
Abstract
Objective:
The effects of repeated lumbar puncture and continuous lumbar cistern drainage on the cognitive function of patients with aneurysmal subarachnoid hemorrhage were compared and analyzed.
Methods:
Retrospective analysis was performed on 59 patients with aneurysmal subarachnoid hemorrhage treated at our Neurosurgery Department between October 2017 and October 2018. According to the hemorrhagic cerebrospinal fluid drainage mode after aneurysm clipping, the patients were divided into the following two groups: the repeated lumbar puncture drainage (Group A, n = 28) and continuous lumbar cistern drainage (Group B, n = 31). Before and 1 month after surgery, the cognitive function of the patients was scored using the Montreal Cognitive Assessment Scale. Scores of 27~30 were defined as normal, and scores of < 27 as cognitive impairment.
Results:
The incidences of cognitive impairment were 46% (13/28) and 32% (10/31) for Groups A and B, respectively, before surgery, but the difference was not significant (P > 0.05). The incidences of cognitive impairment were 35% (10/28) and 12% (4/31) for Groups A and B, respectively, at 1 month after surgery, with significant difference (P < 0.05).
Conclusion:
Compared with repeated lumbar puncture, continuous lumbar cistern drainage for aneurysmal subarachnoid hemorrhage significantly reduced the incidence of cognitive impairment after aneurysm clipping.
1 Introduction
Intracranial aneurysm refers to a tumor-like protrusion caused by arterial wall dilation under increased vascular pressure due to a weak blood vessel wall of the cerebral artery rather than by a solid tumor due to cell proliferation [1]. Compared with the courses of other intracranial diseases (such as tumor and inflammation), the course of aneurysmal subarachnoid hemorrhage is insidious, and acute onset is common (severe hemorrhage can occur within minutes of encephalopathy). The mortality rate of patients with the first onset is as high as 8%~32% [2]. At present, clinical surgical treatment primarily includes interventional embolization and surgical clamping. Both surgical clamping and interventional therapy have certain complications. Cognitive impairment is one of the most important complications, which is caused by vasospasm and damage to brain functional areas after intracranial aneurysm rupture and bleeding. It is generally believed that 12~23 h after aneurysm rupture and hemorrhage, red blood cells in the subarachnoid cavity begin to collapse and release oxyhemoglobin, which leads to cerebral vasospasm via a variety of mechanisms, and is the main cause of cerebral vasospasm after subarachnoid hemorrhage. Rebleeding of aneurysm can be controlled by craniotomy by clipping of the aneurysmal neck, but it is difficult to remove blood clots completely. Repeated lumbar puncture or continuous lumbar cistern drainage for aneurysmal subarachnoid hemorrhage after intracranial aneurysm clipping can remove blood clots and relieve cerebral vasospasm. Although some researchers have conducted related studies on the influence of postoperative cognitive function of intracranial aneurysm, few studies exist on the influence of hemorrhagic cerebrospinal fluid (CSF) drainage mode on cognitive function after aneurysm surgery.
Vascular cognitive impairment is a clinical syndrome that is characterized by different degrees of cognitive impairment caused by cerebrovascular disease and its risk factors [3, 4]. Takata et al. [5] performed animal experiments, which revealed that insufficient cerebral perfusion caused by continuous contraction of intracranial blood vessels was the primary factor leading to cognitive impairment. The rupture of intracranial aneurysms can lead to subarachnoid hemorrhage, which causes the continuous contraction of intracranial blood vessels. The operation of craniotomy aneurysm clipping for patients cannot completely remove the blood in the subarachnoid cavity, so some patients have different degrees of cognitive impairment, which adversely affects the lives of patients. To remove subarachnoid blood in a timely manner, the choice of hemorrhagic CSF drainage mode is crucial. The Montreal Cognitive Impairment Assessment (MoCA) scale is a simple screening tool for mild cognitive impairment designed by Nasreddine from Canada and his team in 2005 [6]. MoCA has good sensitivity and specificity for patients with mild cognitive impairment [6]. Presently, MoCA has been gradually applied in a wider range of diseases, including cerebrovascular diseases [7, 8], craniocerebral trauma [9], and Parkinson’s disease [10 –12]. In this study, MoCA was used to retrospectively analyze the effects of repeated lumbar puncture and continuous lumbar cistern drainage on the cognitive function of patients after aneurysm dissection.
