
Abstract
Objective:
To determine whether a six-session group cognitive behaviour therapy (CBT) programme results in a greater reduction in depression symptoms than a brief intervention alone in cardiac patients with clinically significant symptoms of depression.
Method:
Fifty-seven community dwelling cardiac patients scoring >13 on the Beck Depression Inventory-II (BDI-II) received a single-session brief intervention. They were then block randomised to either six sessions of group CBT (n = 25) or no further intervention (BI; n = 32). All were re-assessed at 2, 6 and 12 months. Differences between treatment groups in the primary (BDI-II) and secondary [rates of depression; anxiety symptoms, as measured by the Hospital Anxiety and Depression Scale-Anxiety (HADS-A)] outcomes were examined using generalised linear mixed models with a random intercept term for the individual.
Results:
Significant improvements were seen for the total group from baseline to 12 months on BDI-II and HADS-A scores. However, no differences were found between the CBT and BI conditions on change in BDI-II score, rates of major depressive episode or HADS-A score. Post hoc analysis on the total group found 12-month symptom non-remission was associated with higher baseline BDI-II score (p = 0.03), more visits to health professionals 12 months prior to baseline (p = 0.05) and a greater likelihood of either drinking alcohol over recommended levels or smoking at baseline (p = 0.01).
Conclusions:
Group CBT of up to six sessions did not result in greater reductions in depression or anxiety symptoms compared with a single-session brief intervention. Further work should focus on the efficacy and role of brief interventions, and addressing smoking and alcohol misuse in cardiac patients with depression.
Introduction
Major depression is seen in around 20% of patients with differing cardiac conditions (Connerney et al., 2010; Freedland et al., 2003; Thombs et al., 2006) and is associated with increased morbidity and mortality (Connerney et al., 2010; Penninx et al., 2001; Rutledge et al., 2006; van Melle et al., 2004). Evidence suggests pharmacotherapy and psychological therapies are effective in reducing depression symptoms in people with cardiac disease (Baumeister et al., 2011). Cognitive behaviour therapy (CBT) is a relatively short and efficacious intervention that is one of the best known empirically-supported non-pharmacological depression treatments (Driessen and Hollon, 2010). CBT can be presented in individual and group formats. Group CBT has been used for secondary prevention in cardiac patients (Gulliksson et al., 2011) and in combination with individual therapy for depression treatment (Saab et al., 2009). However, we are not aware of any published randomised controlled trials (RCTs) of group CBT recruiting depressed cardiac patients and focused on the development of depression management skills (Baumeister et al., 2011).
Pilot work demonstrated a six-session group CBT intervention (the BraveHeart programme) may be effective in reducing symptoms of depression in cardiac rehabilitation graduates who still experienced depression symptoms near the end of the rehabilitation programme (Hambridge et al., 2009). Effect size of the programme was 0.74 six months after treatment. Participant feedback was positive. Participants were recruited after cardiac rehabilitation to allow for the common transient emotional adjustment period that many patients experience in the months following an acute cardiac event (Murphy et al., 2008; Poston et al., 2003). The present study expands on pilot work to determine whether the BraveHeart programme results in a greater reduction in depression symptoms than an individually administered, single-session brief intervention alone. Brief interventions that utilise psycho-education and individualised feedback have been shown to reduce symptoms of depression and psychological distress (Donker et al., 2009) and are less resource intensive than group therapy.
Community-dwelling cardiac patients (two or more months post-cardiac event) currently experiencing depressive symptoms were the target of the present study, rather than hospital inpatients. Broad inclusion criteria were utilised to represent cardiac patients who would likely attend a community-based group programme. While it was expected that a brief intervention may lead to some improvement in depression symptoms, it was hypothesised that group CBT would be associated with a significantly greater reduction in depression symptoms.
Methods
Design and settings
A single blind, block RCT was conducted comparing an individually administered single-session brief intervention followed by six sessions of group CBT with the brief intervention alone for the treatment of depression. Recruitment occurred between June 2006 and May 2008 in the Hunter New England region of NSW, Australia, and was open to people with established cardiac disease and current depression symptoms who were two months or more post-cardiac event. Ethical approval was gained from relevant institutions and all participants provided informed consent.
Participants
Potential participants were aged ≥18 years; had a cardiac event two months or more prior [acute coronary syndrome (ACS); percutaneous coronary intervention (PCI); coronary artery bypass grafting (CABG)] and/or confirmed diagnosis of a heart condition (coronary heart disease, congestive heart failure, cardiomyopathy, chronic atrial fibrillation); were currently experiencing clinically significant levels of depressive symptoms [>13 on the Beck Depression Inventory-II (BDI-II)] at initial screening; and provided informed consent. Exclusion criteria included history of, or current, psychotic illness or organic brain diseases at initial screening; anti-depressant medication for less than one month’s duration (to allow for stable therapeutic doses pre-treatment); and non-English speakers.
