
Abstract
Factor analysis of manic symptoms might be able to indicate dimensions of mania and help in the classification by identifying subgroups. Early factor analytic studies of manic symptoms were conducted more than three decades ago by Murphy and Beigel based on analysis of only 30 patients [1]. Their first factor had loading from the ‘core’ symptoms of mania. The second was bipolar with a large positive loading from items identified as ‘paranoid–destructive’ and a large negative loading from items identified as ‘elation–grandiose’, on the basis of which they proposed two manic subtypes: paranoid– destructive and euphoric–grandiose [1]. Attempts to con-firm the Beigel–Murphy typology of manic states have met with limited success [2,3]. In all these studies, the number of cases was below that usually recommended for the generation of stable factors (i.e. 10-fold the number of items in the scale used for the study) [4].
The generation of interpretable factors requires that appropriate variables be measured in the original observations. Comrey emphasized that variables should provide representative measures of each expected factor and that omitting key variables will seriously alter or obscure the complete factor solution [5]. In this regard, although the Manic State Rating Scale (MSRS) included depressed mood, it did not include many clinically suggestive factors of mixed mania such as lability and anxiety [6]. Double examined the factorial structure of the Young Mania Rating Scale (YMRS) and MSRS on 81 manic patients and found a solution of three factors for both the scales [3,7]. The factor structure of the YMRS identified a psychotic or thought disturbance factor, an overactive and aggressive factor and a hedonism factor, but the scale does not include depression at all. Cassidy et al. using the Scale for Manic States (SMS) developed by themselves overcame these shortcomings and identified five factors [8]. The first and the strongest factor represented dysphoria, with strong positive loadings for depressed mood, lability, guilt, anxiety, and suicidal thoughts and behaviours and a strong negative loading for euphoric mood. The other factors were psychomotor pressure, psychosis, increased hedonic functions and irritable aggression.
Serretti et al. conducted a factor analytic study in 509 bipolar patients using the Operational Criteria Checklist for Psychotic Illness that retrospectively measures psy-chopathology throughout lifespan [9]. They reported a three-factor solution consisting of psychomotor excitement, psychosis and irritability/motor agitation. Dilsaver et al. in a factor analysis of 37 items from the Schedule for Affective Disorders and Schizophrenia studied 105 manic patients and identified four factors corresponding to manic activation, depressed state, sleep disturbance, and irritability–paranoia [10].
