
Abstract
Objective:
Blood oxygenation level-dependent functional magnetic resonance imaging (BOLD-fMRI) in combination with diffusion tensor imaging (DTI) can clearly show the specific relationship between brain tumors and motor pathways. The purpose of this study was to investigate the role of this combination in surgery for brain tumors involving motor pathways.
Methods:
From September 2018 to March 2019, preoperative BOLD-fMRI and DTI examinations were performed in patients with brain tumors involving motor pathways who were being treated in a neurosurgery department. The patients were divided into two groups according to the combined examination results. In one group, the motor pathways were intact; in the other, motor pathways were infiltrated by tumors. The surgical plan was total resection of the tumor as far as possible and with no damage to the motor pathway. The preoperative and postoperative motor dysfunction and the rate of total resection in the two groups were compared.
Results:
Of the 20 patients with intact motor pathways, 15 had normal preoperative motor function, and 5 had preoperative motor dysfunction; of those 5 patients, 3 exhibited postoperative aggravation of motor dysfunction. Total excision was performed in 16 patients with intact motor pathways and incomplete excision in 4. Of the 22 patients with motor pathway infiltration, 8 had normal preoperative motor function and 14 had preoperative motor dysfunction; of those 14, 10 exhibited a postoperative increase in motor dysfunction. Total excision was performed in 8 patients with infiltrated motor pathways and incomplete excision in 14. Statistical analysis showed that there were significant differences between the two groups in preoperative motor function, postoperative changes in motor function, and total surgical resection rate (all p < 0.05).
Conclusions:
First, whether tumors invade the motor pathway is an important factor affecting the degree of preoperative motor dysfunction. Second, the risk for postoperative motor dysfunction was lower in patients with intact motor pathways than in patients with infiltrated motor pathways. Third, the rate of total tumor resection was higher in patients with intact motor pathways than in patients with infiltrated motor pathways. Last, the combination of BOLD-fMRI and DTI aided in the decision to perform total resection.
1 Introduction
The primary motor area (M1) and corticospinal tract (CST) are important components of the motor pathways involved in brain tumor surgery. Information about the M1 can be provided by blood oxygenation level-dependent functional magnetic resonance imaging (BOLD-fMRI), and information about the CST can be provided by diffusion tensor imaging (DTI). BOLD-fMRI and DTI are highly complementary, and both have many advantages, such as being nonradioactive, noninvasive, and repeatable. The combination of BOLD-fMRI and DTI performed before surgery can provide the surgeon with comprehensive information about the patient’s intracranial anatomy. Knowledge about the anatomical relationships among brain tumors, brain functional areas, and subcortical white matter fiber bundles allows the surgeon to choose the most appropriate and minimally invasive surgical approach [1]. In this study, BOLD-fMRI and DTI were combined to examine patients with tumors invading the motor pathways. The value of clinical application of this combination in managing motor pathway tumors was also explored.
2 Materials and methods
2.1 Subjects
All patients consented to the procedures, which were approved by the clinical research ethics committee of Zhongda Hospital, Southeast University. All patients in this study had brain tumors that were treated in the Department of Neurosurgery, Zhongda Hospital, Southeast University from September 2018 to March 2019. 26 were male and 16 were female, and the age distribution was 17 to 71 years, with an average age of 50.71 years.
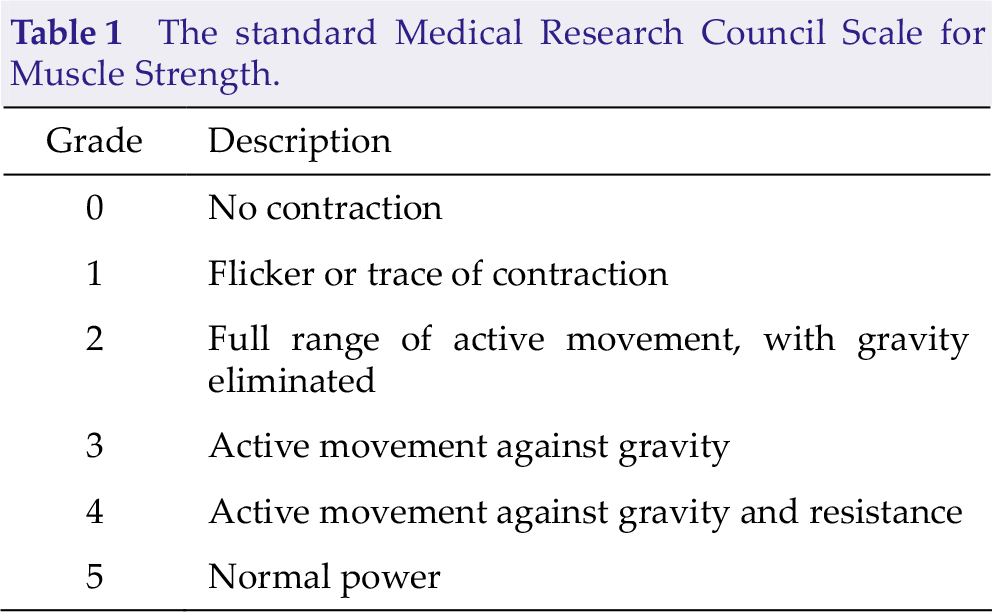
We used the following three conditions to determine eligibility: (1) Preoperative imaging data confirmed the presence of an intracranial space-occupying tumor located near the motor pathway; (2) the patiens were conscious, had the ability to cooperate with doctor in learning the movements associated with functional magnetic resonance imaging, and had muscle strength greater than level 2 in both hands; and (3) the patients were able to tolerate a 30-minute MRI scan while keeping the head still. The Medical Research Council (MRC) Scale for Muscle Strength (also known as the Oxford scale) was used in this study. The patients’ motor function was examined 1 week before the operation (Table 1) and reexamined 10 days after the operation. The contrast mediumenhanced head MRI was repeated within 72 hours after the operation.
