
Abstract
Objective:
To investigate the clinical efficacy of minimally invasive subpial tonsillectomy (MIST) in the treatment of Chiari malformation (type I) with syringomyelia. Method A total of 209 Chiari malformation (type I) patients with syringomyelia were studied. The patients were grouped based on the syrinx diameter changes: complete disappearance group (48 patients), obvious shrinkage group (147 patients), and non-obvious shrinkage group (14 patients). The Chicago Chiari Outcome Scale (CCOS) was used to compare clinical data of the three groups of patients before treatment. The correlations between disease duration and syrinx diameter changes as well as post-treatment clinical symptoms were analyzed. The related factors of efficacy were analyzed.
Results:
Age and disease duration were the oldest/longest in the non-obvious shrinkage group, and the youngest/shortest in the complete disappearance group (P < 0.05). The maximum diameter reduction of syrinx was the greatest in the complete disappearance group, and the smallest in the non-obvious shrinkage group (P < 0.05). The proportions of patients with hypoesthesia, limb weakness, and muscle atrophy were the largest in the non-obvious shrinkage group, and the smallest in the complete disappearance group (P < 0.05). The CCOS score were the highest in the complete disappearance group, and the lowest in the non-obvious shrinkage group (P < 0.05). There were statistically significant (P < 0.05) negative correlations between disease duration and maximum diameter reduction of syrinx, CCOS pain score, CCOS non-pain score, CCOS functionality score, and CCOS complication score, disease duration and hypoesthesia, limb weakness, muscle atrophy, and sleep apnea. Result of multivariate stepwise regression analysis indicated that age, disease duration, and preoperative syrinx diameter were the risk factors for efficacy (P < 0.05).
Conclusion:
For patients with Chiari malformation complicated by syringomyelia, the longer the disease duration, the more difficult it is to achieve syrinx reduction and improve the clinical symptoms. “Minimally invasive subpial tonsillectomy (MIST) and cisterna magna reconstruction” is an improved surgical approach to treat Chiari malformation (cerebellar tonsil herniation). It has the advantages of small incision, less postoperative reaction, and fewer complications, and it emphasizes the reshaping and repair of cerebellar tonsils, reconstruction of cisterna magna, and restoration of cerebrospinal fluid circulation.
Keywords
1 Introduction
Syringomyelia (SM) is a serious chronic and progressive disease of the spinal cord that can result in paraplegia [1], and cerebellar tonsil herniation, also known as Chiari malformation, is recognized as its main cause. Chiari malformation occupies the space of the foramen magnum, causing overcrowding in the posterior cranial fossa, which subsequently results in obstruction of cerebrospinal fluid circulation in the foramen magnum region. As a result, the cerebrospinal fluid circulation and the pressure balance between the cranial cavity and the vertebral lumen were impaired, leading to degeneration, liquefaction, and atrophy of the central parenchyma of the spinal cord and inducing syrinx formation. Surgery is currently the primary treatment for syringomyelia, which relieves pressure in the craniocervical junction, eliminates intrinsic compression factors, and reduces cavitation to relieve the patient’s symptoms [2–4]. It also helps to restore normal cerebrospinal fluid circulation in the cisterna magna [5]. Although more than 20 surgical approaches have been reported to restore cerebrospinal fluid circulation and relieve nerve compression [6], none of the traditional approaches in China and abroad have exhibited satisfactory efficacy in treating Chiari malformation (type I) with syringomyelia. Studies have reported that traditional posterior fossa decompression had multiple complications such as secondary cerebellar ptosis and postoperative scar hyperplasia compression [7–9], and the reoperation rate after decompression was up to 17%. In addition, many studies showed that the herniated cerebellar tonsil had true hypertrophy and the hypertrophic cerebellar tonsil was the cradle of syringomyelia [10]. Therefore, the removal of herniated cerebellar tonsils could relieve posterior cerebral compression, restore cerebrospinal fluid circulation, and reduce the syrinx. The efficacy evaluation criteria for surgical treatment of Chiari