
Abstract
This paper focuses on the social function of painful experience as revealed by recent studies on social decision-making. Observing others suffering from physical pain evokes empathic reactions that can lead to prosocial behavior (e.g., helping others at a cost to oneself), which might be regarded as the social value of pain derived from evolution. Feelings of guilt may also be elicited when one takes responsibility for another’s pain. These social emotions play a significant role in various cognitive processes and may affect behavioral preferences. In addition, the influence of others’ pain on decision-making is highly sensitive to social context. Combining neuroimaging techniques with a novel decision paradigm, we found that when asking participants to trade-off personal benefits against providing help to other people, verbally describing the causal relationship between their decision and other people’s pain (i.e., framing) significantly changed participants’ preferences. This social framing effect was associated with neural activation in the temporoparietal junction (TPJ), which is a brain area that is important in social cognition and in social emotions. Further, transcranial direct current stimulation (tDCS) on this region successfully modulated the magnitude of the social framing effect. These findings add to the knowledge about the role of perception of others’ pain in our social life.
1 Other people’s pain: the perspective of social psychology
Pain is defined as a distressing experience associated with actual or potential tissue damage, involving sensory, emotional, cognitive, and social components [1]. In both humans and animals, painful experiences are manifested in altered facial expressions, gestures, bodily reactions, vocal activities, and behavioral patterns [2]. From an evolutionary perspective, these pain signals are important for survival as they demand attention and express the need for healing and protection [2]. The perception of pain signals that are (unintentionally or intentionally) delivered by another person (i.e., the perception of other people’s pain) is the main topic of this review, which could be emotionally salient and socially meaningful for observers.
Two theories, which focus on different aspects, have described the subjective feelings and reactions triggered by observing pain in others. The first theory is the “empathizing hypothesis”, suggesting that the observation of pain in others triggers empathic reactions (see Section 2 for details). The second theory is the “threat value of pain hypothesis (TVPH)”, which suggests that the threat-detection system could be activated by the perception of pain in others [3]. To be specific, observing pain in others indicates the existence of a potential threat that may harm the observer and thus requires vigilance. Consequently, the threat-detection system is activated and generates an aversive response in the observer. Although the TVPH is relatively new, this hypothesis has received support from recent studies [4, 5].
While the two theories are not necessarily conflicting, this review is mainly interested in the prosocial function of pain indicated by the empathizing hypothesis. Below, we discuss how the perception of pain in others motivates and regulates prosocial actions (e.g., helping), whether and how these effects are driven by social emotions such as empathy and guilt, and how the relationship between social emotion and prosocial behavior manifests in social decision-making paradigms (especially social framing tasks). Exploring these questions can help to explain the basis of successful social interactions [6].
2 Social emotions related to other people’s pain
2.1 Empathy
Pain in others is a salient negative stimulus and can significantly affect the feelings and thoughts of observers [7]. At the neural level, the expression of pain in others activates the so-called “pain matrix” (i.e., the pain-related network: a set of brain regions associated with directly experienced pain) including the anterior insula (AI), the anterior cingulate cortex (ACC), the amygdala, the somatosensory cortex, and supplementary motor areas [7 –10]. This phenomenon indicates that when witnessing others in pain, the observer also experiences pain to some extent [11]. In line with this idea, event-related potential (ERP) research has demonstrated larger amplitudes of the ERP components N1, N2, P3, and late positive potential (LPP) in response to painful, rather than neutral, stimuli [3, 12 –15].
Observing others in a painful condition may elicit empathic emotions. Empathy refers to the capacity to vicariously share the affective states of others and adopt their point of view, which is a hallmark of psychological maturity that allows people to understand how others are emotionally affected by a given event [16–18]. The Perception-Action Model (PAM) proposed by Preston and de Waal suggests that empathic feelings automatically occur [19]. However, this viewpoint contradicts previous findings that empathic responses are restricted by cognitive resources such as working memory load [20]. Brain-imaging [e.g., functional magnetic resonance imaging (fMRI)] studies have shown that there are two components of empathy subserved by distinct brain networks, that is, a bottom-up affective resonance (associated with the mirror neuron system and the limbic system) and a top-down cognitively controlled process (associated with prefrontal cortical circuitries) [7, 21 –23]. Correspondingly, ERP experiments have revealed two temporal stages during the processing of painful stimuli (compared with non-painful ones), including an early, automatic stage of emotional contagion and affective sharing (indexed by the N1 and N2 components) and a late, higher-level stage that controls empathic responses and creates a self–other distinction (indexed by the P3 and LPP) [24 –26].
