
Abstract
An explicit assumption of current classification schemes for the eating disorders is that it is useful to distinguish between eating disorders characterized by the use of purging behaviours, namely self-induced vomiting and/or misuse of laxatives or diuretics, and those not involving the use of these behaviours. In the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) [1], this is signified by the separation of anorexia nervosa (AN) into binge/purge and restricting subtypes, and of bulimia nervosa (BN) into purging and non-purging subtypes. Non-purging weight control behaviours include extreme dietary restriction, excessive exercise and the use of diet pills.
Subtyping of AN is generally supported by the evidence, in that AN patients who report binge eating and/or purging behaviours have been found to have higher levels of eating disorder and comorbid psychopathology, poorer impulse control, and poorer quality of life, than restricting AN patients [2, 3]. Similarly, it is often assumed that the occurrence of purging behaviours indicates a more severe form of BN [2] although evidence for the subtyping of BN is less compelling. Interpretation of findings from early studies [3–6] is complicated by the fact that non-purging BN (BNNP) was often defined solely by (the occurrence of binge eating and) the absence of purging behaviour, as opposed to the presence of non-purging methods of weight control. As a result, many individuals receiving the diagnosis of BNNP will have met criteria for the DSM-IV trial category of binge eating disorder (BED) – a disorder characterized by binge eating in the absence of extreme weight control behaviours – rather than BNNP. Like AN and BN, BED is associated with high levels of comorbidity with anxiety and affective disorders and poor quality of life [3, 7]. In addition, BED is associated with obesity and poor overall health [7]. Further, BED appears to be more common than both AN and BN [8].
More recent, better designed, studies have produced conflicting results concerning the validity of BN subtyping [9–11]. Walters et al. [9] found no differences between purging and non-purging bulimics with respect to demographic and personality variables, and rates of depression, anxiety disorders and alcoholism, in a population-based sample of twins. In a clinical sample of individuals with BN-type eating disorders, Tobin et al. [10] found no differences between purging and nonpurging BN subgroups on measures of eating disorder psychopathology and general psychiatric disturbance. In contrast, Garfinkel et al. [11], in a very large communitybased sample, found that purgers had higher rates of comorbidity for depression, social phobia and alcohol dependence, as well as prior sexual abuse and parental discord, than non-purgers.
Evidence concerning the relationship between BN and BED is also conflicting. In a community-based study of women with recurrent binge eating, Hay and Fairburn [12] found no significant differences between participants with BED and those with BNNP on measures of general psychopathology, self-esteem and social adjustment. However, individuals with purging BN had more severe eating disorder symptoms, more severe general psychiatric symptoms and poorer social adjustment than those with BED. In addition, participants in both BN sub-subgroups had a poorer outcome at 12months than those with BED. The authors suggested that bulimic eating disorders may exist on a continuum of severity, nonpurging BN being intermediate in severity between BED (least severe) and purging BN (most severe). In contrast, Striegel-Moore et al. [13] found no significant differences between women with purging BN, non-purging BN and BED with respect to weight or shape concerns and current or lifetime prevalence of nine major DSM-IV axis I disorders. However, women with BED were older and less likely to have received treatment specifically for a problem with eating than those with purging BN, and were more likely to be overweight or obese than women in either BN subgroup.
Of note is that in both Hay and Fairburn's [12] and Striegel-Moore et al.'s [13] studies, the number of cases of BNNP was small. This may reflect, in part, the stringent criteria for the non-purging methods of weight control suggested in DSM-IV [1], namely regular ‘fasting’ and/or exercise that ‘… occurs at inappropriate times or in inappropriate settings or continues despite injury or other medical complications’ (p.546). By contrast, in Garfinkel et al.'s study [10, 14], in which ‘strict dieting’ and/or ‘regular exercise’ to prevent weight gain were sufficient for the diagnosis of BNNP, the prevalence of BNNP was approximately three times that of purging BN. The use of these more liberal criteria for BNNP may also explain the greater psychiatric disturbance of participants with the purging form of BN in Garfinkel et al.'s study.