2 Materials and methods
2.1 Patients
The patient selection criteria were as follows: (1) Intracranial aneurysm was diagnosed using whole cerebral angiography. (2) Computed tomography (CT) showed subarachnoid hemorrhage without extensive intracranial hematoma. (3) Preoperative Hunt–Hess grade was I–II. (4) The patients ranged in age from 20 to 70 years and had at least primary school education. (5) Craniotomy aneurysm clipping was successful. (6) Preoperative and postoperative cognitive function MoCA scores were available.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
2.2 Data collection
In this study, 59 patients with aneurysmal subarachnoid hemorrhage from October 2017 to October 2018 were treated in our Neurosurgery Department and confirmed by digital subtraction angiography. Patients with surgical contraindications, severe hepatic and renal dysfunction, and estimated survival time of < 12 months were excluded. All patients underwent intracranial aneurysm clipping within 3 days of onset. Because the Hunt–Hess grades of the selected patients in this study were all Grades I and II, and preoperative CT showed subarachnoid hemorrhage, CSF drainage was required for all patients postoperatively.
The indications for continuous and intermittent CSF drainage in this study were the same as follows: (1) Preoperative Hunt–Hess grades of the selected patients were Grades I and II. (2) Preoperative CT scan showed subarachnoid hemorrhage. In this study, different CSF drainage methods were randomly adopted according to the operation date of the patient. The patients underwent repeated lumbar puncture treatment on even-numbered days and lumbar cistern drainage treatment on odd-numbered days. According to the drainage mode of hemorrhagic CSF, the patients were assigned to either the repeated lumbar puncture drainage group (Group A; n = 28, 16 males, 12 females; mean age, 41.89 ± 15.19 years; range, 20~69 years), or the continuous lumbar cistern drainage group (Group B; n = 31; 17 males, 14 females; mean age, 44.52 ± 15.47 years; range, 23~73 years) (Table 1). Patients in Group A included 12 patients with Hunt-Hess Grade I and 16 patients with grade II. In Group B, there were 13 patients with Hunt-Hess Grade I and 18 patients with Grade II (Table 2). No statistically significant differences were noted in sex, age, and Hunt–Hess grade between the two groups (P > 0.05).
Comparison of basic data between the two groups
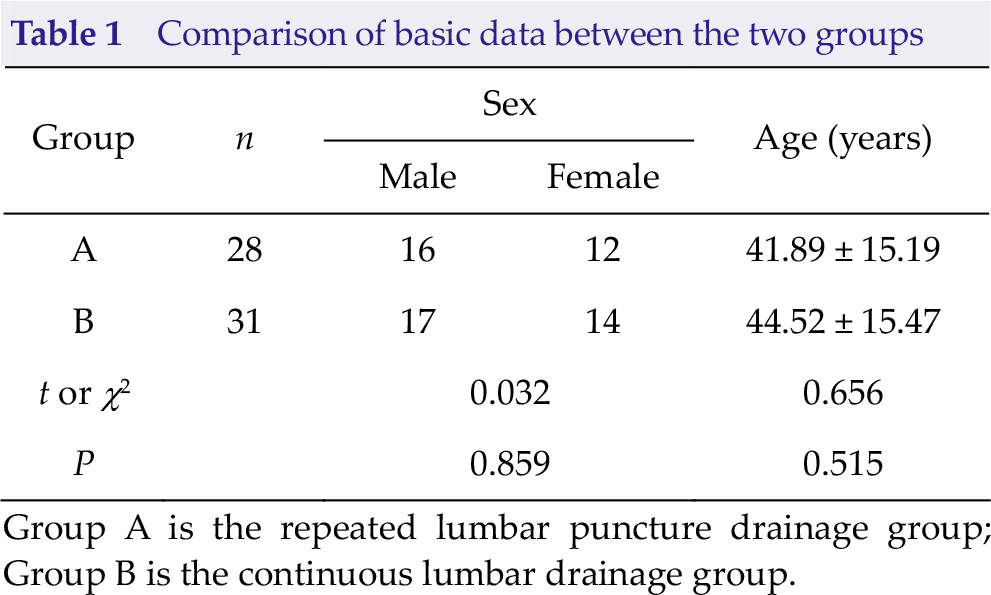
Group A is the repeated lumbar puncture drainage group;
Group B is the continuous lumbar drainage group.