As pointed out by Singer et al., the ability to experience other people’s pain is a core feature of empathy [27]. Pain empathy is grounded in people’s first-hand experiences of pain, given that the perceptions of one’s own pain and another’s pain are subserved by overlapping neurocomputational functions [28 –30] and that they can be similarly modulated by psychological and pharmacological factors (e.g., placebos) [30, 31]. Physical painkillers (e.g., acetaminophen) reduce empathy for others’ pain via the same neural pathways that alleviate one’s own pain [32]. It should be noted that empathy for pain does not involve the entire “pain matrix” [27]. Key regions of the affective component of pain empathy include the AI, ACC, temporoparietal junction (TPJ), and inferior frontal gyrus, while those of the cognitive component include the inferior parietal lobule and mid-cingulate cortex (MCC), according to some recent meta-analyses on brain-imaging evidence [33, 34].
Contextual information about the imminence of a painful event (e.g., visual or verbal cues) may greatly influence one’s own sensations of pain [35 –37]. Likewise, empathy for pain in others is flexible and can be modulated by social context (i.e., the immediate social setting where the ongoing event happens) [38]. To take an example, when participants were exposed to video clips featuring an age-matched individual experiencing pain, their explicit rating for that pain was significantly lower when the pain-taker was responsible for his/her condition (e.g., infected with AIDS resulting from intravenous drug use) compared with when he/she was not responsible (e.g., infected with AIDS resulting from an infected blood transfusion) [39]. According to the literature, other social factors that are known to affect the perception and/or cognitive appraisal of others’ pain include: racial background [26, 40, 41], group membership [42–44], social reputation [45], and social hierarchy [46] of the pain-taker; the social relationship between the observer and the paintaker [4]; whether the pain is accidental or is intentionally inflicted by the observer or by another person [47, 48]; and whether the pain is associated with a reward for oneself [49].
In humans, facial expressions might be the most unambiguous and powerful way to deliver pain signals. Nevertheless, the use of facial stimuli is not required to induce empathy for pain in the laboratory; instead, the understanding that other people are in pain could be inferred from various nonfacial cues. To take an extreme example, a piece of slashed paper (as an artistic gesture) invites a sense of empathic movement, which might be based on imagination, inference, and perspective-taking [50]. To our knowledge, the most frequently used visual stimuli to date are static pictures showing the painful consequences of others’ actions, such as body–object (especially hand–object) interactions. For instance, when participants see that an individual is reaching out his/her hand to touch the sharp end of a knife, their empathic feelings might be elicited before the contact actually happens. In previous studies, the experimental effects of these pictures were compared with those showing the non-painful consequences of similar actions [12, 14, 24, 51]. According to some researchers, the processing of a body–object interaction employs both action representation and outcome expectation of this interaction [52, 53]. More specifically, there are three main stages in this processing: (a) differentiating different types of actions (e.g., approach vs. withdrawal), (b) encoding the sensory and tactile qualities of objects (e.g., noxious vs. neutral), and (c) integrating the information generated from the above two stages in a predictive manner to represent the outcome of the ongoing interaction (painful vs. non-painful) [54, 55]. Recent studies have reinforced this theory from the perspective of brain functions [56, 57].
2.2 Guilt
Guilt is another important social emotion relevant to the topic of this review. As a typical “moral emotion”, guilt is defined as an emotional experience associated with the belief (which may or may not be true) that one is responsible for violating a social norm or one’s own standard of conduct [58]. Guilt is unpleasant but has positive social consequences. People who feel guilty are more likely to make amends to repair the relationship between the transgressor and his/her “victim” [59, 60]. The absence of guilt is a prominent feature of psychopathy, which leads to antisocial behaviors [61]. Guilt could also be classified as a “self-conscious emotion” that features self-reflexive mental processes [62]. According to the classic attributional theory, the activation and operation of guilt depend on the outcome of self-evaluation processes; guilt emerges when a negative social event is attributed to a controllable aspect of the self (e.g., forgetting to fulfill a promise) [63]. In contrast, recent “adaptationist” theories focus on the interpersonal rather than intrapersonal effects of self-conscious emotions [64, 65]. According to this family of theories, guilt increases one’s social value by taking reparative actions, which would be beneficial for individuals to solve adaptive problems in the long run [66 –68]. At the neural level, guilt activates a wide range of elements in the social brain network, including those engaged in selfreferential processing [e.g., the medial prefrontal cortex (mPFC) and MCC] [69, 70] and theory of mind (e.g., TPJ and the superior temporal sulcus) [71, 72]. A recent fMRI study has shown that compared with shame (another self-conscious emotion associated with uncontrollable aspects of the self), guilt activates brain regions linked with theory of mind and emotion regulation (e.g., the dorsolateral prefrontal cortex) more strongly [73].