malformation (type I) with syringomyelia in previous literature reports were mostly subjective [11], although they have made certain positive contributions, the lack of objective quantitative criteria is apparent. At present, MRI is the most simple, accurate, and indispensable examination technique for Chiari malformation with syringomyelia. MRI measures the maximum diameter of the syrinx before and after surgery, helping to include the syrinx diameter change in the evaluation indicators. The Chicago Chiari Outcome Scale (CCOS) evaluation system quantitatively evaluates surgical efficacy from four aspects: pain-related symptoms, non-pain-related symptoms, functionality, and complications. It also adds the objective criterion of imaging evaluation on postoperative syrinx shrinkage. By combining imaging evaluation with clinical symptom assessment, the scale possesses the merits of both subjective and objective evaluation means and has practical clinical application value [12, 13]. Therefore, in this study, Chiari malformation (type I) with syringomyelia was treated by MIST, and the surgical efficacy was evaluated comprehensively via CCOS and imaging evaluation, as well as traditional methods. The report is as follows:
2 Materials and Methods
2.1 General Information
A total of 209 Chiari malformation (type I) patients with syringomyelia diagnosed by MRI were retrospectively analyzed. They were hospitalized at Yuquan Hospital of Tsinghua University within the period of January 2016 to December 2018. Inclusion criteria: 1) Sagittal MRI of the head showed that the inferior border of cerebellar tonsil was ≥ 5 mm below the foramen magnum; 2) Underwent MIST and cisterna magna reconstruction; 3) MRI scan of the spine showed dilated central canal of the spinal cord; 4) Good compliance. Exclusion criteria: 1) Chiari malformations (types II and III) and complex craniocervical junction malformations (including atlantoaxial dislocation, basilar depression, atlanto-occipital fusion, scoliosis, etc.) 2) Incomplete clinical data; 3) MRI of the head showed supratentorial space-occupying lesion or hydrocephalus; 4) Other serious nervous system diseases; 5) MRI of the spine showed infarction, trauma, tumor, or other space-occupying lesions. All subjects provided informed consent and the protocol was approved by the Ethics Committee of the hospital. There were 77 males and 132 females who were aged 21–66 years, with a mean age of (41.50 ± 10.72) years. The disease duration was 21–342 months, and the mean duration was (94.95 ± 77.98) months. The main clinical manifestations were headache in 151/209 patients (72.25%), dizziness in 74/209 patients (35.41%), neck and shoulder pain in 122/209 patients (58.37%), dysphagia in 23/209 patients (11.00%), coughing on fluids in 40/209 patients (19.14%), hoarseness in 14/209 patients (6.70%), ataxia in 15/209 patients (7.18%), nystagmus in 11/209 patients (5.26%), limb numbness in 139/209 patients (66.51%), dissociative sensory disturbance in 146/209 patients (69.86%), limb weakness in 66/209 patients (31.58%), muscle atrophy in 53/209 patients (25.36%), and sleep apnea syndrome in 11/209 patients (5.26%). See Figure 1 for details. Since some patients might have multiple clinical symptoms, the total number of symptoms is greater than the total number of patients. All patients underwent MRI (3.0T) scans of the head, neck, and chest. The cerebellar tonsillar hernias were all below the foramen magnum by more than 5 mm. Syrinx formation was more common in the cervical and thoracic segments, with long T1 and long T2 signals, and some syrinxes showed heterogeneous fluid signals (Figure 2). Syrinxes on axial scan were mostly quasi-circular in the center or near the anterior aspect of the spinal cord (Figure 2), while some syrinxes were collapsed with irregular shapes (Figure 3). The patients were grouped based on the syrinx diameter changes within 6–12 months into the following: complete disappearance group (complete disappearance of syrinx, 48 patients), obvious shrinkage group (more than 30% reduction in syrinx diameter, 147 patients), and non-obvious shrinkage group (less than 30% reduction in syrinx diameter, 14 patients).

Pictures of clinical manifestations related to syringomyelia.
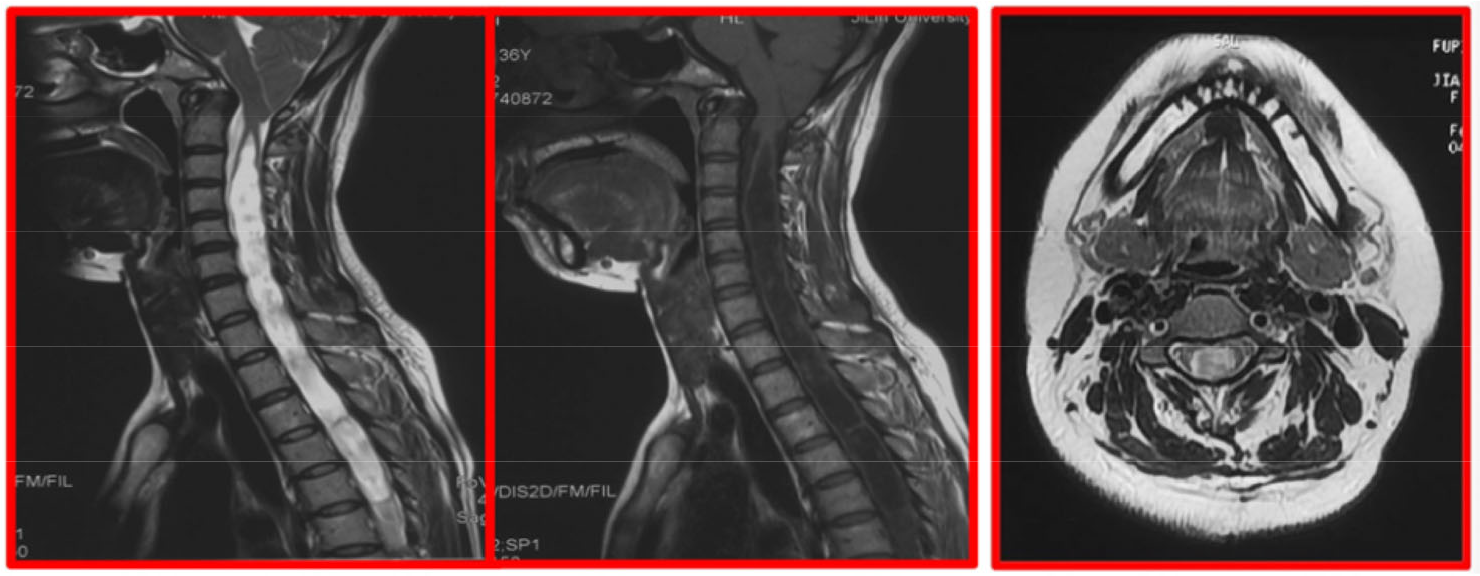
Sagittal MRI scan showing the degree of tonsillar herniation and the extent of syringomyelia, and syrinx on the axial scan, mostly quasi-circular in the center or near the anterior aspect of the spinal cord.
