
Abstract
There are two major research issues with regard to detoxification; one is pathological testing of drug users and the other is rehabilitation methods and techniques. Over the years, domestic and foreign researchers have done a lot of work on pathological changes in the brain and rehabilitation techniques for drug users. This article discusses the research status of these two aspects. At present, the evaluation of brain function in drug addicts is still dominated by a single electroencephalography (EEG), near-infrared spectroscopy (NIRS), or magnetic resonance imaging scan. The multimodal physiological data acquisition method based on EEG–NIRS technique is relatively advantageous for actual physiological data acquisition. The traditional drug rehabilitation method is based on medication and psychological counseling. In recent years, psychological correction (e.g., emotional ventilation, intelligent physical and mental decompression, virtual reality technique and drug addiction suppression system, sports training, and rehabilitation) and physical therapy (transcranial magnetic stimulation) have gradually spread. These rehabilitations focus on comprehensive treatment from the psychological and physical aspects. In recent years, new intervention ideas such as brain–computer interface technique have been continuously proposed. In this review, we have introduced multimodal brain function detection and rehabilitation intervention, which have theoretical and practical significance in drug rehabilitation research.
Keywords
1 Introduction
Drug abuse has been considered as a global public hazard due to its serious impact on national security, social harmony, family stability, and personal health. In the European Union, for example, 250 million individuals aged 15–64 years or 5 out of every 100 adults have used one or more drugs and have spent > 24 billion euros per year on these drugs. On June 17, 2019, the Office of China National Narcotics Control Commission issued the “2018 China Drug Situation Report”, which states that by the end of 2018, there were a total of 2.404 million drug users in China: 1.35 million methamphetamine abusers, accounting for 56.1%; 889,000 heroin abusers, accounting for 37%; 63,000 ketamine abusers, accounting for 2.6%; and 24,000 cannabis abusers, accounting for 1.77%, with an increase of 25.1% every year. Methamphetamine use has exceeded heroin use, thus becoming the most abused drug in our country. There is an increasing trend of abuse among foreigners, entertainers in the entertainment circle, and those who have had overseas study or work experiences. Drug control has a long way to go; local and international researchers in the field of drug treatment have been continuously exploring this aspect and trials using new pathological detection and withdrawal rehabilitation techniques have begun.
From the perspective of drug addiction pathology, Volkow et al. proposed the brain neural circuit, cognitive behavior control circuit, reward circuit, etc., which are closely related to addictive behavior [1]. When the nerve cells of the brain circuit are activated by addictive substances, more dopamine is acquired in different brain regions. When an addicted individual continuously uses addictive drugs, the dopamine concentration in the brain increases with time. The reward circuit’s enhancement of dopamine is correspondingly weakens, triggering the increase in drug dosage. A study on the mechanism of emotional regulation defects reported that despite the negative consequences brought about by a series of drug use, addicted individuals frequently use drugs in large quantities [2]. Wikler, who proposed the drug motivation model in 1948, pointed out that the main motivation for drug use is negative reinforcement [3] and that addicted individuals take drugs to avoid aversion, such as reducing stress. Stress and negative emotions from non‐drug sources increase relapse and rapid craving for drugs [4]. Moreover, drugs have proven to reduce stress [5]. Baker et al. [2] proposed an affective processing model of negative reinforcement; this is a reformulation model of negative reinforcement of drug addiction. They believed that the characteristics of addiction reflect the motivational effects of negative reinforcement and tried to elucidate the characteristics of addiction through the formation of negative reinforcement. They concluded that the main motivation for drug addiction is avoidance of negative emotions. In developed countries such as Europe and the United States, education programs have been established at primary schools and secondary schools as well as universities for conventional prevention of drug abuse. In Britain, a drug rehabilitation system has been established. In Germany, the measures involving detoxification and rehabilitation have been establishes.
In China, Professor Chenglin Zhou and his team focus on research on drug rehabilitation through sports, including joint exercise, basketball, free‐weight training, half squat, push‐up, supine leg bending, prone back flight, aerobic endurance training, and jogging and, finally, relaxation activities. At the same time, it also improves rehabilitation exercises, including Tai Chi and eight‐section brocade, thus slightly improving the physical quality and brain function of drug addicts [6, 7]. According to Min Zhao, a professor from Shanghai Mental Health Center, the research content includes exploration of new methods on the abuse and rehabilitation of psychoactive prescription drugs and the proposed cue task method has achieved some results in the rehabilitation of heroin addicts [8 –10]. The National Institute on Drug Dependence at Peking University focuses on the key scientific problem of “biological mechanism of addiction,” from the micro, mesoscopic, and macro levels of the brain to different research scales in the population; it also explores the pathological memory mechanism of addiction and its intervention strategies to examine the biological mechanism of addiction and relapse, identify its biological markers, and reveal the molecular and loop mechanisms of addiction‐related diseases. Studies have also attempted to improve drug addicts’ attention and self‐control through brain wave mindfulness technique [11 –13].
Pathological studies of drug addiction have been conducted for many years locally and internationally and great progress has been made, which also benefited from the improvement of new detection technologies. Through deepening the understanding of the pathology of drug users, good rehabilitation methods have been continuously proposed. New detection techniques and rehabilitation methods are of great significance in the detoxification and recovery of drug addicts. This article mainly introduces the cutting‐edge technologies and methods in the current detoxification research from the aspects of electroencephalography (EEG) – near‐infrared spectroscopy (NIRS) multimodal brain function detection and rehabilitation intervention combined with NIRS.