Many previous studies have manipulated guilt-like feelings by asking participants to recall autobiographical memories or using script-driven imagination [69, 72, 74 –78]. In the laboratory, guilty emotions can also be generated by perceptions of pain in others when the observer happens to be the pain-causer. Not inflicting harm on others is a universal moral principle. Thus, feelings of interpersonal guilt emerge when people are causally responsible for harming another individual. For example, when participants responded incorrectly in a dot-estimation task designed by Yu et al., a painful stimulation would befall their partner (who was actually a confederate) [70]. In this situation, the feeling of guilt involves otheroriented empathy for pain [79]. Correspondingly, the guilt associated with others’ pain elicits both the cognitive and affective components of the empathy-related network including the TPJ, AI, MCC, and ACC [48, 70, 80]. A recent study showed that the MCC is also recruited in collective (or group-based) guilt when another’s pain is not caused by the participant, but by a third person who is recognized as an in-group member with the participant [81].
Interestingly, the perception of a painful situation can be modulated by moral reasoning when one assumes that other people are feeling guilty. For example, participants rated the level of pain intensity as significantly higher for depictions featuring pain caused by another person compared with self-inflicted ones caused by the protagonist [82]. Further, enhanced hemodynamic activities were found in the amygdala, right TPJ (rTPJ), temporal pole, and posterior cingulate cortex when painful images were described as intentionally caused rather than accidentally caused by another individual [47].
Other kinds of social emotions may be occasionally related to the observation of others’ pain. For instance, an exaggerated expression of pain may evoke feelings of embarrassment and contempt in the observer [83]. We consider this kind of relationship to be less significant and thus make no further elaboration in our review. In the next section, we move on to discuss changes in decision strategies among people who feel empathy or guilt when perceiving (or imagining) others in pain.
3 Pain and social decisions
A decision may be labeled as a “social decision” when it involves a social component, such as deciding about others (whether to marry someone), for others (choosing a school for one’s children), or jointly with others (cooperating with business partners) [84]. Social decision scenarios can be resolved in either an interactive or a unilateral manner. According to classical economic literature (e.g., expected utility theory), emotion plays a negative role in decision-making as it interrupts rational thinking [85]. In contrast, studies in the past few decades have highlighted the significance of emotion in both nonsocial and social decisions [86]. Still, it is under debate in what way emotion influences decision-making. Inspired by pioneers such as Robert B. Zajonc, the “affect-as-information” hypothesis indicates that momentary affective states could serve informational functions in judgment and choice [87, 88]. Further, Paul Slovic points out that emotions act as important cues to aid rational thinking, calling this mechanism an “affect heuristic” [89 –91]. Meanwhile, George Loewenstein suggests that emotional feelings can shape decision-making directly rather than through modulating rational thinking and cognitive evaluation (the “risk-as-feelings” hypothesis); he also differentiates between “anticipated emotions” (i.e., emotions that are expected to be encountered in the future) and “anticipatory emotions” (i.e., emotions generated from the expected outcome) [92]. The so-called anticipatory emotions are the core of the “somatic marker hypothesis” proposed by Antonio Damasio, which states that previous experience associated with an option affects somatic responses (including heart rate, skin conductance, and tonicity) when decision-makers are exposed to the same option again, which could be regarded as somatic markers (of the corresponding option) that guide future decisions. Despite the discrepancies, these theories all belong to the broad class of dual-process models that claim there are two distinct processing modes: a fast, automatic, emotional “system 1” and a more deliberate, controlled, and analytic “system 2” [93 –95]. However, dual-process models have been criticized for their oversimplified nature [93, 96]. More recently, Jennifer Lerner suggested that researchers should distinguish between “integral emotions” (those arising from the decision at hand; e.g., feeling anxious when playing poker) and “incidental emotions” (those arising accidentally at the time of the decision; e.g., feeling sad because of the music being played in the casino); while integral emotions are an essential part of the decision process, incidental emotions might be distracting [86].
It remains undetermined if a unified neural mechanism underlies both social and nonsocial decision-making. Many researchers believe that regardless of whether a social component is involved, different kinds of decision-making are driven by identical neural value computations and corresponding brain processes [84, 97 –99]. For example, the ventral striatum (a key node within the dopaminergic midbrain system) is sensitive to both monetary reward and social approval [100]. One of our recent studies supports this “common neural currency” hypothesis, as a meta-analysis of neuroimaging findings showed that social and nonsocial reward processing engage a common neural circuit consisting of the ventral striatum, ventral tegmental area, and AI [101]. Nonetheless, it is undeniable that social decision-making also activates social-specific regions, including those responsible for social perception, attribution, intention detection, theory of mind, and social emotions such as empathy [102].