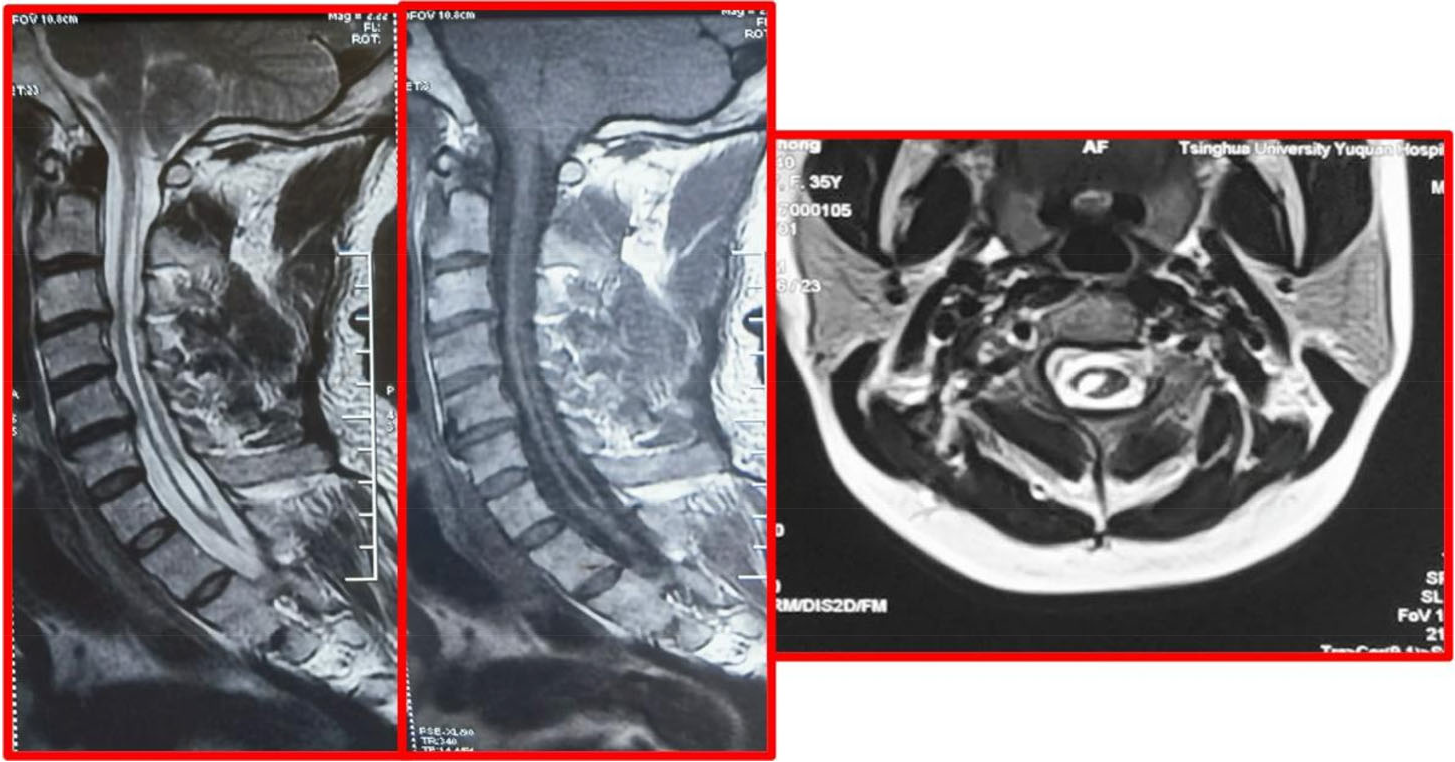
Some collapsed syrinxes with irregular shapes.
2.2 Methods
2.2.1 Surgical method
Minimally invasive subpial tonsillectomy (MIST) and cisterna magna reconstruction The patient underwent general anesthesia and endotracheal intubation, and was in the left lateral decubitus position, with his/her head fixed by a head holder, so that the neck could be extended as much as possible. Skin mark was drawn at 4 cm below the occipital tuberosity in the posterior occipital region. A 1.5–2.5 cm longitudinal incision was made along the posterior occipitocervical skin by incising the scalp and the nuchal line. The self-made retractor was used to expose the squamous part of occipital bone and the posterior arch of atlas. Then the posterior edge of the foramen magnum was exposed, and a small portion of the squamous part of occipital bone was removed while preserving the posterior arch of atlas (when the cerebellar tonsillar hernia exceeded the lower edge of the atlas, the posterior arch of atlas was partially resected). The dura mater was fully exposed after peeling off the atlanto-occipital fascia (Figure 4). The dura mater and the arachnoid mater were incised longitudinally and retracted with silk sutures on both sides, and the adhesions between the brainstem, cerebellar subtonsillar hernia, pia mater, and posterior inferior cerebellar artery were separated. After exposing the median foramen of the fourth ventricle, clear ventricular fluid could be seen flowing out from the base and the outlet of the fourth ventricle, which fluctuates with respiration. Subpial resection was performed to remove the part of cerebellar tonsils that obstructs the median aperture and the lateral cerebellomedullary cistern, so that the median aperture of the fourth ventricle and the lateral cerebellomedullary cisterns were unobstructed. After resection, it was confirmed that there was no active bleeding and then the opening of the pia mater was sealed by electrocoagulation. The arachnoid mater and dura mater were sutured continuously, while the muscle, fascia, and subcutis were closed tightly in layers via subcuticular mattress suture with absorbable sutures. No drainage tube placement was required. The surgical operations of all patients were completed by the same team (Figures 5 and Figure 6).
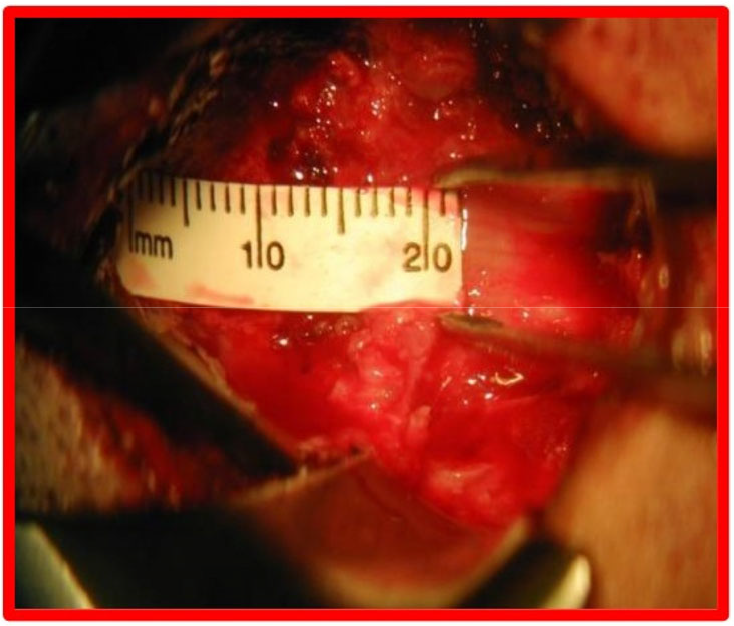
Microscopic separation of the atlanto-occipital fascia to expose the dura mater.