Procedure
Participants were recruited from the John Hunter Hospital cardiac rehabilitation programme and hospital discharge lists; media releases and advertisements; referrals from services and the Hunter Medical Research Institute (HMRI) Research Register. The Low Prevalence Disorder Study Psychosis Screener (Jabelensky et al., 2000) was used to exclude participants with a history of, or current, psychotic illness. Eligible and interested participants completed a one-hour face-to-face baseline assessment with a trained psychologist. Information gathered included current and past mental health symptoms and treatment, medical history, smoking and alcohol use, and waist girth measurements. Participants self-completed questionnaires regarding depression, anxiety, smoking and alcohol use, in addition to other measures not reported here (social support, hostility, demoralisation, quality of life and general functioning). The interviewer then delivered an individualised three-part brief intervention, including feedback of results from the interview, recommendations for treatment, and a letter to the general practitioner (GP) and selected health professionals.
Once a block of participants was recruited, participants in that block were randomly assigned to receive either an additional six weekly group CBT sessions (CBT) or no further intervention (BI). A block randomisation procedure was utilised, with a computer-generated random number sequence created by an independent researcher and placed in an opaque envelope. Maximum block size was 11 with smaller size at times of slower recruitment to ensure minimum time between assessment and allocation. Baseline assessors were informed of condition allocation once all participants in that block had completed their assessment. Participants were informed of their allocation by telephone call and/or letter.
All participants completed follow-up assessments at 2, 6 and 12 months with an assessor blind to treatment allocation. Participants were not blind to treatment status; however, established strategies were implemented to prevent the end-point assessors from becoming aware of treatment status, such as asking the patient not to reveal their allocated condition prior to every assessment interview. Participants were able to access additional treatments outside the research study and these were monitored during follow-up assessments. Participants were reimbursed with $20 per completed assessment.
Interventions
Initial session (brief intervention)
Participants received individualised verbal feedback regarding assessment results, including severity of depression and anxiety symptoms, likely presence of a depressive or anxiety disorder, alcohol consumption over National Health and Medical Research Council (NHMRC) guideline levels, and any other issues of concern. Then, recommendations for treatment; written self-help material on depression, anxiety and stress, with a general focus and in the context of co-occurring cardiac disease; and information regarding relevant mental health and support services were offered to the participants. Last, individualised letters (and phone call if symptoms were severe and/or concerning) were sent to the participant’s selected health professionals (cardiac rehabilitation nurse, GP, specialists) regarding baseline and two-month assessment results.
CBT programme
The CBT group intervention was the BraveHeart Program (Hambridge et al., 2009), a closed group programme consisting of six weekly sessions of CBT of 1.5 hours duration, with an extra hour at weeks 1 and 6. Two trained clinical psychologists (authors AT and JH) delivered the treatment, following the treatment manual, to a maximum group size of 11. Sessions commenced with a group discussion around experiences and learning from homework tasks. Participants were then introduced to various skills and homework was set for the following week. Content included psycho-education regarding emotional distress (Session 1), activity planning (Session 2), thought monitoring and challenging (Session 3), structured problem-solving (Session 4), strategies to increase motivation (Session 5), and a programme review and how to get further assistance (Session 6). An independent research assistant provided ratings on manual adherence and therapist skills in cognitive therapy using the Cognitive Therapy Scale (Young and Beck, 1980).
Measures
The 21-item BDI-II (Beck et al., 1996) is designed to measure severity of depression symptoms and has been shown to have reliable, internally consistent and valid scores in primary care medical patients (Arnau et al., 2001). Items are rated 0–3 (total score range 0–63), with higher scores indicating increased severity. Severity categories have been provided as minimal (0–13), mild (14–19), moderate (20–28) and severe (29–63).
The 14-item Hospital Anxiety and Depression Scale (HADS) (Zigmond et al., 1983), designed for use with medical outpatients, is well validated, including in cardiac patients (Hunt-Shanks et al., 2010). Anxiety was assessed using the anxiety subscale (HADS-A), which consists of 7 items rated 0–3 (total score range 0–21). Severity categories have been provided as minimal (0–7), mild (8–10), moderate (11–13) and severe (14–21).