As two important social emotions, the impact of empathy and guilt on social decision-making is evident in everyday life. The key function of empathy in social interaction is bonding people together. Empathy bolsters prosocial behaviors (e.g., sharing, comforting, helping, and caring for others) by facilitating our comprehension of the affections, motivations, and behaviors of other people [16]. Likewise, guilt promotes prosocial behaviors (e.g., restitution, apologies, confessions, and self-punishment) to benefit victims and repair relationships [62, 73]. When making social decisions, one of our main goals is to avoid anticipated guilt [86]. It has been suggested that guilt aversion is a driving force behind reciprocity [103, 104].
In general, both empathy and guilt strengthen adherence to social norms, which may result from their relationship with morality. Morality can be defined as a set of prescriptive norms about how people should treat one another, including concepts such as justice, fairness, and rights [17, 105]. Empathy can motivate people to behave in accordance with moral principles [17], while guilt indicates that one has violated a moral principle and that it is necessary to remedy the situation. On the other hand, an aversion to the suffering of others is unanimously acknowledged as a moral obligation [106] and is a powerful motivator for humans [107]. Taken together, when one observes others in a painful situation and takes responsibility for that situation, the feelings of empathy and guilt being elicited (which should be categorized as “integral emotions” according to Jennifer Lerner [86]) can significantly affect moral judgment and subsequent decisions about others’ pain (Fig. 1). This mechanism explains why the perception of pain in others motivates and regulates prosocial helping behavior [2]. It would also be theoretically interesting to examine whether empathy-related and guilt-related brain regions are engaged in the trade-off between increasing one’s benefits and avoiding another’s pain (see Section 4.1).
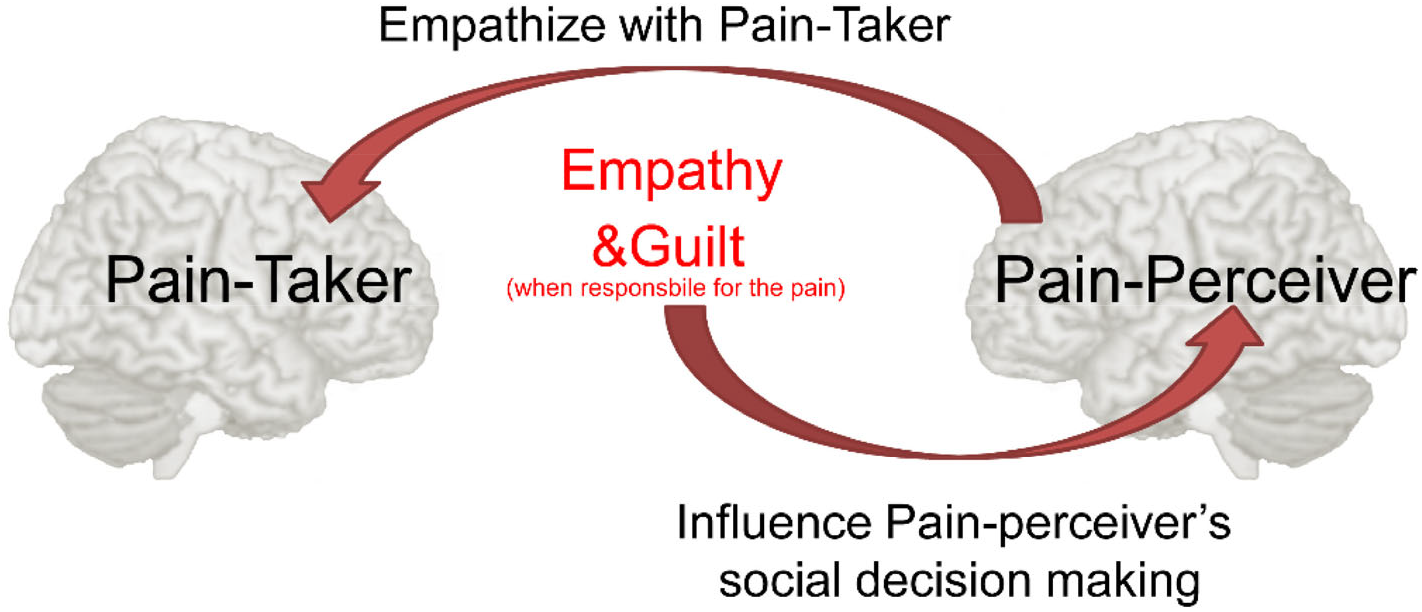
The proposed psychological mechanisms about how the perception of other’s pain affects social decisions.
