
Abstract
Adolescence is a time of rapid physical, psychological, and social development. Unfortunately, this period frequently coincides with the onset of psychiatric illness; three-quarters of lifetime psychiatric disorders will first emerge in adolescence or early adulthood [1]. Diet and nutrition modulate the pathophysiological factors underpinning depressive illness, and there are plausible reasons for examining the potential role of diet in depression [2]. We have recently demonstrated inverse associations between habitual diet quality and the likelihood of clinically determined depressive and anxiety disorders in a large, representative sample of Australian adult women [3], and between the dietary intake of magnesium, which may act as a proxy for a healthy diet, and depression in a large sample of community-dwelling Norwegian adults [4].
Two very recent prospective studies have demonstrated associations between diet quality and incident depression. In the first study of more than 10 000 Spanish adults, a lower incidence of depression was seen in individuals adhering to a Mediterranean diet [5]. In the second study, undertaken in the Whitehall II cohort, a whole food dietary pattern was associated with reduced odds, and a western dietary pattern increased odds, of self-reported depression after five years of follow up [6]. In both of these studies, the study participants were middle aged. Given the importance of adequate nutrition for optimal brain development [7] and function [8], it is of particular interest to examine whether diet quality is also related to depression in adolescents. Only one previous study, which used parental ratings of behaviour, has reported on dietary components and adolescent mental health [9]. This recent study found an inverse association between the consumption of fruits and leafy green vegetables and behavioural problems, and a positive association between a western type dietary pattern (red meat, snack and processed foods) and increased internalizing and externalizing behaviour [9].
We aimed to replicate and extend this finding using a larger sample of adolescents from a diverse range of socio-demographic backgrounds, and utilizing a tool specifically designed to measure adolescent depression by self-report. We hypothesized that a poor quality diet would be associated with higher rates of depression, and a better quality diet related to lower rates, in both males and females in early adolescence. We further hypothesized that the posited associations would only be partly explained by demographic, family, lifestyle, eating behaviour, socioeconomic and other potential confounding factors.
Methods
Participants
The Healthy Neighbourhoods Study was a large observational study conducted in 231 Australian schools in 2006, and focusing on adolescent health and wellbeing. The participants (n = 8255) were year six and year eight students from 30 communities across three states, stratified by level of socio-economic disadvantage. Socio-economic status (SES) was determined using Socio-Economic Index For Areas (SEIFA) scores, based on 2001 Australian census data. The chosen index was the Index of Relative Socio-economic Advantage/Disadvantage (IRSAD), which accounts for high and low income, and the type of occupation from unskilled employment to professional position. A low score as measured by IRSAD identifies the most disadvantaged (quartile 1), and a high score identifies the most advantaged (quartile 4). Half the communities were from regional areas and the other half were from urban areas. A random selection of schools in the selected areas were invited to participate in the survey and just over half (53%) agreed. There was little difference in the participation rate for the education sectors (government, independent and Catholic). Students required parental consent to participate in the survey. The return rate of the consent forms varied across schools, however 92% of the parents who did return the consent forms at year six level gave their permission for their children to participate, and at year eight, 89% consented. Those with missing data on any of the key variables (dietary questions, mental health indicator, or covariates included in analyses) were excluded from analyses (n = 1141, 13.8 %), resulting in a final sample of 7114 adolescents aged 10–14 years (mean = 11.6 years, SD = 0.81).
The Royal Children's Hospital Human Research Ethics Committee and relevant school and institutional ethics committees in each state provided ethical approval for the study.
Dietary measures
The Healthy Neighbourhoods Study included a 14-item dietary questionnaire based on a questionnaire used in the Amherst Health and Activity Study Adult Survey of Child Health Habits [10] and modified to include additional questions about the consumption of breakfast, different types of beverages, and takeaway food. Some items were modified to Australian equivalents. The questionnaire was designed to assess dietary patterns associated with positive energy balance and food behaviours and measures the intake of key foods that are indicative of less/more healthy food choices.