2 New techniques of combined pathological detection with EEG–NIRS
2.1 Feasibility analysis of multimodal physiological index detection with EEG–NIRS
Among research conducted on the detection of pathological indexes of drug addicts, EEG, magnetic resonance imaging (MRI), and positron emission tomography (PET) have precedents for the practical application of drug addicts. EEG is portable, real‐time, and has better time resolution. It mainly records the spontaneous bioelectrical activities of human brain neurons. It is also based on this principle that changes in the EEG findings of drug addicts are detected, thus reflecting the changes in their brain functions. However, a single EEG scan is not enough to detect the changes in their brain functions and cannot expose the brain of drug addicts very well. MRI and PET have better spatial resolution and can be used to detect brain blood oxygen‐dependent levels and blood perfusion, respectively; but they are expensive, require high experimental environment, and need special medical staff to operate. Therefore, there is a need for a technique with a type of acquisition method that is real‐time, portable, easy to operate, and able to reflect the brain functional characteristics and imaging.
In recent years, the emerging NIRS has become an effective technique in measuring the functional activities of the brain [14]. It takes advantage of the specific absorption of oxy‐hemoglobin and deoxyhemoglobin in human blood in 600–800 nm of near‐infrared light, whereas other biological tissues in the brain are relatively transparent in this wavelength range. To measure the changes in near‐infrared light intensity of 650 and 760 nm incidents into the brain tissue, brain hemodynamic data was obtained through Beer–Lambert’s law on conversion and changes in brain functional activity were indirectly obtained [15, 16]. The application of NIRS provides a new approach for determining brain function and a new idea for pathologically detecting drug users.
In view of the portability and better time resolution of EEG and NIRS brain function detection in terms of brain function activity and structure, the EEG–NIRS synchronization technique provides more comprehensive information, which can significantly improve the accuracy of neural signal detection. A combination of NIRS and EEG to achieve simultaneous detection can record the changes in brain activity very well. In cognitive research, Wallois et al. demonstrated in language learning experiments that the information collected by the EEG–NIRS synchronization technique can effectively bypass misleading information caused by the spontaneous signal of NIRS and allow a better understanding of the brain’s activation mechanism [17]. In the field of clinical application, currently, researchers have used the combination of NIRS and EEG in the analysis of brain functional diseases and cognition, such epilepsy [18, 19]; recovery assessment of patients with stroke [20, 21]; and real‐time monitoring of anesthesia during surgery. The EEG–NIRS synchronization technique uses the respective advantages of EEG and NIRS. The synchronization of these two devices can completely explain the functional activities of the brain and provide new ideas for pathological testing of detoxification. However, this detection method has its own limitations. It can only detect the surface activity signal of brain, which cannot keep up with the highly accurate imaging of the brain by MRI and PET. In the future, other techniques combining MRI or PET should be explored. The specific detection method of EEG–NIRS and the preliminary analysis of the system will be described in detail below.
2.2 EEG–NIRS hardware and synchronous acquisition method
The EEG acquisition device introduced here uses a 64‐electrode EEG acquisition device obtained from Neuracle Lifesciences Pvt. Ltd., and the NIRS synchronous acquisition device uses the NIRSIT device obtained from OBELAB Inc., Korea. The EEG electrodes are placed according to the international 10–20 system, and the sampling rate is set to 1000 Hz. In order to ensure appropriate signal quality of the brain electrodes, the impedance is set at < 5 kΩ. In the present study, 48 channels of EEG were selected based on the actual needs and the other parameters used were as follows: NIRSIT light source type, dual wavelength Vertical‐Cavity Surface‐Emitting Laser; technical spectrum, continuous‐wave; wave length, 780 and 850 nm; spatial resolution, 4 mm × 4 mm; sampling rate, 8.13 Hz; number of light sources, 24; and number of detectors, 32. The NIRS system used for the experiment is a functional NIRS device with a total of 204 channels [23] capable of measuring signals from four source–detector separations of 15, 21.2, 30, and 33.5 mm, while allowing measurement of changes in hemo‐dynamic response at different depths [22].
Multimodal detection is particularly common in the study of human brain function and can significantly improve the detection accuracy of neural signals. The combination of NIRS and EEG in achieving simultaneous detection is gaining increasing attention. Both EEG and NIRS record signals through scalp positioning, thus allowing easy integration of the two noninvasive recording processes of the brain activity and evaluation of the brain function in drug users. EEG can capture the time‐domain changes in EEG activity, whereas NIRS relies on the spectral measurement method to quantitatively analyze the blood oxygen metabolism level of brain tissues [24, 25]. EEG combined with NIRS as a multimodal integration tool explains the integration of EEG and cerebral hemodynamics. In addition, the EEG and NIRS measuring devices are small and movable and the measuring process is noninvasive and nonradioactive. To some extent, they can replace the traditional biochemical test or imaging diagnosis method [26 –28]. Fig. 1 depicts the EEG–NIRS device wearing method for acquisition equipment.
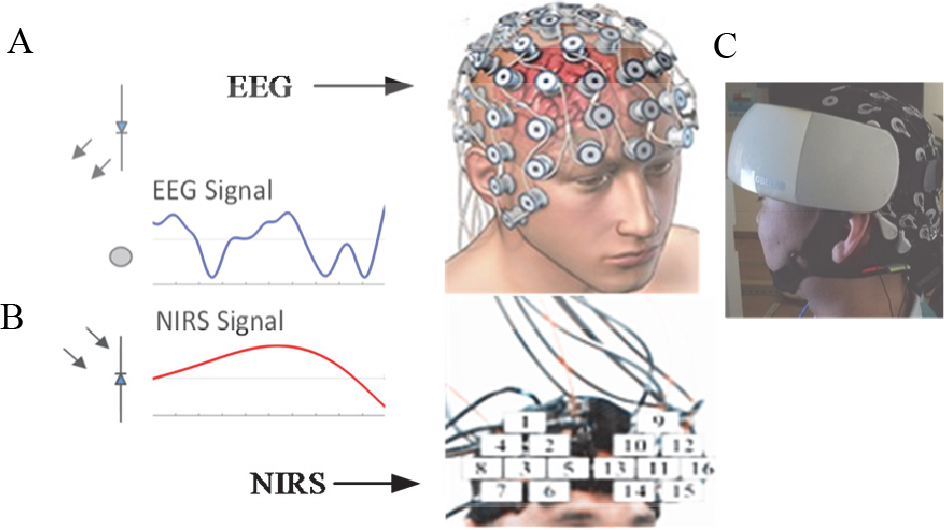
Device wearing method of physiological data collection equipment. (A) and (B) display the EEG device wearing and NIRS equipment. (C) Simultaneous wearable monitoring method for EEG and NIRS devices.