The Structured Interview for DSM-IV (SCID) (First et al., 2002) Major Depressive Episode (MDE), Panic Disorder, Post-Traumatic Stress Disorder, Obsessive Compulsive Disorder and Generalised Anxiety Disorder modules were followed to determine presence of depression or anxiety diagnoses in the last six months.
Substance use (alcohol use and smoking) was assessed using the Opiate Treatment Index (OTI) Tobacco and Alcohol use subscales. The OTI is a valid and reliable measure of substance use, providing 98% and 88% agreement with collateral reports of tobacco and alcohol use respectively (Darke et al., 1992).
Adherence to treatment manuals was rated ‘Yes’ or ‘No’ for each session based on the following criteria: (1) all agenda items for that session were covered; (2) at least 50% of the session was spent on agenda items for that session; (3) no more than 25% of session time was spent on agenda items from other sessions; and (4) no more than 10% of session time was spent on non-agenda items. Criteria were developed based on recommendations provided by Evans et al., (1984). Non-agenda items were recorded to identify potential gaps in the treatment manual.
Therapist competence was measured using the Cognitive Therapy Scale (CTS), developed by Young and Beck, (1980) to measure a therapist’s strengths and weaknesses in the provision of cognitive therapy. The CTS is an 18-item scale with 4 parts: general therapeutic skills; conceptualisations, strategy and technique; additional considerations; and overall ratings and comments.
Analysis
Differences between treatment groups in the primary (BDI-II) and secondary (HADS-A) outcomes were examined using two different models: differences in change in the outcome of interest from baseline (Model 1) and differences in the mean level of the outcome of interest at visits 2–4 adjusting for the baseline value of the outcome variable (Model 2). Each model was fitted using generalised linear mixed models with a random intercept term for the individual. Post hoc analyses were carried out to determine the characteristics of patients