
Abstract
The medical profession has led the way in research into the health of its members and trainees. In particular, research into medical student distress levels has reported elevated levels within this population for several decades. Studies indicate average rates of ‘distress’ to be between 12% [1] and 60% [2]. Studies have explored whether medical students are unusual in their elevated distress levels by comparing with other tertiary disciplines. Medical students showed a significant increase in stress levels between the first and second year of training, more so than economics and physical education students [3]. Conversely, medical students reportedly had less overall stress than post graduate science students [4], or a sample of geography students, but were nevertheless highly stressed [5]. Law students’ distress is also reported to be higher than that of medical students [4,6]. Common mental disorders were also higher in medical students (46%), compared to dentistry (33%), nursing (32%) and physical education students (25%) [7]. The medical profession has extensively researched students’ and clinicians’ distress and as such many are informed of the issues. This is not necessarily the case for the other disciplines, particularly the non-health disciplines.
It is evident that high levels of distress may not be unique to medicine. More recent research indicates that tertiary students in general exhibit high levels of distress symptoms compared to the general population [8,9], have lower quality of life scores, and rate their general health as worse than a sample of working peers [10].
A systematic review of studies in the USA and Canada concluded that female medical students manifest more distress symptoms than their male counterparts [11], although other studies reported equivalent distress levels between the sexes [7,12,13]. Several studies suggested that distress levels at the outset of medical studies are equivalent but females increasingly report more symptoms of distress and anxiety as they progress through the course [11,14].
In an American tertiary student population, 15% of students received professional treatment which was predicted by gender, with females seeking more than their male counterparts [15]. In Sweden, 17% of medical students had sought treatment during their medical training [16]. In Norway, 44% of medical students with mental health problems sought professional help [17], but in the USA only 27% of depressed medical students reported treatment [18]. Treatment rates seem to vary significantly between countries and are most likely dependent on attitudes, stigma associated with mental illness, and access and affordability of health care. Data are limited with respect to medical student and other tertiary student treatment rates.
Specific literature on the distress levels of tertiary students in Australia is limited, as are the rates of mental health treatment. The suspected high levels of distress pose particular problems for tertiary institutions, in terms of the provision of services and approaches to dealing with tertiary student distress. For students undertaking lengthy training regimes prolonged exposure to distress may have important ramifications. This paper aims to: (i) compare tertiary student distress levels with age-matched population distress levels; (ii) determine whether distress levels vary due to discipline, year level, or student characteristics; (iii) examine tertiary students’ self-reported treatment rates; (iv) examine tertiary students’ concern regarding their perceived levels of distress.
Method
Data on distress level, distress concern and treatment rates were gathered via three studies. Study I was a voluntary self-administered web-based questionnaire. Studies II and III were voluntary self-administered anonymous paper-based questionnaires. All studies included a measure of distress and sought information on treatment rates. Study I also sought information on participants’ level of concern regarding the distress they were experiencing. All studies were voluntary for all participating disciplines and students. Informed and written consent was collected for Study I in order for participants to gain access to the web survey. Consent was implied for students participating in Studies II and III by the return of the completed paper based survey. Ethical clearance was received by the Human Research Ethics Committee at the University of Adelaide for 2007.
Participants and setting
Participants consisted of students from the University of Adelaide, a public university in South Australia. The disciplines of Medicine, Law, Mechanical Engineering and Psychology participated in the research. Data were collected consecutively from each of the cohorts (Medicine years 1, 2, 3, 4, 5, 6: Mechanical Engineering years 2, 3: Law years 2, 3: Psychology year 3) between March and October 2007. Overall response rate was 78% (N = 974) calculated as the percentage of those students who participated in the research from those present at recruitment lectures and tutorial groups. Psychology had the highest response rate at 99%, followed by Medicine at 83%, Mechanical Engineering 70% and Law 68%.