Several authors found that atypical manic features could coexist (or be significantly correlated) in some patients with mania, particularly those experiencing a severely manic phase [11–13]. These studies, however, also provided evidence that depression was not always linked to aggression or psychosis in the longitudinal course of a manic episode [12,13]. In order to overcome this problem, some studies included both mania and depression rating scales in their factor analyses [14–16]. The details of the studies along with the principal components extracted have been summarized in Table 1 [1,3,8–10,14–20].
Factor analytic studies of manic symptoms
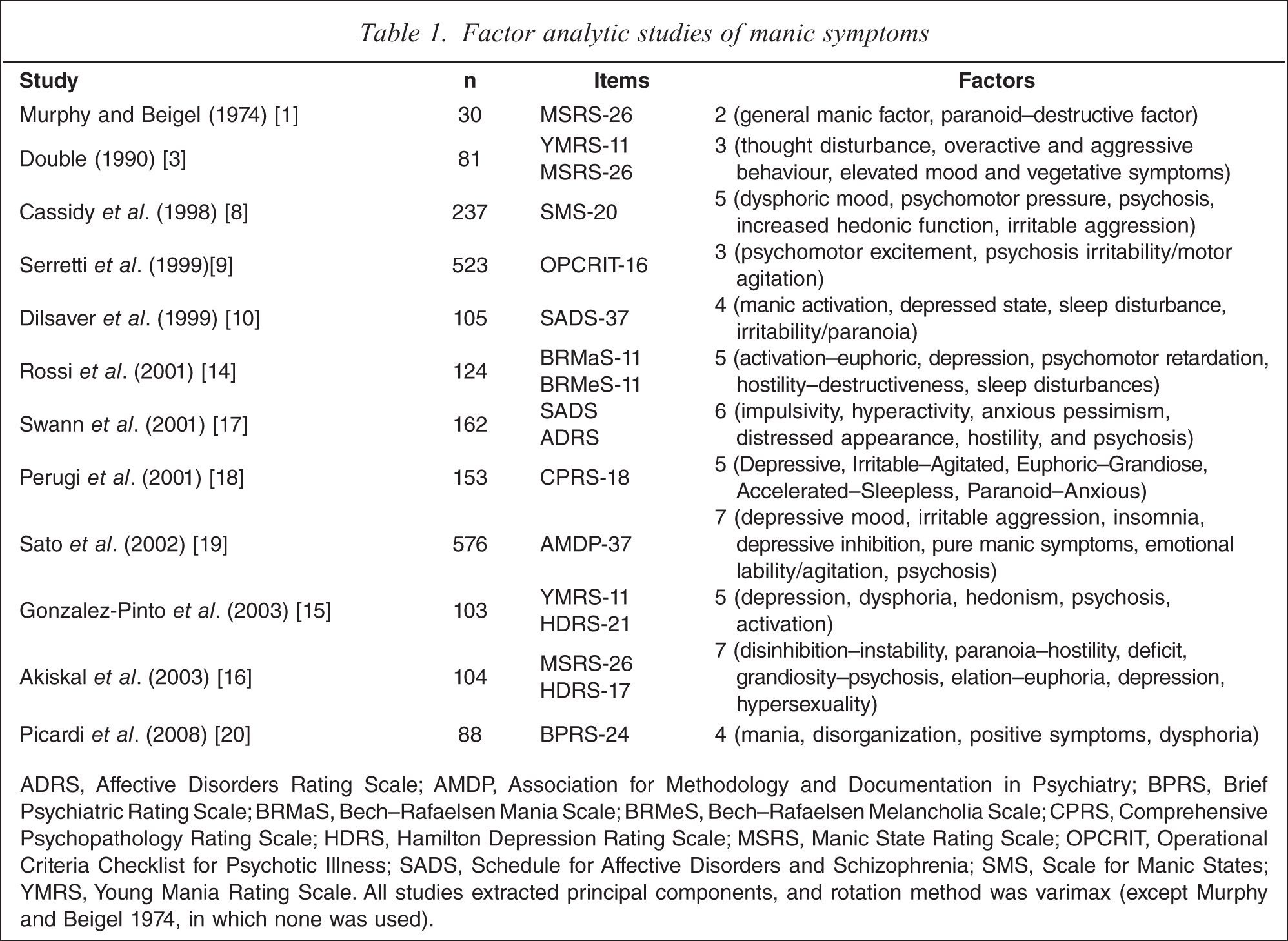
ADRS, Affective Disorders Rating Scale; AMDP, Association for Methodology and Documentation in Psychiatry; BPRS, Brief Psychiatric Rating Scale; BRMaS, Bech-Rafaelsen Mania Scale; BRMeS, Bech-Rafaelsen Melancholia Scale; CPRS, Comprehensive Psychopathology Rating Scale; HDRS, Hamilton Depression Rating Scale; MSRS, Manic State Rating Scale; OPCRIT, Operational Criteria Checklist for Psychotic Illness; SADS, Schedule for Affective Disorders and Schizophrenia; SMS, Scale for Manic States; YMRS, Young Mania Rating Scale. All studies extracted principal components, and rotation method was varimax (except Murphy and Beigel 1974, in which none was used).
Dysphoric features coexisting with the four classic defining features of mania, that is, euphoric mood, psychomotor pressure, grandiosity and irritable aggression have been observed by various researchers [11,12]. Carlson and Goodwin noted that dysphoric features persisted throughout the evolution of manic episodes, and increased as the mania became more severe [12]. McElroy et al. found dysphoric mania to be a distinct affective state as compared to non-dysphoric mania [21]. With a relative dearth of factor analytic studies in mania in this region with an adequate sample size usually recommended for the generation of stable factors, we conducted a study using the SMS [8] that captures the depressive symptoms along with manic symptoms. The aim was to explore the underlying factors of manic symptoms and whether dysphoric features were present in the sample.
Method
The present study was conducted at Central Institute of Psychiatry (CIP), Ranchi, a psychiatry tertiary referral centre in India. The study sample consisted of 225 adult patients (>19 years) who fulfilled the ICD-10-DCR criteria for manic episode [22]. Patients were excluded if they had received a diagnosis of mixed affective episode, in order to ensure homogeneity of the sample. This was done because the conceptualization of mixed mania is still inconsistent due to variations in definitions regarding the required temporal relationship between manic and depressive symptoms [21]. Patients were included in the study after informed consent to participate in the study was obtained.
