
Abstract
Introduction
There is little doubt about the presence of an association between schizophrenia and homicide (Fazel et al., 2009; Large et al., 2009c), whereas opinion is divided about the association between bipolar affective disorder and homicide. Some authors believe that there is an association between mania and serious violence, including homicide (Bassett, 2010; Edwards, 1992), while others suggest that any association is weak or coincidental (Benezech and Bourgeois, 1992).
Examining the relationship between violence and mania is difficult because of the dimensional nature of aggression and because mania is episodic and variable (Malhi et al., 2010). Birth cohort, case linkage and cross-sectional population studies have shown some association between the diagnosis of bipolar disorder and violence. A Danish birth cohort study found that men with a diagnosis of bipolar disorder were twice as likely, and women with bipolar disorder four times as likely, to be convicted of a violent offence as members of the general community (Brennan et al., 2000). A case linkage study from Victoria found that a diagnosis of affective psychosis was associated with three times more convictions for violent offences by men (Wallace et al., 1998). An Israeli study found a significant association between bipolar disorder and self reports of violence (Stueve and Link, 1997), a finding similar to that of the National Epidemiological Survey conducted in the USA (Pulay et al., 2008). A recent study from Sweden found that people diagnosed with bipolar disorder were more likely to commit a violent offence in the 29 years after diagnosis than members of the general community, but this association could mainly be attributed to co-morbid substance use and environmental factors, rather than the diagnosis of bipolar disorder itself (Fazel et al., 2010a, 2010b). None of these studies directly examined whether violence occurred during the manic, depressed or euthymic phases of bipolar disorder. The Dunedin birth cohort study was more specific in reporting a significant association between ‘manic disorder’ and violent behavior (Arseneault et al., 2000) but, like other studies, it did not consider the mental state of the subjects at the time of the reported violence.
Several clinical studies of first-episode psychosis patients have found an association between the presence of manic symptoms and violence. The 10-country study reported that manic excitement was associated with assault in early schizophrenia (Volavka et al., 1997) and later studies of early psychosis have also found an association between elevated mood, and both aggression and actual violence (Dean et al., 2007; Foley et al., 2005; Harris et al., 2010; Milton et al., 2001). A recent meta-analysis of the factors associated with violence in first-episode psychosis found that although manic symptoms were significantly associated with minor violence, mania was not strongly associated with physical assault (Large and Nielssen, 2011). Mania appears to be associated with verbal aggression among hospitalized patients, but is not strongly associated with inpatient violence (Amore et al., 2008; Biancosino et al., 2009; Nielssen et al., 1997; Raja and Azzoni, 2005). There is conflicting evidence about mania and violence after discharge from hospital. The Macarthur study found that in the 20 weeks after discharge from hospital, patients with mania were more likely to commit an assault than patients with schizophrenia, but were less likely to commit an assault than patients with depression or no mental disorder other than substance use (Monahan, 2001). Another large study of violence committed by discharged patients found those with a diagnosis of mania or bipolar disorder had higher rates of violence after discharge than patients diagnosed with depression (Graz et al., 2009).
There are very few reports of manic states among homicide offenders, and the extent to which mania is a risk factor for homicide is unknown. A 25-year national study of 1087 homicides in Austria reported a single offender with mania at the time of the offence (Schanda et al., 2004), and one offender with mania was also reported in an 18-year study of 313 homicides in Barbados (Evans and Malesu, 2001). In a study conducted over 30 years in New Zealand, five of 1498 homicides were committed by people diagnosed with bipolar disorder (Simpson et al., 2004), and a study from Iceland over a period of 79 years reported two of 47 homicide offenders with bipolar disorder (Petursson and Gudjonsson, 1981). Neither of the studies from Iceland or New Zealand employed methods that could identify whether the offenders were manic, depressed or euthymic at the time of the homicides. Several well-conducted studies have reported larger numbers of homicide offenders with bipolar disorder, and a modest association between the diagnosis of bipolar disorder and homicide, but these studies have the same limitation of not considering the mental state at the time of the offence (Fazel and Grann, 2004; Hafner and Boker, 1982; Shaw et al., 1999). Other epidemiological studies of homicide by the mentally ill have found no cases of mania or bipolar disorder (Gottlieb et al., 1987; Koh et al., 2006; Kua et al., 1984; Wilcox, 1985). Hence, the literature provides some evidence of an association between mania and less serious forms of violence, but little direct evidence of an association between mania and severe forms of violence such as homicide and attempted homicide.