2.3 NIRS functional area division
Fig. 2 shows the division of NIRS channels and functional areas. The four high‐level functional areas detected by the forehead near‐infrared equipment are divided into dorsolateral prefrontal cortex, ventrolateral prefrontal cortex, frontal polar prefrontal cortex, and orbital prefrontal cortex. The blue area on the right side of the right dorsolateral prefrontal cortex was identified as channels 1, 2, 3, 5, 6, 11, 17, and 18. The blue area on the left side of the left dorsolateral prefrontal lobe was identified as channels 19, 20, 33, 34, 35, 38, 39, and 43. Channels 4, 9, 10, 40, 44, and 45 were marked green in the ventrolateral prefrontal cortex of the left and right hemispheres. In the left and right hemispheres, channels 14, 15, 16, 29, 30, 31, 32, 46, 47, and 48 were identified as gray areas. The yellow area of frontopolar prefrontal cortex was identified as channels 7, 8, 12, 13, 21, 22, 23, 24, 25, 26, 27, 28, 36, 37, 41, and 42.
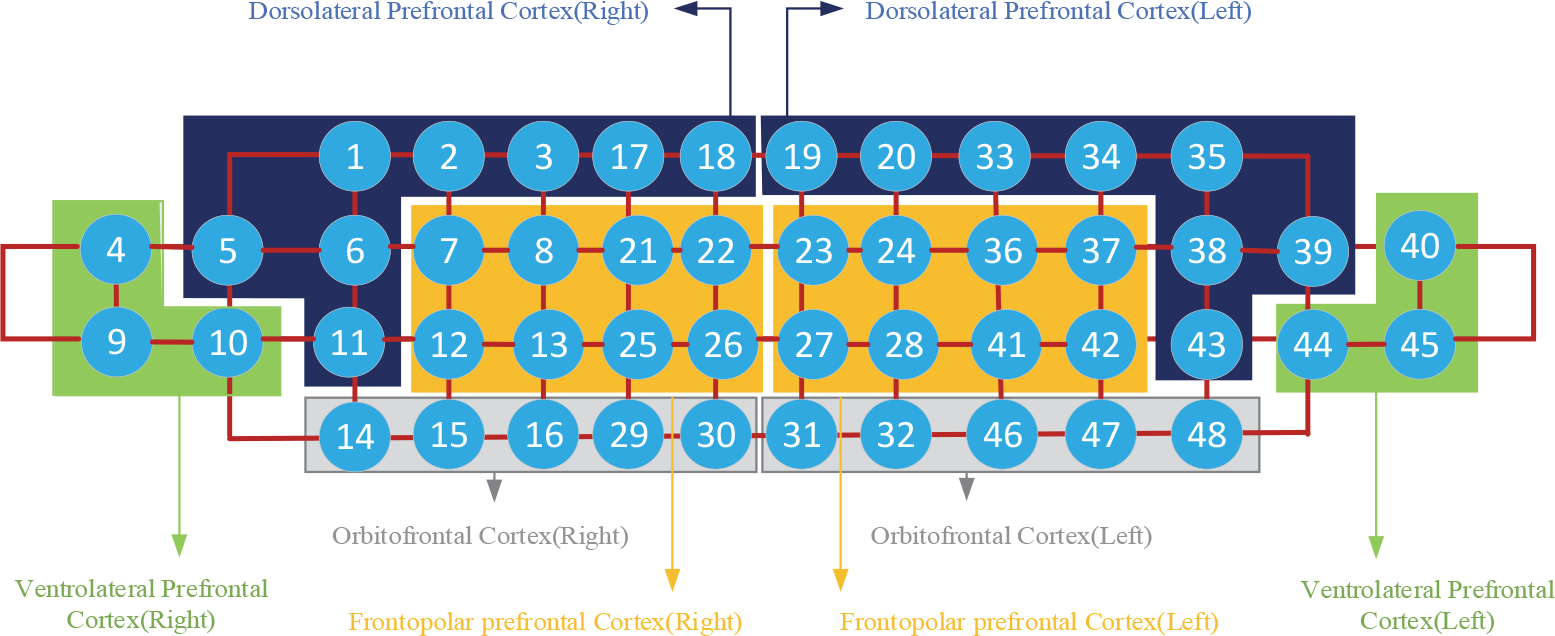
NIRS channel and functional area division.
2.4 Introduction to EEG in drug addicts and healthy people
The typical experimental methods and procedures are described as follows. The subjects were a 31‐year‐old male drug user from Shanghai Qingdong Drug Rehabilitation Center addicted to methamphetamine with frequent use of drugs (average measurement was 0.6 g/day) and a drug history of 13 years; and a 26‐year‐old male graduate student from Shanghai University who was healthy and had no history of drug abuse.