Assessment
Comprehensive Assessment of Symptoms and History [23] was used to interview the study sample, and this had three main sections: present state, past history of psychotic or affective illness, and lifetime history. The SMS [8] was used to measure the severity of mania. It is a 20-item scale with good interrater and test-retest reliability [8]. Additional information from the clinical records and staff observations were incorporated into the ratings.
Factor analysis
The data were analysed using SPSS version 10.0 (SPSS Inc., Chicago, IL, USA). Kaiser-Meyer-Olkin measure of sampling adequacy was >0.6 [24] and Barlett's test of sphericity was significant. Exploratory factor analysis (principal component analysis) was performed to determine factors within the sample. The item ‘guilt’ was excluded from factor analysis because all except one (rating of 1) of the adult sample gave a rating of ‘0’ on this item. Three criteria for retaining the number of components were considered: Kaiser's criterion to retain eigenvalues >1 [24], Cattell's scree-plot inspection for the point of inflexion [25], and Horn's parallel analysis [26]. Parallel analysis was performed with criterion values replicating a randomly generated data set obtained using the regression equations developed by Keeling [27]. Only factor loadings with absolute value >04 were interpreted [28]. Orthogonal rotation (varimax rotation with Kaiser normalization) was initially done that indicated dual loading >04 on more than one factor. Oblique rotation (oblimin rotation with Kaiser normalization, delta at zero) was done that indicated a more interpretable solution. The pattern matrix was interpreted as having no complex variables and a simpler structure.
Results
Demographic factors
The mean (±SD) age of the sample was 30.96 ±9.10 years. The 225 patients consisted of 153 men (68%%) and 72 women (32%%). Mean total Scale for Manic States score (SMS score) was 36.68 ± 6.87. There was a family history of affective illness in 60 patients, non-affective psychosis in 22 and substance dependence in 14 patients. Fifty-four patients (24%%) were in their first manic episode. In the remaining 171 patients, the mean number of manic and depressive episodes was 2.71 ± 2.60 and 0.40 ± 1.00, respectively.
Principal component analysis
Principal component analysis resulted in initial six factors with eigenvalues >1 [24]. The six factors captured 59.29%% of the variance. Parallel analysis using Keeling's regression equation [27] showed that only the first four eigenvalues exceeded the criterion values for a randomly generated data matrix of the same size (255 patients × 19 items). The four factors accounted for 47.16%% of the variance. Furthermore, observing the scree plot (Figure 1), a five-factor solution seemed to be the most appropriate that accounted for 53.59%% of the total variance. Nevertheless, a six-factor solution appeared clinically most appropriate for the present data. Table 2 shows the rotated (oblimin) component matrix for a six-factor solution with factor loadings >0.4 [28] highlighted.
