
Abstract
Suicide and self-harm are significant international public health problems [1,2]. It is estimated that every year more than one million people die by suicide worldwide, with the number of episodes of non-fatal self-harm (depending on definition) estimated at 10 to 100 times greater than the number of deaths [3,4].
Individuals who present to hospital following an episode of self-harm have elevated risks of further self-harm and death by suicide [5–9]. For example, Owens, Horrocks and House [5] reported that the risk of further self-harm was 15% in the twelve months following a non-fatal suicide attempt, and in the four years following the attempt the risk was 23%. There is evidence to suggest that the risk of further suicidal behaviour is particularly high for patients who leave hospital without receiving adequate assessment [10,11].
One factor that has been suggested to influence patient care and the risk of further suicidal behaviour is staff training and attitudes towards patients. Self-harm patients are likely to have contact with multiple staff from a range of specialties during their hospital visit, and the majority of these staff will not have mental health backgrounds. Patients who have harmed themselves may be challenging for these staff, and may elicit negative attitudes and reactions such as frustration, anger, and a lack of empathy.
There is a growing body of literature examining the attitudes of health-care staff towards self-harm patients. Studies have reported that staff feel frustration with patients who are frequently admitted, have difficulty feeling empathy for patients, are uncertain about how to interact with self-harm patients, and lack knowledge about suicide and self-harm [12–17]. Staff also report that they feel inadequately trained to care for self-harm patients, and would welcome training in this area [13,14,16,18].
It has been shown that staff attitudes towards self-harm patients are related to a number of demographic and employment factors. Several studies have reported that older and more experienced staff tend to have more positive attitudes than younger and more inexperienced staff [18–21], although the reverse has also been reported [14]. Other studies have reported that female staff have more positive attitudes than male staff [15,18,21].
However, previous studies of staff attitudes towards self-harm patients have some limitations. Many previous studies have been restricted to emergency department (ED) staff [14,15,19–24]. However, many self-harm patients will have contact with health-care staff from other specialties during their hospital attendance, such as general medical staff and psychiatric staff, and less is known about the attitudes of these staff groups. Furthermore, most previous research has been conducted in the UK [14,16,20,25,26], with a small number of studies from Australia [13,19,27]. There is little or no previous research on staff attitudes towards self-harm patients in New Zealand, despite the fact that suicide rates in New Zealand are relatively high by international standards [28].
The present study examines attitudes towards self-harm patients amongst health-care staff in Christchurch, New Zealand. To examine attitudes across a range of staff groups, participants were drawn from the emergency department, general medical wards, and psychiatric services. The aims of the present study were: (i) to examine the attitudes of healthcare staff towards self-harm patients; (ii) to examine whether these attitudes vary as a function of: individual characteristics (including age, and gender), job characteristics (including occupation, work area, and experience) and burnout; (iii) to examine the specific difficulties and training needs amongst staff working with self-harm patients.
Materials and methods
Study setting and population
Participants were medical or psychiatric staff working at Christchurch Hospital or Hillmorton Hospital, Christchurch, New Zealand. Christchurch Hospital is the main public hospital and sole emergency department in the greater Christchurch area and services a population of approximately 485 000. Hillmorton Hospital is the sole acute adult inpatient psychiatric service in the greater Christchurch area, and also provides a range of adult and youth outpatient psychiatric services. Hospital departments in which staff were likely to have contact with self-harm patients were identified through consultation with department managers. At Christchurch Hospital these departments were the emergency department, intensive care unit, acute medical assessment unit, and four acute medical wards. At Hillmorton Hospital the departments were three acute psychiatric inpatient wards. Staff in these departments were approached during staff handover meetings and invited to participate in the study. Recruitment was carried out over a consecutive 24-hour period in each department. All medical staff working in a department during the 24-hour recruitment period were asked to participate in the study. While this 24-hour period did not cover all staff working in a department, it provided a ‘snapshot’ of staff within a department.
Written informed consent to participate in the study was obtained from all participants at the time of filling out the questionnaire. The study was approved by the Upper South A Regional Ethics Committee.
Measures
Participants completed a written questionnaire which included the following components:
Attitudes towards self-harm patients
The questionnaire contained a series of 18 statements about working with self-harm patients. These statements covered a range of different aspects of working with self-harm patients, including empathy, enjoyment, perceived ability to help, confidence and adequacy of training. For each statement participants were asked to select whether they strongly agreed, agreed, disagreed, or strongly disagreed.