Psychology was chosen as a comparative health discipline to Medicine, while Law and Mechanical Engineering were chosen as similar training-intensive courses to Medicine. The Bachelor of Medicine/Bachelor of Surgery is a six-year undergraduate course. Mechanical Engineering and Law are both four-year degree programmes. Psychology is a three-year degree programme.
Data were compared to 1515 age matched peers (16 to 24 years old) from a South Australian population survey conducted in 2002–2004. Response rate was not cited for this age group but was cited as 69% for the overall sample of 10,229 [19]. Households were selected randomly from electronic white pages.
Measures
The Kessler Measure of Psychological Distress (K10) was selected to measure levels of distress [20], as it also enabled comparisons between the current research data and Australian population surveys. The ten items of the K10 consist of questions based on anxiety and depressive symptoms that have been experienced in the previous four weeks. Respondents rate the ten items using a five-point scale ranging from all of the time (5) through to none of the time (1). Scores from the ten items are summed to give an overall total indicating the level of psychological distress. Interpretation of the K10 summary score is based on a score banding method comprising four levels of psychological distress (low, moderate, high, very high) to enable direct comparison with the normative age matched K10 data [19]. A participant scoring in either of the top two bands was classified as psychologically distressed (a score ≥ 22/50) indicating that the participant has a high risk of developing or having a mental health disorder [21]. The same threshold was used in the South Australia population survey [19]. Sensitivity and specificity data analysis indicates that the K10 is appropriate for screening for anxiety and depression [22].
Socio-demographic data were sought directly from the participating student or from the participating academic discipline. Data gathered included age, sex, year level, discipline, student status (local or international student), location at time of survey (rural or urban educational placement) and primary language spoken at home. Participants also indicated whether they had ever been diagnosed or treated for a mental health problem (yes/no). The level of concern that participants felt about their distress level was gathered using a four-point scale (very concerned (4), moderately, a little, not at all (1)).
Data analysis
A preliminary power analysis was not performed as the sample size was fixed by the number of students enrolled into the academic programmes and by the year levels who agreed to participate in the studies. Since the study designs were quasi-experimental, causality could not be inferred from statistical analyses, only relatedness. The varying sample sizes, frequent heterogeneity of variances and skewed distributions were deemed of sufficient magnitude, coupled with the reliance on categorical Likert-type scales, to warrant the use of non-parametric inferential statistics. The level of significance was set to 0.05 (95% confidence) unless otherwise stated.
Descriptive and inferential statistics were generated using SPSS (version 15; Chicago, IL, USA; www.spss.com). Additional web-based programs were used to calculate z-tests to determine significance between two independent proportions [23] and relative risk and odds ratios [24]. Cohen's d effect size with a Hedges correction for bias was calculated using a downloadable spreadsheet [25]. Descriptive labels for the magnitude of effect sizes and correlations were determined from cut offs set by Hopkins [26]. Bonferroni adjustments were used to control for Type I errors. Since small numbers of multiple comparisons were required (≤ 6 in any one situation), and significant p values were often quite small, it was appropriate to opt for the more conservative Bonferroni calculation. Mann-Whitney U tests, and Kruskal-Wallis tests were used to compare K10 distress means. Spearman's Rho test was used to determine association between variables.
Results
Of the 974 students who participated in one of the three studies, a total of 955 completed the K10. The characteristics of the student sample are displayed in Table 1.