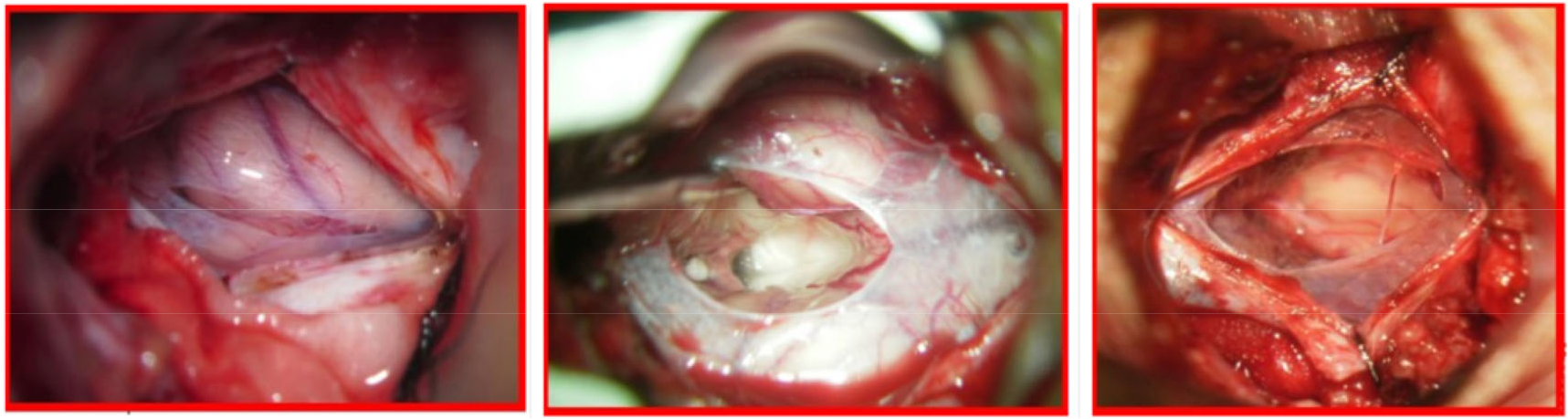
Microscopic incision of the dura mater and retraction with silk sutures on both sides, incision of the arachnoid mater, separation of left and right cerebellar tonsils, and exploration of the median aperture of the fourth ventricle, as well as microscopic subpial resection of part of the cerebellar tonsils to ensure that the outlet of the fourth ventricle and the lateral cerebellomedullary cisterns were unobstructed.

Continuous suturing of the arachnoid mater, the dura mater, and the skin with 8-0 prolene suture, 6-0 prolene suture and 5-0 absorbable suture, respectively.
2.2.2 Evaluation method
1) Efficacy evaluation
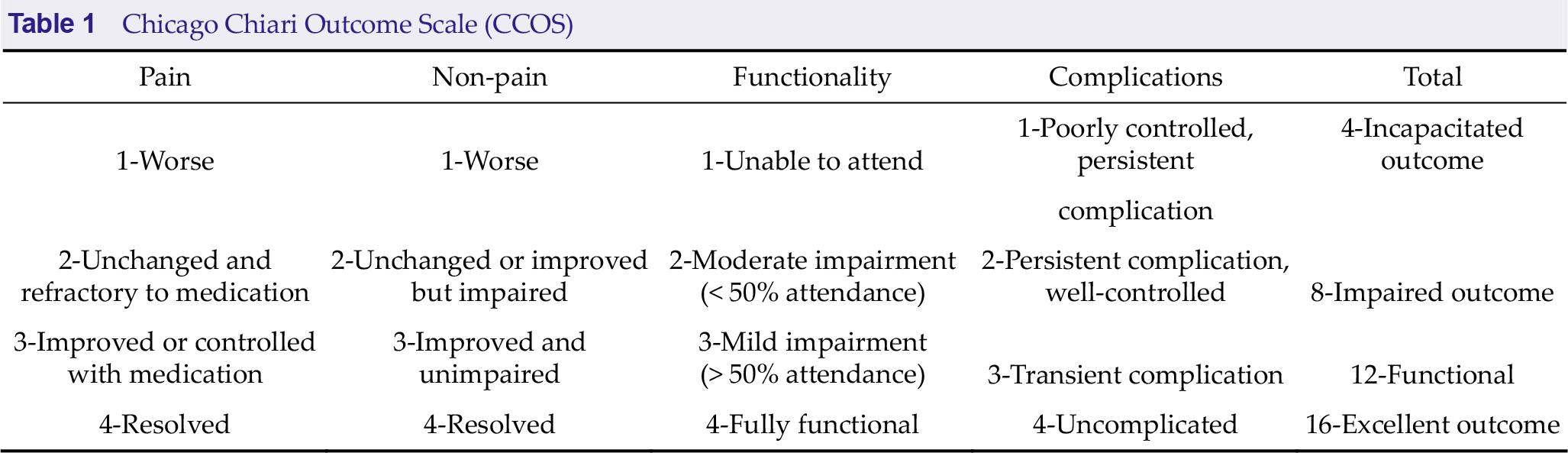
The Chicago Chiari Outcome Scale (CCOS) was selected based on Chinese and international literature to evaluate the prognosis of patients. The scale consists of four categories: pain symptoms, non-pain symptoms, functionality, and surgical complications. A patient is given a score of 1–4 for each item, and the better the prognosis, the higher the score. Improvements in pain and non-pain symptoms were evaluated relative to the patient’s preoperative symptoms. The scores were given by both the physician in charge and the operator. The scores are shown in Table 1.