Comparison of preoperative Hunt-Hess grades between the two groups
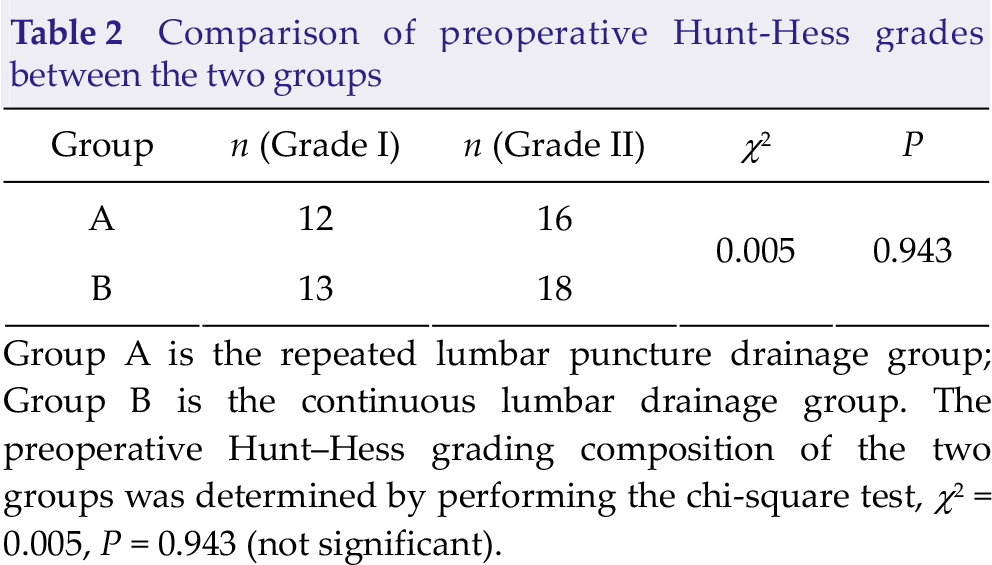
Group A is the repeated lumbar puncture drainage group; Group B is the continuous lumbar drainage group. The preoperative Hunt–Hess grading composition of the two groups was determined by performing the chi-square test, χ2 = 0.005, P = 0.943 (not significant).
The sex compositions of the patients in the two groups were tested by performing the chi-square test, χ2 = 0.032, P = 0.859, and the difference in sex compositions was not statistically significant.
The age distribution of patients in the two groups was normal, represented by mean ± standard. t = 0.656, P = 0.515, the difference in age distributions was not statistically significant.
2.3 Treatment options
The patients’ symptoms were treated with nimodipine, blood dilution, and induced hypertension after surgery. The patients began to use different drainage methods on the first day after surgery: intermittent lumbar puncture was performed in Group A to release 25~35 mL of CSF once a day for 7 consecutive days, and continuous lumbar cistern drainage was performed in Group B with the CSF flow controlled at 150 to 200 mL/d for 7 days.