Responses to these statements were analysed using exploratory factor analysis. Factor analysis was performed in SAS 9.1 [29] using the ‘PROC FACTOR’ procedure with promax (oblique) rotation and a cut off of 0.4. The analysis revealed a maximum of five factors, but a three factor model was selected as it appeared to provide a better fit. One attitudinal statement was removed because it did not load significantly on any factor. Together the three factors explained 48.3% of the total variance. Total scores for each factor were calculated by summing the individual item scores for the items that had factor loadings of 0.4 or above. The total factor scores all had moderate to good reliability, with α = 0.7 or above.
Burnout
Participants completed the third edition of the Maslach Burnout Inventory [30]. The inventory comprises 22 items and participants were required to rate how often they had experienced each item within the last year using a six-point scale ranging from 0 (never) to 5 (always). These items form three subscales: emotional exhaustion, personal accomplishment and depersonalization.
The first item from the emotional exhaustion subscale was omitted due to a clerical error. Data for the remaining 21 items were submitted to a factor analysis using the ‘PROC FACTOR’ procedure in SAS 9.1 with promax rotation. A maximum of five factors were identified, but a three factor model was chosen because it appeared to provide a better conceptual fit. The three factor model revealed a similar pattern of factor loadings to the one observed with the full Maslach scale [30]. Items 4 and 8 from the emotional exhaustion subscale loaded on the depersonalization factor rather than the