Recent studies have demonstrated a positive relationship between empathy for pain and prosocial decisions to help others who are suffering from pain [42, 43]. For instance, participants who experienced enhanced empathy for pain (indexed by self-reported measures and empathy-related brain responses) were more likely to choose costly helping actions, to the extent that they were willing to endure pain themselves to lessen the pain of others [43]. Nevertheless, this effect might be weakened when an observer and a pain-taker are in a competitive (compared with a cooperative) context, as evidenced in one of our studies [4]. Whether the pain-taker could be considered as an in-group (in contrast to an out-group) member is also an issue [42, 43]. Similarly, when a participant’s erroneous responses during a cognitive task result in the application of a painful stimulus to his/her partner, he/she is prone to bearing a proportion of pain for that partner as compensation due to feelings of guilt, especially if he/she is solely responsible for the stimulation [70]. Guilt, but not shame, can increase cooperation among people who generally act uncooperatively [108]. Overall, the aforementioned findings reveal that a (real or hypothetical) painful experience of another person could be a powerful factor influencing social decision-making.
In the next section, we introduce background information about the social framing effect, which is an important topic in the field of decision science. Manipulating others’ pain in experimental designs has produced novel findings about this effect in some of our recent experiments.
4 Social framing effect
4.1 Definition and classic literature
The framing effect occurs when logically equivalent statements (i.e., the frame) about the same decision problem lead people to choose different options [109]. As a decision bias, the framing effect violates the consistency (invariance) axiom of normative rationality [110, 111]. The Asian disease problem (ADP) is a famous example: in a hypothetical situation where an uncommon disease is expected to attack 600 people, participants’ attitudes toward a disease-combating plan are strongly affected by how it is described; they prefer the plan when its outcome is expressed as “200 out of 600 persons will be saved” but avoid the same plan when the outcome is expressed as “400 out of 600 persons will die” [112]. The predominant explanation of this phenomenon is that positive or negative emotions elicited by the frame are integrated into cognitive judgments and subsequently elicit an approach or avoidance tendency, respectively. That is to say, ADP participants switch away from the option associated with 400 deaths because its description generates negative emotions that bias decision-making in a heuristic way. According to Kahneman and Frederick, the framing effect represents a competition between “system 1” and “system 2” [113]. Findings from neuroimaging studies support this viewpoint, as De Martino and colleagues found that, in a gain/loss gambling framing task, the amygdala (closely related with emotional processing) was activated when participants’ decisions were consistent with the framing effect, while the ACC (closely related with inhibition control) was activated when decisions ran counter to the framing effect [see also 114, 115, 116].
There are various ways to divide the framing effect into subtypes [117, 118]. An emerging trend is to distinguish the social from the nonsocial framing effect [119 –121]. This trend was partly inspired by the understanding that the mechanisms of social decision-making might be independent from those of nonsocial decision-making to some degree (see Section 3). However, the definition of the social framing effect is largely unclear in the literature. McDaniel and Sistrunk interpreted this effect as “the framing effect for social decisionmaking” or “the impact of framing on social dilemmas” [122, see also 123]. To be more specific, we define the social framing effect as a phenomenon where varying the description of a social dilemma (or social components in this dilemma) changes individual preferences for different options [124]. An effective social framing manipulation focuses on highlighting conflicts between personal interests and the interests of others [125]. This can be done by emphasizing (a) internalized social norms, (b) how others interpret one’s behavior, or (c) the expectations of each other’s behavior [126].
According to the taxonomy recently proposed by Dufwenberg, Gächter, and Hennig-Schmidt, there are two major approaches to manipulate the social framing effect [103]. The first approach is “valence framing” which puts the same information in an emotionally positive or negative light. For instance, participants might be endowed with some resources and then asked to determine how many resources they want to “give to” (positive framing) or “take from” (negative framing) the public good [120, 127, 128]. Researchers have suggested that positive framing motivates participants to focus on actions that could result in a positive externality for others; consequently, the likelihood of making prosocial decisions is expected to be higher under positive framing than negative framing [103]. The second approach is “label framing” which represents the game situation with alternative labels. For instance, the aforementioned resource dilemma might be described as a “Wall Street Game” or “Community Game” in the task instructions [119, 126, 129, 130]. The rationale is that the “Community Game” (or “Teamwork Game”, “Social Exchange Game”) connotes collective interests and cooperative social norms, thus boosting prosocial decision-making tendencies [119]. Unfortunately, both approaches have yielded equivocal results across different studies [131, 132]. Andreoni [127] and Park [128] reported that the rate of resource contribution to the public good was higher under the positive compared with the negative framing conditions, but Brewer and Kramer [133] found greater contributions under the “take” (or “keep”, “harvest”) compared with the “give” (or “leave”, “contribute”) framing conditions [see also 123, 134, 135]. Meanwhile, the cooperation rate was higher when the prisoner’s dilemma was labeled as a “Community Game” in contrast to a “Wall Street Game” in Liberman, Samuels, and Ross [119], but the reverse was true in Brandts and Schwieren [129]. Finally, there have been many other studies that report weak or no social framing effects [126, 136 –138].