Characteristics of the tertiary students completing the distress measure
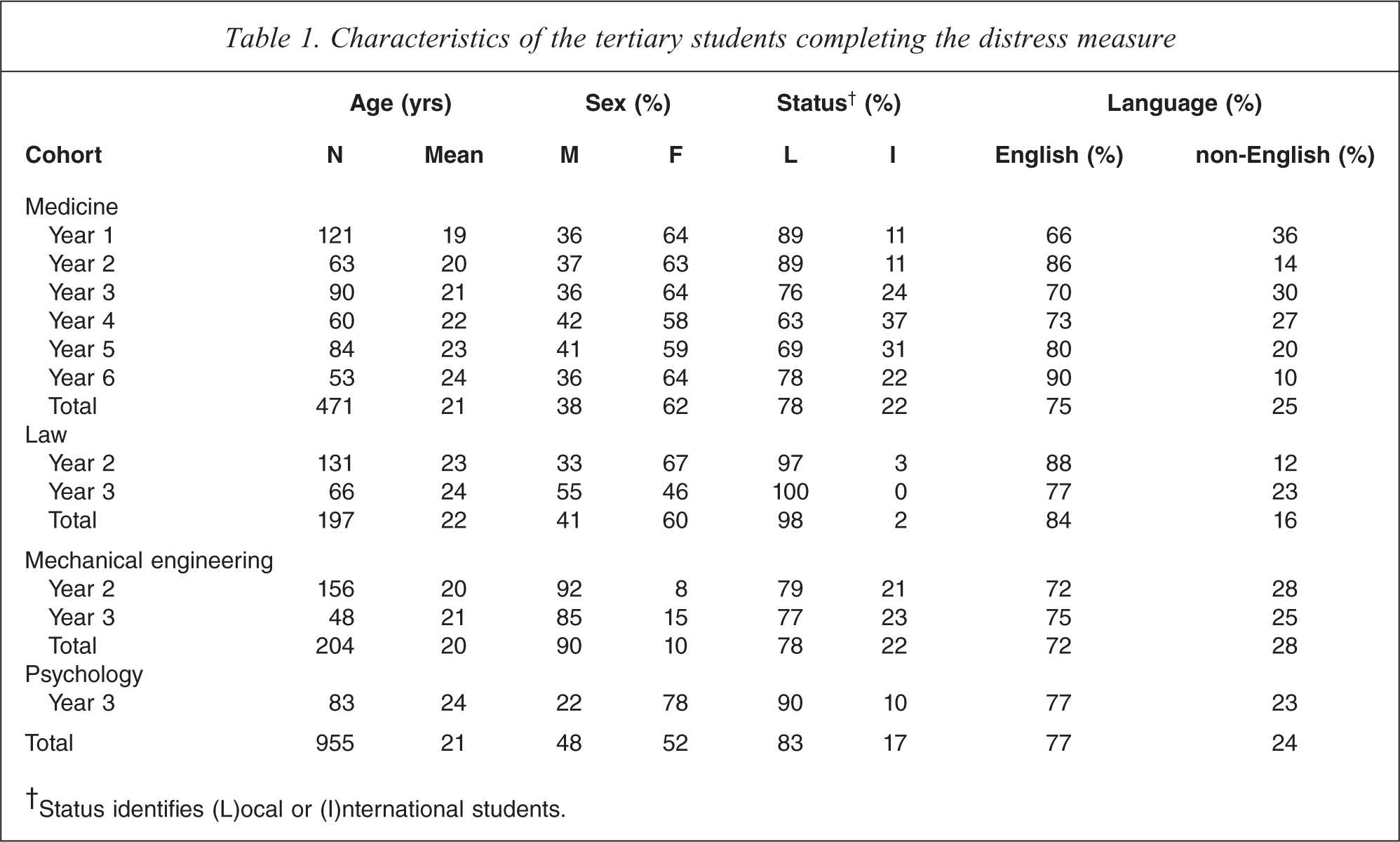
†Status identifies (L)ocal or (I)nternational students.
Distress rates
Of the tertiary students, 48% (n = 458) were psychologically distressed compared to 11% (n = 167) of their age matched population counterparts. Tertiary students were four times more likely to be classified as psychologically distressed (Relative Risk (RR) = 4.4, CI = (3.7 – 5.1), Odds Ratio (OR) = 7.5, CI = (6.13 – 9.22)) than population peers. Of the law students, 58% (n = 155) were classified as psychologically distressed, followed by 52% (n = 107) of mechanical engineering students, 44% (n = 207) of medical students and 40% (n = 33) of psychology students.