The EEG–NIRS combination was used for the actual testing of drug users. For the 31‐year‐old male drug user, the average medication dose was approximately 0.6 g/day and the average duration of drug use was > 13 years. EEG mainly analyzed the changes in EEG amplitude induced by drug addicts when they participated in the experiment, which was based on the data collected by the established experimental paradigm. The first stage of the experimental paradigm was to enter the resting state for 10 min. The second stage was the task state that lasted for 6 min. The subject was made to watch some pictures of two categories—drug pictures and neutral pictures. The third stage took 4.6 min, wherein only neutral pictures were shown to the subject. As shown in Fig. 3, #1 neutral2 (blue waveform) shows the EEG amplitudes induced by the neutral pictures shown to subjects in the experimental paradigm; #2 neutral (red waveform) shows the EEG amplitudes induced by the pictures shown to subjects during the second stage of the experimental paradigm; #3 positive (black waveform) shows the EEG amplitudes induced by the drug pictures in the second stage.
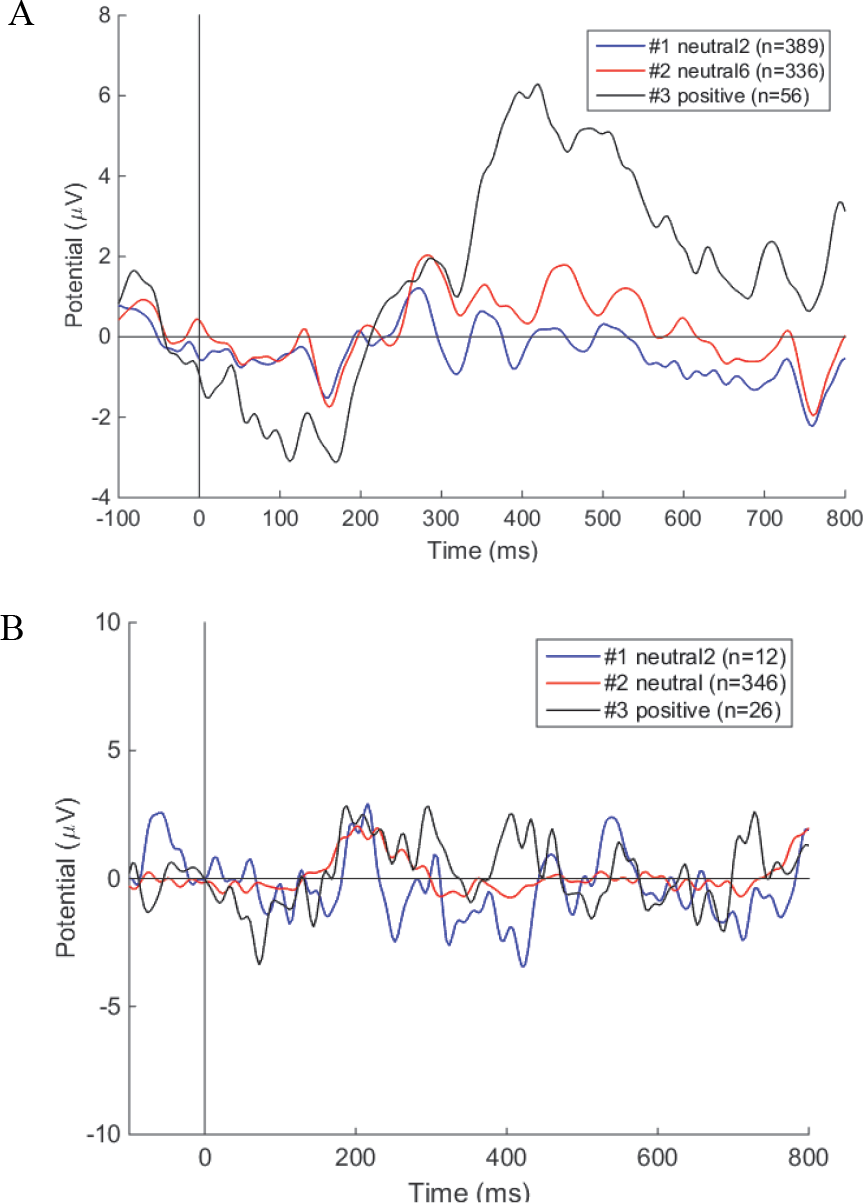
EEG amplitude changes in drug addicts (A) and healthy individuals (B). In drug addicts, drug pictures induced higher wave amplitudes on the positive axis and a larger negative value on the negative axis in EEG waveform. In healthy individuals, the EEG display tends to be stable.
Fig. 3 (A) shows that drug users were very sensitive and excited to drug pictures and that they induced higher EEG amplitudes on the positive axis, with a larger negative value. Fig. 3 (B) shows the results in healthy individuals, wherein no difference was identified in the brain wave amplitude induced by a drug picture and neutral picture. Healthy individuals are not addicted to drugs and are therefore not be excited on seeing a drug picture, whereas drug addicts are excited on seeing the drug picture because of their inner desire for drug addiction. This also proves that the wave amplitude of drug addicts on seeing drug pictures is significantly different from that on seeing neutral pictures, thus indirectly proving the change in brain function in drug addicts as well.
2.5 Introduction of NIRS in drug rehabilitation
The prefrontal cortex is a high‐level functional area of the brain. Damage to the prefrontal functional area can cause unpredictable effects on working memory, cognitive control, and mood. Some researchers have found that the dorsal lateral prefrontal cortex exhibits low activation in methamphetamine abusers and that there are defects in normal choice cognition and target motivation behavior [29]. Dieler et al. found that compared with neutral or positive emotional content, negative emotional content can significantly activate the right dorsal lateral prefrontal region and the right ventral lateral prefrontal region [30]. The prefrontal activation of long‐term drug abuse also changed. In Fig. 4, NIRS brain functional imaging shows the plain view and three‐dimensional view, which is based on the analysis of the data collected by the experimental paradigm that has been set. The experimental paradigm of NIRS data acquisition and EEG acquisition is the same. This is a synchronous acquisition method of EEG and NIRS.