Chicago Chiari Outcome Scale (CCOS)
2) Safety evaluation
Clinical symptoms such as headache, dizziness, neck and shoulder pain, dysphagia, coughing on fluids, hoarseness, ataxia, nystagmus, hypothermia or (and) limb sensation, and movement disorder were recorded in eCRFs and compared between groups.
3) Observation measures
The general clinical data of the three groups of patients before treatment were compared. Inter- group comparisons were made on the patients’ post-treatment CCOS scores. The correlations between disease duration and syrinx diameter changes as well as post-treatment clinical symptoms were analyzed. The related factors of efficacy were analyzed.
2.2.3 Statistical methods
SPSS 23.0 was used for statistical analysis. The measurement data were represented by mean ± standard deviation (`c ± s), which were first tested for homogeneity of variance to ensure that the conditions for multivariate analysis of variance (ANOVA) were met, and then ANOVA was adopted for inter-group comparisons. Enumeration data were represented by frequencies and percentages, and subjected to inter-group comparisons by c2 tests. The correlation analysis was performed using Pearson correlation test. The related factors were investigated with multivariate stepwise logistic regression analysis. When P was < 0.05, the difference was considered statistically significant.
3 Results
3.1 Inter-group comparison of subjects’ general information before treatment
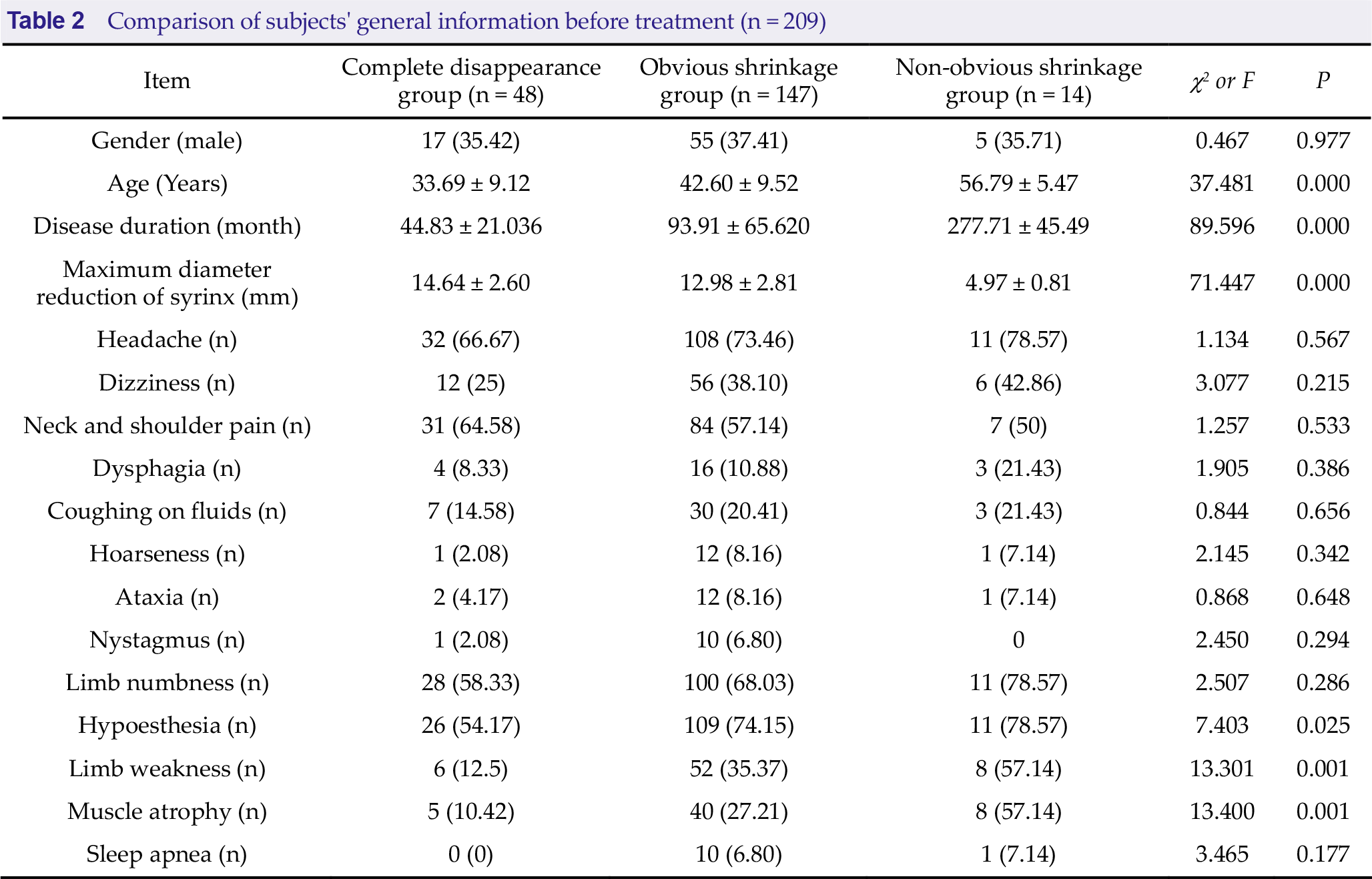
A total of 209 subjects were included in this study and all the subjects underwent MIST and cisterna magna reconstruction. Inter-group comparison results showed that age and disease duration were the oldest/longest in the non-obvious shrinkage group, followed by the obvious shrinkage group, and the youngest/shortest in the complete disappearance group (P < 0.05). The maximum diameter reduction of syrinx was the greatest in the complete disappearance group, followed by the obvious shrinkage group, and the smallest in the non-obvious shrinkage group (P < 0.05). The proportions of patients with hypoesthesia, limb weakness, and muscle atrophy were the largest in the non-obvious shrinkage group, followed by the obvious shrinkage group, and the smallest in the complete disappearance group (P < 0.05). Refer to Table 2 for details.
