
Abstract
Objective:
To analyze the instrumentation-related complications of patients with lumbar degenerative disc diseases (LDD) who underwent minimally invasive transforaminal lumbar interbody fusion (MIS- TLIF) and to discuss the potential strategy for the control of these complications.
Methods:
A total of 87 patients with LDD were treated with the MIS-TLIF procedure. Complications, including malposition or breakage of guide pin, percutaneous pedicle screw (PPS) or cages, neurological deficit, and superior-level facet joint violations, were determined during and after the surgery. Computed tomography (CT) was used to evaluate the PPS accuracy and the superior-level facet joint violations.
Results:
A total of 386 PPSs were used. During the surgery, 3 (0.8%) guide pin and 1 (0.3%) PPS perforated the anterior wall of the vertebral body, respectively. One (0.3%) PPS was pulled out during the reduction of slip. Malposition of the cages occurred in 6 (1.6%) PPSs. These were all adjusted accordingly during the surgery. All the patients received > 2 years of follow-up. No loosening or breakage of PPS and cage was observed, but CT showed 27 (7.0%) PPSs misplaced. No neurological deficit related to misplaced PPS was observed. The total facet joint violation (FJV) rate was 36.2%, with grade 2 and grade 3 violations is 21 (12.1%) and 6 (3.4%), respectively.
Conclusion:
MIS-TLIF has similar instrumentation-related complications with open TLIF. Accurate preoperative evaluation and improved surgical techniques can effectively reduce these instrumentation-related complications.
Keywords
1 Introduction
Transforaminal lumbar interbody fusion (TLIF) was initially proposed in 1982 to avoid intraoperative dural sac and nerve root traction injury [1]. Foley et al. first reported the use of minimally invasive TLIF (MIS-TLIF) to reduce intraoperative paraspinal muscle injury. The clinical outcomes of MIS-TLIF, including lower blood lost, less initial postoperative pain, less analgesic medication use, early rehabilitation, and shorter hospitalization, were confirmed in several studies [2, 3]. Some papers have reported one or two perioperative instrumentation-related complications, including misplacement or breakage of the guide pin, percutaneous pedicle screw (PPS) or cages; neurological deficit; and superior-level facet joint violations (FJV). In this study, we summarized the clinical data of 87 patients who underwent MIS-TLIF procedure for lumbar degenerative disc disease (LDD) treatment and analyzed the incidence of instrumentation-related complications and control strategy.
2 Materials and methods
2.1 General patient information
A total of 87 patients with LDD (mean age 54.2 ± 19.6 years, ranged 22–80 years); 29 males, 58 females) who had 2 years follow-up data and computed tomography (CT) images were included in this study. All patients underwent the MIS-TLIF procedure by the same spine surgeon, among whom 68 and 19 patients received single and two-level surgery, respectively. The affected levels were L3–L4 in 21 cases, L4–L5 in 57, and L5–S1 in 28. The preoperative diagnosis was lumbar spondylolisthesis in 42 patients (40 with Meyerding grade Ⅰ and 2 with grade Ⅱ spondylolisthesis), severe lumbar spinal stenosis (LSS) in 26, LSS with instability in 12, and lumbar surgery revision in 7. A total of 386 PPSs were used in this series. All the patients consented to the procedures, which were approved by the clinical research ethics committee of Qilu Hospital, Shandong University, China.
2.2 Surgical procedures
The patients were under general anesthesia and in the prone position. Briefly, the TLIF surgical procedure at the left L4–L5 is as follows: L4–L5 pedicles were marked preoperatively with fluoroscopy. After the Jamshidi needles were inserted in the bilateral L4 pedicles, their placement was confirmed by fluoroscopy examination, and they were removed to place the guide pins. The same method was used for guide pin implantation in the bilateral L5 pedicles. A skin incision (about 3 cm-long) was made between the guide pins on the left side to reach the fascia under the skin. The incision was then gradually expanded to implant the Luxor minimally invasive retractor and expose the L4–L5 facet joints. Subsequently, the facet joints and hypertrophied ligamentum flavum were removed for complete decompression.
For a patient with central LSS, the retractor was inclined to decompress the contralateral spinal canal. Then, the intervertebral discs and cartilage endplate were removed. The cage was filled with autologous bone particles, and the allogeneic bone particles were implanted into the intervertebral space. Finally, the pedicle screws were inserted along the guide pin, and the connecting rods were inserted and locked (Fig. 1).