who did and did not meet remission criteria at 12 months (BDI-II ≤13 and do not meet SCID criteria for Major Depressive Episode in the last 6 months). Differences were examined using Fisher’s exact test for categorical variables and t-tests for continuous variables. Data analysis was carried out using PASW Statistics Version 18.0.0 (SPSS Inc., Chicago, Il, USA), and SAS software Version 9.2 (SAS Institute Inc., Cary, NC, USA). Statistical significance was defined by a p-value <0.05. Final sample size at 12 months (20 CBT and 27 BI) provided 82% power to detect a treatment effect size of 0.85 (using 0.05 level two-tailed significance tests).
Results
Sample characteristics
A total of 160 potential participants were identified through cardiac rehabilitation (30%), referrals from services (3.8%), media (34.3%), hospital discharge lists (20%) and the HMRI Research Register (11.9%). Of these, 57 were eligible and interested, and attended an initial assessment (Figure 1). Reasons for non-participation included ineligibility (61.2%), refusal (26.2%) or being uncontactable (12.6%). The majority of the final sample (n = 57; 72% male; mean age = 62 years, SD = 10 years) had past admissions or treatment for ACS, PCI, or CABG (n = 50, 88%). The remaining (n = 7, 12%) had only received treatment for congestive heart failure, chronic atrial fibrillation or cardiomyopathy. No significant differences occurred between the CBT (n = 25) or BI conditions (n = 32) on any of the baseline characteristics (Table 1).
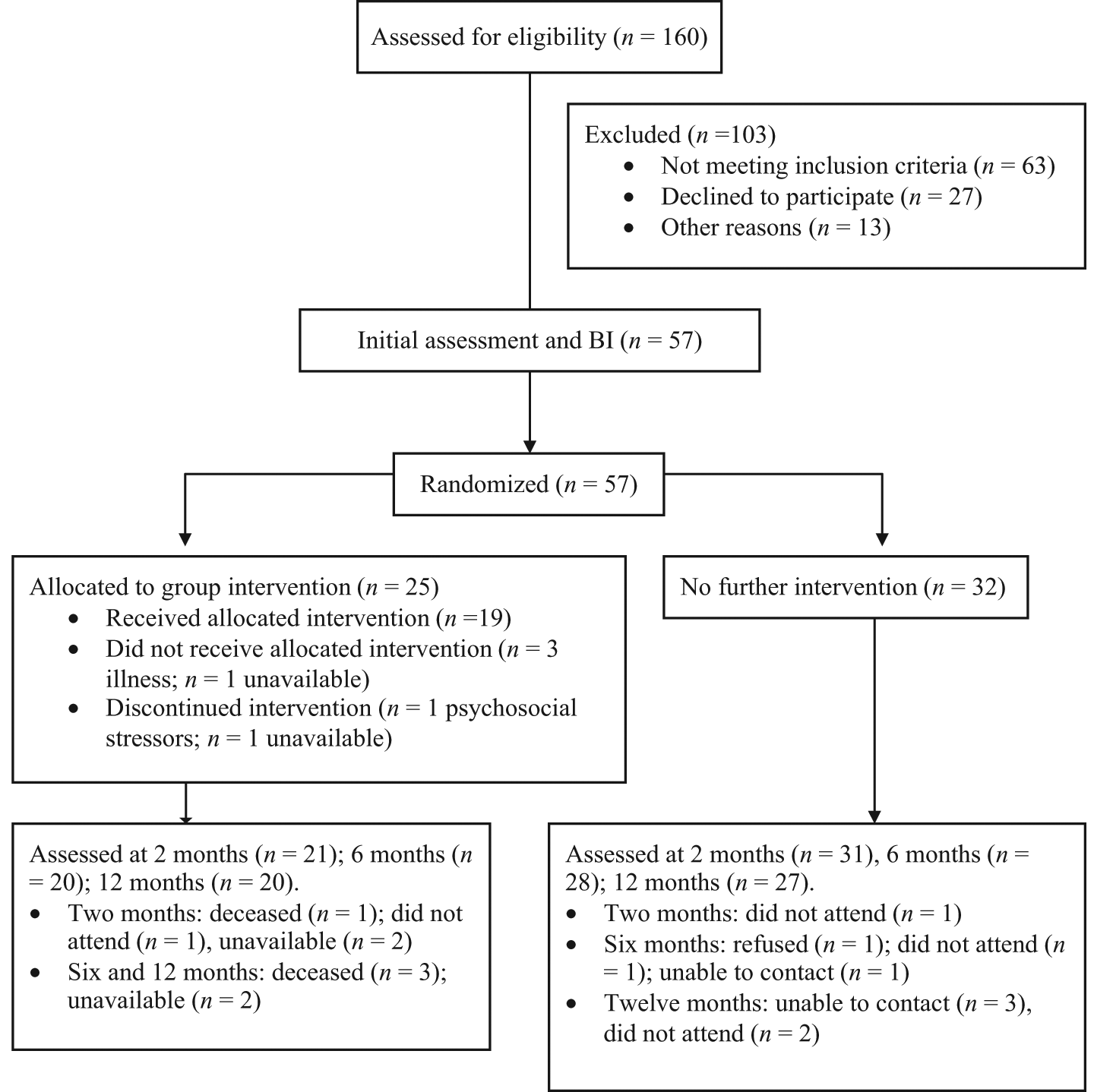
Participant flow through the study.
Demographic and other baseline characteristics.
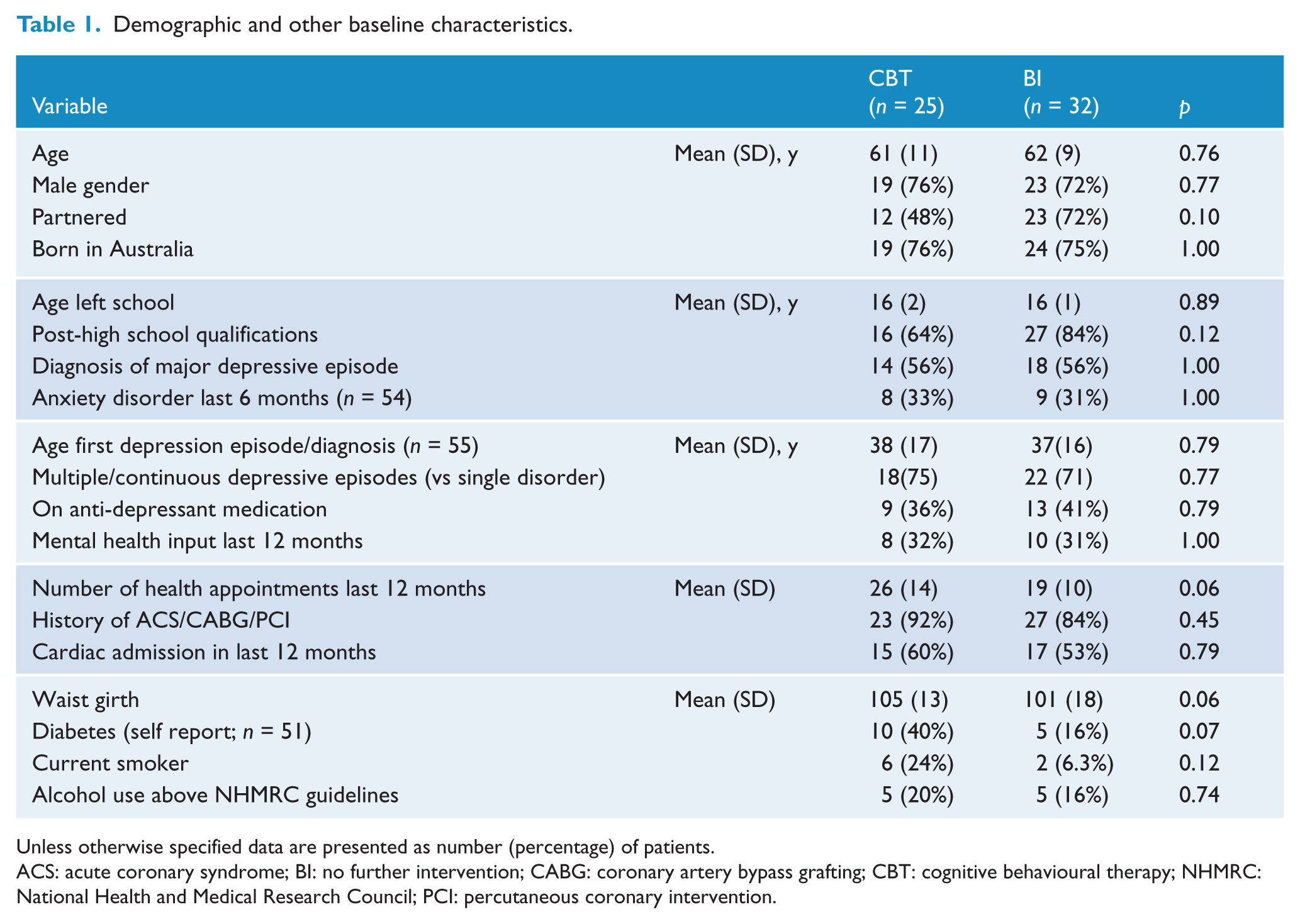
Unless otherwise specified data are presented as number (percentage) of patients.
ACS: acute coronary syndrome; BI: no further intervention; CABG: coronary artery bypass grafting; CBT: cognitive behavioural therapy; NHMRC: National Health and Medical Research Council; PCI: percutaneous coronary intervention.
Treatment uptake and fidelity