Many factors might have accounted for these heterogeneous results [134]. To our knowledge, most previous studies asked participants to make decisions about economic benefits accruing to themselves and to others [120, 125, 134, 136, 138 –142]. Nevertheless, people generally care about their own monetary outcomes far more than those of others [107]. In this case, the influence of social framing on behavioral tendencies might be limited, especially for those who have a lower level of social preference [125]. Intriguingly, Crockett et al. recently designed a social dilemma examining preferences relating to subjective cost and physical pain: participants were asked if they would give up an amount of money in exchange for avoiding a painful electrical shock for themselves or for an anonymous other person [107]. Their results revealed that participants were more likely to trade-off their profits against the pain experienced by others rather than by themselves, indicating a “hyperaltruistic” tendency. (In contrast, a follow-up experiment indicated that participants were unwilling to harm themselves for others’ profit [143]). The findings from Crockett et al. [107] reveal that another’s pain boosts prosocial decisions more reliably compared with another’s economic income, thus making it practical to manipulate prosocial tendencies across different framing conditions (i.e., to create a social framing effect).
4.2 Our recent progress
Inspired by the study of Crockett et al. [107], we recently developed a social decision task that took others’ pain into account. Before the experimental session, each participant was introduced to a partner (confederate), who played the “victim” that would be exposed to the risk of receiving an electrical shock during the task. The probability of one’s partner receiving this shock increased proportionally with individual preferences for income maximization. The participant and his/her partner sat in different rooms since the expression of pain is unnecessary for eliciting social emotions including empathy and guilt (see Section 2). In each trial, the participant was shown a runway on a computer screen, which represented two possible outcomes on its left and right ends; one outcome (a costly helping one) was that the participant would lose 5 Chinese RMB from his/her final payment, but the partner would avoid the shock in this trial, and the reverse was true for the other outcome. Each participant was then asked to move an avatar on the runway to indicate his/her relative preference for the two possible outcomes. The resolution of the slider was 10%, which means there were nine different options (10%–90%) for the participant to choose.
Two framing conditions in our task described the possible outcomes in different ways. In the harm framing condition, it was implied that the shock was delivered as a result of the participant’s own action (“harm the other person by administering a painful electric shock and keep all your payment”); in the help framing condition, the shock was described as a part of the task (“help the other person to avoid a painful electric shock and subtract 5 RMB from your own payment”). In our opinion, participants should have experienced a stronger moral conflict with their social responsibilities in the harm frame and therefore would be more likely to choose the costly options to help (Fig. 2A).