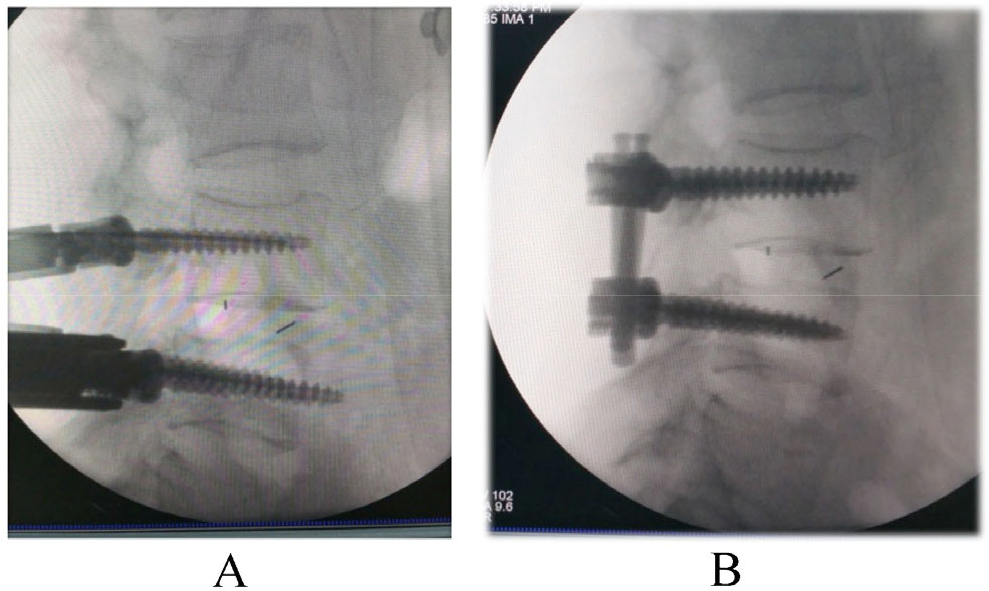
Lumbar spinal stenosis with instability at L4–L5 in a 56-year-old female patient. (A)Left pedicle screw at L5 penetrated the anterior wall. (B)The screw was adjusted during the surgery.
2.3 Observation of instrumentation-related complications
Complications were monitored during and after surgery, including malposition or breakage of guide pin, PPS or cages; neurological deficit; and superior-level FJV.
2.4 Image evaluation
CT was used to evaluate the PPS accuracy and superior-level FJV 3 months after surgery. The following screw misplacement grading systems were used to assess the screw placement accuracy [4, 5]: grade 0, no pedicle perforation; grade 1, 0–2 mm; grade 2, 2–4 mm; grade 3, 4–6 mm; grade 4, > 6 mm. The location of the pedicle wall penetrations (lateral, medial, superior, and inferior) was also recorded. Facet joint violation was classified as follows [6]: grade 0, screw not in facet; grade 1, screw in lateral facet but not in facet articulation; grade 2, penetration of facet articulation by screw; and grade 3, screw travels within facet articulation.
2.5 Statistical analyses
SPSS 12.0 statistical software (SPSS Inc., USA) was used for the statistical analyses. Unpaired t-test and χ 2 test were performed to determine the statistical significance with α level set at 0.05.
3 Results
During the surgery, 3 (0.8%) guide pins perforated the anterior wall of the vertebral body (VB). One (0.3%) PPS perforated the anterior wall of VB, and the patient experienced abdominal pain for 3 days (Fig. 1). Two PPSs (0.5%) were pulled out during the reduction of slip because of severe osteoporosis and violent manipulation (Fig. 2). Malposition of cages occurred in 6 (1.6%) PPSs, wherein 5 were too close to the spinal canal and the other was inserted into the L5 VB. These were all adjusted accordingly during the surgery. No neurological deficit caused by instrumentation was observed.