Based on the results of a previous study of homicide and psychosis (Nielssen et al., 2007) and a related study of a complete series of people convicted of severe non-lethal violence (Yee et al., 2010), we formed the hypothesis that there was little if any association between mania and severe forms of violence. Hence we expected to find few homicide offenders with mania among a complete sample of people who were considered to have committed severe violent offences because of mental illness. To examine this hypothesis we conducted a retrospective observational study of a complete sample of people found not guilty by reason of mental illness (NGMI) of serious violent offences in NSW.
Methods
Sample
The District and Supreme Courts of NSW deal with severe violent offences, including murder, attempted murder, wounding or an assault resulting in serious injury. Less serious offences are dealt with in the Local Courts. In NSW, the common law defence of mental illness is based on the ‘McNaughten rules’ (McNaughten, 1843). However, the test for NGMI has been extended to include defendants who are ‘unable to reason with sense and composure’ about the wrongfulness of their actions as a result of mental illness (Porter, 1933), which has been interpreted to include the effect of manic states. Although the defence of mental illness in NSW is based on the same common law test as in the United Kingdom, as a result of the different interpretation of the McNaughten rules after Porter, the per capita rate of NGMI verdicts in NSW is about 20 times greater than in England and Wales (Large et al., 2008).
The NSW Mental Health Review Tribunal (MHRT) holds detailed records of all people found NGMI in NSW. We examined the files of all those found NGMI of murder, attempted murder, wounding or an assault resulting in serious injury in NSW during the 17 years between 1992 and 2008. Hence, this sample was defined by the presence of a mental illness that was severe enough to warrant a verdict of NGMI and violent offences that were serious enough for the accused to be committed to trial to the District or Supreme Courts of NSW. The sample and methods of the study are described in detail in a related paper (Nielssen et al., 2011). Data were extracted from the statements of police and other witnesses, written judgments and psychiatric reports tendered in court, using methods described in earlier studies of homicide in NSW (Nielssen et al., 2007, 2009a, 2009b).
Diagnostic reliability
The study relied on the psychiatric diagnoses made by experienced expert witnesses, who use the diagnostic criteria of the Diagnostic and Statistical Manual (American Psychiatric Association, 2000) or the International Classification of Diseases (World Health Organisation, 1990). For the purpose of this study, we defined mania in three ways: (a) the manic phase of bipolar disorder; (b) the hypomanic phase of bipolar disorder; and (c) the manic syndrome in association with schizo-affective disorder. Clinical diagnoses, rather than a diagnosis generated using a structured diagnostic interview, are generally used in homicide research (Bennett et al., 2011; Meehan et al., 2006) because of legal and practical issues in conducting research in prison settings and because of doubts about the validity of structured interviews performed on people with psychotic illness, especially in prison settings (Nielssen and Misrachi, 2005). However, the psychiatric diagnoses, including the diagnosis of mania, made by psychiatrists acting as expert witnesses in criminal proceedings in NSW have been shown to be highly reliable (Nielssen et al., 2010b) and to be consistent with the diagnoses made by treating doctors (Large et al., 2010a).
Data extraction and reliability
The following information was collected:
Socio-demographic data, including age at time of the offence, sex, marital status, number of years of education and employment history.
Clinical data, including whether there was a family history of mental illness, any history of head injury, any history of childhood trauma or neglect, self-harm or suicide attempt, substance use history, psychiatric diagnoses, past contact with mental health services, past admission to hospital, duration of symptoms of psychosis, including the duration of untreated psychosis in first-episode patients, treatment adherence, the presence and nature of any delusional beliefs, and the presence of auditory hallucinations or disorganized thinking.
Criminological data, including any history of conduct disorder, past convictions, relationship to the victim, use of a weapon, and intoxication at the time of the offence.
The data were independently extracted from the relevant documents by OBN and MML, with no disagreements about the presence of a diagnosis of mania.
