
Abstract
We prospectively investigated the potential of positron emission tomography (PET) using the somatostatin receptor (SSTR) analogue 68Ga-DOTATATE and 2-deoxy-2[18F]fluoro-D-glucose (18F-FDG) in diffuse parenchymal lung disease (DPLD). Twenty-six patients (mean age 68.9 ± 11.0 years) with DPLD were recruited for 68Ga-DOTATATE and 18F-FDG combined PET/high-resolution computed tomography (HRCT) studies. Ten patients had idiopathic pulmonary fibrosis (IPF), 12 patients had nonspecific interstitial pneumonia (NSIP), and 4 patients had other forms of DPLD. Using PET, the pulmonary tracer uptake (maximum standardized uptake value [SUVmax]) was calculated. The distribution of PET tracer was compared to the distribution of lung parenchymal changes on HRCT. All patients demonstrated increased pulmonary PET signal with 68Ga-DOTATATE and 18F-FDG. The distribution of parenchymal uptake was similar, with both tracers corresponding to the distribution of HRCT changes. The mean SUVmax was 2.2 ± 0.7 for 68Ga-DOTATATE and 2.8 ± 1.0 (t-test, p = .018) for 18F-FDG. The mean 68Ga-DOTATATE SUVmax in IPF patients was 2.5 ± 0.9, whereas it was 2.0 ± 0.7 (p = .235) in NSIP patients. The correlation between 68Ga-DOTATATE SUVmax and gas transfer (transfer factor of the lung for carbon monoxide [TLCO]) was r = .34 (p = .127) and r = .49 (p = .028) between 18F-FDG SUVmax and TLCO. We provide noninvasive in vivo evidence in humans showing that SSTRs may be detected in the lungs of patients with DPLD in a similar distribution to sites of increased uptake of 18F-FDG on PET.
DIFFUSE PARENCHYMAL LUNG DISEASE (DPLD) is associated with significant morbidity and has an incidence of 57 in 100,000 per year. It consists of a heterogeneous group of diseases with varying amounts of interstitial inflammation and fibrosis. 1 Whereas the prognosis and treatment are relatively good for nonspecific interstitial pneumonia (NSIP), treatment options are limited and the prognosis is poor for idiopathic pulmonary fibrosis (IPF). Development of new and effective treatment options is urgently needed. Using the currently available clinical end points such as serial lung function and survival data, trials of novel agents will be long in duration and require costly clinical studies. However, at present, there is a lack of useful biomarkers to directly quantify or monitor disease activity in DPLD.2–5
It was recently demonstrated that 2-deoxy-2[18F]fluoro-D-glucose (18F-FDG) positron emission tomography (PET) signal is consistently raised and can be objectively measured in patients with DPLD.6–9 The spatial resolution of PET is limited, and 18F-FDG is a nonspecific tracer. 10 So it could be argued that its uptake in DPLD is secondary to inflammation either of the interstitium or in infected dilated airspaces consequent on adjacent fibrosis11,12 rather than active fibrogenesis.
Somatostatin receptor (SSTR) analogues labeled with positron emitters have recently become available. 13 These tracers have higher specificity in terms of cellular targeting than 18F-FDG, which simply reflects glucose metabolism. SSTRs are expressed on monocytes and lymphocytes but have not been described on neutrophils.14,15 This reflects the clinical observation that patients with pneumonia show uptake of 18F-FDG but not of the somatostatin analogue DOTATATE in the affected lung. 11 Moreover, somatostatin analogues were recently shown to suppress pulmonary fibroblasts in animals in vivo and in human pulmonary fibroblasts in vitro. 16 Indeed, there is potential for radionuclide imaging as previously described using conventional gamma imaging. 17 However, this type of imaging is limited by resolution compared to PET. 18
In this study, we performed imaging of DPLD patients with a somatostatin analogue PET tracer and compared the PET findings to those using 18F-FDG. The hypothesis was that the greater cellular targeting of DOTATATE would result in different uptake characteristics in comparison with 18F-FDG. Therefore, a broad spectrum of DPLD was included in the study, ranging from predominantly fibrotic processes (IPF) through mixed inflammatory and fibrotic patterns (NSIP) to inflammatory predominant patterns (cryptogenic organizing pneumonitis [COP]) on the basis of high-resolution computed tomography (HRCT).