Twenty-five participants were allocated to CBT. Baseline assessments for these participants occurred 1–36 days before treatment initiation (median = 14, IQR 6.5–22 days). Four CBT participants (16%) did not commence the group programme, 1 (4%) discontinued after 1 week and 1 (4%) discontinued after 3 weeks. Of the remaining participants, 4 (16%) attended 4 sessions, 6 (24%) attended 5 sessions and 9 (36%) attended 6 sessions. Fidelity analysis was conducted on 15 sessions (3 lost because of recording issues) and all sessions met adherence criteria. The average ‘Overall’ therapist rating on the CTS was 3.2 (SD = 0.6), which equates to a ‘good’ ranking (this should be interpreted with caution as the CTS was not designed for manualised group programmes conducted by multiple facilitators). Topics raised by participants not included in the manual were around guardianship, social support, alcohol use and medication.
For participants for whom data were available, no differences were seen between the CBT or BI conditions in (a) number of participants who had mental health professional input during the 12-month study period [CBT n = 8 (44%) vs BI n = 12 (43%), p = 1.0, Fishers Exact Test] or (b) number of participants who were on anti-depressant medication at the 12-month assessment [CBT n = 11 (55%) vs BI n = 11 (41%), p = 0.39, Fishers Exact Test].
Change in depression and anxiety symptoms
There was no significant difference in change over time between the CBT and BI conditions on the BDI-II or HADS-A (Table 2). Significant improvements were seen for the total group from baseline to 12 months (reduction in BDI-II scores (95% CI) = 9.9 (7.4–12.4), p <0.0001; reduction in HADS-A scores (95% CI) = 3.6 (2.5–4.8), p <0.0001; with adjustment for clusters). No difference was found in the rate of CBT or BI participants who were in the ‘minimal’ symptom severity category (scores <14) at 2, 6 or 12 months; had a diagnosis of MDE at 6 or 12 months; or met remission criteria (i.e. BDI-II in the ‘minimal’ range and not meeting SCID criteria for MDE) at 12 months.
Depression and anxiety symptoms and depression diagnoses at all time points.