Under the same experimental paradigm, changes in NIRS findings were obtained. At the moment in Fig. 4 (A), the dorsal lateral prefrontal cortex and ventral lateral prefrontal cortex of drug addicts were less activated. In Fig. 4 (B), the dorsal lateral prefrontal cortex, ventral lateral prefrontal cortex, frontal polar prefrontal cortex, and orbitofrontal cortex were less activated. The low activation of these prefrontal cortical functional areas validated the changes in cognition and control, mood, and other aspects of drug users. The prefrontal cortex of healthy individuals did not show such low activation [Fig. 4 (D)–(F)].
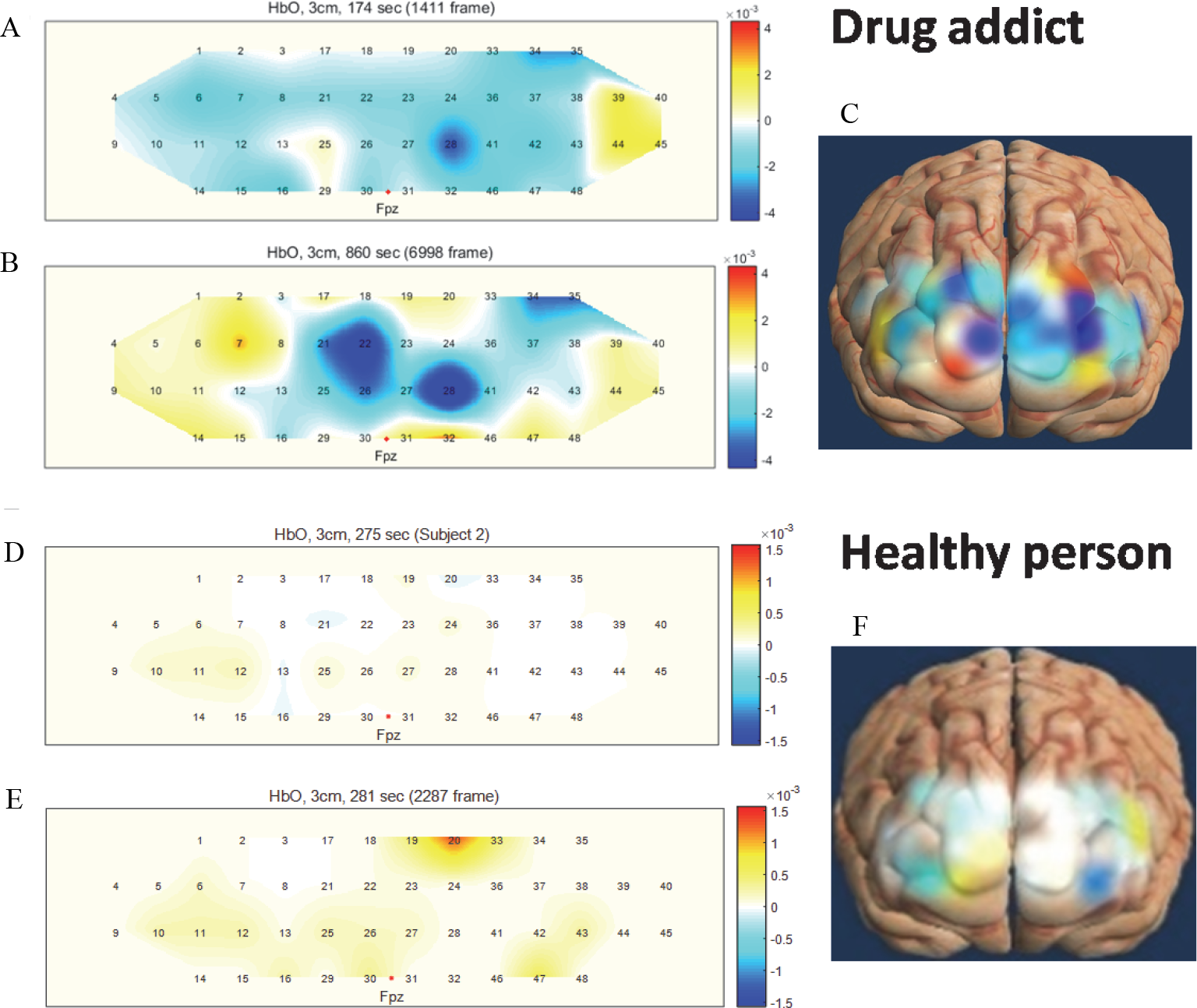
Near‐infrared brain functional imaging in drug addicts and healthy individuals. (A) and (D) changes in hemoglobin concentration, randomly selected within 10 min of the first stage to display. (B) and (E) changes in hemoglobin concentration, randomly selected within 6 min of the second stage. (C) and (F) three‐dimensional display of changes in hemoglobin concentration. The selected time is any time within 2 min after the end of the experimental paradigm.
3 Existing rehabilitation methods and new rehabilitation technologies
3.1 Drug intervention
The euphoria of drug addicts and the discomfort induced by drug withdrawal cause mental and physical dependence. Once drug withdrawal occurs, negative emotions, such as pessimism, irritability, hostility, and hallucination, increase. It then prompts drug users seeking drugs to quickly improve their mental state. Drug intervention is more common in heroin drug addiction. Heroin addicts yawn, cry, shed tears, and refuse to eat and drink water once they stop taking drugs. In severe cases, they will experience cold sweats and trembling and have difficulty in sleeping. Methadone is currently the most common and effective relieving drug for heroin addicts. It is an essential auxiliary drug after heroin withdrawal. It has analgesic effects and can produce respiratory depression, pupil shrinkage, sedation, and other characteristics. It cannot be used for a long time period because it can result in dependence.