The diagnosis of BNNP is particularly uncommon in clinical samples of BN patients, and this is the case irrespective of the way in which the non-purging methods of weight control are defined [10, 15]. This might simply reflect higher levels of general psychological distress and/or functional impairment – and in turn a greater likelihood of treatment being sought – associated with the use of purging behaviours. However, it also is possible that bulimic-type eating disorders not involving the use of purging, namely BNNP and BED, may not readily be recognized as psychiatric disorders by those affected, or by primary care practitioners, and may therefore be less likely to be referred to specialist treatment than those involving purging [13]. In general, the use of clinical samples in informing the classification of BN-type eating disorders is problematic, because individuals with these disorders receiving specialist treatment have been found to be atypical in a number of ways [16].
To inform the classification of BN-type eating disorders, we compared levels of eating disorder psychopathology and functional impairment associated with the use of purging and non-purging methods of weight control in a large community-based sample of women reporting regular binge eating episodes. The prior use of health services was also compared between subgroups. In view of the increasing evidence concerning the clinical significance of BED, we were also interested to consider the characteristics of individuals reporting recurrent episodes of binge eating in the absence of extreme weight control behaviours.
Method
Design and participants
The research was conducted as part of the Health and Well-Being of Female ACT Residents Study, a large-scale epidemiological study of disability associated with the more commonly occurring (bulimictype) eating disorders among young adult women in the community. Participants were residents of the Australian Capital Territory (ACT) region (population 323 000), which includes the city of Canberra.
Self-report questionnaires were posted to a sample of 10 000 female ACT residents aged 18–42 years, selected at random from the electoral roll and stratified by age in 5-year bands as follows: 18– 22 years; 23–27 years; 28–32 years; 33–37 years; 38–42 years. Individuals in the first and third of these age bands were slightly oversampled because data from a pilot study indicated that individuals with incorrectly listed addresses were over-represented among participants in these age groups [17]. The questionnaire included measures of eating disorder psychopathology, health-related quality of life (functional impairment), general psychological distress, and health-service utilization. Body mass index (BMI, kg/m2)was calculated from self-reported height and weight. Previously we found a very high correlation (r = 0.97) between BMI calculated in this way and BMI calculated according to measured height and weight [18].
Completed questionnaires were received, following reminder letters, from 5255 individuals, which represented a response rate of 57.1% after incorrectly listed addresses (n = 684) and individuals away from home at the time of the survey (n = 112) were taken into account. This is a conservative estimate of true response because not all individuals with incorrectly listed addresses will have been identified [17]. Only information concerning age was available for non-respondents. However, a detailed analysis of pilot data found no evidence for the existence of non-response bias [19]. The sample comprised approximately 10% of the total population of females aged 18–42 in the ACT region and was representative of this populationwith respect to marital and employment status, education, children and first language [20].
The ACT is a highly urbanized region and this was reflected in the characteristics of participants. Thus, 85.3% of participants were born in Australia and 91.8% had English as a first language. Approximately 90% had completed 12 or more years of formal education and close to half (47.4%) had completed some form of tertiary study, including 12.5% who had completed a postgraduate qualification. Fifty-five per cent of participants were married or living as married, 43.8% had one or more children, 62.8% were currently employed either full- or parttime, 15.6% were full-time students, and 17.5% nominated home duties as their main activity. The mean age of participants was 30.26 years (SD = 7.22). Mean BMI was 24.52 kg/m2 (SD = 5.25).
Measures
Eating Disorder Examination Questionnaire (EDE-Q)
The EDE-Q [21] is a 36-item self-report measure derived from the Eating Disorders Examination interview (EDE) [22], the latter being the accepted ‘gold standard’ in the field [23]. The EDE-Q focuses on the past 28 days and is scored using a seven-point, forced-choice, rating scheme. Subscale scores – relating to dietary restraint, eating concerns, concerns about weight and concerns about shape – and a global score, may be derived from the 22 items addressing attitudinal aspects of eating-disorder psychopathology [24]. A high level of agreement between EDE-Q and EDE subscale scores has been shown in both community and clinical samples [18]. Frequencies of eating disorder (i.e. overeating and compensatory) behaviours are assessed in terms of the number of episodes occurring during the past 4weeks. These items do not contribute to subscale scores. Two types of ‘overeating’ episodes are assessed, those in which a loss of control is experienced and an objectively large amount of food is consumed (objective bulimic episodes, OBEs), and those in which a loss of control is experienced but in which the amount of food consumed is not objectively large (subjective bulimic episodes, SBEs). The regular occurrence of OBEs is required for the diagnoses of BN and BED in DSM-IV [1].