Based on Dietary Guidelines for Children and Adolescents in Australia [11], a healthy diet score was constructed from answers to four dietary items (response options 1–6: none through to five or more serves per day). Participants were given a point for each of the following: breakfast everyday before school; low fat dairy food at least once per day; at least two serves of fruit per day; and at least four serves of vegetables per day. The range for the final score was zero (no points) to four, which was subsequently recoded as categories 1 (low healthy diet) to 5 (high healthy diet). An unhealthy diet score was derived from the sum of answers to the following four questions: consumption of hamburgers, hot dogs or sausages; potato crisps or savoury snacks; biscuits, doughnuts, cake, pie or chocolate; and sweet drinks such as soft drinks, cordial, Big M, flavoured mineral water etc. (response options 1–6: none through to five or more serves per day); plus a question regarding the frequency of takeaway foods (response options 1–6: less than once per month through to most days). The possible range for the unhealthy diet score was thus 5–30. The unhealthy diet score was subsequently categorized into quintiles (Q1 ≤ 8, Q2 = 9–10, Q3 = 11, Q4=12–14, Q5≥15).
Mental health
Depression was measured utilizing the Short Mood and Feelings Questionnaire (SMFQ), an instrument designed for use in epidemiological studies of depression for children and adolescents [12]. The SMFQ comprises 13 items relating to mood states (scale 0–2, yielding total score ranging from 0 to 26), has high internal consistency (α≥ 0.85), and correlates with other well-validated measures such as the Children's Depression Inventory (CDI) and the Diagnostic Interview Schedule for Children (DISC) depression scale [12].
Covariates
SES was categorized using IRSAD scores, described above. Father and mother's work status comprised three categories: zero (not working, retired, or not cohabitating), one (part-time work), and two (full-time work). Father and mother's education also comprised three categories: one (did not complete high school), two (completed high school), and three (has a university degree). Family environment was measured using two scales developed for the Communities That Care youth survey [13]. Poor family management was assessed using nine questions, including questions such as “would your parents know if you did not come home on time?” and “the rules in my family are clear”. Family conflict was measured with three questions, including “people in my family have serious arguments” and “people in my family often insult or yell at each other”. Both scales had a four-point response scale (NO!, no, yes, YES!), and were subsequently dichotomized to represent low (mean ≤3) and high (mean >3) risk. Attitudes to eating were assessed using the Adolescent Diet Scale [14] and comprised the sum of eight questions with response options ranging from zero (seldom/never) to four (almost always). The scale included questions such as “Do you try to avoid ‘fattening’ foods or foods with sugar in them?” and “Do you skip meals other than breakfast because you are watching your weight?”. Physical activity level was based on the question: “Over a normal week, on how many days were you physically active for a total of at least 60 minutes per day?” with scores ranging from zero through to seven (subsequently recoded as 1–8). Smoking was based on the question “in the last 30 days have you smoked cigarettes” and comprised the categories zero (no) through to four (10 or more times). Body mass index (BMI) was calculated, from measurements made at the time of data collection, as weight/height2 (kg/m2).
Statistical analysis
Total SMFQ scores were calculated, and a dichotomized depressive symptomatology variable was created using the cut-point value (≥ 8 = symptomatic) suggested by Angold et al. [12]. Independent samples t-tests and Chi-square analyses were used to test for differences on the covariate measures according to the depressive subgroups. Associations between diet scores and other variables were measured using Pearson's r or Spearman's rank correlation coefficient (Spearman's rho). Those categorized in extreme quintiles/categories of diet score were also identified.
Logistic regression models were developed to estimate odds ratios with 95% confidence intervals using symptomatic depression (no/yes) as the outcome variable and diet quality scores as the exposures of interest. Covariates including age, gender, SES, father's and mother's education and work status, physical activity, smoking, BMI, family conflict, poor family management, and dieting behaviour, were tested against depression in univariate analyses, then added sequentially to the models in order to assess the relative impact of each on the relationship of interest. Effect modification by age or gender was also assessed. A separate analysis assessed differences between those included/not included in the analyses on the basis of missing data. All analyses were conducted using SPSS (V16) and statistical significance accepted as p < 0.05.
