence rate of anxiety disorders (7907.2 prevalent cases per 100,000 of the population, 95% UI: 6993.5–8953.8) and depressive disorders (6262.1 prevalent cases per 100,000, 95% UI: 5712.0–6901.3) than males, while males demonstrated significantly higher prevalence of drug use disorders (2524.8 per 100,000, 95% UI: 2407.2–2666.9) and alcohol use disorders (1581.9 per 100,000, 95% UI: 1403.0–1795.2) than females.
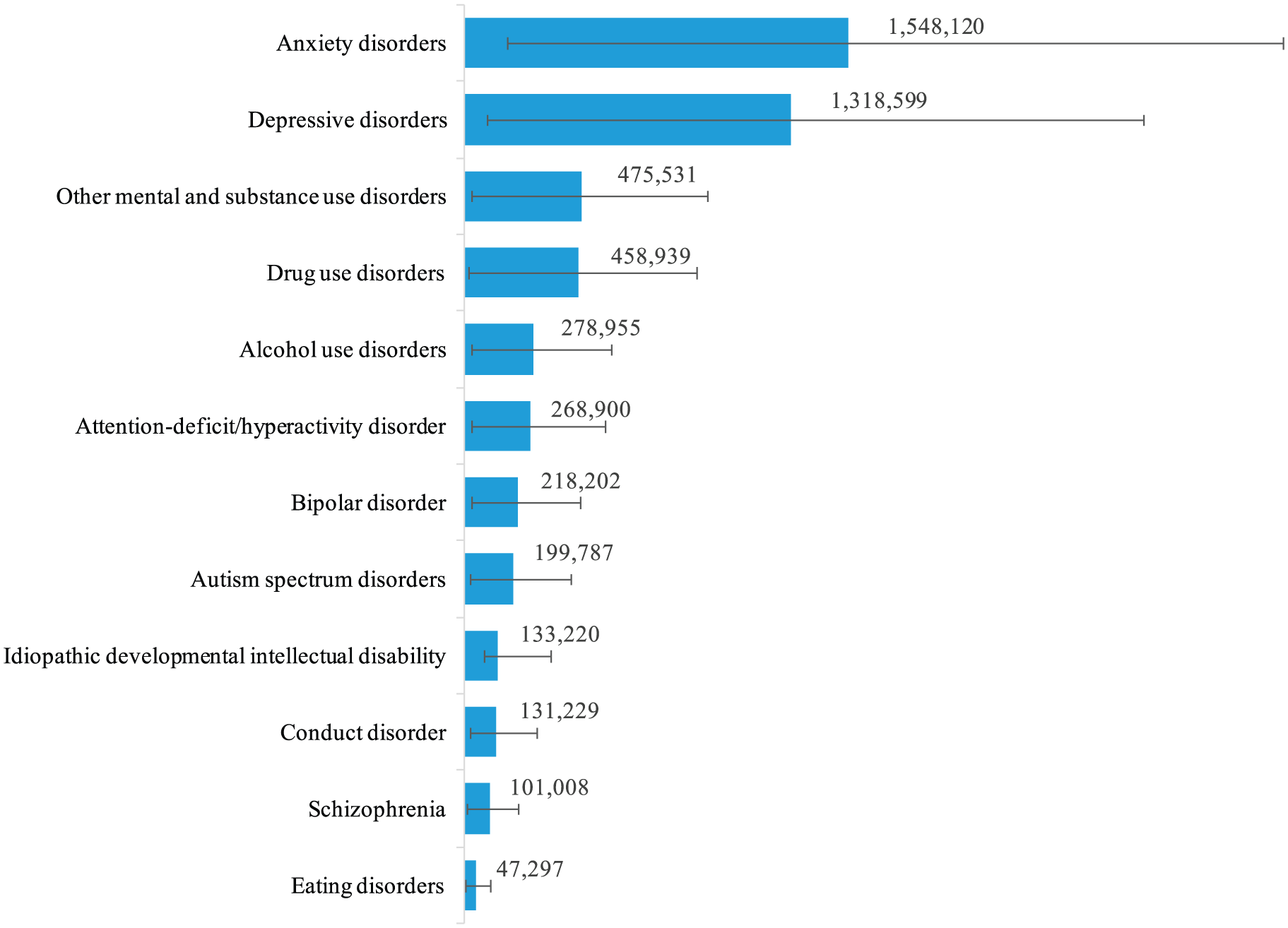
Number of prevalent cases and 95% UIs by each mental and substance use disorder in 2015 in Australia.