Medical Outcomes Study Short-Form disability scale (SF-12)
The SF-12 [25] is a 12-item measure of health-related quality of life derived from the 36-item form [26]. Items of the SF-12 are summarized into two weighted scales (Physical Component Summary scale, PCS; Mental Component Summary scale, MCS), designed to assess impairment in everyday functioning associated with physical and mental health problems. Each scale is scored to have a mean of 50 and standard deviation of 10 (in the US population), with lower scores indicating higher levels of impairment. The SF-12 has robust psychometric properties [27] and its validity in the Australian population has been shown [28]. In this study the MCS was the primary measure of functional impairment. A score of 40 or less on the MCS is considered indicative of moderate impairment, while a score of 30 or less indicates severe impairment [28]. Scores on the measure of general psychological distress (K-10) [29] were highly correlated with those on the MCS (r = 0.76) and therefore are not reported.
Health service utilization
Participants were asked whether they had ever sought professional help for a problem with eating or weight. A ‘yes’ response to this question was followed by a second question concerning the nature of the problem for which help was sought, namely ‘a problem with eating, such as “feeling out of control with your eating”’; ‘a problem with weight, such as “concern about the effect of being overweight on health”’; and ‘a problem with both eating and weight’. For the present purpose, the latter two categories were collapsed and contrasted with the first category.
Definitions of binge eating, purging and non-purging behaviours
Recurrent (or ‘regular’) binge eating was defined as the occurrence, on average, of one or more OBEs per week during the past 4weeks. This threshold was chosen in preference to the DSM-IV criterion of twice per week, because evidence for the validity of the latter is weak [2] and because we found acceptable agreement between EDE-Q and EDE assessment of recurrent OBEs, defined in this way, in pilot work (κ = 0.53, t = 7.98, p < 0.001) [18]. Participants who reported regular (i.e. at least weekly) use of self-induced vomiting, laxatives or diuretics, in order to influence weight or shape, and who did not report regular use of non-purging methods of weight control, namely excessive exercise, extreme dietary restriction, or diet pills, were defined as ‘purgers’. Participants who reported