The standard Medical Research Council Scale for Muscle Strength.
2.2 MRI equipment and imaging methods
The GE Signa HDxt 3.0T medical magnetic resonance scanner (GE Healthcare, Chicago, IL, USA) was used in this experiment. To prevent head movement, the physician communicated with the patient before the operation, and the patient’s head and whole body were immobilized in a static supine position during the MRI examination, and the gap between the head and the MRI head cover was filled with sponge padding.
2.3 BOLD-fMRI method
We performed the experiment in a blocked design, and chose a mode of motion alternating with rest. In order to avoid excessive sensory stimulation, we designated the clenching of both hands as the state of motion. In motion state: clenched fist then opened palm, frequency was 2 seconds once, lasted for 30 seconds. In rest state: opened palm, stayed stationary for 30 seconds. Therefore, after patients moving for 30 seconds, their hands were immediately stationary for 30 seconds. The BOLD signal was collected during the whole scanning process, which was comprised of five cycles of movement alternating with rest. Each cycle lasted for 60 seconds, hence the entire scanning process took 300 seconds (Fig. 1). After BOLD-fMRI was completed, DTI was conducted.

Blocked design task diagram. In each block, the patient’s hands moved for 30 seconds (labelled as 1) and rested for 30 seconds (labelled as 0). Five blocks were performed during the scanning process, which lasted for a total of 300 seconds.
2.4 DTI examination method
The DTI scanning result was presented to the post-processing workstation in the Digital Imaging and Communications in Medicine (DICOM) 3.0 format, and the fractional anisotropy and color tensor plots were calculated after the fractional data processing in the workstation. In this study, the regions of interest (ROI) were the two levels of the lateral cranial cerebrum and the front of the posterior internal capsule limb. DTI was performed to determine whether the brain tumor invaded the CST, the reconstruction of which was performed with iPlan 2.6 FiberTracking (BrainLab, Munich, Germany). The fractional anisotropy threshold selected is between 0.15 and 0.2, according to specific conditions.
2.5 BOLD-fMRI combined with DTI
In this study, volume rendering software was used to conduct three-dimensional reconstruction of the results; then the brain tumor, M1 region, and CST elements of the images were fused in the anatomical map to create a clear three-dimensional diagram of intracranial structural relations, which was then used to guide surgical treatment.
2.6 Classification of the relationship between preoperative tumors and motor pathways
We categorized the patients into two groups according to whether the tumor infiltrated the M1 region and CST. Patients in whom the tumor caused only the displacement of the M1 region or CST, but did not invade those areas, were designated as having intact motor pathways.
In patients in whom the tumor infiltrated the M1 region, the signal intensity of the M1 region changed, or the CST was partially or even completely fractured; these patients were designated as having infiltrated motor pathways.
2.7 Surgical methods
For the two types of relationship between the tumor and the motor pathway (intact and infiltrated motor pathways), we adopted different surgical resection methods. According to the BOLD-fMRI and DTI results of patients, a reasonable surgical approach and plan were devised. Through the fusion of the two images, we selected different surgical approaches, cortical incision sites, cortical traction directions, and degrees of tumor resection.