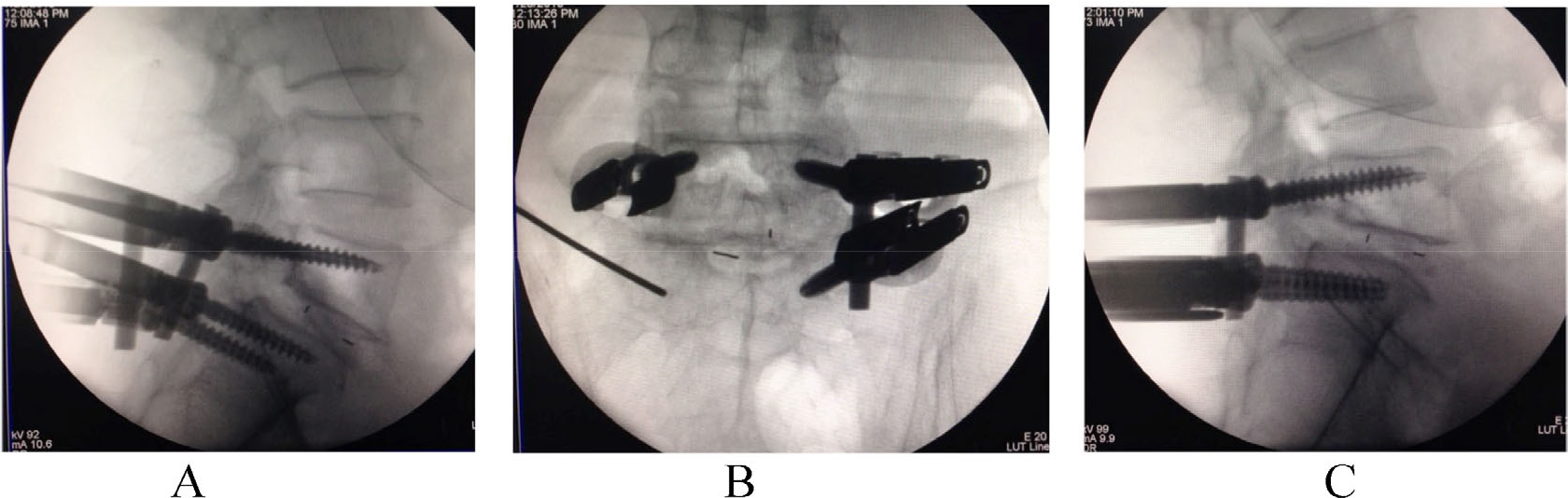
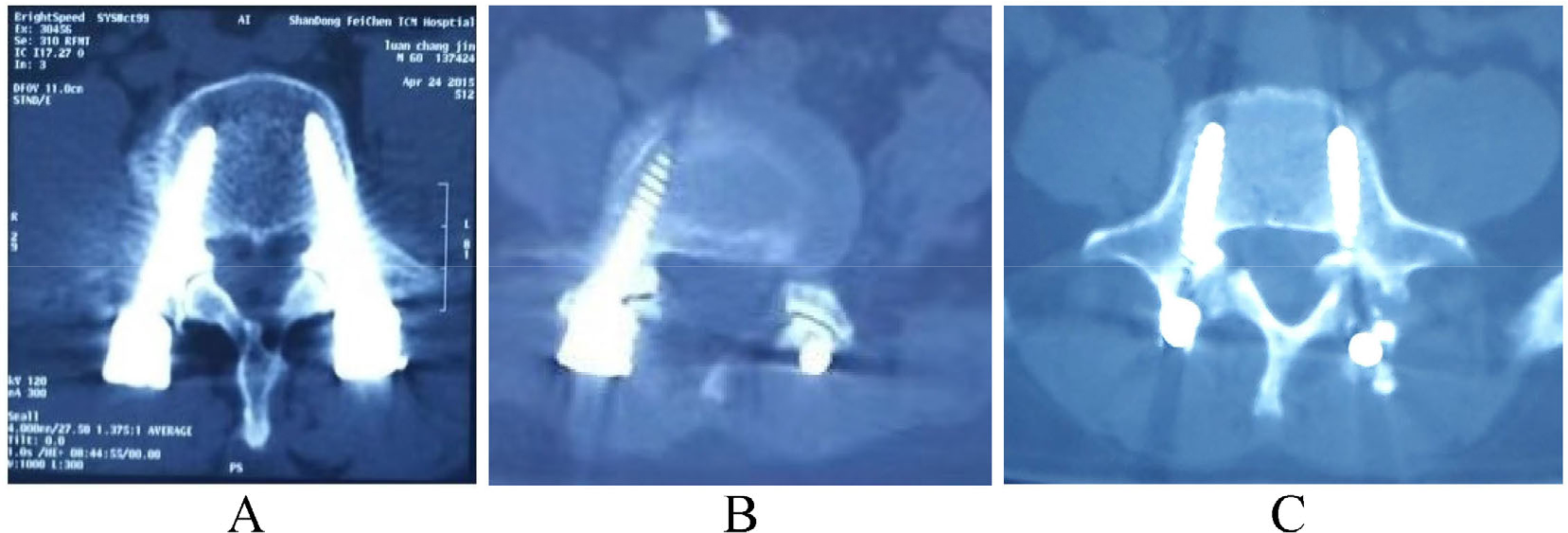
Spondlylolisthesis in a 55-year-old male patient. (A) The right S1 screw was pulled out during the process of inserting the rod. (B)The trajectory was filled with autograft bone and inserted with the guide pin. (C) The pedicle screw and rod were reinserted.