2.4 Cognitive function assessment test method
The Chinese version of the MoCA scale was used to evaluate the patients. The Chinese version of the MoCA scale was previously revised according to the Chinese cultural background: (1) In the visuospatial and executive tests, “A, B, C, D, E” of the connection test were revised to the Chinese pronunciation of “Jia, Yi, Bing, Ding, Wu” respectively. (2) In the naming test, “rhino” was revised to “cow”, an animal familiar to the Chinese. (3) In the memory test, “velvet” and “church” were revised to “silk” and “hotel”, respectively, which are familiar to the Chinese. (4) In the attention test, identifying the English letter A was revised to identifying the Arabic number 1, which is familiar to the Chinese. (5) In the language repeat test, “I only know that John is the one to help today” and “The cat always hid under the couch when dogs were in the room” were revised to “He has not returned since he went out” and “He returned home to find the room full of his friends”, respectively, for the Chinese aphasia examination. (6) In the fluency test, “Name the maximum number of words in 1 minute that begins with the letter F” was revised to “Say as many animal names as possible in 1 minute”. The Chinese version of MoCA was used to score the cognitive function of Groups A and B before and 30 days after surgery, respectively. The MoCA scale had a total score of 30 points, scores of 26~30 points were defined as normal, and scores < 26 points were defined as cognitive impairment.
2.5 Statistical analysis
SSPS version 23.0 statistical software was used to analyze the data. The t test and chi-square test were used. At the level of a = 0.05, P < 0.05 was considered to be indicative of statistical significance, and all chi-square tests and P values were bilateral.
3 Results
3.1 Comparison of the incidences of cognitive impairment between the two groups before surgery (number of cases)
The incidence of cognitive impairment was 46% (13/28) in Group A, and 32% (10/31) in Group B before surgery (Table 3). No significant difference was noted in the incidences of cognitive impairment between the two groups (P > 0.05).
Comparison of the incidences of preoperative cognitive function between the two groups (number of cases).
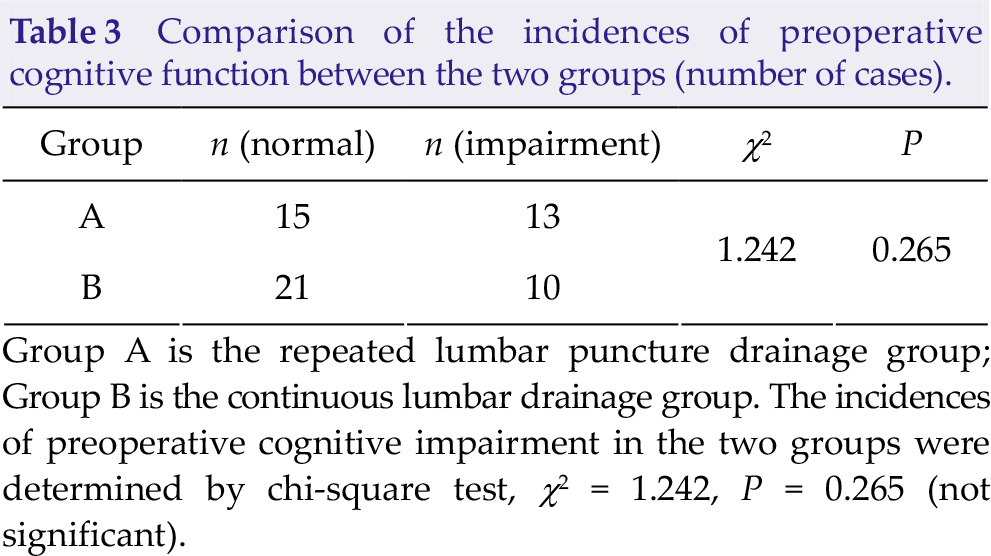
Group A is the repeated lumbar puncture drainage group; Group B is the continuous lumbar drainage group. The incidences of preoperative cognitive impairment in the two groups were determined by chi-square test, χ2 = 1.242, P = 0.265 (not significant).