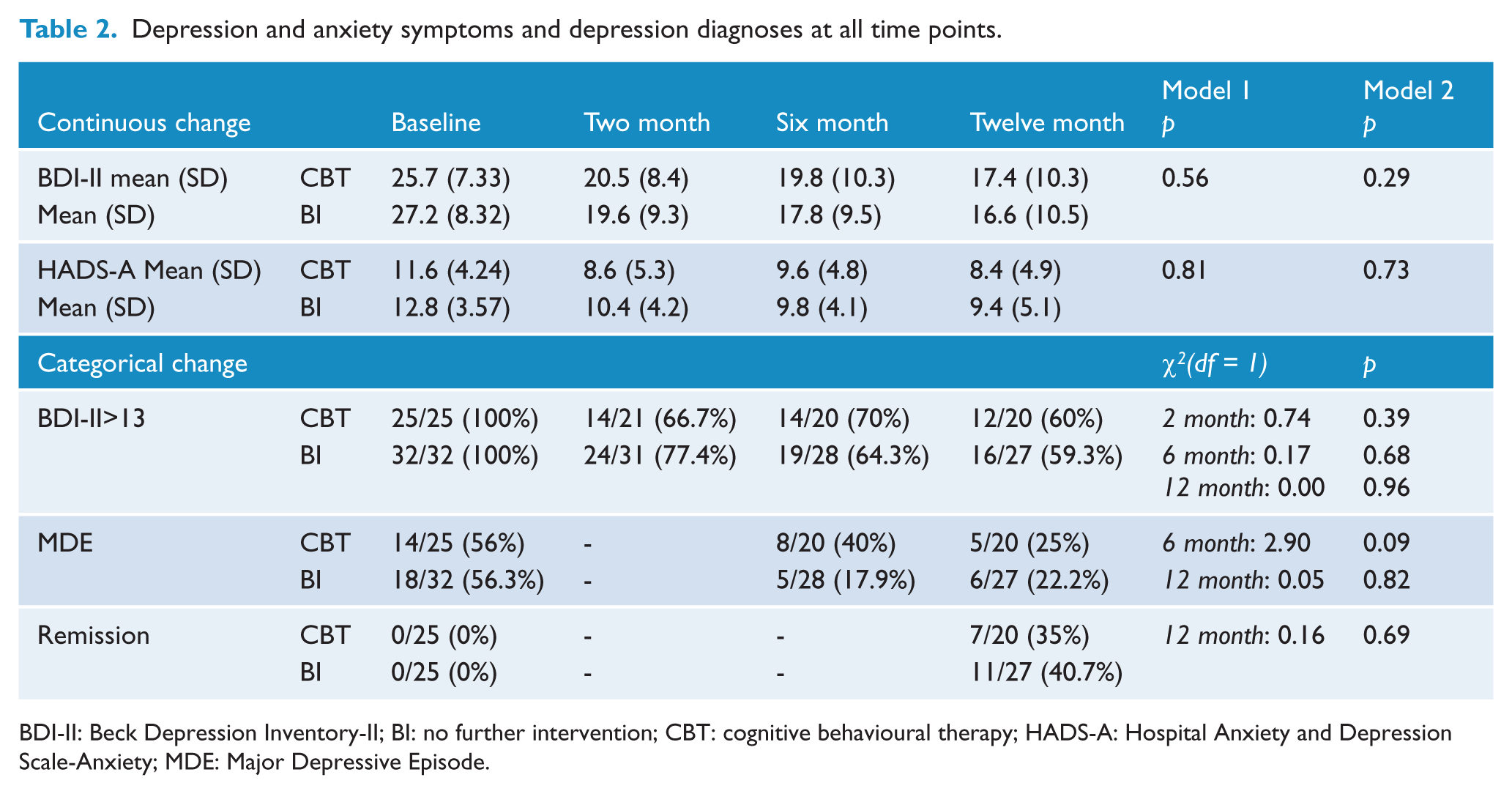
BDI-II: Beck Depression Inventory-II; BI: no further intervention; CBT: cognitive behavioural therapy; HADS-A: Hospital Anxiety and Depression Scale-Anxiety; MDE: Major Depressive Episode.
Predictors of depression remission at 12 months
As no difference in treatment response was found between the conditions, the two groups were collapsed into a single group to examine baseline factors associated with remission from depression at 12 months. Categorical variables included: gender, partner status, any cardiac admissions in the 12 months prior to baseline, current smoker and/or alcohol misuse (alcohol use above NHMRC guidelines, defined by an OTI score of >2) at baseline, depressive episode at baseline (on SCID interview), any anxiety disorder at baseline (on SCID interview), course of depression symptoms (single episode/ multiple or continuous episodes), on anti-depressant medication at baseline, and any mental health input 12 months prior to baseline. Continuous baseline variables examined included: age, number of appointments with all health professionals in the 12 months prior to baseline, waist girth, age of first depressive episode, baseline depression score (BDI-II), and baseline anxiety score (HADS-A). Participants who did not meet remission criteria at 12 months had significantly higher baseline BDI-II scores, more visits to health professionals in the 12 months prior to baseline and were more likely to smoke and/or drink alcohol over recommended levels at baseline (6 of 7 smokers and 9 of 10 alcohol users did not reach remission).