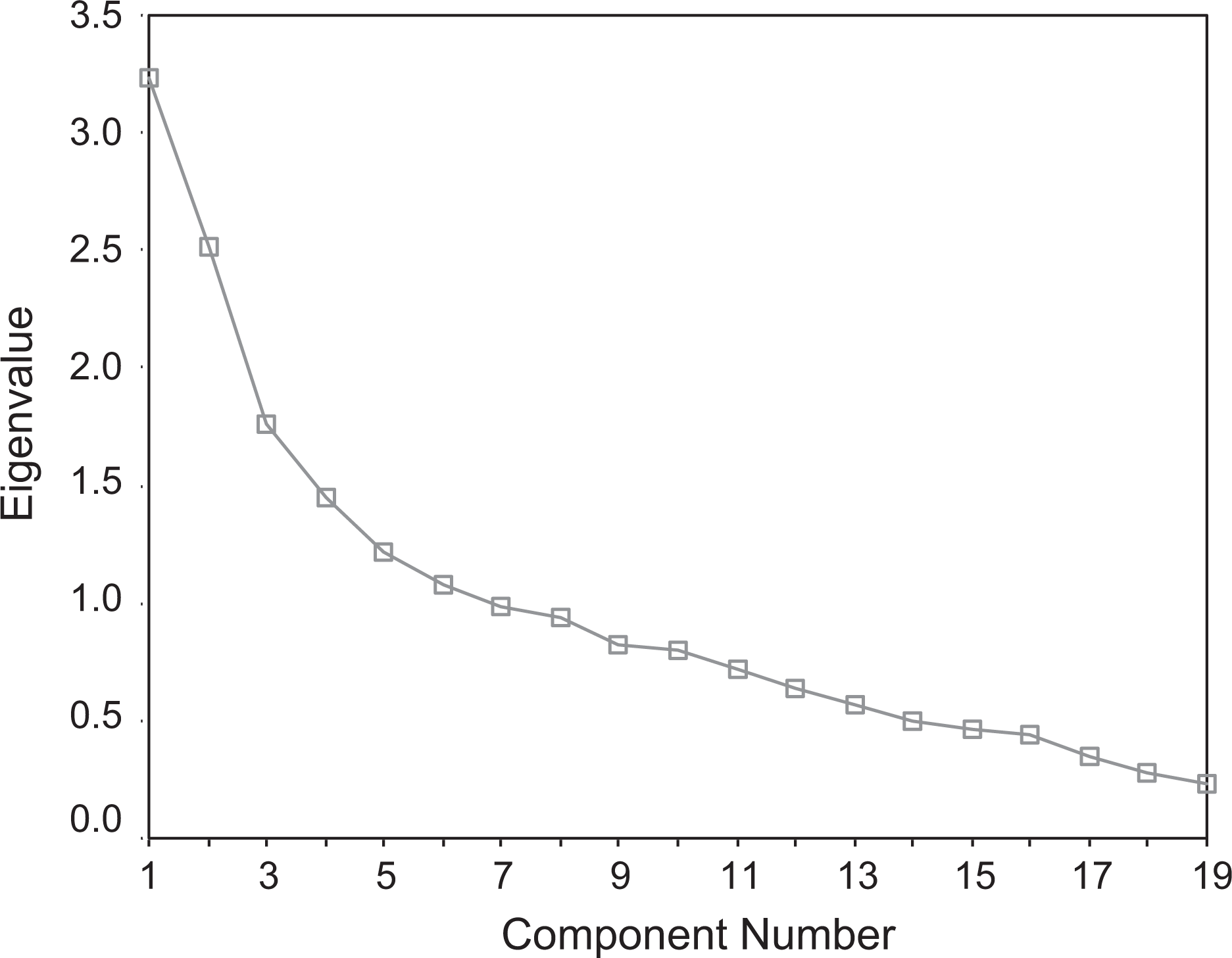
Scree plot of extracted components.
Factor structure of Scale for Manic States
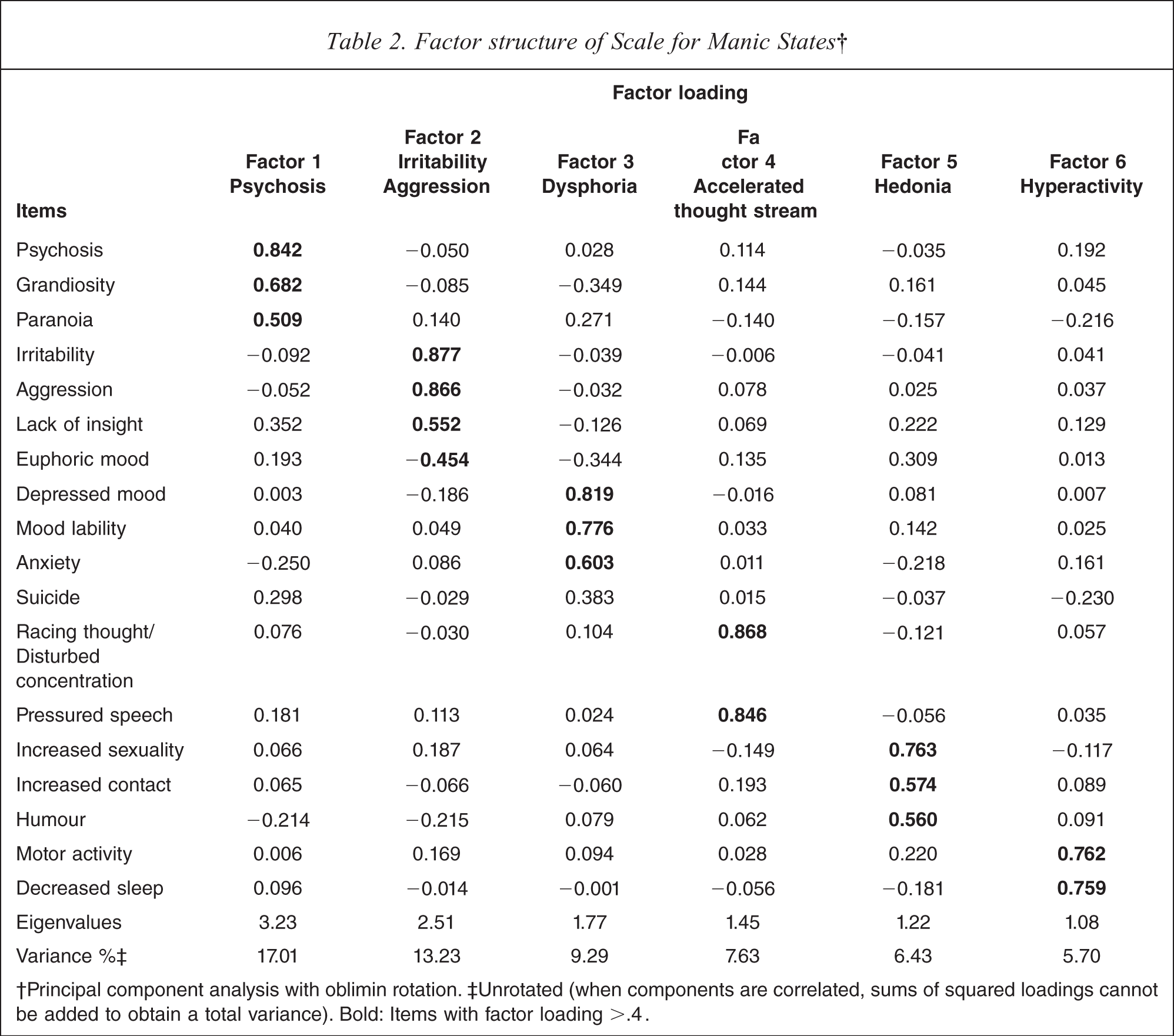
†Principal component analysis with oblimin rotation. ‡ Unrotated (when components are correlated, sums of squared loadings cannot be added to obtain a total variance). Bold: Items with factor loading >.4.
Factor 1 was the strongest and had highest positive loadings from psychosis, grandiosity and paranoia and represents ‘psychosis’. Factor 2 included irritability, aggression and lack of insight, which seemingly represented ‘irritability aggression’. Factor 3 included depressed mood, mood lability and anxiety, and appeared to represent ‘dysphoria’. Factor 4 included racing thoughts/disturbed concentration and pressured speech, which seemed to represent ‘accelerated thought stream’. Factor 5 consisted of increased sexuality, increased contact and humour, and appeared to represent ‘hedonia’. Factor 6 consisted of motor activity and decreased sleep and appears to represent ‘hyperactivity’. Figure 2 shows the distribution of factor scores; all except irritability aggression had a non-normal distribution (Kolmogorov–Smirnov test).