3.2 Comparison of the incidences of cognitive impairment between the two groups 1 month after surgery (number of cases)
The incidence of cognitive impairment was 35% (10/28) in Group A and 12% (4/31) in Group B at 1 month after surgery (Table 4). A significant difference was noted in the incidences of cognitive impairment at 1 month after surgery between the two groups (P < 0.05). Compared with repeated lumbar puncture after aneurysm surgery, continuous lumbar cistern drainage after aneurysm clipping significantly reduced the incidence of cognitive impairment in the patients.
Comparison of the incidences of cognitive impairment 1 month after surgery between the two groups (number of cases)
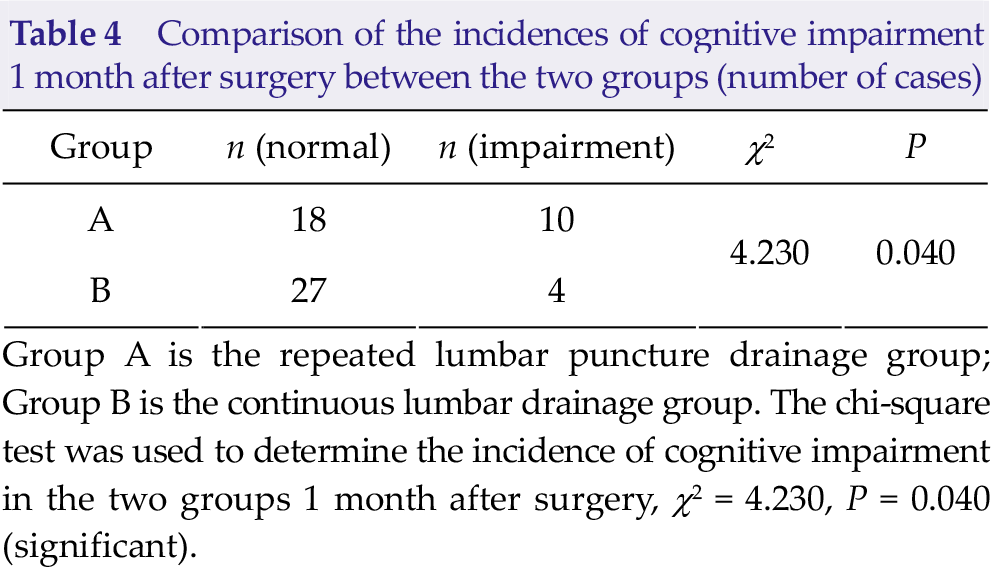
Group A is the repeated lumbar puncture drainage group; Group B is the continuous lumbar drainage group. The chi-square test was used to determine the incidence of cognitive impairment in the two groups 1 month after surgery, χ2 = 4.230, P = 0.040 (significant).
4 Discussion
4.1 Intracranial aneurysm clipping and cognitive impairment
To fully expose the aneurysmal tumor body and neck during surgery, it is inevitable that the surrounding brain tissue be pulled, which affects the blood supply to some brain tissue by causing ischemic injury and eventually cognitive impairment [13, 14]. However, there is increasing evidence that the most important factor associated with cognitive impairment caused by aneurysmal subarachnoid hemorrhage is the hemorrhage itself and the secondary brain injury related to the hemorrhage rather than the location or surgical intervention of the aneurysm [15]. In patients with aneurysmal subarachnoid hemorrhage, no significant difference in long-term cognitive function after craniotomy with clamps or interventional therapy has been found. Subarachnoid hemorrhage is the primary cause of cognitive impairment; thus, surgery does not cause new cognitive impairment [15 –17].