emotional exhaustion factor. Otherwise the pattern of factor loadings was the same as in the original inventory. The reliabilities for the sub-scales were good (α = 0.83 for emotional exhaustion, α = 0.77 for depersonalization, and α = 0.78 for personal accomplishment). Because the factor pattern observed with the reduced 21-item inventory was very similar to that observed with the full inventory, throughout the rest of this paper ‘Maslach Burnout Inventory’ refers to the reduced 21-item version of the test.
Job characteristics
The survey included a series of questions about the participant's job. These included: occupation; number of hours worked in the last week; primary work area; length of time in the job; and length of time in the specialty.
Individual characteristics
The survey also gathered information on participants’ personal and demographic characteristics, including age, gender and highest educational achievement.
Statistical analysis
All statistical analyses were conducted in SAS 9.1 [29].
Factor analysis used the PROC FACTOR procedure with promax (oblique) rotation and a cut off of 0.4 (Tables 1 and 2).
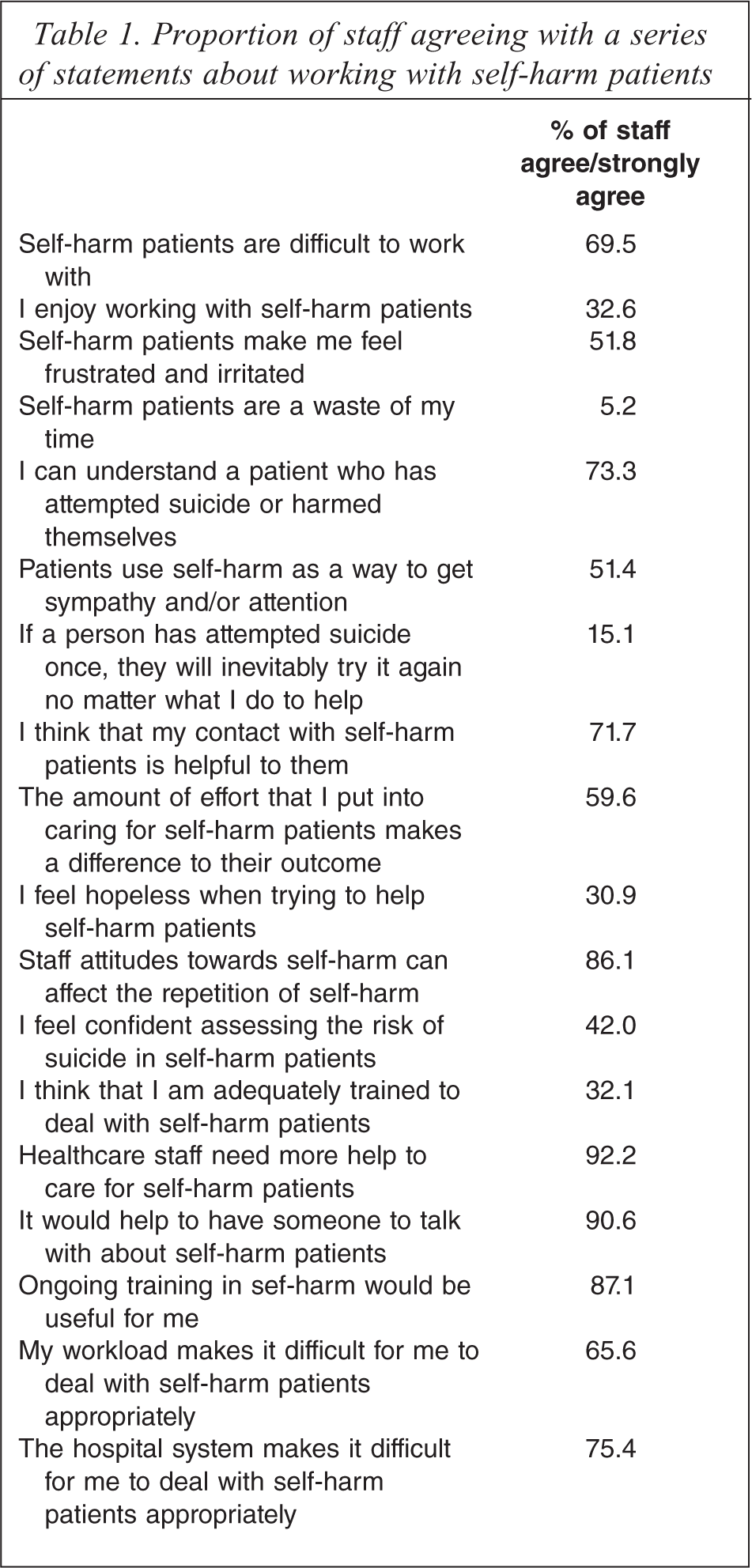
Proportion of staff agreeing with a series of statements about working with self-harm patients
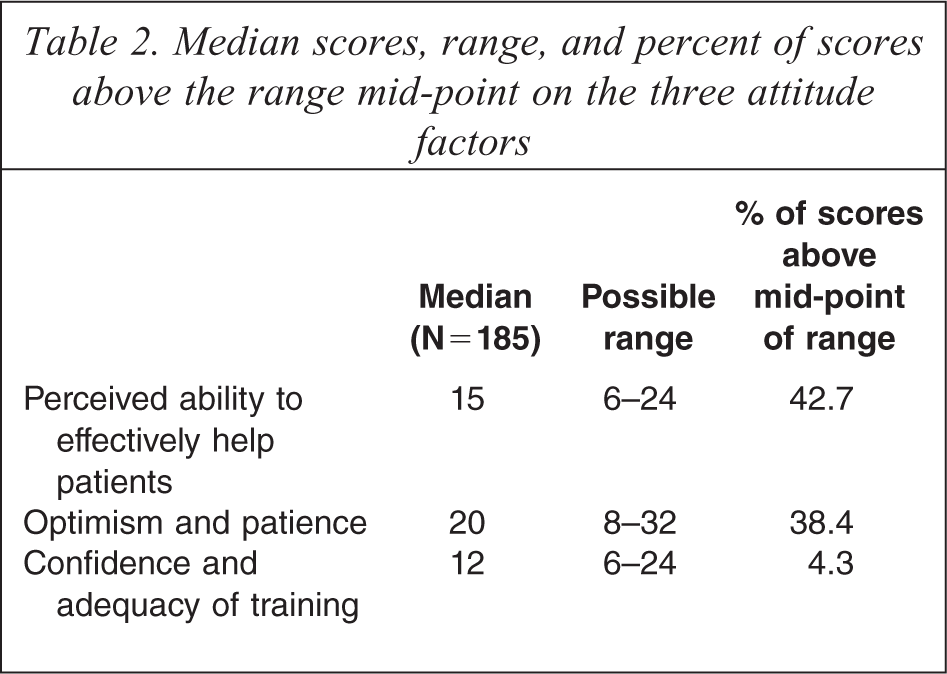
Median scores, range, and percent of scores above the range mid-point on the three attitude factors
Associations between attitude scores and individual characteristics, job characteristics, and burnout scores (Table 3) were examined using multiple regression models in which the attitude score was modelled as a function of the individual characteristics, job characteristics and burnout scores.