Results
The median SMFQ score was 5 Interquartile range (IQR = 2–10). Neither age nor gender was an effect modifier. Table 1 presents characteristics of the study participants above and below the symptomatic cut-off (≥ 8 = symptomatic) for the SMFQ. Comparisons indicated that a higher proportion of those categorized as symptomatic were female; less physically active; smoked cigarettes; were in the risk category for both family conflict and poor family management; had lower SEIFA scores; had higher dieting scores; and had a father who was not employed in full-time work and did not have a tertiary degree.
Characteristics of study sample (n = 7114): Short Mood and Feelings Questionnaire (SMFQ) non-symptomatic versus SMFQ symptomatic. Results presented as mean (±SD), median (IQR), or N (%)
A higher proportion of those not included in the final analyses on the basis of missing data were from lower SES backgrounds; had parents who were less likely to be working full-time and with lower educational levels; and were at risk for family conflict and poor family management. They were also slightly younger, and had higher scores on the Adolescent Dieting Scale. However, there were no differences observed on total SMFQ scores or in the proportions of those symptomatic on the SMFQ.
Table 2 presents correlations between both healthy and unhealthy dietary scores and covariates. A higher healthy diet score was associated with: younger age; more physical activity; less smoking; higher paternal and maternal education; higher paternal employment status; higher SES; lower risk of family conflict and poor family management; and a higher dieting score. In contrast, an unhealthy diet was associated with: being male; a lower dieting score; less physical activity; greater family conflict and poor family management; smoking; lower parental employment and education status; a lower BMI; and lower SES. Most of these correlations were weak, however, and statistically significant as a function of the large sample size.
Correlations (Pearson's r or Spearman's Rho) between diet scores and covariates
Signifcance:∗p < 0.01, ∗∗ p < 0.001.
Table 3 presents results of the logistic regression analyses, with scores on the healthy diet score as exposures against symptomatic depression. Compared to individuals with the lowest score on the healthy diet scale, being in the category with the highest score (5/5) nearly halved the likelihood of being symptomatic. The inverse relationship of healthy diet score to symptomatic depression was apparent both before and after adjustments for age, gender, physical activity, father's work status, SES, adolescent diet scale, and family conflict and largely followed a dose-response curve. Adjustment for the variables of smoking, father's education, mother's education and work status, poor family management and BMI, did not attenuate the relationship between diet scores and symptomatic depression, and these variables were not included in the final models. Figure 1 presents the mean SMFQ scores (and 95% confidence intervals) for each category of healthy diet score, and demonstrates that the pattern of association between dietary scores and SMFQ scores is concordant with the odds ratios for symptomatic depression.
Odds ratios (95% confidence intervals) for symptomatic depression across categories/quintiles of healthy and unhealthy diet scores (n= 7114)
aAdjusted for age, gender, physical activity, father's work status, socio-economic status, adolescent diet scale, and family conflict.
Mean total Short Mood and Feelings Questionnaire score (95% CI) for each category of healthy diet score.
Table 3 also presents odds ratios for symptomatic depression across quintiles of unhealthy diet score. In this analysis, quintiles two, three, four and five are compared to quintile one (lowest) on the unhealthy diet scale. Results indicated a significant, dose-response relationship between unhealthy diet and odds of being symptomatic for depression. After adjustments for age, gender, physical activity, father's work status, SES, adolescent diet scale, and family conflict, being in the highest quintile of unhealthy diet score increased the likelihood of symptomatic depression by nearly 80% when compared with those in the lowest quintile. Again, adjustments for smoking, father's education, mother's education and work status, poor family management and BMI, did not alter these relationships. Figure 2 presents the mean SMFQ scores (and 95% confidence intervals) for each quintile of the unhealthy diet score, concordant with the odds ratios for symptomatic depression.