hard exercise for weight or shape reasons at least daily, going without food for periods of 8 or more waking hours in order to influence weight or shape every day, or almost every day, or regular use of diet pills, and who did not report regular purging behaviours, were defined as ‘non-purgers’. The above definition of extreme dietary restriction was chosen because the DSM-IV criterion of regular ‘fasting’ may be overly restrictive [30].
The prevalence of specific eating disorder behaviours in the total sample as assessed by the EDE-Q is given in Table 1. Of the 559 participants (10.6% of the total sample) who reported recurrent episodes of binge eating, 442 (8.4%) did not report the regular use of either purging or non-purging weight control behaviours (‘non-compensating binge eaters’), 41 (0.8% of the total sample) reported the regular use of purging, but not non-purging, behaviours, and 62 (1.2%) reported the regular use of non-purging, but not purging, behaviours. Fourteen individuals (0.3%) reported regular episodes of binge eating and the regular use of both purging and non-purging methods of weight control.
Per cent (%) frequency of regular (at least weekly) occurrence of specific eating disorder behaviours (past 4 weeks), in young adult women (n = 5255)
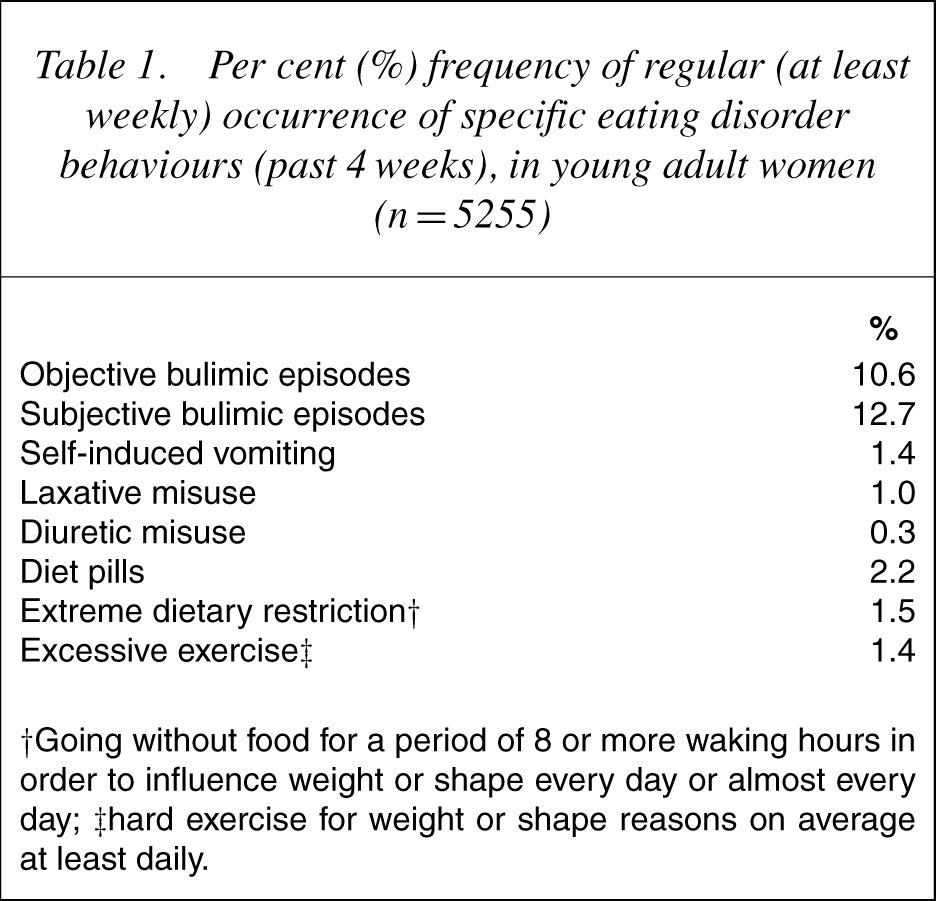
† Going without food for a period of 8 or more waking hours in order to influence weight or shape every day or almost every day; ‡hard exercise for weight or shape reasons on average at least daily.
Statistical analysis
Data were first inspected for normality. Analysis of variance was used to compare mean scores on continuously distributed dependent variables, namely EDE-Q global scores and scores on the SF-12 MCS, as well as age and BMI, between subgroups of binge eaters. Data for individuals not reporting regular episodes of binge eating were included for comparative purposes. Data for participants (n = 14) who reported (regular episodes of binge eating and) both purging and non-purging methods of weight control were excluded on account of the small size of this subgroup. Post-hoc tests were used to identify the source of any F-values significant at the 0.05 level. Tukey's HSD test was used for this purpose because this method takes into account the use of multiple comparisons without being overly punitive. Logistic regression was used to compare use of health services between subgroups. Linear regression was used to identify the eating disorder behaviours that best predicted functional impairment, as measured by the SF-12 MCS, among participants reporting regular episodes of binge eating.