All patients received > 2 years of follow-up. No loosening or breakage of PPS or cages was observed. CT showed 27 (7.0%) misplaced PPSs, including 20 (5.2%) grade 1 screws, 4 (1.0%) grade 2 screws, 2 (0.5%) grade 3 screws, and 1 (0.3%) grade 4 screws (Fig. 3, Table 1). Eighteen PPSs (grade 1 in 15 PPSs, grade 2 in 3 PPSs) penetrated the medial pedicle cortex, and 9 PPSs (grade 1 in 5 PPSs, grade 2 in 1 PPS, grade 3 in 2 PPSs, and grade 4 in 1 PPS) penetrated the lateral pedicle cortex. Misplaced PPSs were located at L4 (13 screws), L5 (9 screws), and S1 (5 screws). The patient with 1 (0.3%) grade 4 misplaced pedicle screw, which penetrated the lateral pedicle cortex, had unilateral low back pain. No neurological deficit related to the misplaced PPSs was observed during the follow-up.
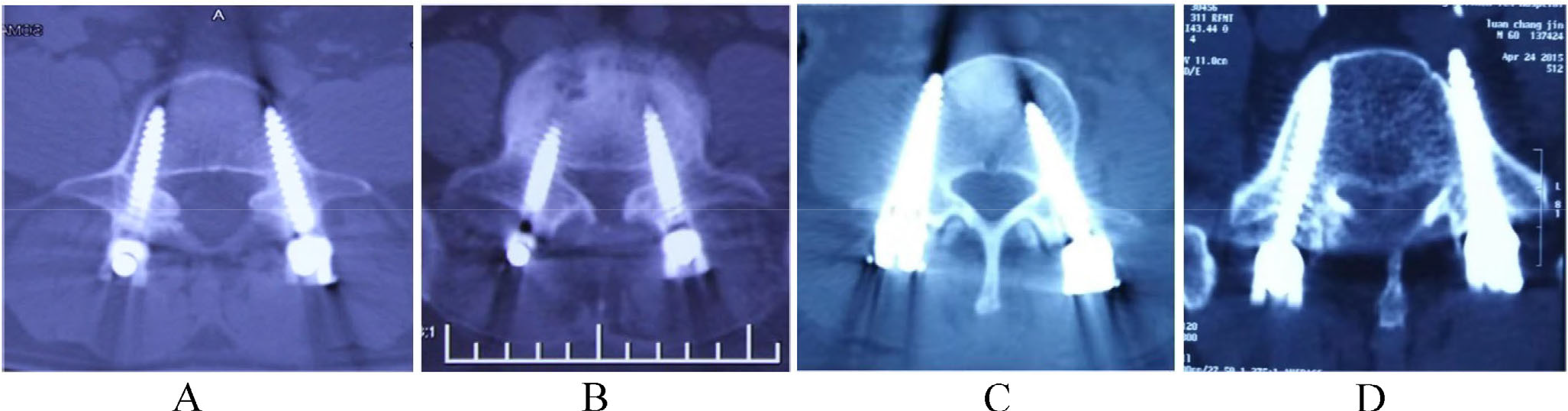
The PPS accuracy. (A) Grade 1 PPS (left). (B) Grade 2 PPS (left). (C) Grade 3 PPS (right). (D) Grade 4 PPS (left).
PPS misplacement rate.