The mean K10 summary score for the tertiary student sample was 22.05 (SD = 7.20, CI = 21.59 – 22.51) with a median K10 score of 21. Student characteristics and the corresponding K10 mean scores are provided in Table 2. There were no statistically significant differences in K10 mean scores between local and international students, primary English speakers and non-English speakers, or those students based in a rural environment in the last month and those that were urban-based. There was a statistically significant difference between males and females but the effect size (d = 0.16) was trivial. Female students had a negligibly increased risk of psychological distress (RR = 1.2, CI = (1.1 – 1.4), OR = 1.4, CI = (1.1 – 1.8)). There was an overall statistically significant difference between the disciplines. This difference was most likely due to the high K10 means found in Law and Mechanical Engineering. Within these two disciplines the confidence intervals for the K10 means overlapped, but they did not overlap with the confidence intervals for Psychology and Medicine. This clustering suggested that the disciplines could be numerically and logically collapsed into a dichotomous variable consisting of health disciplines (Medicine and Psychology) and non-health disciplines (Law and Mechanical Engineering). Participants from the non-health disciplines had significantly higher K10 means than participants from the health disciplines, although the effect size was small (d = 0.30).
K10 summary score means for the tertiary student sample as a function of the students’ characteristics (sex, status, primary language, location) and discipline
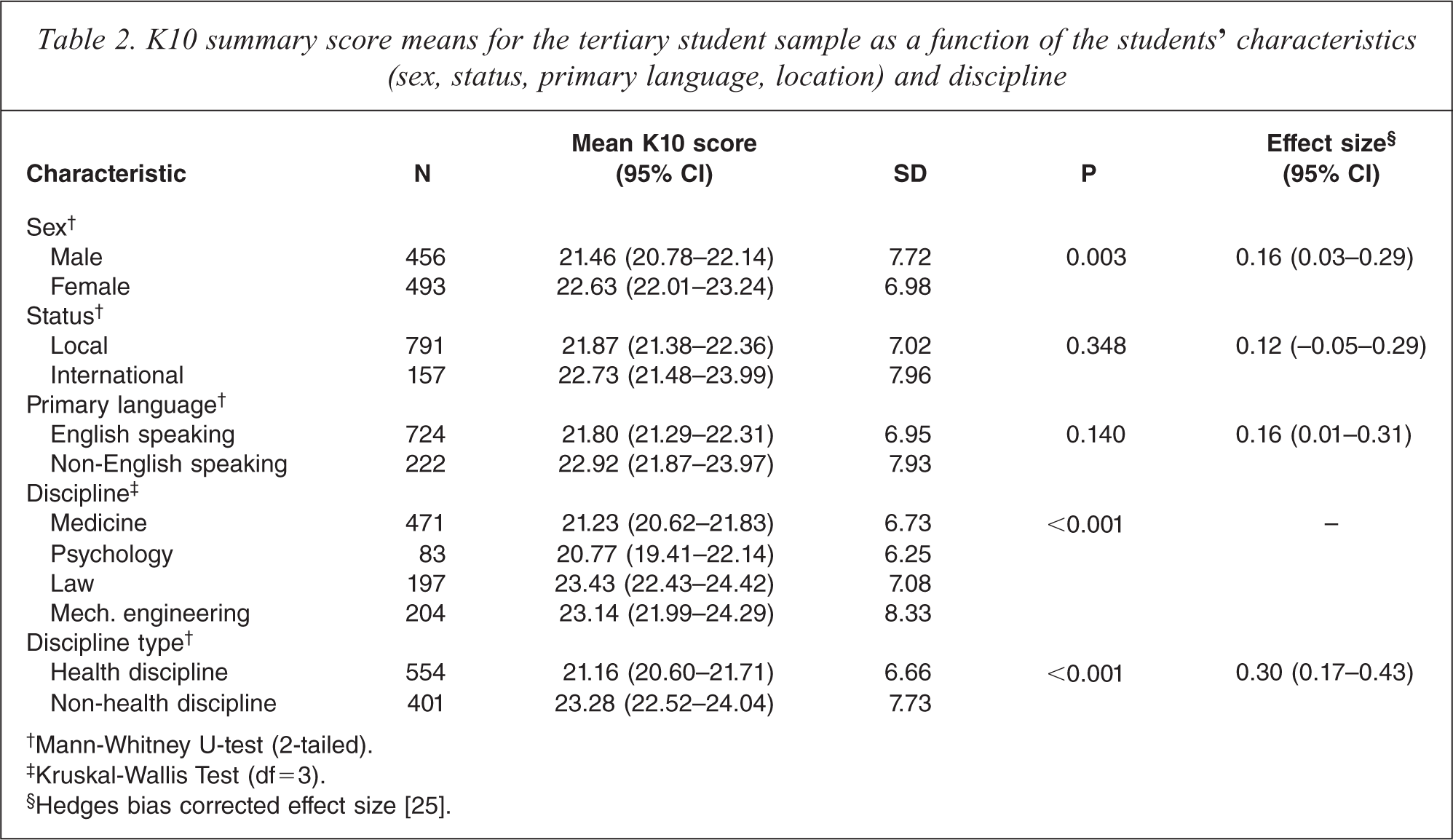
†Mann-Whitney U-test (2-tailed).
‡Kruskal-Wallis Test (df=3).
§Hedges bias corrected effect size [25].