Ethical approval
Approval to conduct the study was obtained from the Human Research and Ethics Committee of St Vincent’s Hospital.
Results
Twelve (4.4%) of 272 offenders found to be NGMI of violent offences were reported to have been manic (Table 1) . Two were in the manic phase of bipolar disorder, and the remaining 10 were in the manic phase of schizo-affective disorder. There were no cases with the diagnosis of hypomania. A further 86 people were described as being depressed at the time of the offence, none of whom were in the depressed phase of bipolar disorder and three of whom were given the diagnosis of schizo-affective disorder. Most of the remaining offenders, described in more detail in a related publication (Nielssen et al., 2011), were diagnosed with a schizophrenia-spectrum psychosis (234, 86%).
Characteristics of 12 patients found NGMI of violent offences who were described as manic at the time of the offence.
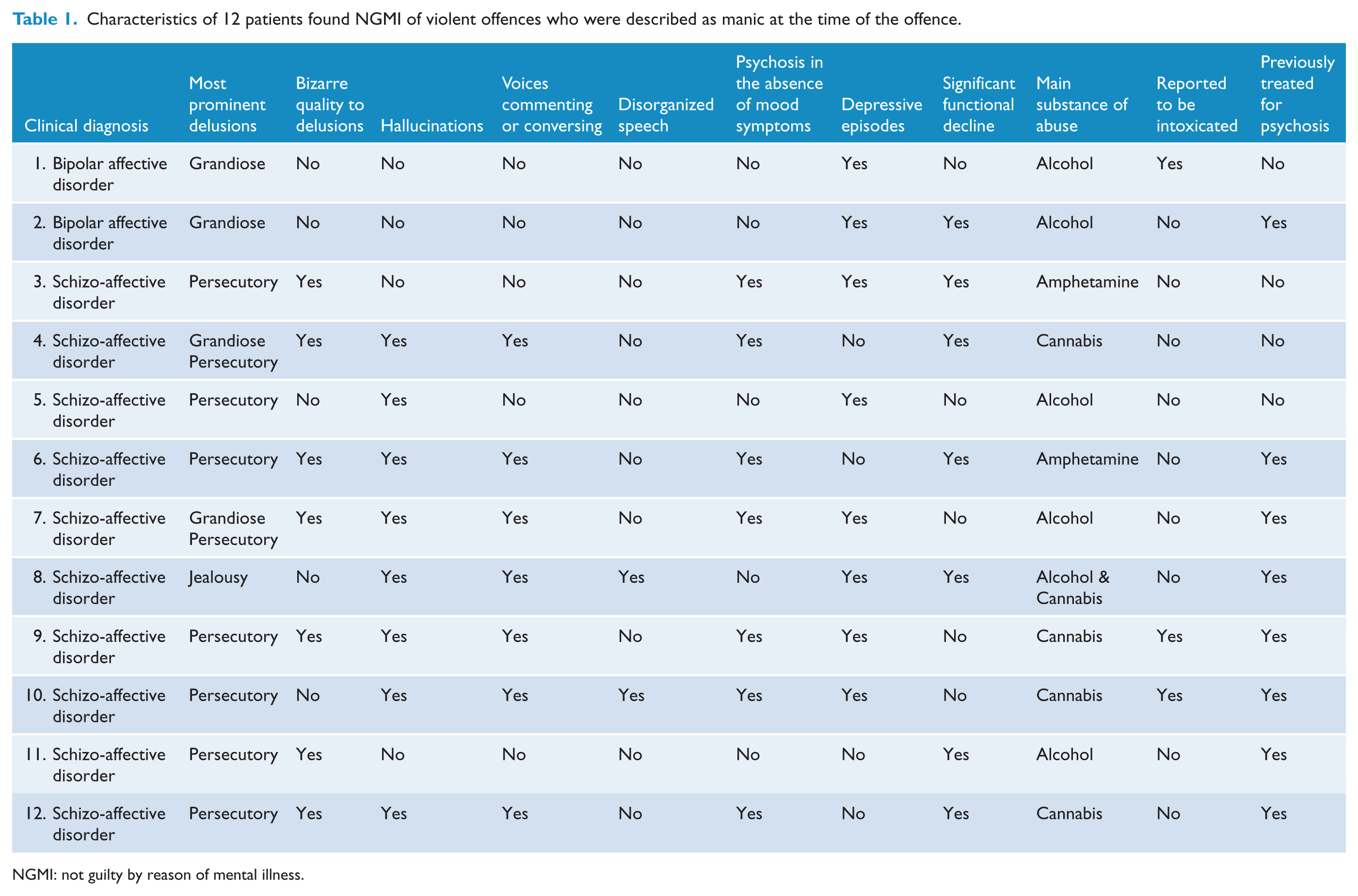
NGMI: not guilty by reason of mental illness.