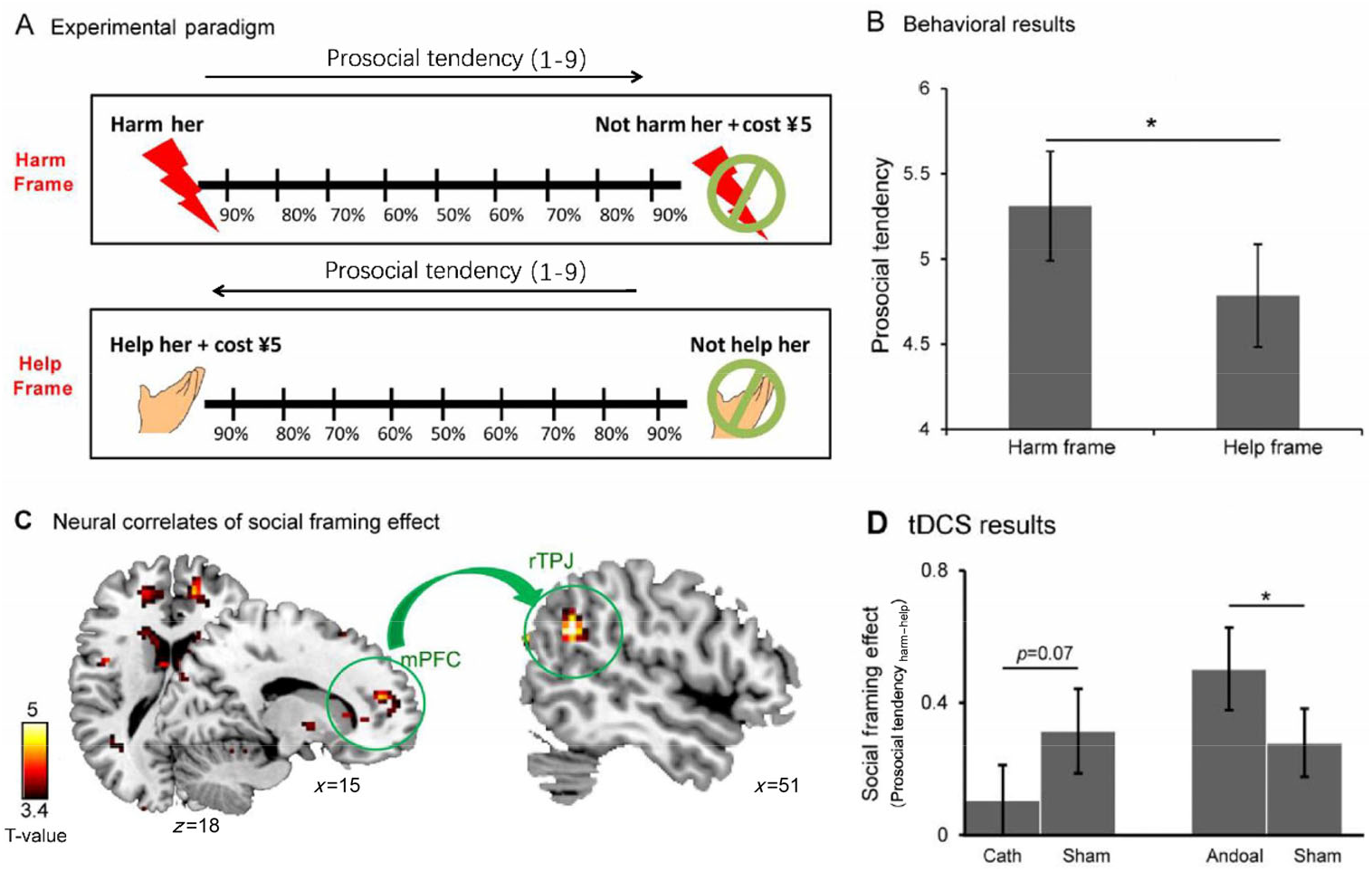
(A) Experimental design of our social framing task. The arrow above each frame indicates the direction of prosocial tendency corresponding to the choice. (B) Behavioral data of our neuroimaging experiment as indicated by difference of average prosocial tendency of all participants between harm and help frames. (C) Functional connectivity between the rTPJ and mPFC was underlying the observed behavioral social framing effect (i.e., participants showed significantly higher prosocial tendency in harm frame than they did in help frame). (D) Behavioral data of our tDCS experiment. Social framing effect was calculated as prosocial tendency harm−help = prosocial tendency harm frame − prosocial tendency help frame.
The behavioral results supported our hypothesis, that is, participants made many more prosocial decisions under the harm framing condition than the help framing condition, leading to a significant social framing effect (Fig. 2B). We also collected fMRI data during the task and found that the activation level of several brain regions increased as a function of the social framing effect size (parameter estimation). Among these regions, the bilateral TPJ became the focus of our further analyses due to its importance in the social brain network [144]. Permutation tests confirmed that the rTPJ (but not its left counterpart) could identify the trials in which participants’ decisions were consistent with the social framing effect (i.e., prosocial decisions under the harm framing condition, but not under the help framing condition) and the trials in which participants’ decisions ran counter to this effect. Moreover, psychophysiological interaction analysis revealed that the strength of the rTPJ–mPFC connection predicted the social framing effect size (Fig. 2C), possibly reflecting the impact of social emotions on decision preferences at the neural level [124].
As brain-imaging techniques, including fMRI, are constrained in making causal inferences [145], we then conducted a second experiment using transcranial direct current stimulation (tDCS) to examine whether the rTPJ plays a critical role in the social framing effect (Fig. 2D). Participants were asked to finish our social framing task as well as the classic monetary framing task from De Martino et al. [146] in two days. The sequence of these two tasks was counterbalanced across participants. The results showed that compared with sham stimulation, the social framing effect size increased under anodal (excitatory) stimulation but decreased under cathodal (inhibitory) stimulation of the rTPJ; in contrast, the nonsocial (monetary) framing effect was insensitive to tDCS manipulation [124].