Previous analytical comparisons between the disciplines may have been confounded by differing educational levels in the discipline samples. Distress levels were therefore analysed by comparing year level 3 students only, across all the disciplines. Eliminating educational level as a confounding factor did not markedly alter the distress level differences between the disciplines. Statistical comparisons were undertaken between all discipline combinations resulting in six comparisons. As multiple comparisons were made, a Bonferroni correction was applied to set alpha at 0.008. No statistically significant differences were detected between any of the discipline combinations under the more stringent level of alpha. Examination of the effect sizes for Psychology (M = 20.77, SD = 6.25) and Law (M = 23.3, SD = 7.23), and for Psychology and Mechanical Engineering (M = 23.96, SD = 8.7), indicate the effects were small (d = 0.38 and d = 0.44 respectively), furthermore, the confidence intervals were wide.
Educational level and distress rates
The analysis of distress level differences between year levels was only undertaken on the medical cohort data. Students from all of the six year levels of medicine participated, whereas in the non-medical disciplines only students from one to two year levels participated. In the medical school sample the proportions of psychologically distressed students varied between the year levels, although the use of the Kruskal-Wallis test did not show this to be statistically significant. Year 5 students had the highest proportion of psychologically distressed students (56%) and year 6 students had the smallest proportion at 26% (Table 3). It is evident from Table 3 that the K10 mean score peaked in year 5. At the University of Adelaide the major medical barrier examinations occur at the end of year 5 and data collection took place during the second half of this academic year when the impending examinations would have been uppermost in the students’ minds. Conversely, year 6 has the lowest K10 mean score, a year when there are no major examinations but instead a progressive summative assessment of the clinical experience.