2.7.1 The relationship between brain tumors and M1 region was determined by BOLD-fMRI
We adapted the optimal surgical method, chose the most appropriate surgical position, and determined the minimally invasive cortical incision location according to the relative position and distance between the brain tumor and the M1 region: (1) If BOLD-fMRI examination showed that the brain tumor was in front of the M1 area, the cortical incision was made in the anterior central gyrus, and the patient was placed in the supine cephalic position. (2) If BOLD-fMRI examination showed that the brain tumor was behind the M1 area, the cortical incision was made posterior to the central posterior gyrus, and the patient was placed in the lateral position. (3) If BOLD-fMRI examination showed that the brain tumor was below the M1 region, one of two options was selected: For brain tumors that shifted the M1 region forward, the cortical incision was posterior, and the patient was placed in the lateral prone position; and for brain tumors that shifted the M1 region backward, the cortical incision was anterior, and the patient was placed in the supine cephalic position. The guiding principle of surgery was to avoid damage to the motor pathway while the maximum possible amount of brain tumors was removed.
2.7.2 The relationship between brain tumor and corticospinal tract was determined by DTI
According to the relative positions of and distance between brain tumor and CST, the optimal surgical resection scheme was as follows: (1) If the DTI examination showed that the tumor caused only CST displacement, the surgeon would remove all the tumor without damaging the nearby CST during the operation. (2) If the DTI examination showed that the tumor caused partial fracture of the CST, the surgeon had to protect other unbroken areas of the CST during the operation and remove as much of the tumor as possible. If the relationship between tumor boundary and CST was unclear, the surgeon could adapt the tumor resection as necessary. (3) If the DTI examination showed that the tumor causes complete CST rupture, the surgeon could attempt complete tumor resection.
2.8 Statistical analysis
Patients’ motor function was examined within 1 week before surgery and reexamined within 10 days after surgery. MRI was repeated within 72 hours after surgery. The differences between the two groups of patients in preoperative motor function preservation, changes in postoperative motor function, and rates of operative total resection were compared. SPSS statistical software package version 23.0 was used to process and analyze the data, and chi-square tests were used to conduct statistical analysis for the comparison between the two groups.
3 Results
3.1 Case data
Of the 42 patients with brain tumors who underwent BOLD-fMRI and DTI examinations before surgery, 20 had intact motor pathways and 22 had infiltration of motor pathways (Table 2).
Characteristics of patients.
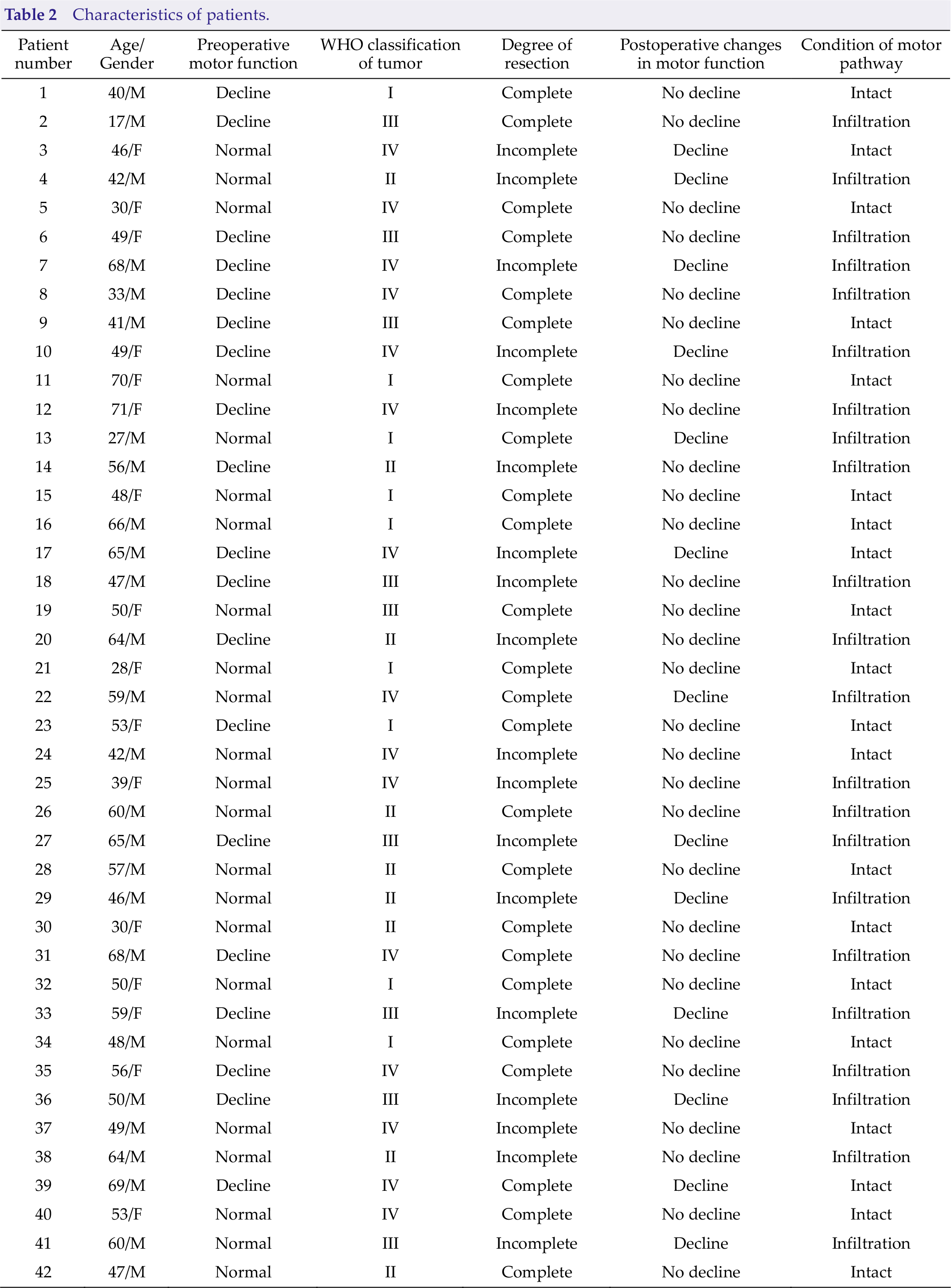
There were 26 male patients and 16 female patients. Their ages ranged from 17 to 71, with an average age of 50.71.
3.2 Comparison of preoperative motor function status between the two groups
Of the 20 patients whose motor pathway was intact, 15 had normal preoperative motor function; in the other 5, motor function was poorer in varying degrees. Of the 22 patients with infiltration of motor pathways, 8 had normal preoperative motor function, and 14 had varying degrees of motor function decline. Statistical comparisons of the two groups revealed significant differences in preoperative motor function, χ2 = 6.313, p = 0.016 (Table 3).