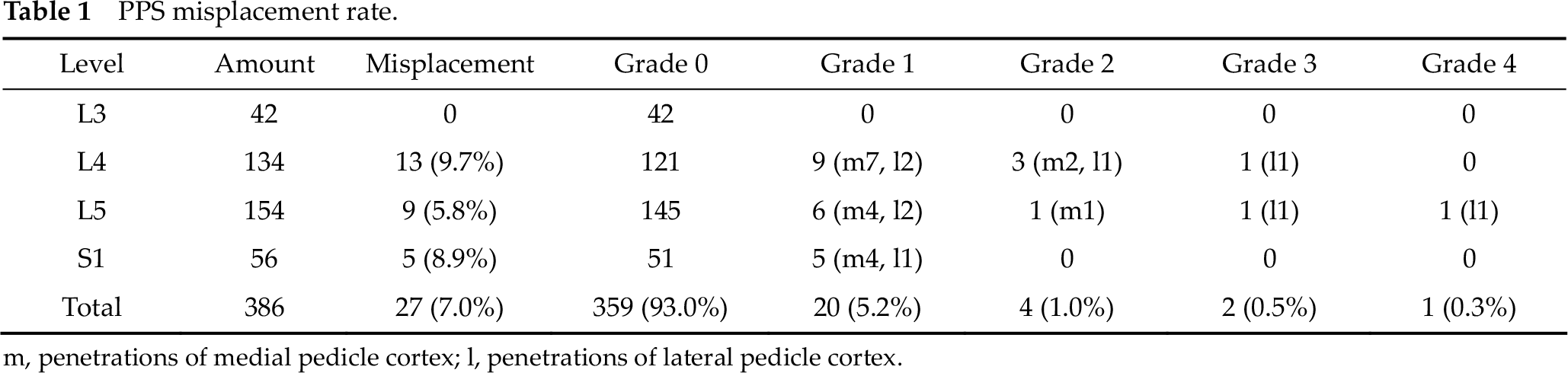
m, penetrations of medial pedicle cortex; l, penetrations of lateral pedicle cortex.
Only the screws at high position of vertebral body have possibilities of FJV, the total amount of which is 174 (42 at L3, 92 at L4, 40 at L5). The total FJV rate was 36.2%, among which grade 2 and grade 3 violation occurred in 21 cases (12.1%) and 6 cases (3.4%), respectively (Fig. 4, Table 2). The highest occurrence of FJV was at L5 in this series (P < 0.05).
FJV of PPS. (A) Grade 0 PPS (left) and grade 1 PPS (right). (B) Grade 2 PPS (right). (C) Grade 3 PPS (right).
PPS top-level FJV rate.

4 Discussion
4.1 Intraoperative complications
4.1.1 Guide pin-related complications
In this series, 3 (0.8%) guide pins perforated the anterior wall of VB, but there were no related clinical symptoms after the surgery. The guide pin perforation was mainly due to insufficient surgical experience. Osteoporosis or PPS insertion in different directions with the guide pin may cause pin perforation in the anterior wall of VB. During surgery, surgeons should maintain the PPS at the same direction with the guide pin. Moreover, during the process of pedicle screw insertion, a clamp should be used to hold the guide pin at the original position and avoid being pushed forward by the PPS. Continuous intraoperative fluoroscopy is the best way to avoid such complications for inexperienced surgeons.
4.1.2 PPS and interbody cage-related complications
One PPS perforated the anterior wall of VB leading to 3 days abdominal discomfort, but with no further complications. Two PPSs were pulled out when the surgeons tried to insert the connecting rod. One of them was pulled out during reduction of slip because of severe osteoporosis, the other was caused by violent manipulation. For these two PPSs, autograft bone was placed into the trajectory of the pedicle screws, and screws with larger diameter were used to ensure sufficient fixation strength. Nevertheless, for the former one, the reduction of slip was given up and in situ fixation was used to avoid fixation failure. For patients with advanced age (especially females) and severe osteoporosis, precise preoperative evaluation (e.g., bone density, PPS diameter, reducing the slip or not) should be considered carefully.
Malposition of cages at L5–S1 levels occurred in 6 (1.6%) PPSs. Five of them were inserted at shallow position, which can be easily adjusted, whereas the remaining cage was inserted into L5 VB. There are many reasons for the occurrence of such complications, e.g., lack of surgery experience, limited working space, size of cages, and height of interbody space. In this series, the main reason was that the sacral slope (SS) was too high in these patients, which makes it difficult to insert the cages through minimally invasive retractor in such an oblique angle. For such cases, there should be more attention to reduce the SS by adjusting the patients’ prone position before the surgery to make it easier to insert the cages. Moreover, before inserting the cages, fluoroscopy should be used to confirm the inserting position and direction, especially at the L5/S1 level.
4.2 Postoperative PPS-related complications
In this series, all patients received > 2 years of follow-up. No loosening or breakage of PPS and cages was observed. CT was used to evaluate the PPS accuracy and superior-level FJVs 3 months after the surgery.