Demographic data
There were 10 males and two females, with a median age of 32 (range 20–77). They had an average of 11 years of education and all but one had previously been employed. Three were born overseas and two were from non-English speaking countries.
Criminological variables
Seven (5%) of 138 homicides and five (4%) of 134 assaults resulting in serious injury were committed during an episode of mania. One of the homicide offences occurred in the course of a motor vehicle accident, for which the accused was found NGMI because of the effect of severe manic symptoms. Four had a prior criminal conviction, but none had been sentenced to a term of imprisonment. Six of the victims were strangers, including the driver of the other car and a fellow patient psychiatric in a psychiatric hospital.
Clinical features
The 12 offenders with mania all had grandiose delusional beliefs, including three who believed they were Jesus or some kind of messiah. The other patients believed they had special powers or responsibilities. In the two cases in which the victims were children, the subjects had grandiose religious beliefs, including one patient who believed he could raise the child from the dead and another who believed she was exorcising a demon. In four cases, grandiose delusions were either prominent or were the only delusional beliefs, whereas the remaining patients also had persecutory or other kinds of delusional beliefs. Four of the 12 had never received treatment for psychotic illness and were in their first episode of psychosis. Three of those had illnesses of relatively acute onset, with durations of untreated psychosis of 3, 4 and 12 weeks respectively, and one was reported to have had psychotic symptoms for a year prior to the offence. None of the previously treated patients were adherent to psychotropic medication at the time of the offences. Each of the 12 had a history of some form of substance abuse and two were reported to be intoxicated with alcohol at the time of the offence.
Ten of the 12 were diagnosed with schizo-affective disorder by the assessing clinicians. Nine of the patients diagnosed with schizo-affective disorder had either delusional beliefs that were bizarre in nature or reported hallucinations of voices conversing or directing their actions; seven were reported to have experienced psychotic symptoms while euthymic; and six had a marked decline in social or occupational performance, suggesting that the schizophrenic dimension of their schizo-affective disorder was prominent (see Table 1).
Discussion
The main finding of this study was that 12 of 272 people found NGMI of a severe violent offence were in a manic state at the time of the offence, including seven of 138 people found NGMI of homicide. One person was in the manic phase of bipolar disorder at the time of a homicide. During the period of the study, 1729 people were charged with a homicide offence in NSW. Hence, the main finding of this study is consistent with earlier studies that reported very few people in manic states who had committed homicide offences.
This study has a number of limitations. The sample was defined by legal verdicts, and it is possible that people in manic states were less likely to reach the threshold for an NGMI verdict than people with other psychotic disorders because of the absence of the type of bizarre delusional beliefs that might increase the likelihood of agreement about the availability of the defence of mental illness (Large et al., 2009b). In earlier studies of NGMI verdicts, the proportion of patients with a diagnosis of bipolar disorder has ranged from 4% in Michigan (Packer, 1985), 12% in Illinois (Wettstein and Mulvey, 1988) to 16% in Missouri (Linhorst, 1997), which suggests that thresholds for the defence of mental illness might influence the proportion of offenders with bipolar disorder who are found NGMI. None of these studies reported whether the patients were in the manic phase of bipolar disorder at the time of the offence, nor was it clear how many of the offences by people with bipolar disorder involved violence. The diagnoses made by court experts could be less reliable than the health service diagnoses used in cohort and case register studies. It is also possible that undiagnosed mania or hypomania was present at the time of other offences but had resolved by the time the person was examined by a psychiatrist and was never raised in court.