Proportion of psychologically distressed medical students in each year level of the six-year undergraduate degree
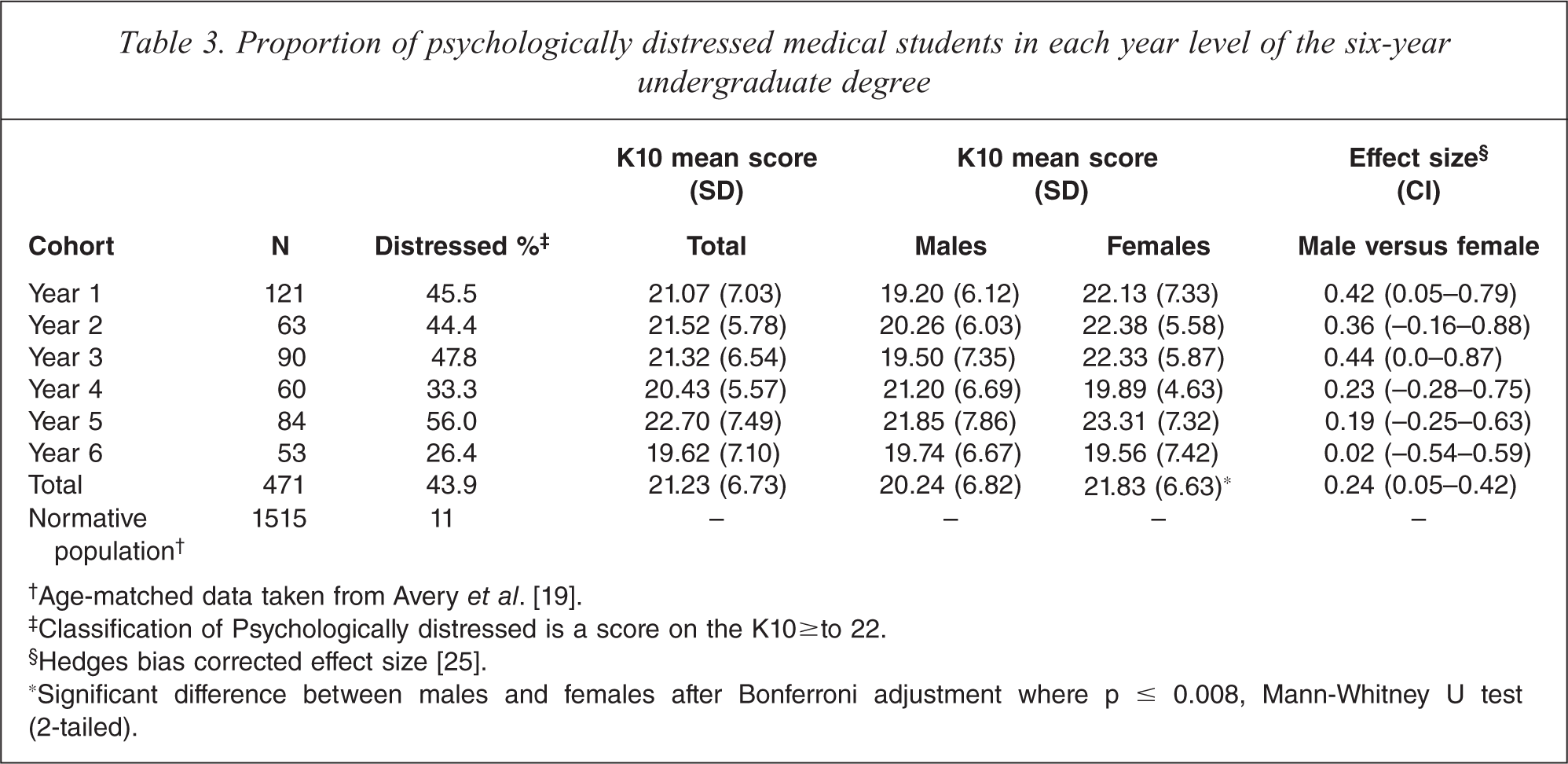
Females in years 1 to 3 had higher distress levels than their male colleagues (Table 3). The average distress level for females then dropped below the male average in year 4 (the first major clinical year), increased dramatically in year 5 (when the final barrier medical examinations were held) and then equalled the male average by year 6. These results may hint at some gender preferred learning styles, with perhaps females finding practical patient centred learning less distressing than problem based learning, which would explain the drop in distress in years 4 and 6 which are exclusively patient contact years. The sharp increase of distress levels of both males and females in year 5 are most likely attributable to the final barrier exams, where females perhaps find the situation more distressing than males.
Although an overall significant difference between the K10 mean scores for males and females was evident, there were no statistically significant differences between the females and males in any of the individual year levels after a Bonferroni adjustment was used to set the alpha level to 0.008 (Table 3). However, a small effect size was found between male/female K10 mean scores for year 1 and year 3, indicating that females had higher distress levels in these years. Larger sample sizes, had they been possible, may have increased the power of finding differences between the sexes in any given year level. Caution should be employed when interpreting these results given that the data are from one medical school only and any differences found may be an artefact of the medical school curriculum at this school.