Discussion
We compared a group intervention with a brief intervention alone and found no difference in outcome between the two approaches. Both the CBT and BI conditions were associated with an improvement in depression and anxiety symptoms. Categorically, both groups moved from the high end of the ‘moderate’ range of depression symptoms at baseline, to the ‘mild’ range of symptoms by 12 months. Improvements seen were similar to pilot results despite the present sample having higher baseline depression scores (a BDI-II score of 26 compared to 22 (Hambridge et al., 2009)).
The primary limitation of the study is the small sample size, limiting study power to detect treatment effects smaller than 0.85. However, a trend to greater change in the CBT group was not seen in any outcome measure. Indeed, the only trend seen was for lower rates of major depressive episode at 6 months in favour of the BI group, with 17.5% of BI participants meeting criteria for MDE at 6 months compared with 40% of CBT group participants.
Several other limitations are worth noting. Sample heterogeneity resulting from broad inclusion criteria around cardiac presentation and no exclusion criteria regarding age or (non-psychotic) psychiatric diagnoses or treatments may have masked differences in treatment response. However, as the resulting sample is likely to be representative of the mixed characteristics of people that would participate in a community-based depression treatment group this is also a study strength. Additionally, the block randomisation process, chosen to minimise time between baseline assessment and group commencement, is less ideal than individual randomisation. No adjustment was made for the clustering as this would have made little difference to the null result. Furthermore, while no significant baseline differences occurred between conditions, trends were seen for the CBT group to be less likely to be partnered, more likely to have self-reported diabetes, report more visits to health professionals in the 12 months prior to baseline and have greater waist girth. These differences may have led to differential treatment response. A larger study with faster recruitment rates would allow for an individually randomised study of a closed group programme. However, this would limit recruitment sites to densely populated metropolitan areas, impacting on the generalisability of findings.
While group CBT has been previously shown to be effective (Huntley et al., 2012), our results are in line with a recent meta-analysis of CBT in people with concurrent physical illness (Beltman et al., 2010). This analysis found that only individual, and not group, CBT led to significant treatment effects, suggesting that individual CBT may be more appropriate for people with concurrent physical illness. Alternatively, it may be that the intensity of the CBT intervention in the present study was insufficient to lead to improvements above what can be gained by a single session individual intervention. Of those invited to attend the group, only 36% attended all 6 group sessions. Reducing the number of components covered (to cognitive or behavioural or problem-solving strategies alone) may ensure participants learn a single approach well regardless of whether therapy sessions are missed. In patients with arthritis it was found that the effect of cognitive therapy was not enhanced by adding behavioural components (Sharpe and Schrieber, 2012). There is evidence for problem-solving therapy as a treatment for depression in people with executive dysfunction (Arean et al., 2010), cancer (Nezu et al., 2003), and medically ill outpatients (Gellis et al., 2007). Problem-solving therapy has been found to have lower drop-out rates than CBT in depression treatment studies (Cuijpers et al., 2008).
Characteristics of participants meeting and not meeting remission criteria at 12-month assessment.