Materials and Methods
Patients
Institutional Review Board permission and informed patient consent were obtained for this prospective study. Twenty-six patients (19 males, 7 females; mean age 68.9 ± 11.0 years) with DPLD were recruited for combined PET/HRCT studies using both a 68Ga-SSTR analogue and 18F-FDG. All patients were diagnosed with DPLD following multidisciplinary review on the basis of clinical and pulmonary function test (PFT) findings and the HRCT features. Ten patients had IPF diagnosed on the basis of concordant clinical and imaging findings according to the American Thoracic Society-European Respiratory Society criteria. 2 Twelve patients had NSIP, 11 diagnosed clinically on the basis of imaging features and 1 diagnosed on open lung biopsy. Four patients had other forms of DPLD; two patients had biopsy-proven COP, one patient had amiodarone-associated interstitial fibrosis, and one patient had asbestosis. Infection and thoracic malignancy were excluded on clinical and radiologic grounds. Full PFTs were performed. The clinical profile of the patients is summarized in Tables 1, Table 2, and Table 3.
Clinical Profile of the 10 Patients with Idiopathic Pulmonary Fibrosis Recruited for This Study

FDG = fluoro-D-glucose; IPF = idiopathic pulmonary fibrosis; SUVmax = maximum standardized uptake value; TLCO = transfer factor of the lung for carbon monoxide.
Lung biopsy was performed.
Pulmonary function tests are percent predicted.
Clinical Profile of the 12 Patients Recruited with Nonspecific Interstitial Pneumonia for This Study
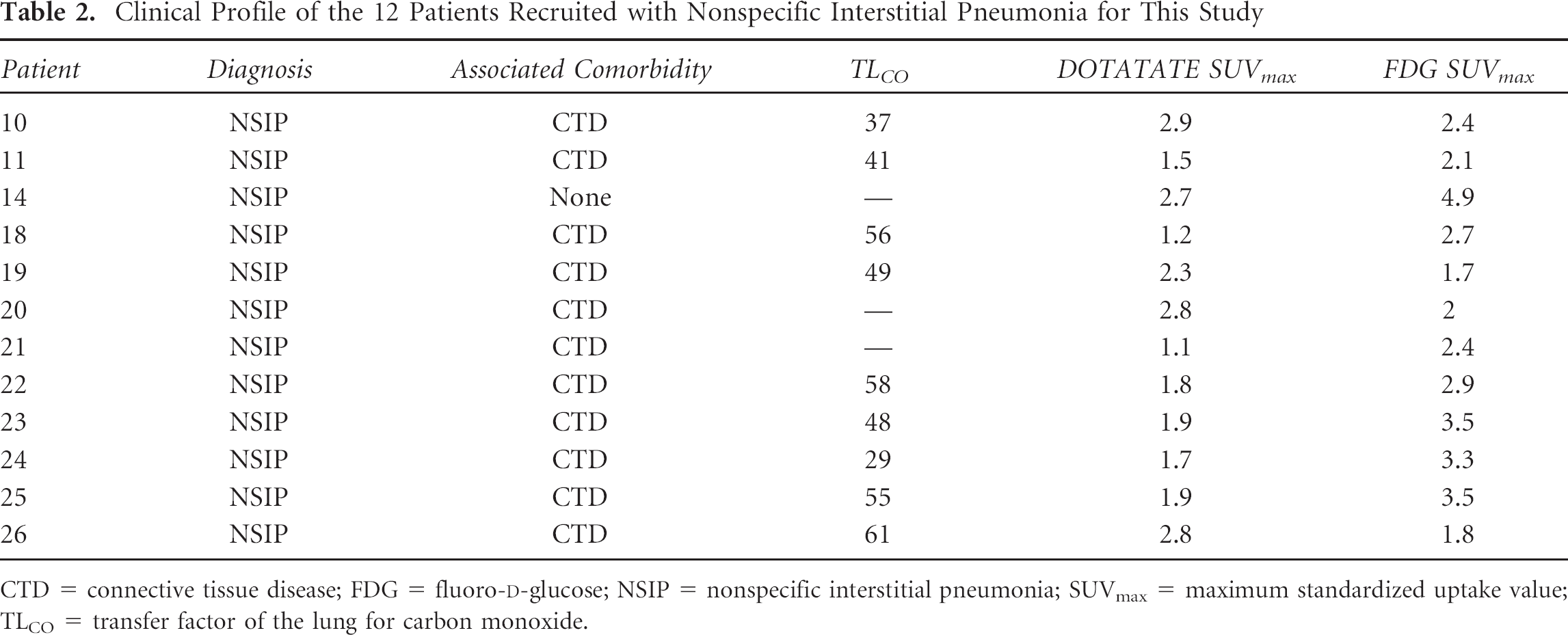
CTD = connective tissue disease; FDG = fluoro-D-glucose; NSIP = nonspecific interstitial pneumonia; SUVmax = maximum standardized uptake value; TLCO = transfer factor of the lung for carbon monoxide.
Clinical Profile of the 4 Patients with Other Forms of Diffuse Parenchymal Lung Disease (not Idiopathic Pulmonary Fibrosis or Nonspecific interstitial Pneumonia) Recruited for This Study

COP = cryptogenic organizing pneumonia; CTD = connective tissue disease; SUVmax = maximum standardized uptake value; TLCO = transfer factor of the lung for carbon monoxide.