Regression coefficients and p-values for significance from the regression models
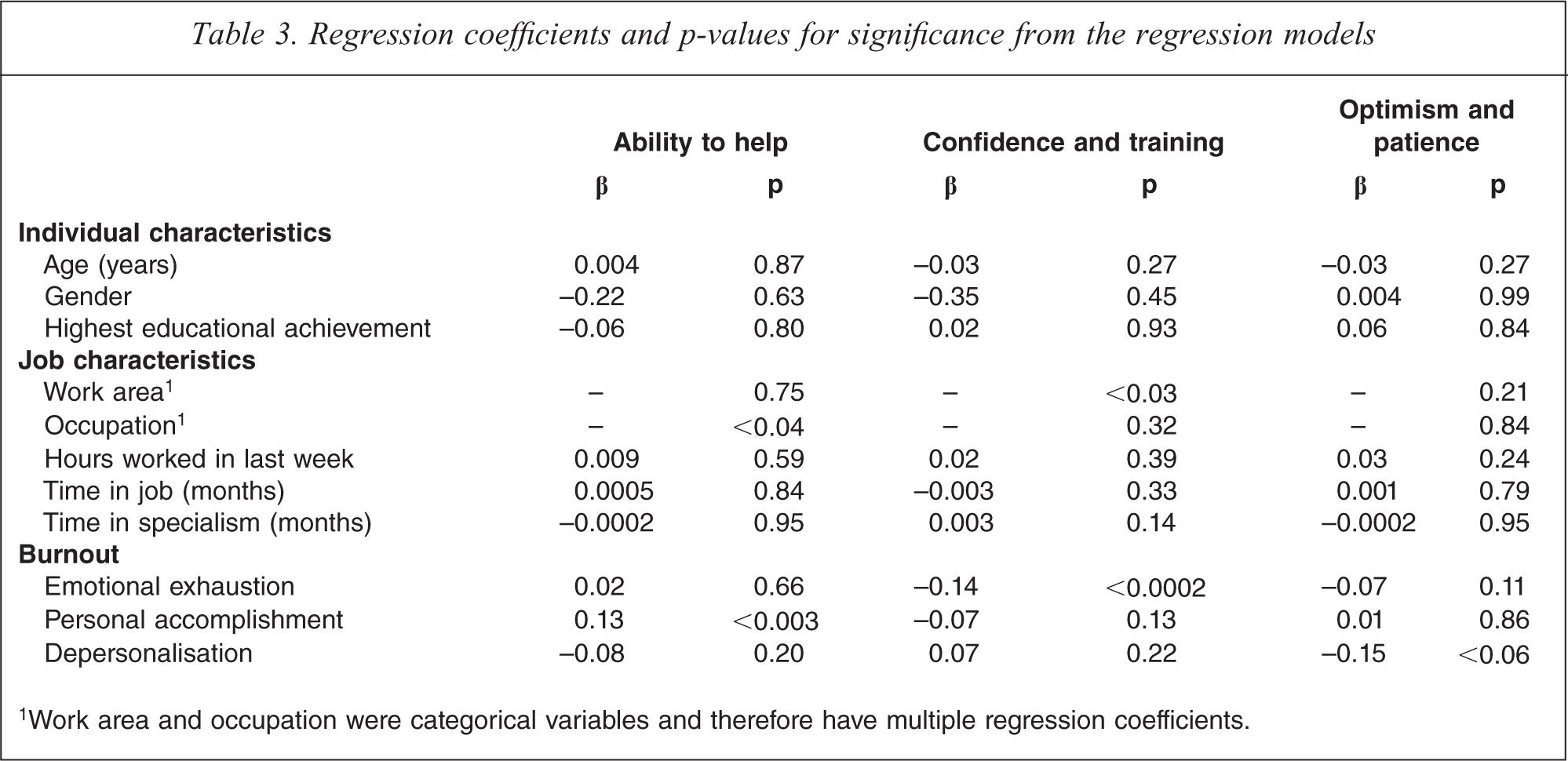
1Work area and occupation were categorical variables and therefore have multiple regression coefficients.