Non-fatal burden
MSDs were the leading cause of YLDs in Australia in 2015, accounting for 718,700 YLDs (95% UI: 528,100–922,500) or 24.3% (95% UI: 20.9–27.5%) of all YLDs. This equated a rate of 2955.0 MSD YLDs per 100,000 of the population (95% UI: 2171.1–3793.1). The number of YLDs increased since 1990 (478,100 YLDs, 95% UI: 349,600–611,600) although this was due to Australia’s population growth and ageing as the rate of MSD YLDs did not change significantly over this period (2808.1 YLDs per 100,000, 95% UI: 2053.5–3592.1).
Fatal burden
In 2015, MSDs were responsible for 61,500 YLLs (95% UI: 53,800–67,800) in Australia, making them the ninth leading cause of YLLs and explaining 2.6% (95% UI: 2.3–2.9%) of all YLLs in Australia. The rate of MSD YLLs increased between 1990 (193.3 YLLs per 100,000, 95% UI: 179.8–208.0) and 2015 (253.1 YLLs per 100,000, 95% UI: 221.3–278.9) with this driven by drug use disorders.
Total burden
In 2015, MSDs were the second leading cause of DALYs in Australia after neoplasms. They contributed 780,200 DALYs (95% UI: 586,300–983,800), equating to 14.6% (95% UI: 12.2–16.6%) of all DALYs in Australia and a rate of 3208.0 DALYs per 100,000 (95% UI: 2410.4–4045.1). This rate did not change significantly from 1990 (3001.4 DALYs per 100,000, 95% UI: 2246.9–3775.9). When controlling for variations in the age structure of the population, the age-standardized rate of MSDs in Australia in 2015 (3068.3 DALYs per 100,000, 95% UI: 2300.9–3866.8) did not differ significantly from the global mean (2183.3 per 100,000, 95% UI: 1627.1–2766.3) nor like countries including the United States, Canada, New Zealand or the United Kingdom.
Within MSDs in Australia, depressive disorders, drug use disorders and anxiety disorders were responsible for almost 66% of all DALYs due to MSDs as shown in Figure 2. Depressive disorders were the third leading cause of burden in Australia in 2015 after low back and neck pain and ischaemic heart disease. Drug use disorders (10th) and anxiety disorders (12th) were also in the top 20 leading causes of DALYs in Australia in 2015. Despite having the highest disability weight in GBD 2015, schizophrenia was ranked 26th due to its relatively low prevalence.