3.2 Psychological intervention
The psychological rehabilitation intervention in drug addicts includes: (1) psychological treatment technologies, such as interactive strike vent module, interactive shout vent module, intelligent physical and mental decompression cabin, and virtual reality (VR) technique; and (2) physical exercise, which is scientific exercise training. These rehabilitation techniques are popular in China and other countries.
3.2.1 Interactive strike vent module
For drug users, especially those who try to quit drug use forcibly for the first time, the changes in the surrounding environment and living patterns are likely to produce emergency symptoms of emotional anxiety and depression, and their emotions become unstable. The unbalanced psychology will be seriously distorted in long‐term depression and will cause adverse consequences. The strike vent system showed in Fig. 5 allows the addicts to release bad emotions and relieve psychological pressure by beating. This accounts for 2 years in isolation.

Strike vent system.
3.2.2 Interactive shout vent module
The interactive shout vent module (Fig. 6) is a type of setting to release emotions. Drug addicts use this approach to release their negative emotions, thus improve their mood. This system adopts the mode of passing through different barriers, which is interesting and interactive. After a long‐term drug abuse, drug users will experience large emotional changes showing irritability, anxiety, depression, sadness, and despair. For the first time, drug users in the drug rehabilitation center will develop emergency depression and anxiety symptoms; they can better relieve stress and negative emotional effects through this approach.

Interactive shout vent module.
3.2.3 Intelligent physical and mental decompression cabin
The intelligent physical and mental decompression system (Fig. 7) will generate a decompression plan according to the personal situation of each drug user. Music relaxation hypnosis and other methods enable students to relieve fatigue and emotional and psychological pressure as well as relax psychological, physical, and physiological synchronization. Drug addicts are more anxious in an enclosed environment. The intelligent physical and mental decompression cabin guides deep sleep and allows drug addicts to relax completely, achieve decompression, and regulate mental state.

Intelligent physical and mental decompression cabin.
3.2.4 VR technique drug addiction suppression system
The VR approach can build a three‐dimensional virtual environment that integrates sight, hearing, and touch through computers. The immersive, interactive, and conceptual features of this technique are potential advantages in the treatment of addiction [31]. At present, VR is widely used, especially in the area of entertainment, given that its immersive effect has a strong impact of space and reality. The VR drug addiction inhibition system shown in Fig. 8 creates a near‐real drug use environment for drug users. By restoring the real crowd and drug use scene, drug users can immerse themselves into the virtual environment to generate a strong psychological desire. When the video is played, pictures of the damage experienced by drug users are added, which will make the drug users feel disgusted and eventually regretful. This is a disgusting therapy constructed by the VR technique. This method makes use of the aversive conditioned reflex by combining the target behavior of drug addiction that needs to be quit with unpleasant or punitive stimulation and finally achieve the quitting or reducing of the target behavior.

Virtual reality drug addiction suppression system.
3.2.5 Exercise training for detoxification
Some researchers found that aerobic exercise can improve depression, anxiety, and other symptoms in drug addicts [32]. Others found that aerobic exercise of moderate intensity reduces cravings for a short term [33, 34]. Therefore, it can be noted that scientific movements are helpful in suppressing drug addiction and improving moods. Under the advocacy of the Chinese government, sports training for drug detoxification has been extensively conducted. Two aspects are considered in sports detoxification. First, during the period of drug rehabilitation, the living environment of drug addicts is enclosed and the lifestyle is single; through sports, the physical function and mental state of drug addicts are improved. Second, the dependence on drugs has weakened the self‐control and perseverance ability of drug addicts, and they hope to build up their self‐confidence during drug rehabilitation through doing sports. Some researchers have developed sports rehabilitation exercises, such as Tai Chi and eight‐section brocade, and have achieved good results [35 –37]. Fig. 9 shows that sports rehabilitation exercise is a necessary sports training course at Shanghai Qingdong Drug Rehabilitation Center, which has a positive effect on improving physical quality and regulating mood.
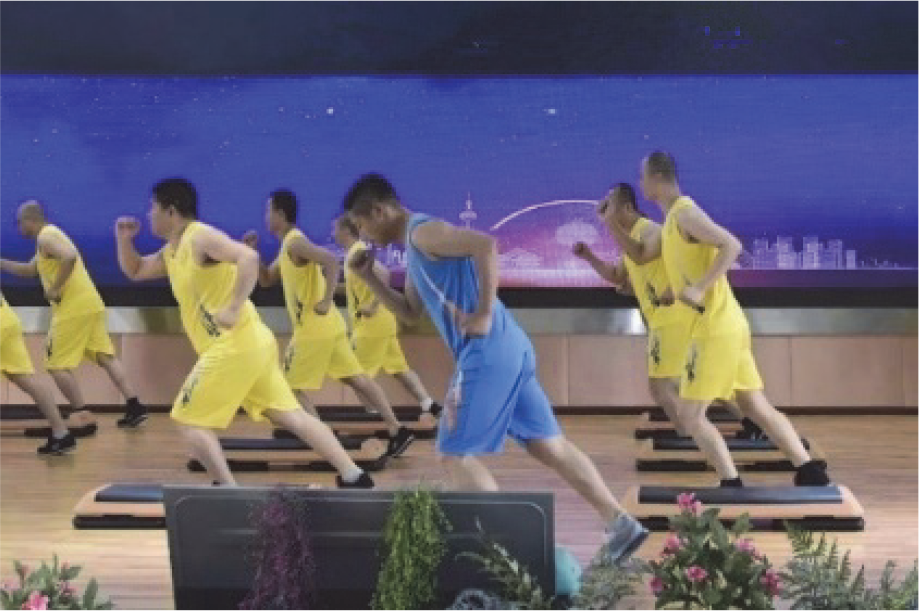
Exercise training.