Differences in the proportion of participants from different work areas mentioning specific difficulties and training needs (Tables 4 and 5) were tested for statistical significance using a Chi-squared test for independence.
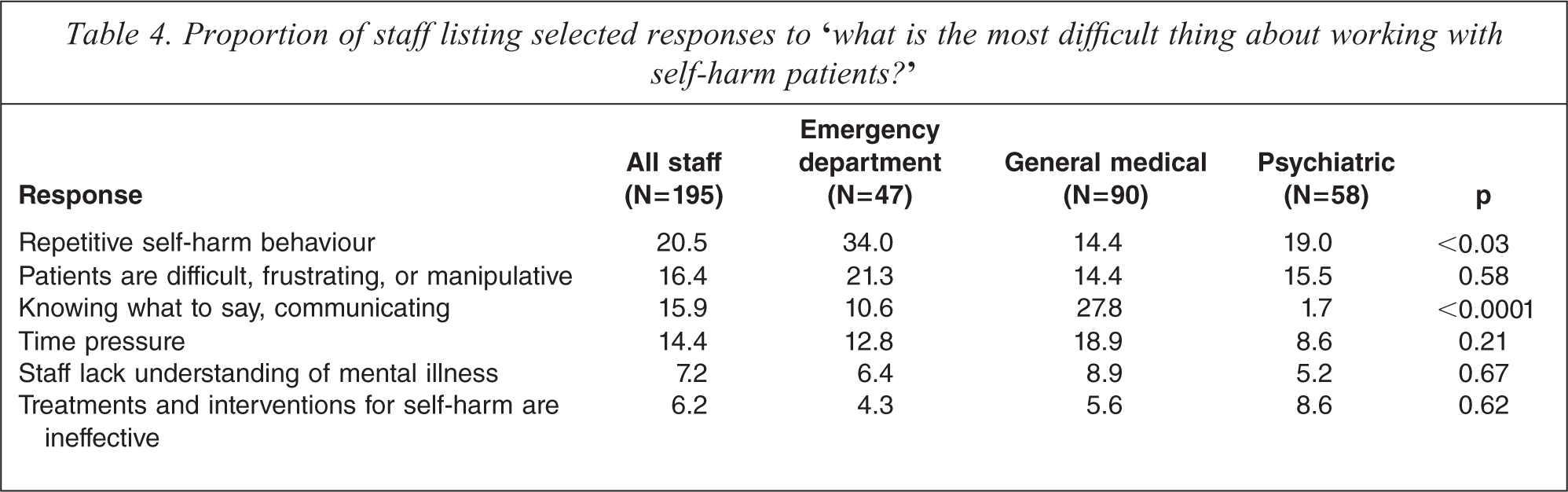
Proportion of staff listing selected responses to ‘what is the most difficult thing about working with self-harm patients?’
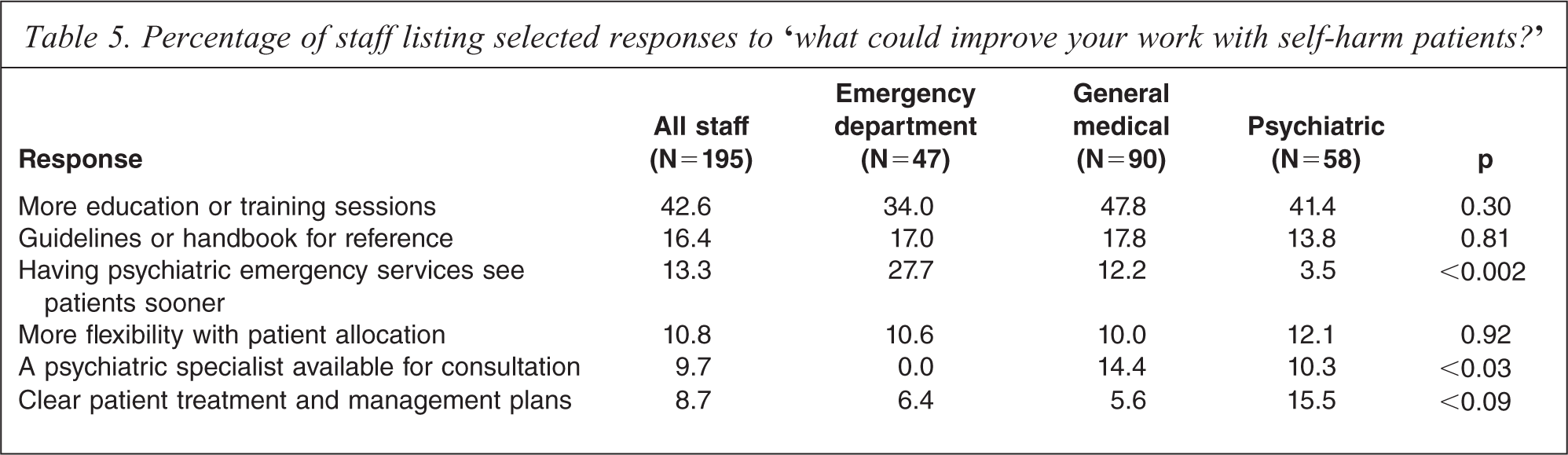
Percentage of staff listing selected responses to ‘what could improve your work with self-harm patients?’