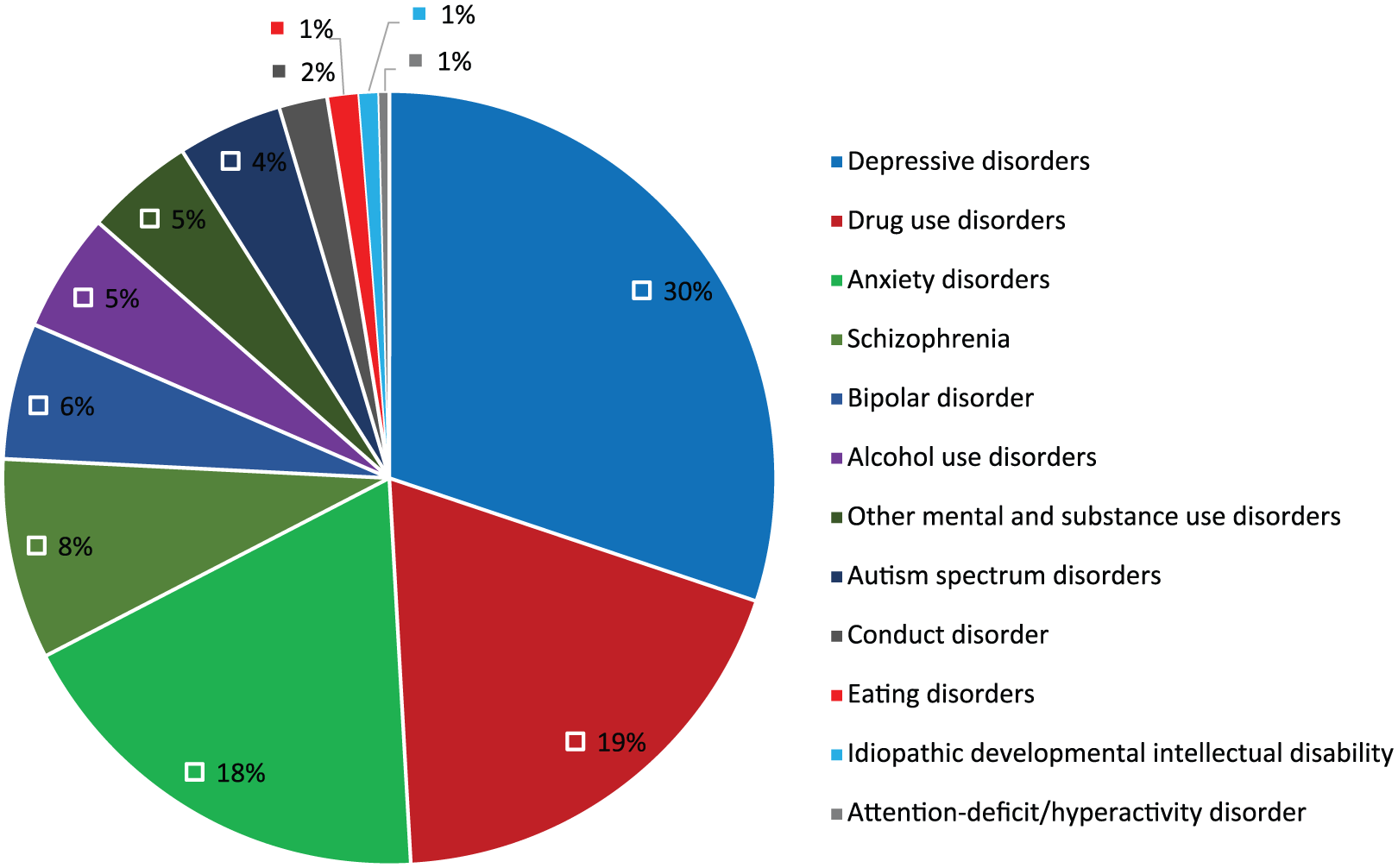
Proportions of DALYs for mental and substance use disorders in 2015 in Australia.
The overall DALY rate of MSDs in males and females did not differ significantly in Australia in 2015 as shown in Table 1. However, males experienced significantly higher DALY rates of drug use disorders, alcohol use disorders and ASDs compared to females, while females had higher DALY rates for eating disorders than males (Table 1).
The rate of DALYs by disorder for males and females in Australia in 2015.