Results
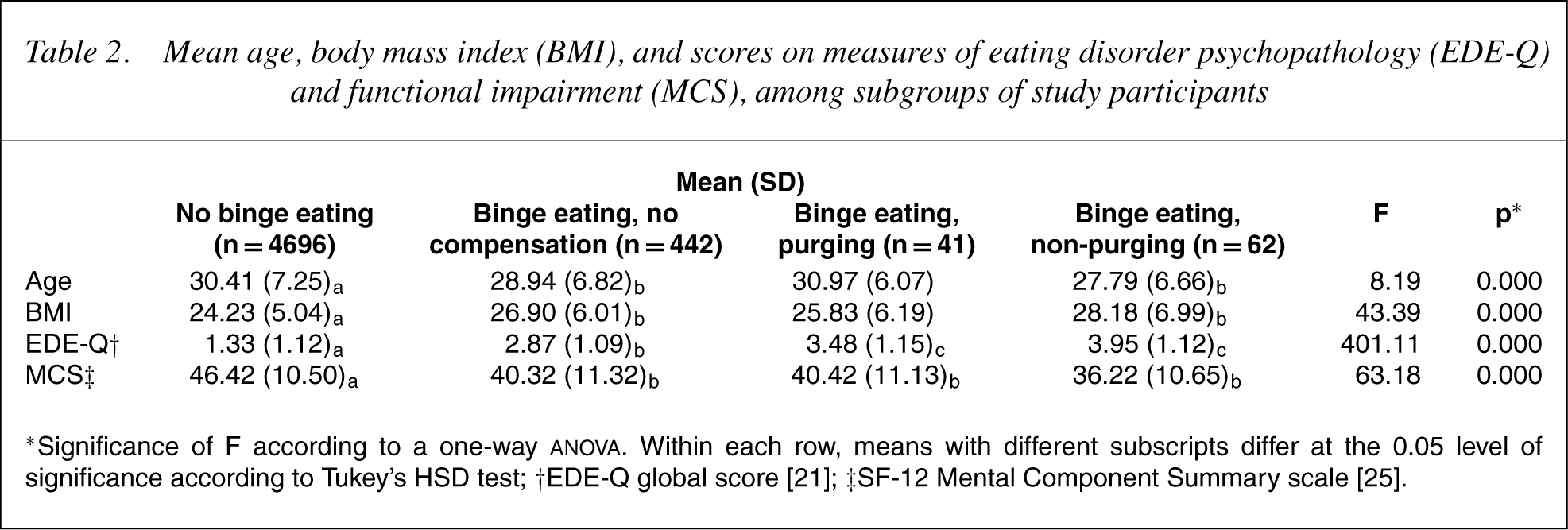
Table 2 shows mean age, BMI, and scores on the EDE-Q and MCS, among individuals in each subgroup. Non-purgers tended to be younger and heavier than purgers and non-compensating binge eaters, however these differences did not reach statistical significance. Scores on the EDE-Q were higher, and scores on the MCS lower (indicating greater impairment), among binge eaters than among non-binge eaters, as would be expected. Scores on the EDE-Q tended to be higher, and scores on the MCS tended to be lower, among non-purgers than among purgers and non-compensating binge eaters. However, only the difference between non-purgers and non-compensating binge eaters on the EDE-Q was statistically significant.
Mean age, body mass index (BMI), and scores on measures of eating disorder psychopathology (EDE-Q)and functional impairment (MCS), among subgroups of study participants
Whereas the proportion of participants who had ever sought treatment for an eating or weight problem was similar between purging (52.8%) and non-purging (46.3%) subgroups (χ2 1 = 0.36, p = 0.55), the proportion of purgers who had sought treatment specifically for a problem with eating was higher than that of non-purgers (30.0% vs 4.3%). This difference was significant according to a chi-squared test (χ2 1 = 5.17, p = 0.02), but was no longer significant after age and BMI were statistically controlled (adjusted OR = 0.43, CI = 0.03–5.95; p = 0.53). Approximately one-third (33.8%) of participants who reported binge eating in the absence of extreme weight control behaviours had ever sought treatment for an eating or weight problem, of whom 11.4% had sought treatment specifically for a problem with eating.
Results of the multiple regression analysis are shown in Table 3. Frequency of extreme dietary restriction and frequency of hard exercise forweight or shape reasons were the only eating disorder behaviours that significantly predicted functional impairment. Whereas higher levels of extreme dietary restriction were associated with higher levels of impairment, higher levels of hard exercise for weight or shape reasons were associated with lower levels of impairment.
Multiple regression analysis of eating disorder behaviours predictive of impairment in everyday functioning, as measured by the SF-12 Mental Component Summary scale (MCS)