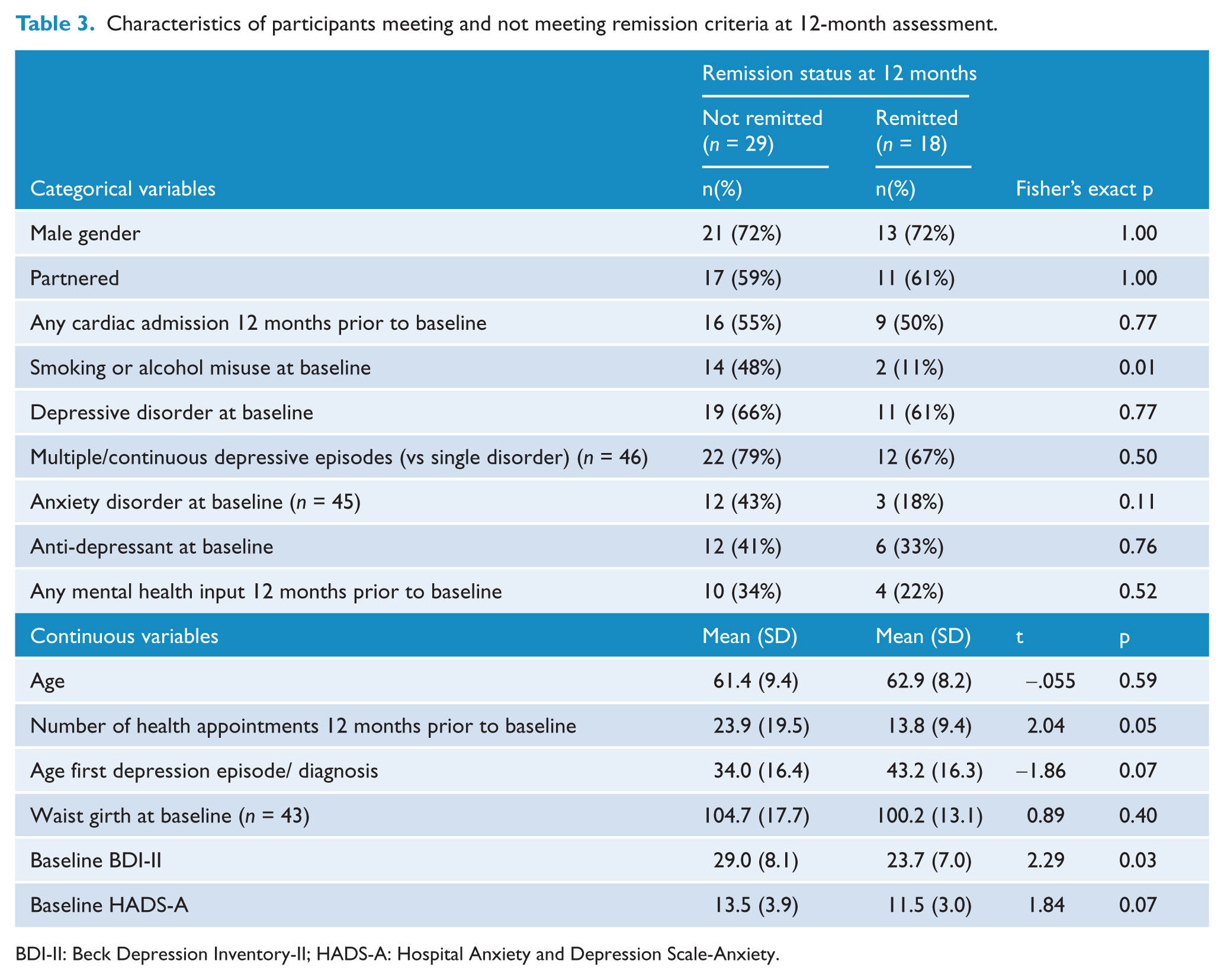
BDI-II: Beck Depression Inventory-II; HADS-A: Hospital Anxiety and Depression Scale-Anxiety.
Non-response to depression treatment following acute myocardial infarction has been associated with increased cardiac morbidity (de Jonge et al., 2007). In our sample non-remission of symptoms was associated with higher levels of baseline depression symptoms, greater healthcare utilisation 12 months prior to baseline, and smoking and/or alcohol use above recommended levels at baseline. Clearly, smoking, alcohol and depression comorbidity should be targeted in future studies. Brief and longer integrated interventions for comorbid depression and alcohol problems have been shown to be effective (Baker et al., 2010; Kay-Lambkin et al., 2009), while psychosocial interventions have been found to be effective in assisting cardiac patients in smoking cessation (Barth et al., 2008). These interventions should be further evaluated in depressed cardiac patients to examine the impact on both substance use and mood outcomes.
Further work should focus on the efficacy and role of brief interventions for depressed cardiac patients. Improvement seen in depression scores from baseline to 12 months across both conditions may be indicative of intervention efficacy or they may be regression to the mean. To confirm that these improvements were associated with the interventions rather than other factors, a further trial is required to establish the superiority of a single-session intervention over a no intervention control group. Additionally, as clinical psychologists were responsible for delivering both interventions, efficacy of brief interventions delivered by other health professionals and/or by other delivery options (telephone, internet) could also be explored. Even if group therapy offers additional benefits for members that were not captured in the chosen outcome measures, other treatment options need to be available for those who cannot, or do not want to, participate in a group programme. Providing intervention options that vary in intensity and focus will improve the reach and efficacy of treatment for cardiac patients with depression symptoms.
Footnotes
Acknowledgements
The authors wish to thank the HMRI Research Register and staff from the John Hunter Hospital cardiac rehabilitation programmes.
Funding
This research was funded by a grant from Australian Rotary Health.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.