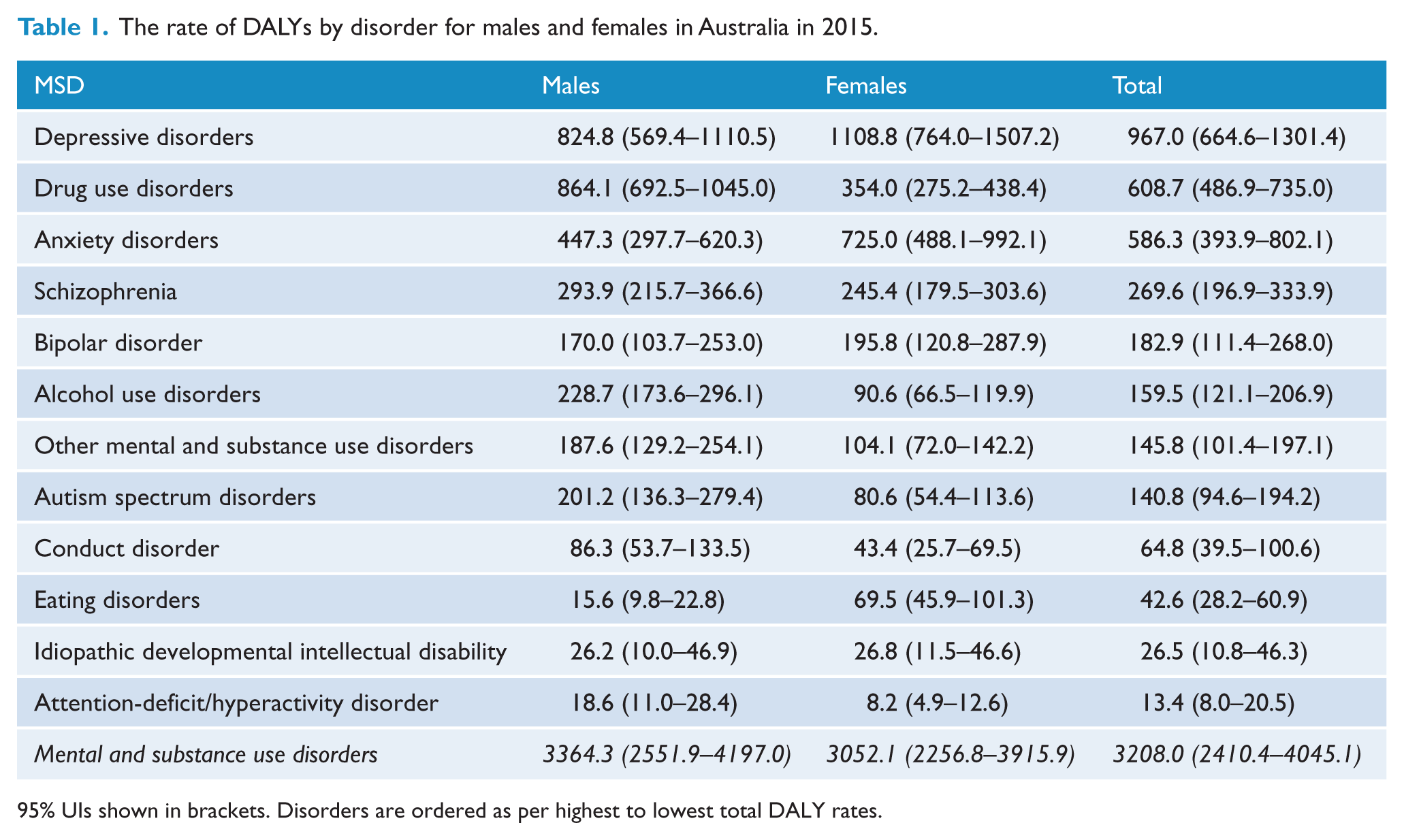
95% UIs shown in brackets. Disorders are ordered as per highest to lowest total DALY rates.
Figure 3 shows DALY rates in 2015 for each disorder by age in Australia. Burden due to MSDs was present across the lifespan, peaking during young adulthood and slowly declining with age. Depressive and anxiety disorders had the highest rates of burden in most age groups, while conduct disorder, ASDs and anxiety disorders contributed the majority of MSD burden during childhood.