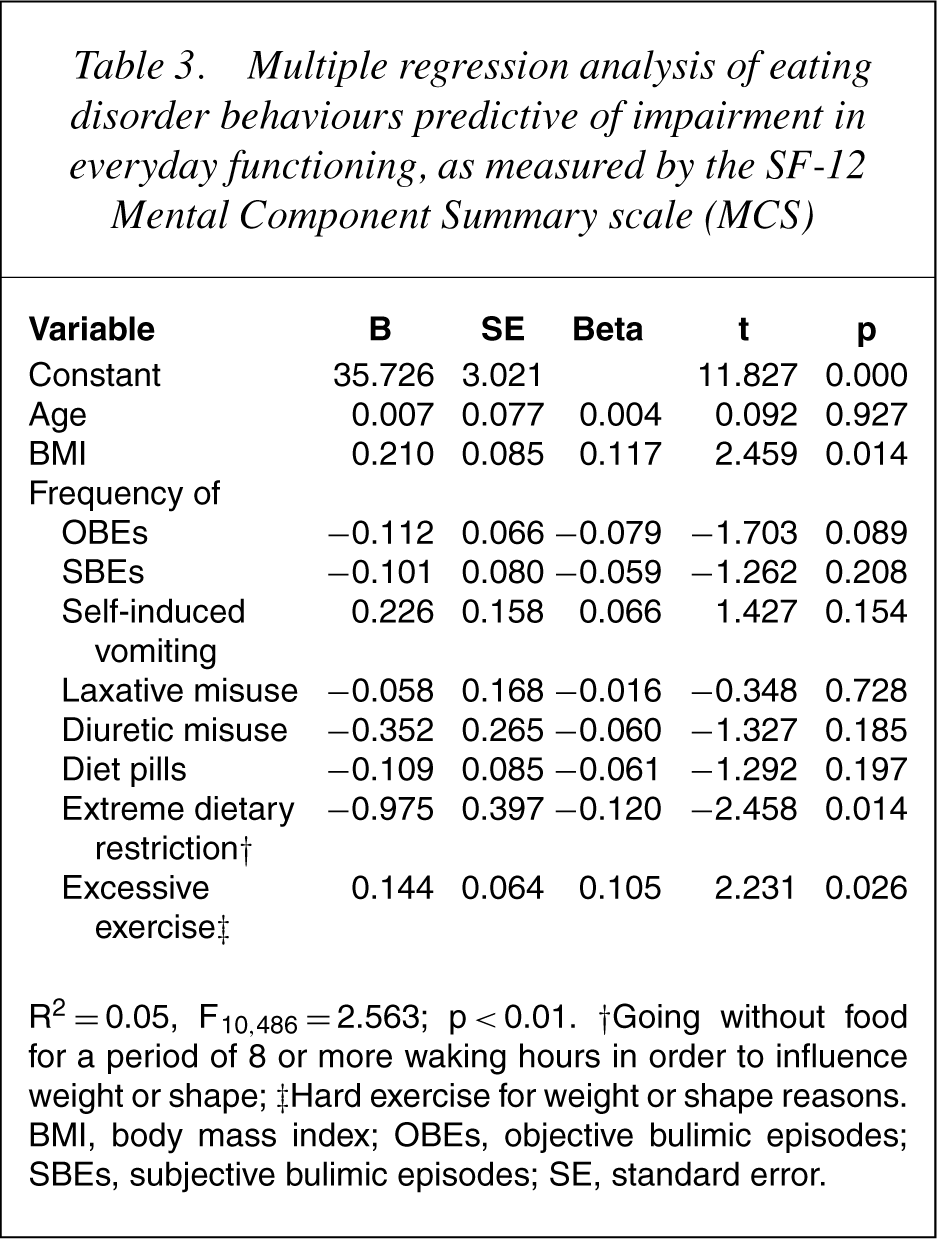
R2 = 0.05, F10, 486 = 2.563; p < 0.01. †Going without food for a period of 8 or more waking hours in order to influence weight or shape; ‡Hard exercise for weight or shape reasons. BMI, body mass index; OBEs, objective bulimic episodes; SBEs, subjective bulimic episodes; SE, standard error.
Discussion
We examined the correlates of purging and non-purging methods of weight control in a large community-based sample of young adult women who reported recurrent episodes of binge eating. Participants who engaged in binge eating in the absence of extreme weight control behaviours also were included in the analysis. Non-purgers tended to be younger and heavier and have higher levels of eating disorder psychopathology and functional impairment than purgers and non-compensating binge eaters, however these differences were not statistically significant. Inmultivariate analysis, frequency of extreme dietary restriction was the best predictor of functional impairment. Purgers were more likely than non-purgers to have sought treatment specifically for a problem with eating, however this difference was no longer statistically significant after between-group differences in age and BMI were controlled. These findings call into question the validity of subtyping of BN into purging and non-purging forms as outlined in DSM-IV.
A notable strength of the present study was the use of a large and representative community-based sample of women, thereby avoiding the biases inherent in clinical samples of individuals with BN-type eating disorders [16]. However, the findings cannot be considered a direct test of the validity of the DSM-IV classification of BN-type eating disorders, for several reasons. First, in defining recurrent binge eating, we used the Oxford criterion [22] in preference to the DSM-IV criterion of two or more episodes per week. This decision was made because no important differences have been identified between individuals who binge and purge once a week and those who do so two or more times per week [2]. Second, recurrent binge eaters were identified on the basis of selfreport assessment. Concordance between self-report and interview assessment of overeating behaviours has frequently been found to be poor and it is generally assumed that self-report assessment is inferior [23]. However, in pilot work we found acceptable agreement between self-report and interview assessment of recurrent binge eating [18].