Comparison of subjects’ general information before treatment (n = 209)
3.2 Inter-group comparison of post-treatment CCOS scores
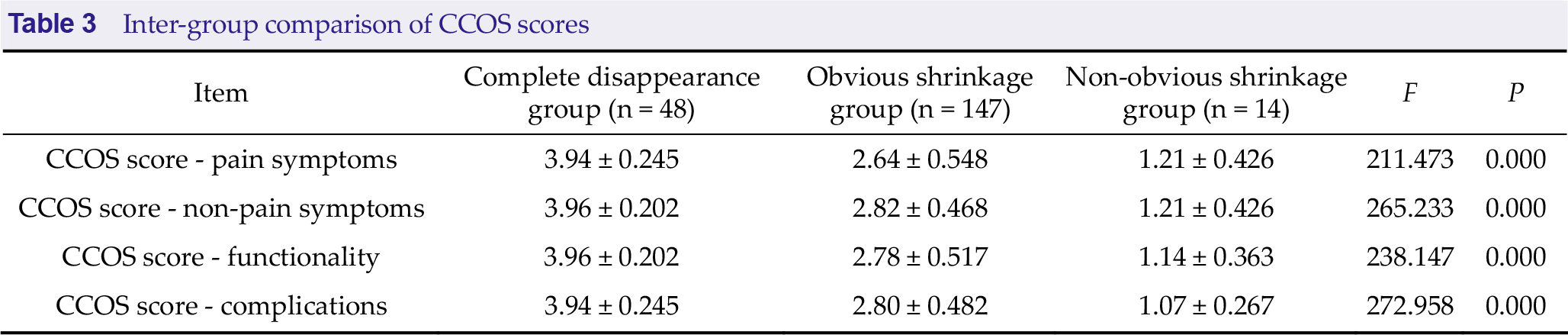
Post-treatment CCOS scores were the highest in the complete disappearance group, followed by the obvious shrinkage group, and the lowest in the non-obvious shrinkage group (P < 0.05). Refer to Table 3 for details.
Inter-group comparison of CCOS scores
3.3 Correlation between disease duration and syrinx diameter changes
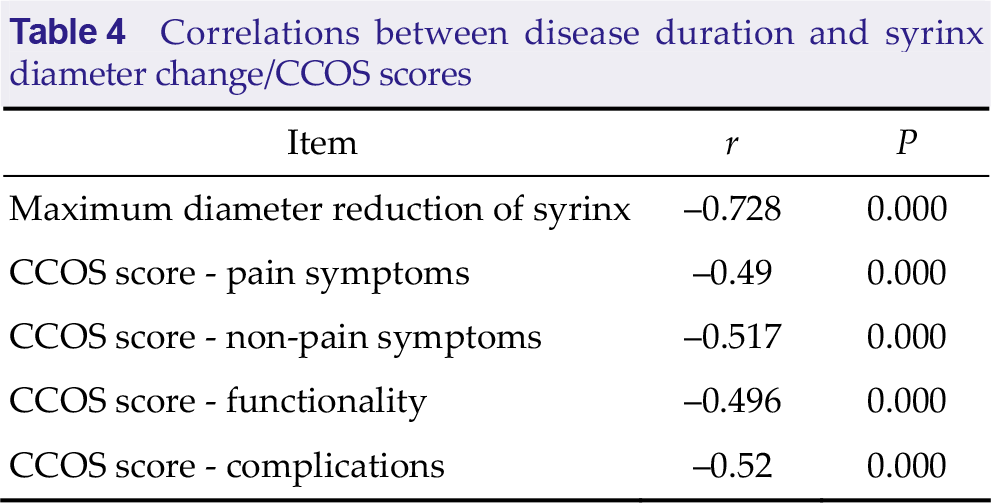
Pearson correlation test revealed that there were statistically significant (P < 0.05) negative correlations between disease duration and maximum diameter reduction of syrinx, CCOS pain score, CCOS non-pain score, CCOS functionality score, and CCOS complication score. Refer to Table 4 for details.
Correlations between disease duration and syrinx diameter change/CCOS scores
3.4 Correlation between disease duration and post-treatment clinical symptoms
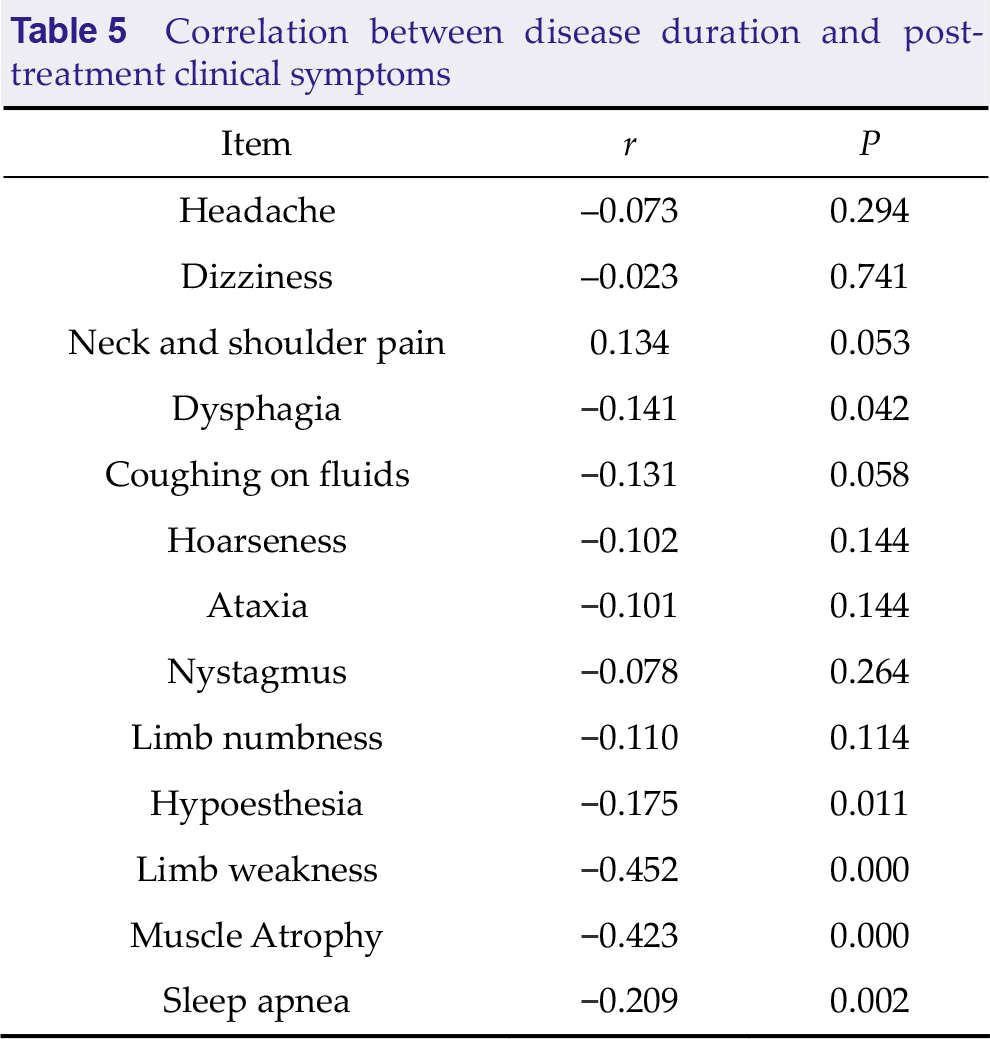
Pearson correlation test showed that there were statistically significant (P < 0.05) negative correlations between disease duration and hypoesthesia, limb weakness, muscle atrophy, and sleep apnea. Refer to Table 5 for details.