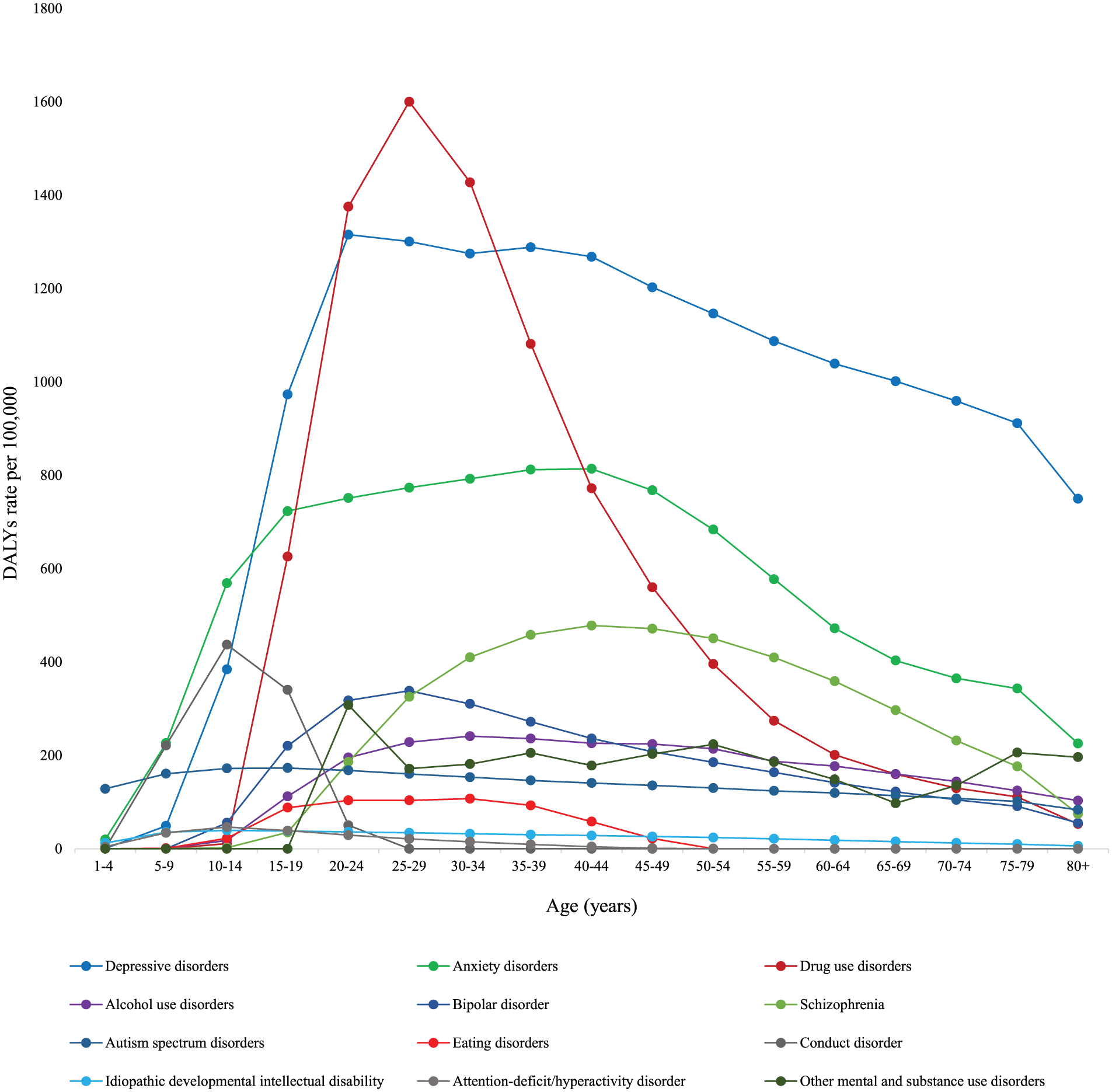
The rate of DALYs for each mental and substance use disorder by age group in Australia in 2015.