4.2 Hemorrhagic CSF drainage and cognitive impairment after intracranial aneurysm occlusion
Cognitive impairment refers to the absence of attention, feeling, intelligence, thinking, memory, self-knowledge positioning, and other psychological activities, which results in abnormal thinking and judgment and impairment of the brain’s advanced intelligent processing associated with learning and memory, thus causing damage to the composite function. An important cause of cognitive impairment is aneurysmal subarachnoid hemorrhage [17], after which, most patients suffer from shortterm or long-term cognitive impairment to varying degrees, with an incidence rate ranging from 7% to 60%, and even severe cognitive impairment 4~7 years after onset [18]. Studies have found that aneurysmal subarachnoid hemorrhage causes brain injury and cognitive impairment due to multiple factors, which include delayed cerebral ischemia, direct injury to cerebral hematoma, increased intracranial pressure, and chronic hydrocephalus [19]. Although surgery can clip aneurysms and prevent blood from entering the subarachnoid space through ruptured aneurysms, surgery cannot remove all subarachnoid hematoceles, so residual hematoceles can still lead to vasospasm in patients, thus affecting cognitive function. Therefore, drainage of hemorrhagic CSF after aneurysmal clipping is very important to reduce the incidence of postoperative cognitive impairment in patients.
4.3 Advantages and disadvantages of lumbar cistern continuous drainage
Lumbar puncture is an important auxiliary examination commonly used for neurological diseases, which is of great value for the diagnosis and treatment of diseases. On the basis of conventional lumbar puncture, Vourc'h G [20] first reported in 1963 regarding lumbar drainage treatment of CSF in patients with a large pool and obtained good curative effect. After nearly 50 years of development, large waist pool catheter drainage of CSF has become a common indispensable procedure in neurosurgery for treatment of diseases of the nervous system, and the scope of applications is increasing.
The results of this study showed that the incidence of cognitive impairment was significantly lower in Group B (continuous drainage) than in Group A (repeated drainage) 1 month after surgery (P < 0.05). This finding indicates that continuous lumbar cistern drainage reduced the incidence of cognitive impairment in patients after aneurysmal clipping. Under normal circumstances, the rate of CSF generation in adults is 0.35 mL/min, and about 500 mL of CSF can be produced every day. The continuous lumbar cistern drainage adopted in this study mainly follows the law of human CSF circulation and regeneration. Under the premise of being close to human physiological pressure, the larger the drainage volume, the shorter the time to remove hematoceles, reduce the hematocele residue, and effectively relieve the cerebral vasospasm. However, in this study, some patients in the lumbar cistern continuous drainage group still had cognitive impairment after surgery, which was primarily due to diffuse brain injury and secondary complications caused by subarachnoid hemorrhage, such as cerebral vasospasm and intracranial pressure increase, resulting in cognitive impairment [14, 21]. Repeated lumbar puncture drainage with a large waist pool and larger flow can accelerate the rate of removal of subarachnoid hemorrhage, reduce the stimulation of hemorrhagic cerebrovascular CSF, reduce the degree of cerebral vasospasm, and reduce the incidence of postoperative cognitive impairment in patients with aneurysms, but the disadvantage is that large pool drainage is not absolutely safe, so the following factors must be considered: (1) The rate of drainage and total amount of drainage must be controlled every day. An excessively fast drainage speed can easily lead to low cranial pressure or even cerebral hernia. Dagnew et al. [22] comprehensively reviewed previous studies, it is thought that excessive drainage of symptomatic I cerebellar tonsillar hernia deformity will lead to an incidence < 10% and a degree of asymptomatic I degree cerebellar tonsillar hernia deformity rate > 70%. (2) The operation must be standardized, principles of sterility should be followed, iatrogenic infection should be avoided, and the fixed pipeline should be changed regularly. (3) The puncture needle in the lumbar epidural kit is extremely sharp. During the operation, appropriate force should be exerted to grasp the needle and move it forward slowly. It is important not to exert too much force that may cause lumbar spine and nerve root injury. (4) The pipe must be properly fixed and some space reserved for the patient to roll over and move on the bed. (5) The drainage time must be strictly controlled because an excessively long time will increase the risk of intracranial infection.
Our results suggest that continuous lumbar cistern drainage is a very effective method for the treatment of aneurysmal subarachnoid hemorrhage, and it can reduce the incidence of postoperative cognitive impairment. Therefore, the first choice for hemorrhagic CSF drainage after aneurysmal clipping should be continuous lumbar cistern drainage.
Footnotes
Conflict of interests
The authors declare that they have no conflict of interests.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81671819).