Correlation between disease duration and post- treatment clinical symptoms
3.5 Multivariate stepwise logistic regression analysis on treatment efficacy
Multivariate stepwise regression analysis was performed with the complete disappearance, obvious shrinkage, and non-obvious shrinkage of syrinx after treatment as the dependent variables, and age, disease duration, and preoperative syrinx diameter as the independent variables. Results indicated that age, disease duration, and preoperative syrinx diameter were the risk factors for efficacy (P < 0.05). Refer to Table 6 for details.
Multivariate stepwise logistic regression analysis on prognostic factors

3.6 Comparison of postoperative complications
Compared with previous studies, there was no significant difference in complications between patients with Chiari malformation and syringomyelia after partial tonsillectomy and traditional posterior fossa decompression (P > 0.05) (Table 7).
Comparison of postoperative complications.

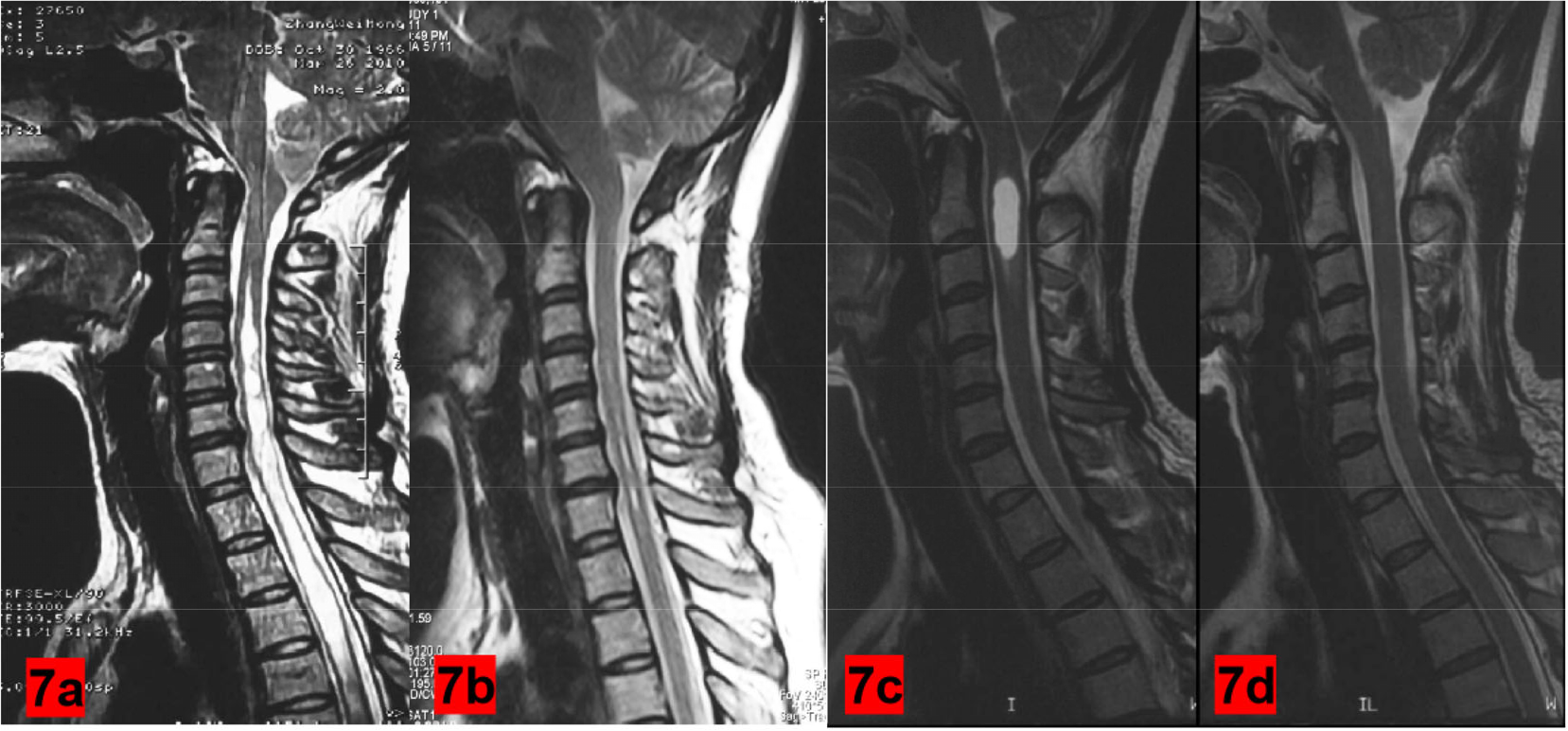
3.7 Preoperative and postoperative imaging comparison
After the implementation of “minimally invasive subbringeal subtonsillar hernia resection (MIST) and cisterna reconstruction”, the occipital magnum pool space was normal and the spinal void was significantly reduced and disappeared; the posterior arch could be preserved (Figures 7).