The above psychological interventions are mainly used to improve mental disorders and psychological problems in drug users. At present, the physical treatment method used in drug treatment is the transcranial magnetic technique, which has been tested by some researchers in drug treatment. At the same time, considering the safety hazards of human trials, there are only few applications.
3.3 Physical therapy
Transcranial magnetic stimulation (TMS) is the current method of physical therapy. It is a new type of electrophysiological technique that acts on the cerebral cortex by generating potential actions through electromagnetic fields, thereby generating excitatory or inhibitory effects on cerebral cortical functions. Magnetic signals can stimulate the nerves of the brain through the skull without attenuation. The magnetic field is used to stimulate the left dorsal lateral prefrontal cortex functional area, thereby relieving drug users’ excitement of drugs, reducing the degree of craving, and achieving the purpose of treatment. It has been used for various disorders such as epilepsy, depression, schizophrenia, rehabilitation, cerebral palsy. This method can reduce drug craving in a short time. Fig. 10 shows the application setting of TMS. A small number of individuals at the drug rehabilitation facility in Shanghai have been treated with this method.
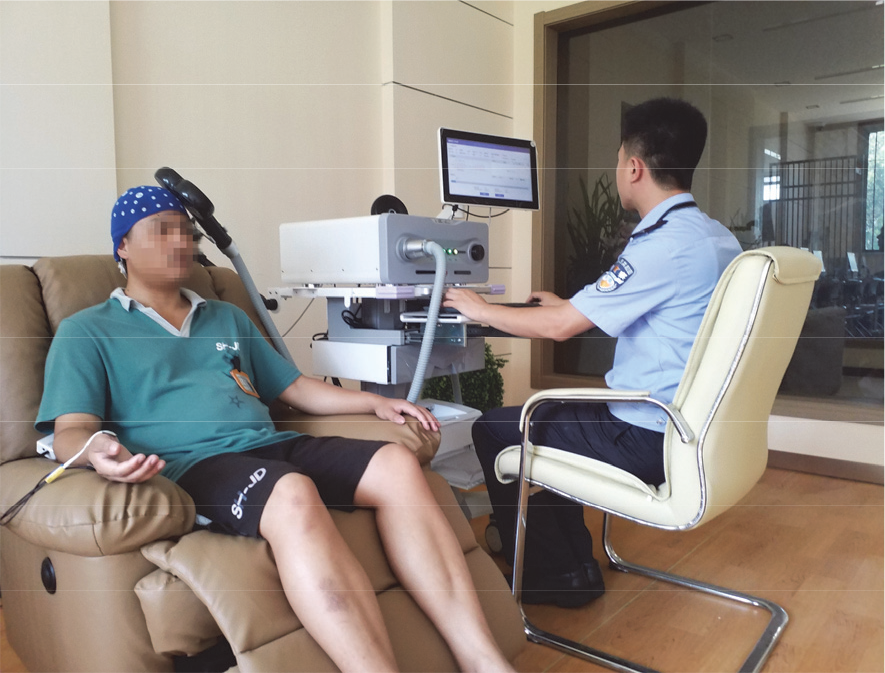
Transcranial magnetic stimulation technique application.
3.4 Brain–computer interface (BCI) rehabilitation technique
In terms of self‐control and attention training in drug users, there are no researchers on the market to develop and practice drug detoxification. In psychology, self‐confidence is mainly established through mindfulness and psychological consultation, lacking of objective and effective self‐control training methods. The BCI technique is theoretically a direct communication and control channel established between the human brain and a computer or other electronic devices. Through BCI, humans can express ideas or manipulate devices directly through the brain. Some scholars have monitored the decrease in alpha rhythm and the increase in beta rhythm in heroin addicts within early withdrawal [38 –40]. According to the situation of drug addicts, the training system of BCI can be used to improve the changes in brain function and can simultaneously help in improving attention and self‐control. Some researchers have reviewed the characteristics and application of the BCI technique, including the EEG signal processing technique, and sports imagination training, such as for stroke, which play a role in rehabilitation [41, 42]. Therefore, BCI is also a potential attempt in drug treatment.
The rehabilitation system scheme of BCI shown in Fig. 11 includes the addiction assessment module (First), brain electrical activity imagination modeling (Second), and closed‐loop feedback training module (Third). The addiction assessment module includes NIRS data collection (module 1) using portable NIRSIT. According to the experimental paradigm, the addicts are divided into three categories to collect NIRS data—mild, moderate, and severe. The NIRS data is transmitted to the VR training model (module 3) in EEG motor imagination modeling (Second), and the training model (module 3) is selected according to the degree of addiction. EEG motor imaging modeling (Second) includes motor imaging relationship modeling (module 2) and the VR training model (module 3). Modeling of motor imagination relationship 2 includes realizing EEG preprocessing; feature extraction; classification of convolutional neural network; and identifying left‐hand, right‐hand, and two‐foot motion imagination tasks and converting them into corresponding control commands (turn left, turn right, forward) to control the operation of mountaineering racing in the model designed by VR. The closed‐loop feedback training module (Third) includes real‐time collection of drug addicts in the game control EEG information displayed on the PC, real‐time feedback of the data changes on the PC whether the game control is correct, and reminder to focus on the movement of imagination. The idea is to screen individuals with different levels of addiction and design VR control games with different levels of difficulty according to different levels of addiction. With this approach, the self‐control ability of drug addicts is trained and the drug rejection ability is improved. The BCI rehabilitation technique is a new rehabilitation program. Although there is no mature application case in drug treatment, it has been applied in the rehabilitation of nervous system diseases, such as stroke and mental depression. Drug addiction is also a brain disease that provides a new rehabilitation idea for the exploration of drug rehabilitation and will be tested further.