Treatment rates
Overall, 11% (n = 103) of tertiary students reported that they had been diagnosed or treated for a mental health problem. Those participants reporting treatment had significantly higher K10 means (M = 25.94, SD = 8.02) than those who stated they were not treated (M = 21.59, SD = 6.94), U(N = 949) = 29 589.0, p <0.001. The effect size was moderate (d = 0.62).
There were considerable differences in diagnosis or treatment rates across the disciplines, with Mechanical Engineering having the lowest rate at 6% (n = 12), followed by Medicine, 10% (n = 47), then Law, 12% (n = 24) and Psychology the highest at 24% (n = 20). Overall, 48% (n = 458) of tertiary students were classified as psychologically distress, with 11% (n = 103) self reporting a diagnosis or treatment for a mental health problem.
Females were significantly more likely to report being diagnosed or treated for a mental health problem than were males (14% versus 7% respectively), z = −3.42, p <0.001, 2-tailed. Similarly, local students were more likely to be report being diagnosed or treated for a mental health problem compared to international students (12% versus 6% respectively), z = 1.98, p = 0.048, 2-tailed. There was no difference between English and non-English speakers in terms of the proportions of students diagnosed or treated for mental health problems.
Distress concern
In Study I, the web-based study, participants (Medicine year 1, year 3, year 5 rural cohort, Law year 3 and Mechanical Engineering year 3) were asked how concerned they were about their distress (N = 336). Participants responded using a four-point Likert-type scale with the options not at all (1), a little (2), moderately (3), very (4). N = 92, 27%, of tertiary students were not at all concerned by distress, 42% (n = 140) were a little concerned, and 31% (n = 104) were moderately to very concerned. N = 9, 19% of mechanical engineering students, 11% (n = 7) of law students and 8% (n = 18) of medical students reported they were very concerned. The K10 score correlated highly with the students’ concern rating rs(953) = 0.67 (CI = 0.61 – 0.73), p < 0.001.
Discussion and conclusion
Distress rates and levels
The University of Adelaide tertiary students were four times more likely to be classified as psychologically distressed than age matched peers from the South Australian population [19]. This equated to nearly half of the tertiary student sample being classified as psychologically distressed compared to 11% of age matched population peers. Other measures of distress used in the student population (e.g. Beck's Depression Inventory, CES-D, GHQ, Higher Education Stress Inventory, Major Depression Inventory and the SF-36) have also shown similar prevalence of mental health problems [11].
Comparison of K10 scores within disciplines indicated that there were more law and mechanical engineering students classified as psychologically distressed than there were not. Overall, the health disciplines (Medicine and Psychology) were slightly less distressed than their non-health counterparts. The medical literature has consistently reported increased distress rates among medical students and clinicians (primarily with comparison to general population data), and the paucity of comparative discipline data has perhaps masked the wider spectrum of the problem.
The results from this research suggest that high distress levels may be a phenomenon spread across the tertiary student body rather than limited to medical students alone. This is in line with findings from researchers in other countries [8,9]. Nevertheless, the disciplines selected for this research may have some bearing on the high rates of distress reported. Law students have previously demonstrated similar levels of distress as found in Medicine [4,6]. Since Mechanical Engineering was chosen because of its training intensity this may also explain the distress reported in this sample. Psychology is perhaps the least training intensive course and interestingly its rates of distress were the lowest of the disciplines examined but were still higher than the population sample. It is quite possible that examination of other disciplines would produce different results. The disturbing factor from all of these findings is not that one discipline may be comparatively more distressed than another, but that they all appear to be more distressed than age matched peers from the general population.
Why the tertiary student distress rates are significantly higher than age matched population peers was not investigated in this study. The changing culture of universities may well be contributing to these distress levels. Students have many competing demands including part-time work, time intensive university commitments (often found in disciplines such as medicine, law and mechanical engineering) and family obligations. These demands can minimize time for social activities and relaxation which could contribute to the rates of distress reported.