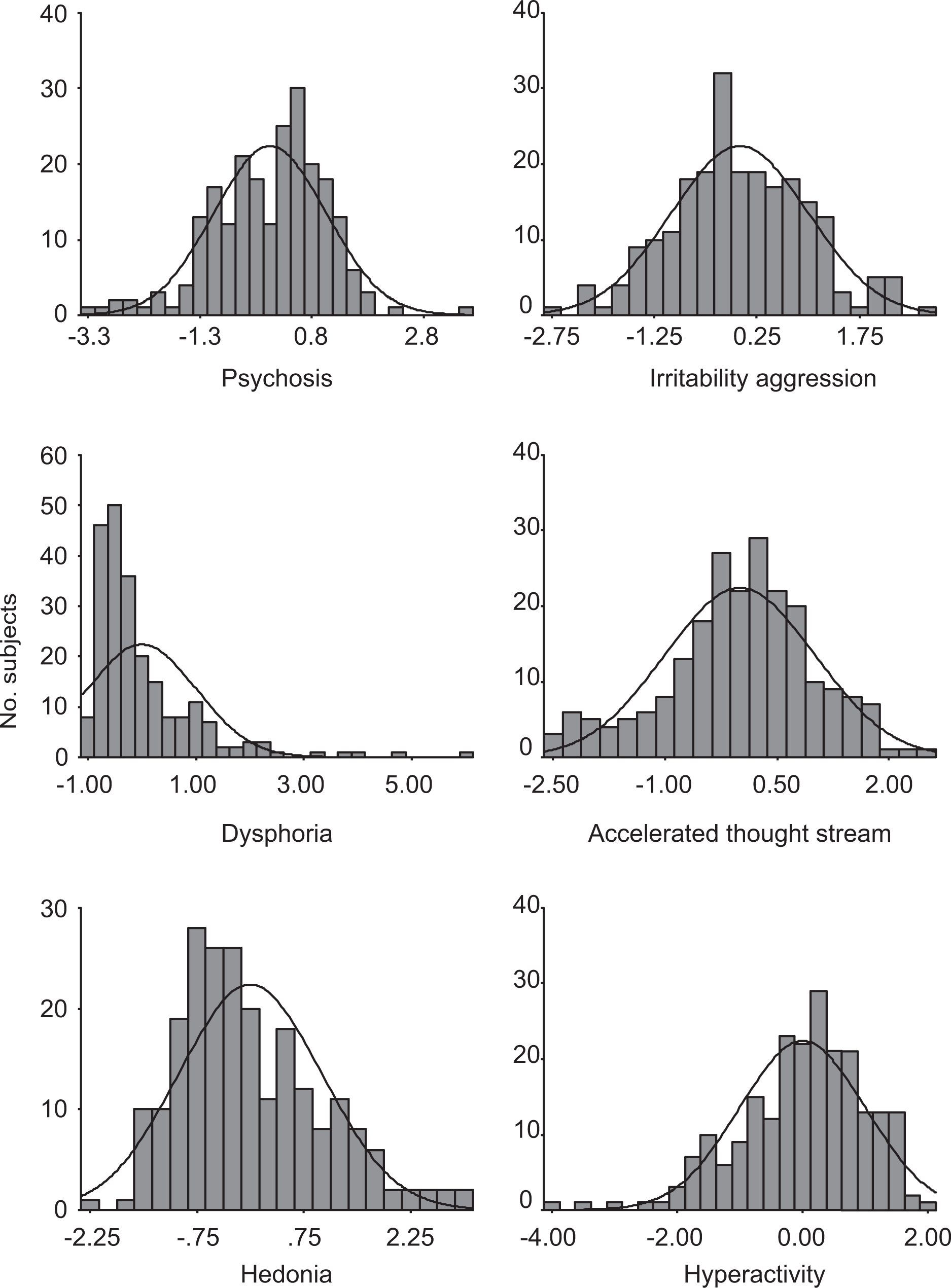
Distribution of factor scores.
Discussion
The principal component analysis of manic symptoms using Scale for Manic Symptoms indicated four–six factors depending on the method of retaining factors used. Although it has been demonstrated that both Kaiser's criterion and Catell's scree test tend to overestimate the number of components and parallel analysis has been recommended will be more appropriate the number of factors [29], in the present study six factors appear to be clinically most relevant and describe various aspects of manic syndrome consistent with the literature. The rotated factors accounted for a high proportion of the variance (59.29%%) and had a simple structure.
The first factor represented psychosis, with highest loadings from psychosis, fograndiosity and paranoia. This factor was similar to the third factor of the Cassidy et al. study that used SMS [8]. Lack of insight had a loading >0.3 in the present study, whereas it had a higher loading in the Cassidy et al. study [8]. This is similar to the fourth factor of Dilsaver et al. who, along with delusions and suspicious-ness, also found irritability in this factor [10]. It is also analogous to factor 1 of Double [3], which contained items of insight, language thought disorder and content of Young's mania scale. This factor does not have a clear counterpart in the analysis of Murphy and Beigel [1] and Rossi et al. [14], which might be because they used a mania scale that did not have defined items for psychosis. The present sample, which were referrals to a tertiary hospital and included severe cases of mania, might account for the emergence of psychosis as the first factor. The emergence of psychosis as an independent factor suggests that they are separate from the core manic features and lends support to the classification of mania with and without psychotic symptoms. Kendler et al. found a class of schizomania in their latent class analysis of psychosis [30].