Results
Response rate
A total of 303 questionnaires were distributed to staff. Of these, 195 completed questionnaires were returned, a response rate of 64.4%. Staff represented a range of medical specialisms (36 medical doctors, 11 psychiatric doctors, 103 medical nurses, 45 psychiatric nurses). The sample consisted of 54 males and 133 females, and ages ranged from 22 to 64 with a median of 37.
Attitudes to self-harm
Table 1 shows the proportion of staff who agreed or strongly agreed with a series of statements about working with self-harm patients. Overall, staff tended to have a mixture of positive and negative attitudes towards self-harm patients. The majority of staff felt that self-harm patients were difficult to work with (69.5%) and that staff needed more help to care for such patients (92.2%); only 32.6% of staff stated that they enjoyed working with self-harm patients. However, staff also had positive attitudes towards self-harm patients, with 73.3% of staff stating that they could understand a patient who has harmed themselves, 71.1% stating that they believed their contact was helpful to self-harm patients, and only 5.2% believing that self-harm patients were a waste of staff time.
To examine whether the attitudes in Table 1 reflected a single scale or several subscales, factor analysis was conducted (see Methods for details). The analysis identified three factors. The first factor, ‘perceived ability to help’, measured the extent to which staff believed that their contact was helpful to self-harm patients, and that the amount of effort they put into care made a difference to patient outcomes. The second factor, ‘optimism and patience’, measured the extent to which staff enjoyed working with self-harm patients, were not frustrated by patients or working conditions, and were optimistic that patients would improve. The third factor, ‘confidence and training’, measured the extent to which staff felt confident working with self-harm patients and believed that they were well trained to work with those patients.
Table 2 shows the median scores for staff on each of the three attitude factors, the potential range for factor scores, and the proportion of the sample who had scores above the mid-point of the potential range. In all cases, higher scores indicate more positive attitudes. Overall, scores were moderate for the ‘perceived ability to help’ factor (median of 15, with 42.7% of scores above the mid-point) and the ‘optimism and patience’ factor (median of 20, with 38.4% of scores above the mid-point), reflecting the fact that staff felt moderately confident that they can help self-harm patients, were not particularly frustrated with patients or working conditions, and were somewhat hopeful about patients’ outcomes. However, scores were low for the ‘confidence and training’ factor (median of 12, with 4.3% of scores above the mid-point) reflecting the fact that staff did not feel confident in working with self-harm patients and believed that they were not adequately trained to work with these patients.