Preoperative motor function status in the two patient groups.

3.3 Comparison of postoperative changes in motor function between the two groups
In comparison to preoperative motor function, the 42 patients exhibited one of two results with regard to postoperative motor function: (1) unchanged or improved motor function and (2) a decline in motor function. In 17 patients with intact motor pathways, postoperative motor function either did not change or improved, but 3 patients showed different degrees of functional decline. In 12 patients with infiltration of motor pathway, postoperative motor function either did not change or improved, but 10 patients showed different degrees of functional decline. Chi-square tests showed statistically significant differences in postoperative changes in motor function between the two groups, χ2 = 4.546, p = 0.047 (Table 4).
Postoperative changes in motor function of the two groups.

3.4 Comparison of total surgical resection rates between the two groups
Postoperative MRI examination was used to evaluate the degree of surgical resection. All the patients underwent MRI reexamination within 72 hours after surgery. Among the 20 patients with intact motor pathways, imaging demonstrated complete resection in 16 and incomplete resection in 4. Among the 22 patients with infiltration of motor pathways, imaging demonstrated complete resection in 8 and incomplete resection in 14. Chi-square tests revealed statistically significant differences between the two groups in the rates of total resection, χ2 = 8.145, p = 0.006 (Table 5).
Total resection rates in the two groups.

4 Discussion
Surgery for tumors in the areas of the motor pathways often leads to major postoperative dysfunction, and in severe cases, loss of self-care ability. The tumor must be removed to the maximum extent possible to reduce the chance of recurrence, but the injury to normal brain tissue should be minimized to reduce the incidence of motor dysfunction [2, 3]. Although conventional MRI can show the boundaries of tumors, surgeons cannot always distinguish the anatomical relationship among the CST, M1, and tumors. In two previous studies, during the operation, the CST was inevitably damaged, which caused motor function damage [4, 5].
The combination of BOLD-fMRI with DTI in the treatment of intracranial tumors has been studied previously. Holodny et al. [6] applied the two imaging methods in combination to guide surgical resection of brain tumors, and the results showed that postoperative complications were significantly reduced. Niu et al. [7] used BOLD- fMRI and DTI to investigate the CSTs of 16 patients with intracranial tumors and demonstrated that the two techniques could localize the entire CST fiber pathway and accurately describe the spatial relationships of CST fibers to the tumor. These results illustrate the reliability of fMRI-guided DTI in surgery for brain tumors. The combination of BOLD-fMRI and DTI enhances the identification of tracts of interest in brains with anatomical deformations, which provides neurosurgeons with a more accurate approach for visualizing and localizing white matter fiber tracts in patients with brain tumors. This approach enhances surgical performance and preserves brain function.