Criteria for ‘extreme dietary restriction’ and ‘excessive exercise’ differed from those given in DSM-IV [1]. Recently, Cooper and Fairburn [30] have argued that the use of an overly stringent criterion for extreme dietary restriction, namely fasting, in DSM-IV has led to the virtual elimination of BNNP as a diagnostic category. The findings of Hay and Fairburn [12] and Striegel-Moore et al. [13] are consistent with this hypthothesis. Hence, the less stringent criterion of ‘going without food for a period of 8 or more waking hours in order to influence weight or shape’ daily, or almost daily, was used in the present study. The prevalence of 1.5% in the total sample for such behaviour suggests that this criterion was not overly liberal, but if such a view is taken, then the finding that ‘extreme dietary restriction’ was the best predictor of functional impairment among binge eaters is all the more striking.
Tobin et al. [10] also found that extreme dietary restriction was the best predictor of psychosocial impairment in a clinical sample of individuals with BN-type eating disorders. These authors suggested that the use of multiple compensatory behaviours may be a better predictor of psychiatric disturbance than the occurrence or frequency of any specific behaviour. Unfortunately, the number of participants reporting the use of both purging and non-purging methods of weight control in the present study was too small to address this hypothesis. Evidence from clinical samples supports the hypothesis that the use of multiple methods of purging, at least, is associated with high levels of psychiatric disturbance [31, 32].
It would be more difficult to argue that the definition of excessive exercise used in the present study, namely ‘hard exercise for weight or shape reasons at least daily’, was too liberal, though whether frequency of exercise is a useful component of the definition of ‘excessive exercise’ in eating disorders research is a matter of opinion. Research conducted by the authors in the same population suggested that exercise is excessive – that is, most strongly associated with elevated levels of eating disorder psychopathology and functional impairment – when it is undertaken solely to influence weight or shape and when its postponement is associated with intense guilt [33, 34]. These terms were not used in the present study because levels of eating disorder psychopathology and functional impairment among non-purgers may have been artificially inflated by the use of terms known to be highly correlated with these variables.
The fact that excessive exercise, as defined in the present study, was associated with lower levels of functional impairment in multivariate analysis may reflect ego-syntonic aspects of frequent hard exercise [35]. Previously [33] we noted that levels of exercise are higher in the ACT than in other regions of Australia. Hence, it would be of interest to replicate this finding in a different sample. It would also be helpful to replicate the present findings using a different measure of functional impairment. Whereas generic measures are useful from a from a public health perspective, a ‘disease-specific’ measure of impairment would likely be more sensitive to the effects on functioning of different subgroups of binge eaters [36]. Finally, it would be of interest to know the long-term outcome of the different subgroups, because data of this kind also are important in informing the classification of psychiatric disorders [12]. Unfortunately, the cost of prospective community-based studies of psychiatric disorders is typically prohibitive.
In view of qualifications concerning the assessment of binge eating noted previously, any conclusions concerning the comparative levels of impairment associated with BN and BED, as defined in DSM-IV, must be considered tentative. However, the findings do suggest that the regular occurrence of binge eating is associated with considerable impairment in functioning, irrespective of the occurrence of extreme weight control behaviours. Moreover, the number of individuals reporting recurrent binge eating in the absence of extreme weight control behaviours was approximately four times that of participants reporting binge eating and purging or non-purging behaviours. Hence, the present findings might be seen to add to the growing body of evidence supporting the prevalence and clinical significance of BED [7, 8].
The finding that non-purgers (and non-compensating binge eaters) tended to be heavier than purgers is consistent with findings from previous research [9, 11] and may reflect a tendency for overweight individuals to use nonpurging methods of weight control. The fact that purgers were more likely than non-purgers to have sought treatment specifically for a problem with eating also is consistent with previous research [13]. This finding may reflect, in part, the great prevalence of overweight in the non-purging subgroup, since the difference was no longer significant after age and BMI were statistically controlled. The tendency of purgers to be younger than non-purgers may reflect a tendency for the use of purging behaviours to decline with age [37].
In sum, we found no evidence to suggest that the use of purging behaviours is associated with higher levels of eating disorder psychopathology or functional impairment than that of non-purging method of weight control, in a large community-based sample of women reporting regular episodes of binge eating. Although not a strict test of the subtyping of BN as outlined in DSMIV, these findings call into question the validity of this scheme.
Footnotes
Acknowledgements
This research was supported by grants from the Private Practice Fund at The Canberra Hospital, the ACT Department of Health and Community Care, and ACT Mental Health Services. Thanks also to Ross Crosby PhD for his assistance with the statistical analysis.