Tables 1 and 2 showed that staff believed that they were able to help self-harm patients and felt optimistic about patients’ outcomes, but did not feel confident or adequately trained to work with self-harm patients. However, Tables 1 and 2 considered the attitudes of staff as a single group, and did not consider whether attitudes may be associated with specific individual or job characteristics. To examine this, the factor scores in Table 2 were fitted with linear regression models in which each of the three attitude factors was modelled as a function of individual characteristics (age, gender, highest educational achievement); job characteristics (work area, occupation, hours worked in the last week, length of time in current job, length of time in current specialty; and burnout (Maslach Burnout Inventory scores for emotional exhaustion, depersonalization, and personal accomplishment). Table 3 reports the regression coefficients and p values for significance for each of the covariate factors in each of the regression models. The table shows:
None of the individual characteristics were significantly associated with any of the three attitude factors (all p >0.05). There were almost no significant associations between job characteristics and the three attitude factors. The only exceptions were occupation, which was significantly associated with perceived ability to help (p < 0.04), and work area, which was significantly associated with confidence and training (p < 0.03). Paired comparisons revealed that psychiatric nurses scored slightly higher on the ‘perceived ability to help’ factor than all other occupations (p < 0.08), and that emergency department staff scored slightly lower on the ‘confidence and training’ factor than general medical staff (p < 0.09). There were some significant associations between the Maslach Burnout Inventory scores and the three attitude factors. The ‘perceived ability to help’ factor was significantly associated with personal accomplishment (p < 0.003); and the ‘confidence and training’ factor was significantly associated with emotional exhaustion (p < 0.0003). There was an association between the ‘optimism and patience’ factor and depersonalization, although this association did not quite reach significance (p < 0.06).
To assess specific difficulties and training needs when working with self-harm patients, participants were asked to list the most difficult aspects of working with self-harm patients and what could be done to improve their work with these patients. Responses to these questions were made in free format and were later coded and classified according to their major themes.
Table 4 lists the most frequent responses from staff to the question ‘what is the most difficult thing about working with self-harm patients?’ The table shows all responses that were listed by more than 5% of the total sample. Specific difficulties may vary across different work areas, therefore the table shows the proportion of all staff who listed each response, and also the proportion of staff from each work area (emergency department, general medical, and psychiatric services) who listed each response. The table also shows the p values for significance for the difference in response frequency between staff in different work areas.
Staff listed a range of difficulties about working with self-harm patients, including patient behaviour, communication difficulties, lack of knowledge about mental illness, time pressure, and a lack of effective interventions. In most cases, there were no significant differences between different work areas in the proportion of staff listing each difficulty. Frustrating, difficult or manipulative behaviour from patients, time pressure, a lack of understanding of mental illness, and a lack of effective interventions and treatments for self-harm were mentioned with similar frequency by ED, general medical and psychiatric staff (all p >0.21). However, there were two difficulties that were listed with significantly different frequencies by staff in different work areas. More than one quarter of general medical staff (27.8%) stated that communicating with patients was one of the most difficult things about working with self-harm patients, while only 10.6% of emergency department staff and 1.7% of psychiatric staff mentioned this difficulty (p < 0.0001). Repetitive self-harm behaviour was listed as a difficulty more often by emergency department staff (34%) than by general medical staff (14.4%) or psychiatric services staff (19%) (p <0.03).
Table 5 shows the most frequent staff responses to the question ‘What could improve your work with self-harm patients?’ The table shows only those responses that were listed by more than 5% of staff. Specific training needs may vary across different work areas, therefore the table shows the proportion of all staff who listed each response, and also the proportion of staff from each work area who listed each response. The table also shows the p values for significance for the difference in response frequency between staff in different work areas.
There were considerable similarities, but also some important differences, between the responses of staff from the three work areas. For some of the responses, there was no significant difference in the proportion of staff from different work areas who listed the response. More education and training, provision of guidelines or a handbook for reference, and more flexibility with patient allocations were mentioned by similar proportions of emergency department, general medical and psychiatric services staff (all p >0.30). However, other responses were significantly more likely to be listed by staff in particular work areas than by staff in other work areas. For example, 27.7% of emergency department staff stated that having psychiatric emergency services see patients sooner after their admission to ED would improve their work, compared to 12.2% of general medical staff and 3.5% of psychiatric services staff (p < 0.002). Amongst general medical staff, 14.4% stated that having a psychiatric specialist available for advice and consultation would be useful, compared to 0% of emergency department staff and 10.3% of psychiatric services staff (p < 0.03). There was a difference between the proportion of staff in different work areas listing clearer patient treatment and management plans, although this difference did not quite reach significance (p < 0.09). This response was listed by 15.5% of psychiatric services staff, but only 6.4% of emergency department staff and 5.6% of general medical staff.
Discussion
This paper examined attitudes towards self-harm patients amongst health-care staff working in Christchurch, New Zealand. The main findings from the study are discussed below.