The effects of sex differences, student status and primary language spoken on distress levels
Females had significantly greater K10 scores compared to males but examination of the effect size showed this difference to be trivial. This finding reflects those of a recent Queensland study of tertiary students attending a university health service where no gender differences in distress rates were found using the same instrument [27]. Student status (local/international) or primary language (English/not English) made no difference to the K10 scores of this tertiary student sample. The sample was representative of local and international enrolled student rates, which eliminated research selection bias as an issue. The findings suggest that membership of an ethnic culture does not predispose the international students to increased distress levels.
Mental health treatment rates
Of the tertiary students, 11% indicated they had been diagnosed or treated for a mental health problem. This is slightly below the 15% rate reported in an American study [15] and the 17% by Swedish medical students [16]. Rates of diagnosis or treatment varied considerably between the disciplines with psychology students twice as likely to be treated as law and medical students, and four times as likely as the mechanical engineering students. Psychology students were on average slightly older than students from the other disciplines, and greater age has been associated with increased help seeking [28]. It is also possible that psychology students have higher levels of mental health literacy which stimulate help seeking. In the tertiary student sample, females were more likely to report treatment for a mental health problem compared to males, as were local students compared to international students. Since the discipline of psychology consisted of 78% females and 90% were local students, these ratios alone could account for the higher treatment rates seen in this discipline.
Students reporting treatment for mental health problems had significantly higher K10 scores compared to those who did not report treatment. This finding supports previous research indicating that the dominant determinant of help seeking was the severity of the mental health problem [28]. Further exploration is needed to determine other actions and strategies taken by students to deal with psychological distress other than formal treatment options.
Effects of educational level on distress levels
Overall, educational level had little effect on distress levels, as determined by comparison of K10 scores with the six year levels of medical training at this university. However, it was apparent that there were sex related differences in distress levels over time during training. These variances, although not significant overall, may be an artefact of the curriculum structure at this medical school, but they nevertheless hint at possible gender preferred learning styles. In general, distress levels remain statistically equivalent across the entire six years of the medical course, which is a disturbing result given that 44% of the medical students were classified as psychologically distressed. The cross-sectional research design allowed the possibility of cohort effects, and a prospective study may have demonstrated significant variation in distress levels during progression through the six-year medical course. Another study of distress in a six-year undergraduate medical course has found that depressive symptoms increased during the clinical training periods [13]. Given that distress levels increase even further during postgraduate training [29] there is some cause for concern and a need to understand the consequences of exposure to extended periods of distress.
Student concern about their perceived distress level
Mechanical engineering students were the most concerned (19%) about their distress, followed by law (11%) and medicine (8%). There was also a significant correlation between the concern scale and the K10 scores, indicating that the higher the K10 score the more concerned was the student. The fact that their concern shows a strong correlation with the K10 score indicates that participants had some insight into their own mental health status, but whether this amount of concern prompted help seeking was not determined.
Research limitations
In the University of Adelaide medical student sample there were proportionally more females compared to Australian national enrolments in 2007 (62% versus 53%). Thus sex differences reported in these results should be generalized to other medical cohorts with caution. However, only slight differences between the sexes were found in relation to distress levels, despite the greater proportion of females in this cohort. All of the studies were cross-sectional rather than longitudinal, thus the findings could be affected by cohort effects. Several common socio-demographic characteristics of students that have been shown to affect distress levels were not included in these studies, namely: socio economic status, employment status and relationship status.
Conclusion
These findings reveal distress rates to be much higher in the tertiary student population than in age matched population data. Future research is needed to determine whether similar rates are found amongst the non-professional disciplines, post-graduate students and in alternative universities. The low treatment rates suggest traditional models of support for students may not be sufficient or are not accepted by the student body.
Footnotes
Acknowledgements
The authors would like to thank the disciplines and students who agreed to take part in the research.