We further explored whether the social framing effect was sensitive to social context, given that empathy for pain is highly context-dependent and that the neural response to others’ pain can be modulated by contextual factors [11, 147, 148]. Specifically, we used an impression-forming procedure from the study by Singer et al. [45] to manipulate each participant’s impression of his/her partner. Prior to the social framing task, each participant and two partners (confederates) played a one-round Dictator Game together, in which the partners acted as dictators to individually allocate 10 RMB between themselves and the real participant. One partner behaved fairly (evenly allocating the money), but the other one behaved unfairly. Then the real participant was asked to finish the social framing task with his/her partners playing the “victims” in different trials. We found an effect of impression forming on participants’ general attitudes, that is, participants were more likely to help a “fair” victim compared with an “unfair victim” at a cost to themselves. However, the social framing effect size (i.e., the behavioral difference between two framing conditions) was generally unaffected. These results are consistent with previous findings that empathic responses were reduced when participants viewed expressions of pain on an unfair person compared with a fair person [45].
In our opinion, the decision to “harm” others is more morally reprehensible than “not to help” others, which triggers a stronger conflict between moral values and material concerns [124]. Stronger empathic emotions and/or feelings of guilt are elicited accordingly, which are the main driving forces of the social framing effect observed in our studies. It should be noted that these emotions were anticipatory in our experiments, as the participants did not actually observe others in pain. In accordance with this finding, previous research has shown that the rTPJ is responsible for representing moral conflicts [149, 150]. Nevertheless, we did not employ explicit measures of emotional feelings in these experiments. In one of our most recent studies, we asked participants to fill the Questionnaire of Cognitive and Affective Empathy [151] and found that individual levels of the cognitive empathy trait do play a prominent role in the trade-off of painful experiences between oneself and others.
5 Summary and future directions
Researchers in the field of pain science are generally more interested in emotional feelings elicited by painful experiences at first-hand, including frustration, worry, anxiety, and depression [152, 153]. In contrast, this paper focuses on emotional feelings (particularly empathy and guilt) elicited by the observation of pain in other people. The influence of these emotions on social behavior and social decisions is discussed. Overall, previous findings have shown that empathy and guilt form a bridge between concerns for other people’s pain and prosocial behavior (e.g., costly helping). The relationship between pain observation, emotion, and morality can assist in understanding the social nature of human beings and is of scientific value for researchers and clinicians to investigate. Also, others’ pain could be used to manipulate the emotional feelings of participants in psychological research. By asking participants to make a trade-off between economic benefits and another’s experience, our recent studies have provided insight into the neural mechanisms of the social framing effect. The role of the rTPJ has been highlighted in these studies, which is not surprising given its importance in socio-emotional processing and moral judgment. More generally, our findings support the opinion that neural correlates of social and nonsocial decision-making are dissociated, given that the rTPJ is not recognized as a key region for the nonsocial framing effect [115, 146].
When taking individual differences into account, the implications of our findings for clinical science are worth noting. For example, it is well known that people with autism spectrum disorders are insensitive to the pain of others [154, 155]. Thus, it would be practically meaningful to examine whether this insensitivity is evident at the behavioral level (e.g., a smaller social framing effect size). From this perspective, our social framing paradigm has the potential to assist in the clinical observation of mental disorders. In addition, regarding the impact of emotion on decision-making (see Section 3), an unsolved problem is whether empathy and guilt elicited by pain in others modulate decision-making directly (as suggested by the risk-as-feeling hypothesis) or through cognitive evaluation (as suggested by the affect-as-information hypothesis). Finally, our findings indicate a close relationship between reward processing and pain processing, which has been acknowledged recently and needs to be explored further [156, 157].
Because of space limitations, this paper is mostly devoted to social emotions resulting from others’ pain. Put inversely, pain could be utilized as a tool to alleviate these emotions. When participants were reminded of an incident of unethical behavior, they tended to undergo physical pain (e.g., holding hands in ice water) and rated that experience as more painful [158]. In this case, the pain might serve as a self-punishment or be construed as cleansing to reduce the feelings of guilt [159]. Further, experiencing physical pain facilitates self-reward with guilty pleasures [160]. These phenomena indicate that beyond the scope of our review, there are still numerous issues to be explored regarding the dynamics between pain, emotion, and social behavior.
Footnotes
Conflict of interests
The authors declare that they have no conflict of interests.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 31871109, No. 31571124, No. 31900779), the Youth Innovation Promotion Association CAS (No. 2019088), and the Major Program of the Chinese National Social Science Foundation (No. 17ZDA324).