Overall, staff had a mixture of positive and negative attitudes towards self-harm patients. This finding is consistent with previous studies from other countries which have also reported mixed positive and negative attitudes towards self-harm patients, and low levels of confidence about working with self-harm patients [12–17]. Factor analysis of responses to the attitude items revealed three factors: perceived ability to help; optimism and patience; and confidence and training. Scores were moderate to high for the perceived ability to help and optimism and patience factors, indicating that staff believed their contact was helpful to self-harm patients, were not especially frustrated with patients, and felt optimistic about patient outcomes. However, scores on the confidence and training factor were low, indicating that staff did not feel confident working with self-harm patients and did not believe their training in self-harm was adequate.
Scores on the three attitude factors were not significantly associated with individual characteristics, including age, gender, and experience, and there were few associations between attitudes and job characteristics. This finding contrasts with several previous studies which have reported that older, more experienced staff tend to have more positive attitudes [18–21], and that females have more positive attitudes than males [15,18,21]. There were, however, significant associations between burnout and attitudes, with higher levels of burnout being associated with more negative attitudes on some of the factors. Previous studies of the relationship between work stress and attitudes have yielded inconsistent results, with an early study by Suokas and Lonnqvist [23] reporting that greater levels of work stress were associated with more negative attitudes towards self-harm patients, but a more recent study [24] reporting that psychological distress (presumed to measure stress) is not associated with attitudes.
Staff comments revealed both similarities and differences between the specific difficulties and training needs of staff in different work areas. Staff reported difficulties such as repetitive self-harm behaviour, frustrating and manipulative patient behaviour, communication difficulties, and time pressure. The most common suggestions for changes that would improve their work with self-harm patients included having more education or training sessions, and the provision of a handbook or guidelines for working with self-harm patients.
The findings from this study indicate a need for additional staff training in working with self-harm patients. While overall attitudes were not especially negative, confidence about working with self-harm patients was low. There was a strong desire for additional training and information about self-harm amongst staff from all three work areas (emergency department, general medical wards, and psychiatric services). Previous studies have suggested that even brief training courses can significantly improve staff knowledge and attitudes towards self-harm patients [17,31], although not all training programmes and interventions have been shown to improve attitudes [32–34]. These training courses may be able to be integrated into existing continuing medical education sessions. Preferably new training programmes would be evaluated in randomized controlled trials to determine whether they have a significant impact on staff knowledge and attitudes prior to being widely implemented.
It is interesting to note that in the present study, psychiatric services staff did not score significantly higher than other staff on any of the attitude factors, including the confidence and training factor. This is surprising given that psychiatric staff are likely to have had substantially more training and experience with self-harm than general medical staff. This finding suggests that additional training about self-harm is necessary for all staff working with self-harm patients, including psychiatric staff, although the content of this training may need to be modified for different staff groups in order to take account of baseline differences in knowledge and experience.
Staff comments indicated that staff working in different areas share many similar difficulties and training needs, suggesting that some interventions to improve staff attitudes and confidence may be applied to multiple staff groups. However, staff comments also indicated a number of differences, suggesting that any broad training may need to be supplemented by more specific training that addresses the specific difficulties faced by staff in particular work areas.
The finding that negative attitudes are related to higher levels of burnout through high emotional exhaustion and low personal accomplishment suggests that improvements in staff attitudes may also be gained by reducing work stress and burnout amongst healthcare staff.
A limitation of this study is the relatively low response rate (64.4%), although the response rate in the present study was higher than that in many other questionnaire based attitude studies [14,24,27]. It was not possible to collect information on those participants who did not complete the questionnaire so that they could be compared to the response sample. Therefore, it is possible that the sample of participants who responded may not be representative of the total population of health-care staff who care for self-harm patients. Another limitation of the study is that the sample of participants was drawn from one hospital in Christchurch, New Zealand. It is not clear to what extent the results of the current study will generalize to other hospitals in other countries.
These limitation notwithstanding, the results of the current study suggest that healthcare staff in New Zealand have a strong desire to help self-harm patients but lack confidence in their ability to do so. These attitudes are evident amongst emergency department staff, general medical staff, and psychiatric staff. Staff comments indicate a number of ways in which staff confidence and training could be improved, including additional training sessions and the provision of handbooks and guidelines. Additional training and education about self-harm has the potential to improve staff confidence and attitudes and enhance patient care.
Footnotes
Acknowledgements