The second factor represented irritability aggression, similar to factor 5 of Cassidy et al. in which irritability and aggression had loaded on a factor separate from psy-chomotor acceleration [8]. This is also similar to factor 2 of Gonzalez-Pinto et al. [15] and factor 4 of Dilsaver et al. [10]. Negative loading from euphoric mood in this factor confirms that irritability–aggression and euphoria are antithetical dimensions in mania [3]. Mood can also be viewed as a continuum, with poles of aggression and irritability on one end, and euphoria on the other. It also supports the existence of two separate subtypes of mania: ‘euphoric’ and ‘irritable’.
Factor 3 represented a dysphoric mood factor that has loading from depressed mood, mood lability and anxiety. It is similar to the first factor of Cassidy et al. that included further items such as suicidal thoughts and guilt in the dysphoric pole [8]. In the present study suicide had a loading >0.3, consistent with the study by Cassidy et al. [8]. Signs and symptoms such as lability and anxiety have been hypothesized to characterize dys-phoric mania [13]. Because patients with a clinical diagnosis of mixed episode were excluded from the study, this finding suggests that dysphoria features even in pure manic episodes. A similar result was reported by Cassidy et al. [8], Rossi et al. [14], Gonzalez-Pinto et al. [15] and Picardi et al. [20], whereas this factor was not evident in other studies such as that by Murphy and Beigel, and Double [3], which did not include depressive symptoms in the scales [1,3]. Inclusion of dysphoric features in the clinical diagnosis of mania merits further consideration.
Factor 4 was accelerated thought stream. In contrast to the previous factor analytic studies in which a single factor of ‘psychomotor acceleration’ was found, in the present study motor and psychic acceleration have been delineated on two different factors, that is, factors 1 and 4, respectively. Similar findings were seen in the study by Double, who had delineated psychic acceleration in cluster 1 and motor hyperactivity in cluster 4 [3].
Factor 5 represented hedonia, identical to that of factor 4 of Cassidy et al. [8], although grandiosity and euphoric mood did not appear to be related to this factor in the present study. This factor is reminiscent of the euphoric– grandiose symptom cluster observed by Beigel and Murphy [1] and the third factor of Double [3]. As suggested by Cassidy et al. [8], humour and hypersexuality can be conceptualized as alternative expressions of elevated mood and self-esteem.
Factor 6 represented hyperactivity with high loadings from motor activity and decreased sleep. Bauer et al. found that the ‘activation’ subscale represented an essential feature of mania [31]. The study by Zheng and Lin also demonstrated that changes in the dimension of activity contributed substantially in assessing the severity of mania as well as depression [32]. Increased motor/psychomotor activity as a cardinal symptom of mania has been emphasized by various earlier researchers [12,33]. Although changes in mood are the hallmark of mania in the current nosological criteria, they are little supported by factor analytic studies. The relative weight of activity level as opposed to mood in diagnosis of mania may need reconsideration. Previous studies have found a factor of combined psychic and motor hyper-activity, that is, ‘psychomotor acceleration’ [8,34], but in the present study psychic acceleration and motor acceleration have been delineated on two different factors (i.e. factors 4 and 6 respectively). Swann et al. reported a cluster of irritable mania without hyperactivity [17]. The separation of these two components also provides evidence towards different subtypes of mania in which there is a dissociation of psychic and motor activity.
Conclusion
The four classic defining features of mania appeared as factor 2 (irritable aggression), factor 4 (accelerated thought stream), factor 5 (hedonia) and factor 6 (hyperactivity) in the present study, which suggests the importance of these defining features. Dysphoria appeared as a separate factor in the present sample, which is consistent with recent studies. This again substantiates the observation that non-inclusion of depressive symptoms in previous studies might have led to exclusion of this factor. The present data support the view that euphoric and irritable mania are two different subtypes. The factors generated in the present study describe useful research and clinical dimensions for the study of mania. In addition to mood they capture psychosis, hedonia, and psychic and motor acceleration. These factors allow the characterization of individual patients on these dimensions, which may extend the ability to study the relationship of features of mania to biological markers, prognosis, and treatment response.