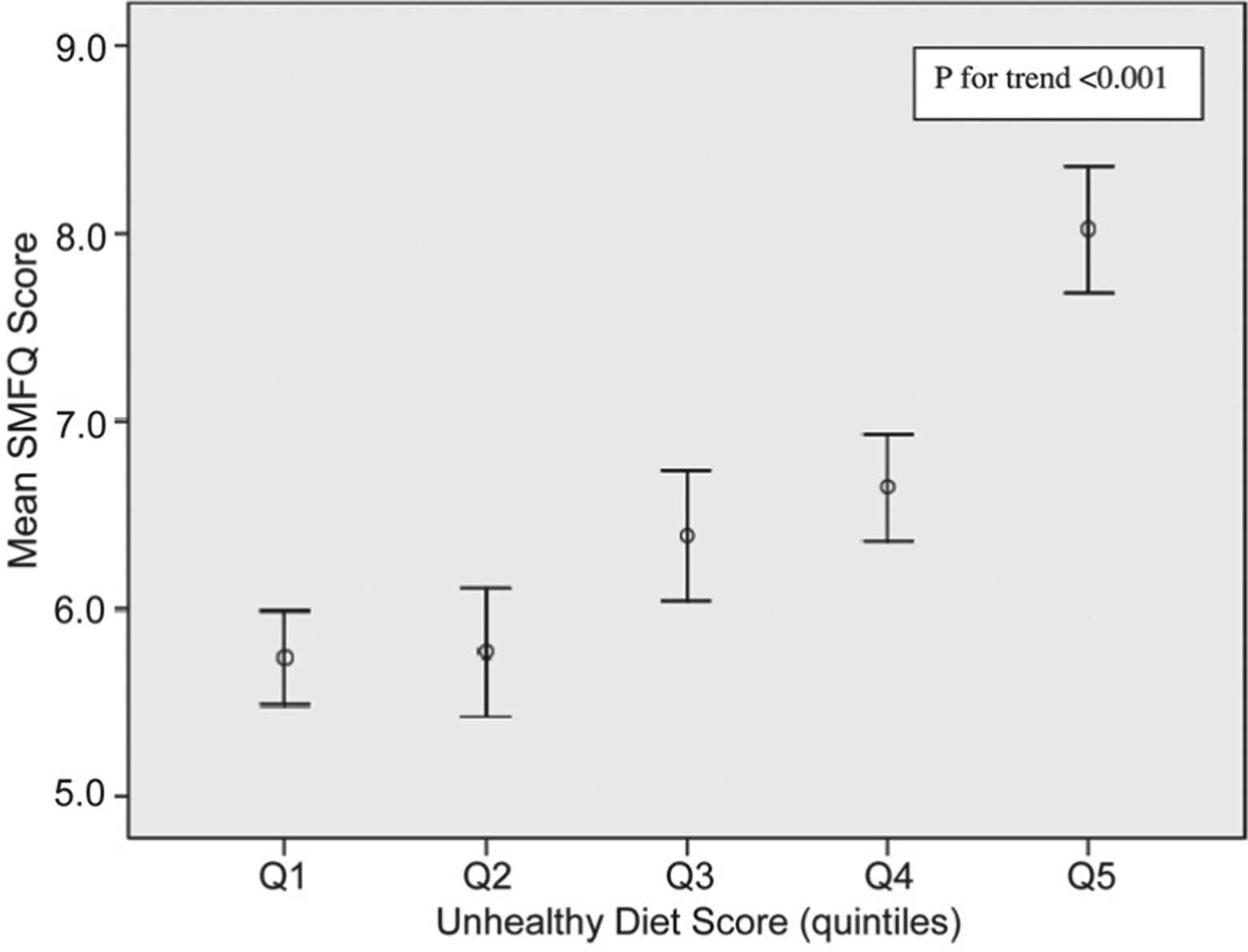
Mean total Short Mood and Feelings Questionnaire score (95% CI) for each quintile of unhealthy diet score.