4.2.1 Misplaced PPS
The misplacement rate of open thoracic and lumbar pedicle screws was reported as high as 42%, and neurological injury occurrence was 2%–11% [7, 8]. Wiesner reported PPS misplacement rate at 6.6%, with only 1 PPS penetration in the medial pedicle cortex that caused minor neurological deficit [4]. Oh et al. compared the accuracy of 558 open pedicle screws (OPS) with 498 PPS using CT, and the results revealed no statistical difference between the accuracy rate of OPS (13.4%) and PPS (14.3%) [9]. A relatively higher incidence of lateral penetration was observed in the OPS group (66.7% vs. 43.7%), whereas the incidence of medial, superior, and inferior penetrations was higher in the PPS group.
According to our results, PPS is a safe technique with minor complication. In this series, there were only 27 misplaced PPSs (7%), including 20 (5.2%) grade 1 screws, 4 (1.0%) grade 2 screws, 2 (0.5%) grade 3 screws, and 1 (0.3%) grade 4 screw. Misplaced PPSs were located at L4 (13 screws), L5 (9 screws), and S1 (5 screws). Consistent with the result of Oh et al., the medial cortex penetration rate was higher in the PPS group in this study. Eighteen PPSs (grade 1 in 15 PPSs, grade 2 in 3 PPSs) penetrated the medial pedicle cortex, but there were only 3 grade 2 screws, and neurological deficit associated with the misplaced PPSs was not observed during the follow-up. Nine PPSs (including 5 grade 1 PPSs, 1 grade 2 PPS, 2 grade 3 PPSs, and 1 grade 4 PPS) penetrated the lateral pedicle cortex. The patient with 1 (0.3%) grade 4 pedicle screw had persistent unilateral low back pain.
4.2.2 Facet joint violation
An important consideration in all cases with instrumented pedicle screw is to prevent the development of adjacent-segment disease by limiting injury to the adjacent-level structures, particularly the superior facet. Damage to this facet joint can contribute to the increased stress at the adjacent level, and possibly leads to radiological and symptomatic adjacent-segment stenosis, which requires additional surgery and increases medical costs [6, 8, 10, 11]. Cardoso et al. reported that a bilateral FJV in axial rotation resulted in a significant increase of range of motion (ROM) at the adjacent segments than that in the instrumented cases with intact facet joints [8]. A finite element analysis revealed that FJV owing to pedicle screws resulted in 166.7% and 132.1% increase of the facet contact force at corresponding L3–L4 under extension and torsion moments, respectively, compared with that in the intact model [10]. Shah et al. reported that FJV occurred in 30% of the patients and 20% of the screws even with the Wiltse muscle-splitting approach. Despite of taking specific intraoperative precautions (e.g., surgical approach and the pedicle entry point to avoid FJV), it was still not possible to completely avoid it [11]. Moshirfar et al. analyzed 235 open lumbar–sacrum fusion cases and reported that top-level FJV occurred in 15% of the cephalad pedicle screws and in 24% of the patients [12]. Violations occurred more frequently in the leftside single-level fusions, particularly those at L5.
There are conflicting data in the published literature regarding the effect of percutaneous insertion of pedicle screw on facet joint impingement. Babu et al. evaluated 126 open and 153 percutaneous cases and reported that percutaneous procedures had a higher overall violation grade and a greater incidence of high-grade violations than the open procedures [6]. Yson et al. compared cranial FJV rates between open and PPSs that were inserted under 3-dimensional image guidance [13]. They reported that the overall FJV rate was 18.9%, with the open technique having a remarkably higher violation rate than the percutaneous technique. There was also a trend of an increasing likelihood of FJV at the level from L1 to L5.
In this series, the total FJV rate was 36.2%, with an occurrence of 12.1% (21 cases) and 3.4% (6 cases) for grade 2 and 3 violation, respectively. Furthermore, the highest rate of FJV occurred at the level of L5. Although the starting point of PPS is at nine o’clock, it is still very difficult to completely avoid FSJ, especially at the L5 level. These may be caused by the following two reasons: (1) the anatomical variation of L5 pedicle sometimes makes it very difficult to get a clear view under fluoroscopy; and (2) the PPS cannot be inserted under direct view, and therefore, the insertion only relies on radiographic and limited tactile feedback to determine the screw entry site and trajectory. To avoid FSJ, precaution should be considered in choosing the starting point and direction and the pedicle should not be placed in too deep position.
5 Conclusion
MIS-TLIF has similar instrumentation-related complications with open TLIF. Accurate preoperative evaluation and improved surgical techniques can effectively reduce these instrumentationrelated complications.
Footnotes
Conflict of interests
The authors declare that they have no conflict of interests.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81272024).