Smits et al. [8] applied fMRI and DTI together to guide the operations in 9 cases of intracranial tumors, and the results showed that the combination of the two not only made up for the limitations of their respective clinical applications but also improved the rate of total tumor resection and the postoperative preservation of patients’ motor function. Wang and Wang [9] studied high-grade gliomas with BOLD-fMRI and DTI; their main objective was to evaluate the efficacy of integrating the data from BOLD-fMRI and that of DTI into radiation treatment planning for high-grade gliomas located near the primary motor cortexes and CSTs. They found that such integration was feasible and beneficial. Widdess- Walsh et al. [10] conducted a study on patients with focal epilepsy and found that by combining BOLD-fMRI and DTI before surgery, they could accurately depict the anatomical location of the epileptogenic focus. With thorough surgical planning, the rate of resection of epileptic lesions was high, and the incidence of surgical sequelae was low. Werring et al. [11] combined the two methods to study a patient with hypertensive cerebral hemorrhage at the site of internal capsule. After a year and a half of follow-up, the patient’s clinical symptoms of pyramidal tract injury disappeared; through BOLD-fMRI examination, Werring et al. found that the M1 area on the healthy side was activated, and a small amount of compensatory activation was also found in the M1 area on the affected side. They believed that the motor function rehabilitation mechanism of stroke was closely related to the ipsilateral compensatory activation of the motor function cortex and the anatomical direction and structural integrity of CST.
Our study showed that there was a significant difference in preoperative motor function between the patients with intact motor pathways and those with tumor infiltration. In those with intact motor pathways, the tumor did not destroy the nearby M1 area and CST, and so the patients generally had no motor dysfunction or just slight impairment. In patients with infiltrated motor pathways, the tumor had destroyed the nearby M1 area and CST, and so most affected patients had different degrees of motor dysfunction before surgery, depending on the degree of infiltration. This study also showed significant postoperative differences between the two groups of patients. In patients with intact motor pathways, the tumor caused only the displacement, not invasion, of the M1 region and CST. The anatomical relationship between these areas and the tumor was clear, and so resection was relatively easy and postoperative motor dysfunction was relatively rare.
In patients with infiltrated motor pathways, the destruction of M1 area and CST increased the complexity of the anatomical relationship. It was difficult for the surgeon to recognize the boundary between the tumor and the M1 area and CST, and so the operation was relatively difficult, and postoperative motor dysfunction was more common.
We believe that surgical risk is lower in patients with intact motor pathways than in patients with infiltrated motor pathways. This study showed a significant difference in the rate of total resection between the two groups of patients. In patients with intact motor pathways, the boundaries between the M1 and CST and the tumor were clear, and the tumors could be removed entirely without damage to the M1 and CST. In patients with infiltrated motor pathway, the boundaries between the M1 and CST and the tumor were unclear; thus surgeons had difficulty removing the tumors without damaging the M1 area and CST. If the scope of resection were expanded blindly, motor function could be impaired. Therefore, the rate of total tumor resection in patients with infiltrated motor pathway was low.
BOLD-fMRI and DTI, as new technological innovations, have their own shortcomings [12, 13]. Partial volume effect, image artifacts, and erroneous ROI selection can occur. This study had some limitations: (1) Because ROI selection for DTI is highly subjective, the imaging conditions and tracer algorithm cannot be completely unified. (2) The M1 area shown in BOLD-fMRI examination is determined by neurosurgeons only through subjective judgment; objective and unified judgment criteria are lacking. (3) The BOLD-fMRI study required the patients to be conscious and able to complete both fist-clenching motions as ordered. The ability of patients to complete the examination task as required varies, which may have some influence on the experimental results. With the progress of medical science and technology and the increasing maturity of various technologies, DTI and BOLD-fMRI will be combined with intraoperative navigation systems in the future. We believe that such technology will play a greater role in basic research and clinical application.
5 Conclusions
This study has shown (1) that the presence or absence of tumor invasion into the motor pathway affects the degree of preoperative motor dysfunction; (2) that patients with intact motor pathways had a lower risk of motor dysfunction than did patients with infiltrated motor pathways; (3) that patients with intact motor pathways had a higher rate of total tumor resection than did patients with infiltrated motor pathways; and (4) that the combination of BOLD-fMRI and DTI aided in the decision to perform total resection.
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the clinical research ethics committee of Zhongda Hospital, Southeast University, and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants in the study.
Conflict of interests
The authors declare that they have no conflict of interests.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81671819).