Finally, an analysis of extreme quintiles/categories of diet scores indicated that individuals with a low healthy diet score were not the same participants as those with high scores on the unhealthy diet; of those in the lowest two categories for a healthy diet, only 515 (7.2%) of these participants fell also into the top two quintiles for an unhealthy diet. Of those in the top two categories for a healthy diet, however, 1557 (21.9%) were also in the lowest two quintiles on the unhealthy diet score.
Discussion
In this study we report that both a lower adherence to the consumption of foods promoted by the Dietary Guidelines for Children and Adolescents in Australia [11] and recognized as important components of a healthy diet, and greater consumption of unhealthy and processed foods, are associated with increased odds for self-reported symptomatic depression in adolescents. These relationships remained robust after adjustment for a wide range of potential confounding factors.
These findings support previous research reporting associations between diet quality and mental health outcomes in adolescents [9], and between diet quality and depression in adults, both cross sectionally [3] and longitudinally [5,6]. They suggest that both low intakes of nutrient-dense foods, and/or high intakes of high-energy, nutrient-poor foods are related to an increase in the likelihood of adolescents being depressed. However, it would seem that an increase in the risk for symptomatic depression related primarily to those scoring at the extremes of the dietary ranges, with a significant decrease in the odds ratio for depression associated with even one healthy dietary practice, and less difference evident between the subsequent categories. Only a small number of individuals who were low on the healthy diet score were also high on the unhealthy diet score, indicating that the highest odds for depression according to the different measures of dietary intake were not seen in the same individuals. It appears that adolescents with a low healthy diet score do not necessarily replace their healthy foods (such as fruits, vegetables and low fat dairy), with less healthy options (such as sweets, savoury snacks and takeaway foods), but may instead consume a limited range of other foods, such as bread, cereals, and meat. Conversely, a larger number of individuals scored both high on the healthy diet score and low on the unhealthy diet score, indicating that those eating a healthier diet are less likely to additionally eat unhealthy and processed foods on a regular basis.
In interpreting these results, the characteristics of this study should be considered. A particular problem in the study of diet and disease is the potential for associations to arise because of confounding by factors in the individual's background and social context. We were able to assess SES at the household (parent's work and educational status) and the area level (IRSAD scores), as well as self-reported health behaviours (physical activity and smoking). Moreover, important aspects of family environment (conflict and poor family management) that are likely to have an impact on both diet and mental health in adolescents were included as potential confounders. The demonstrated associations between diet and depression status were robust after adjustments for these factors, however it is not possible to rule out residual confounding as an explanation for these findings.
Due to the cross-sectional design of this study, the direction of the relationship between diet and depression cannot be determined. Appetite changes are a common feature of major depressive disorder in adults [15] and dietary choices may be influenced by mental health status. Adolescents are often concerned with physical appearance, body weight and shape [16], and food choices may be associated with unhealthy weight control behaviours, which may also be related to depression [17]. In this study, however, we were able to assess adolescents’ attitudes to food and dieting and exclude unhealthy dieting behaviours as a confounder in the relationship between diet quality and depression. Moreover, previous longitudinal research [5,6] does not support the reverse causality hypothesis.
The questions that were used to assess healthy diet quality did not include several other accepted components of a healthy diet (such as wholegrains, olive oils, and fish), while the unhealthy diet questions may not have captured all aspects of unhealthy food consumption (e.g. white bread, sweet spreads, fatty and processed meats). Nor did we have information regarding the composition of breakfasts consumed. There is likely to have also been some degree of social desirability bias in the answers to questions regarding the frequency of fruit and vegetable consumption, as guidelines regarding the adequate intake of fruit and vegetables are likely to be familiar to many students through educational programs directed at this age group. Moreover, bias may have also resulted from differential dietary reporting by those with depressive symptoms. The survey items used may be less accurate than more in-depth measures of dietary intake, such as 24-hour dietary recall or food frequency questionnaires. However, given that such measures may be unreliable in adolescents [18], simpler dietary questionnaires such as we have used, are likely to afford sufficient information to adequately rank individuals in terms of their diet quality [19].