4 Discussions
Syringomyelia has been proven to be associated with Chiari malformation, spinal cord trauma, subarachnoid adhesions, etc. [14] Many previous theories explained the mechanism of syringomyelia secondary to Chiari type I malformation [15–20], but there is currently no definitive conclusion. We believe that reconstruction of the cisterna magna and restoration of cerebrospinal fluid circulation in the subarachnoid space is the fundamental strategy of treatment. At present, there are two main surgical approaches for the treatment of type I Chiari malformation with syringomyelia: One is posterior fossa decompression (PFD) [17], which has certain therapeutic effect but limited efficacy, and syringomyelia is prone to recur. The other is posterior fossa reconstruction (PFR), a modified technique to eliminate the defects of PFD [18]. On the basis of PFD, PFR reconstructs (or enlarges) the cisterna magna with the subarachnoid space being intact, repairs the incision with an artificial dura mater (or autologous fascia), and suspends it like a tent to keep the cerebrospinal fluid unobstructed. However, PFR did not open the arachnoid mater and the cerebrospinal fluid circulation was not improved. Clinical observation by Vanaclocha et al. [19] suggests that repair of incisions with artificial dura mater (autologous fascia) is prone to cerebrospinal fluid leakage, subcutaneous effusion, pseudomeningocele, and even intracranial infection.
Years of clinical practice have demonstrated that, during surgical treatment of Chiari malformation (type I) with syringomyelia, if a large piece of the occipital bone is removed, the contents of the posterior cranial fossa will lose bony support, leading to ptosis of cerebellum, the fourth ventricle, and nerve tissue, which induces mechanical traction to the brain stem and nerve root, resulting in new symptoms. Cisterna magna reconstruction [21] reconstructs the cisterna magna obstructed by cerebellar tonsils, and restores cerebrospinal fluid circulation. In 2004, Professor Zhang Yuqi proposed the surgical treatment with tonsillectomy plus central canal opening for Chiari malformation with syringomyelia [20, 22], which has become the most reliable surgical approach to treat the disease.
In this study, a total of 209 patients were treated by MIST and cisterna magna reconstruction, among whom 48 patients (22.97%) had complete disappearance of syrinx, 147 patients (70.33%) had obvious shrinkage, and 14 patients (9.52%) had non-obvious shrinkage. Up to 93.30% of the patients had improved symptoms after minimally invasive surgery. Analysis in previous literature showed a symptom improvement rate of 77.8% after treatment for Chiari malformation (type I) with syringomyelia [5]. It can be seen that minimally invasive surgery has significant advantages in the treatment of Chiari malformation (type I) with syringomyelia. In addition, the CCOS scores were the highest in the complete disappearance group, followed by the obvious shrinkage group, and the lowest in the non-obvious shrinkage group (P < 0.05), providing validating evidence on the efficacy study. The correlation analysis found that statistically significant (P < 0.05) negative correlations existed between disease duration and the maximum diameter reduction of syrinx, each category of CCOS score, hypoesthesia, limb weakness, muscle atrophy, and sleep apnea. Thus, disease duration is a major risk factor for the disease. Multivariate analysis also validated this result. The reconstruction of cisterna magna and the reshaping and repair of cerebellar tonsils are the aims of this approach, which can enlarge the volume of the posterior cranial fossa, especially the cisterna magna in the foramen magnum region, and normalize the brain proportion in the foramen magnum region. Compared with the surgical enlargement of posterior fossa, the approach in this study could reconstruct a normal cisterna magna while preserving as much occipital bone as possible. It effectively relieved the obstruction of the foramen magnum region, restored cerebrospinal fluid circulation, and kept the local cerebrospinal fluid circulation unobstructed. As a result, the root cause of the disease was eliminated, preventing the development and deterioration of lesions. After surgery, syrinx shrinkage, cisterna magna restoration, and relieved symptoms were observed in the patients, indicating good clinical efficacy and low clinical defect rate. Additionally, the posterior occipital incision was 2.0–3.0 cm, and the total bleeding volume was about 20–30 mL, which was notably superior to the traditional craniotomy. Besides the advantages of small surgical incision and slight tissue damage, the approach also helped to reshape and repair the malformation in the foramen magnum region. The incidence of complications in MIST group (11.01%) was higher than that in traditional posterior fossa decompression group (8.11%), P > 0.05.Therefore, based on the results of this study, we conclude that “minimally invasive subpial tonsillectomy (MIST) and cisterna magna reconstruction” is an improved surgical approach for the treatment of Chiari malformation (type I) with syringomyelia, with encouraging efficacy and few complications.
Footnotes
Acknowledgments
We thank Jun Hua Wang, Yi Ou Liu for the comments on the content of the article, and we would like to thank all participants who participated in the study for their time and involvement.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Consent to participate
All patients provided written informed consent at the time of entering this study.
Ethics approval
This work is approved by Ethics Committee of Tsinghua University Yuquan Hospital.
Declaration of conflicting interests
All contributing authors report no conflict of interests in this work.
Funding information
There is no funding support for this article.
Author contribution
Hao Li completed the collection, collation and statistics of the original data, as well as the operation, literature search and the writing of the first draft of the article. Zhiqiang Cui provided advice and guidance, and revised the first draft, Yong Liu provided the direction and ideas of the research.