The findings of this study are supported by the results of three related studies of mental illness and serious offences in NSW. In an earlier study of homicide and psychotic illness we located two cases of people with the diagnosis of bipolar disorder who were charged with murder but were found guilty of manslaughter on the grounds of substantial impairment by abnormality of mind (Nielssen et al., 2007). Both had previously been treated for episodes of mania but were depressed at the time of their offences. Hence, we have been able to identify as few as three homicide offenders with bipolar disorder, one of whom was manic at the time of the offence, out of a total of 1729 people charged with homicide offences. In a second study of a consecutive series of 110 cases in which pairs of psychiatric reports were prepared in criminal proceedings in higher courts, we found that two of 110 cases involved a person diagnosed with mania. This study included defendants who were found guilty, not guilty and not guilty by reason of mental illness of a range of violent and non-violent offences (Nielssen et al., 2010b). In a third study of 661 consecutive cases of serious non-lethal violent offences dealt with in the District Court, we found another two people who were reported to be manic at the time of their offences (Yee et al., 2010). The findings of these studies suggest that mania is rare among samples of people charged with serious offences in NSW, especially serious violent offences.
The small proportion of manic patients among the perpetrators of serious violent offences is also consistent with studies of severe self-inflicted violence. Bipolar disorder is an unusual diagnosis among the case reports of patients who self-enucleate or amputate their own limbs or genitals, who almost all have a schizophrenia-related psychosis (Large et al., 2009a, 2010b). Similarly, we found few patients with a diagnosis of bipolar disorder among the survivors of suicide attempts by jumping from a height (Nielssen et al., 2010a) or potentially lethal self-stabbing (Nielssen and Large, 2009). Hence, we conclude that there is little evidence for an association between mania and severe violence to one’s self or to others.
The reason for the association between manic states and minor forms of aggression found in a number of studies, especially those conducted in hospital wards, might be the increased intrusiveness and decreased frustration tolerance observed in people who are manic. However, more serious forms of violence by the mentally ill are usually associated with frightening or distressing delusional beliefs, which are more typical of a schizophrenia-related psychosis than mania, and include the beliefs that the victim presents an immediate threat to the patient or that the victim had done the patient a terrible wrong (Nielssen et al., 2007). The grandiosity and increased confidence that is often present in mania could even be protective against serious violence. Manic patients might also retain some capacity for moral reasoning and empathy for other people, despite the effect of accelerated thinking and pleasure-seeking behavior. By contrast, the blunting of emotional responses and the impoverishment of thinking associated with schizophrenia-related psychosis could deprive many schizophrenic patients of the capacity for empathy as well as moral reasoning.
Another factor that might influence the propensity of patients with bipolar disorder to commit offences is the increased tendency to act on impulse, despite some controversy regarding whether impulsivity is a trait shared by many bipolar patients or is limited to the manic phase of illness (Moeller et al., 2001). An increased tendency to act on impulse may account for some less serious violence in psychiatric wards, and can also be found in the accounts of non-violent offences committed by patients in manic states and by manic patients with co-morbid substance use disorder (Carpiniello et al., 2011).
Substance abuse and other co-morbid disorders have been identified as factors that increase the propensity of people with bipolar disorder to commit offences, including violent offences. This observation is supported by the findings of our studies, because all 12 manic patients found NGMI had the additional diagnosis of a substance abuse disorder and two were intoxicated with alcohol at the time of the offense. In the related study we found, two cases of mania among those convicted of severe non-lethal violent offences also had substance abuse disorder and were affected by substances at the time of their offences (Yee et al., 2010). Hence, it is quite possible that the severe violence committed by those patients whilst manic was mainly due to the effects of substance use.
Conclusion
Although mania is considered to be a risk factor for aggression, there is little evidence of an association between mania, homicide or other severe forms of violence.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
Dr Nielssen has received speaker’s fees from AstraZeneca. Professor Malhi has served on advisory boards for, received honoraria from, and has been funded directly for research by AstraZeneca, Eli Lilly and Co., Jansen-Cilag, Lundbeck, Organon, Pfizer, Sanofi-Aventis, Servier and Wyeth.