There were observed differences between those included in the analyses and those not included on the basis of missing data; those not included were from more disadvantaged backgrounds and had higher dieting scores. Regardless, there were no differences between the groups on the outcome measure, and, as adolescents from disadvantaged backgrounds were more likely to have poorer quality diets, any bias is likely to tend towards under-rather than over-estimation of the reported associations. The Healthy Neighbourhoods Study sample cannot be considered as representative of the population, as it was selected to equally represent the quartiles of SES and rural/urban location. As such, these results may not be generalizable to the population. However, the inclusion of adolescents from a wide range of socio-demographic backgrounds, the stringent measures employed to address issues of confounding, and the use of a valid and reliable measure of self-reported depression [12] are all important strengths in this study. Finally, the large sample size allowed for the effects of multiple interacting variables of small effect to be determined.
While residual or unmeasured confounding may explain these results, several biological mechanisms could also explain the demonstrated relationship between adolescent diet and depression. A poor quality diet may influence depressive status via two pathways: both by increasing the risk of nutrient deficiencies, which are associated with depression [20,21], as well as the duration [22] and severity [23] of depressive illness, and by having a direct detrimental impact on biological systems that underpin the pathogenesis of depression [2]. For example, experimental data indicate that a diet high in saturated fat activates the stress response system and reduces the ability of normal feedback mechanisms to return the stress system to homeostasis [24,25]. High fat and high sugar diets also promote obesity and insulin resistance, which in turn contribute to systemic inflammation [26]. Dietary factors such as a high glycemic load diet [27] and a western type dietary pattern [28] are also associated with increased systemic inflammation. Pro-inflammatory cytokines are thought to directly mediate many of the behavioural, neuroendocrine, and neurochemical changes seen in depressive illnesses [29].
Nutritional exposures during periods of rapid growth may also impact on the risk for depression via a detrimental impact on brain development and plasticity, and by modifying gene expression. Adequate nutrition in childhood appears to be essential for the optimal development of the human brain [30], and brain derived neurotrophic factor (BDNF) may be of particular interest as it plays a central role in neurogenesis and is also regarded as a crucial factor in depressive illness [31]. In animal models, a high-fat, refined sugar diet reduces levels of BDNF within 3 weeks, with a resulting impact on functioning that is independent of nutritional deficits, obesity or insulin resistance [32]. Moreover, increasing evidence from the nascent field of nutrigenomics indicates that nutrients have the potential to alter gene expression during critical periods of development [33,34]. As such, nutrition perinatally or in early life may have the potential to influence later health via its capacity to alter gene expression and cell function over the long term [35].
Conclusion
We have demonstrated cross-sectional relationships between the quality of adolescents’ diets and their depression status. These relationships were not fully explained by age, gender, SES, family environment, problematic dieting behaviours, body habitus, or lifestyle behaviours other than diet, however reverse causality and/or residual or unmeasured confounding cannot be ruled out as explanations for these findings. Nevertheless, these results are concordant with recent studies in adults [3,5,6], and support the hypothesis that poor quality diets play a role in increasing the risk for adolescent depression. If further longitudinal studies confirm these associations, the potential exists for the development of an evidence-based strategy for the primary prevention of adolescent depression, based in part on dietary modification. Such modifications would align with other current public health strategies aimed at reducing the impact of child and adolescent obesity [36], and hold the promise of reducing the burden of depression in the community.
Footnotes
Acknowledgements
An NHMRC Project Grant #334304 funded the Healthy Neighbourhoods Study. Associate Professor Leslie is supported by an NHMRC Public Health Fellowship #301261. Professor Toumbourou is supported by a VicHealth Senior Research Fellowship. Dr Jacka was the recipient of postgraduate scholarship funding from the “Australian Rotary Health” and is supported by NHMRC project grant #454356.
The funding providers played no role in the design or conduct of the study; collection, management, analysis, and interpretation of the data; or in the preparation, review, or approval of the manuscript.
Dr Jacka had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.