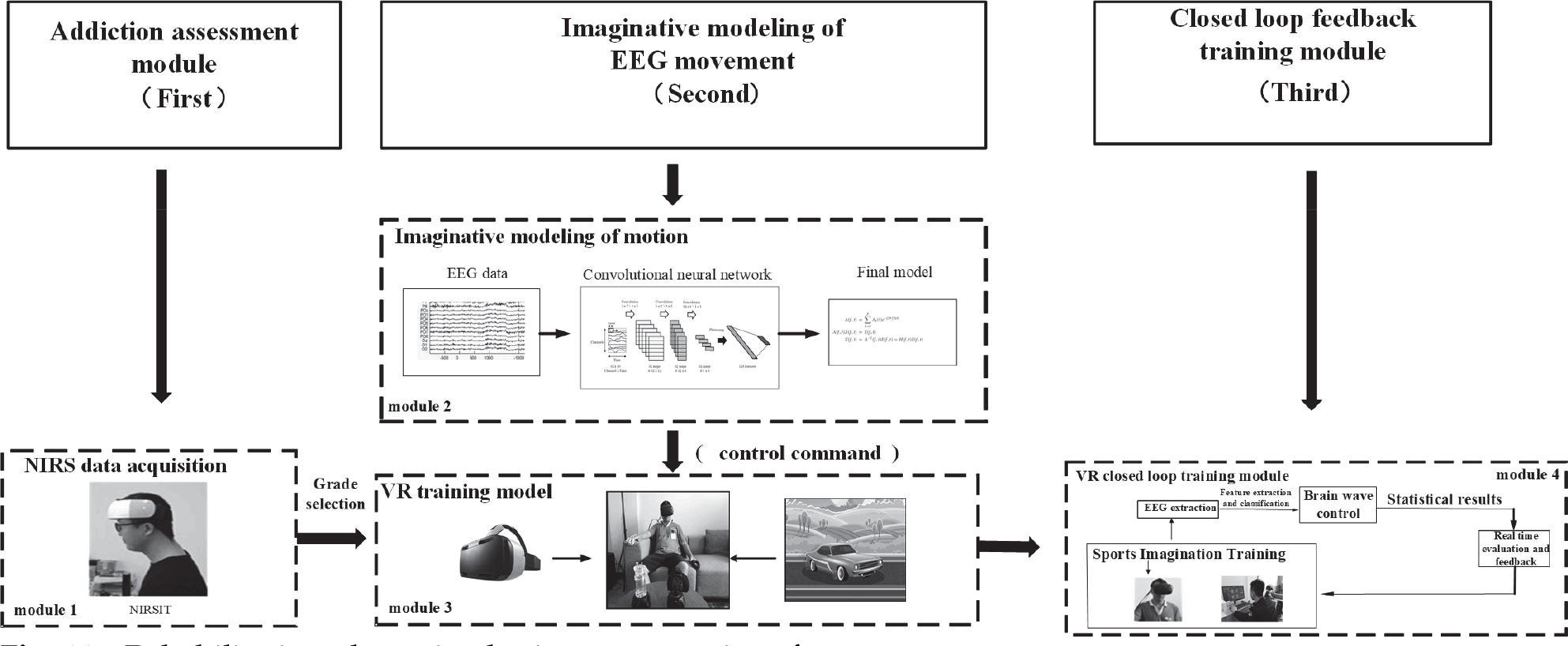
Rehabilitation plan using brain–computer interface.
4 Conclusions
The problem of drug abuse has not been fundamentally curbed worldwide, including China. Drug rehabilitation research is related to the physical and mental health, national security, and social stability of drug addicts. Effective physiological detection technique and rehabilitation methods have far‐reaching significance for scientific drug rehabilitation. Rehabilitation is the most important measure for drug addicts. New rehabilitation theories and methods need researchers to participate in the daily management of drug rehabilitation centers to solve the problems of rehabilitation training. This paper introduces the new technique of noninvasive multimodal brain function detection combined with EEG and NIRS, which has played better roles in the practical application of drug rehabilitation.
In terms of rehabilitation methods, the current rehabilitation technique is introduced in terms of three aspects: drug treatment, psychological intervention, and physical therapy. Among them, the intelligent physical and mental decompression system, emotional ventilation, VR technique addiction inhibition system, and scientific sports training have been well applied in the current rehabilitation system. The new rehabilitation technique based on BCI is currently at the discussion stage and the proposed method will also bring new hope for drug rehabilitation training.
Footnotes
Conflict of interests
All contributing authors declare no conflict of interests.
Financial supports
This project was supported by Key Research & Development Project of National Science and Technique Ministry of China (No. 2018YFC‐ 0807405, No. 2018YFC1312903), National Defense Basic Scientific Research Program of China (No. JCKY2017413C002), National Natural Science Foundation of China (No. 61976133) and 111 Project (No. D18003) and Scientific Research Project of Theoretical Research on Drug Rehabilitation of Judicial Administration of the People's Republic of China (No. 19ZD03).
Acknowledgements
The authors thank the Shanghai Drug Rehabilitation Administration and Shanghai Qingdong Drug Rehabilitation Center for their support, and all the people who contribute to the writing of the article.