Discussion
The contribution of MSDs in Australia’s burden of disease has been recognised over recent decades and the Australian Government placed mental health among nine national health priority areas in 1996, aiming to reduce burden and improve the health status of Australians (AIHW, 2017). About US$8 billion per annum now spent on mental health–related services in Australia, including residential and community services, hospital-based services (both inpatient and outpatient) and consultation with specialists and general practitioners (MHSA, 2016). The policy initiatives have continued with the upcoming Fifth National Mental Health Plan (The Department of Health, 2016) seeking to revise the national approach to mental health over the next 5 years and the National Drug Strategy 2016–2025 (Australian Government, 2015) aiming to prevent the uptake of harmful drug use and reduce the harmful effects of drugs in Australia. Commitments to research funding have also been made, with the Australian Government’s 2011 strategic investment in mental health research of US$26.2 million for 5 years (NHMRC, 2015). In line with the increased policy attention there is evidence of an increase in treatment rates for mental disorders (Jorm et al., 2017, Whiteford et al., 2014).
However, GBD 2015 found that MSDs remain the leading cause of YLDs and the second leading cause of DALYs in Australia in 2015, and there has been no significant change in DALY rates between 1990 and 2015, and the only significant trend over time was an increase in YLLs due to drug use disorders. To compare, there has been a significant reduction in the burden of cardiovascular diseases worldwide, including Australia over the same period of time (Roth et al., 2017). These findings indicate that the increased attention MSDs have gained in policy and research has not been translated into a detectable decrease in burden. This can be partially explained by the fact that to observe an impact of policy changes requires several years; therefore, it might be premature to state that initiatives on mental health in Australia are not effective. However, previous research has suggested that 60% of the burden of 10 mental disorders would be unavertable even with optimal treatment at optimal coverage (Andrews et al., 2004). This would suggest that research to improve the efficacy of interventions is needed. It has also been suggested that greater attention should be paid to prevention (Jorm et al., 2017), focusing on the risk factors and predictors of MSDs and the broader societal factors that can influence prevalence and burden. Early intervention and treatment of MSDs need to be integrated into all facets of health system, as well as criminal justice, welfare and education systems, for burden to be fully addressed.
Although GBD 2015 is the most comprehensive assessment of disease burden to date, there are limitations that must be considered when interpreting the findings. For example, GBD only considers disability in terms of health loss and does not consider the impact of an MSD on future outcomes, families, or society. The estimation of YLLs for mental disorders is challenging as they are rarely listed as the primary cause of death in vital registration systems or they cannot be coded as such under ICD coding systems. For example, many deaths occurring in people with schizophrenia are certified and coded to other diseases and injuries as the underlying cause, such as self-harm, unintentional injuries, infectious diseases, substance use, cardiovascular disease and cancers (Wang et al., 2016). Furthermore, in GBD, suicide is categorised under injuries rather than MSDs. As such, the YLL component does not reflect the significantly increased risk of premature mortality in people with mental disorders (CHESNEY et al., 2014). However, work is underway to address this in future iterations of GBD, and a previous comparative risk assessment analysis showed that MSDs accounted for over 50% of YLLs due to self-harm.
Conclusion
MSDs are significant contributors to the total burden of disease in Australia. Despite decades of policy attention accompanied by increased treatment rates, the burden has remained unchanged over the 25 years to 2015. The sector needs to develop more efficacious interventions and pay increased attention to prevention if the burden of MSDs is to be reduced.
Footnotes
Acknowledgements
The authors gratefully acknowledge all core and corresponding members of the Global Burden of Disease Study 2015 who assisted in estimating the burden of mental and substance use disorders.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.