Lung biopsy was performed.
Pulmonary function tests are percent predicted.
Imaging
Radiolabeling of ≈ 50 μg DOTATATE ([DOTA-DPhel, Tyr3]-ocreotate) with 600 to 1,200 MBq 68Ga was performed with fully automated equipment from Eckert & Ziegler (Berlin, Germany). 19 The automated preparation was done under sterile conditions in an isolator, and the labeling yield was analyzed by high-performance liquid chromatography (HPLC).
Images were acquired 1 hour after injecting 200 MBq of 18F-FDG or 175 MBq of 68Ga-DOTATATE using a dedicated combined PET/64-detector computed tomography (CT) unit (GE Healthcare Technology, Waukesha, WI). For both the 18F-FDG and DOTATATE studies, three imaging sequences of the thorax were performed while the patient remained supine on the table throughout – “physical coregistration.” CT was performed for attenuation correction using 64 × 3.75 mm detectors, a pitch of 1.5, and 5 mm collimation (140 kVp and 80 mA in 0.8 seconds). Maintaining the patient's position, a whole-body PET emission scanning was performed and covered an area identical to that covered by CT. Next, maintaining the patient's position, deep inspiratory HRCT was performed using 64 × 1.25 mm detectors, a pitch of 0.53, and 1.25 mm collimation (120 kVp and 100 mAs). Somatostatin analogue acquisitions were carried out in three-dimensional mode (4 minutes/bed position), whereas 18F-FDG acquisitions were carried out in two-dimensional mode (8 minutes/bed position). Forty-seven transaxial emission images of 3.27 mm thickness (pixel size 3.9 mm) were reconstructed using ordered subsets expectation maximization (OSEM) with two iterations and 28 subsets. The axial field of view was 15.7 cm per bed position.
Image Analysis
The methodological details of our technique and its reproducibility in DPLD have already been described. 6 PET/CT images were reviewed by a radiologist with dual accreditation in nuclear medicine with a long-term interest in cardiothoracic PET/CT (< 5 years). PET/CT images were loaded onto an Advantage workstation (GE Healthcare Technology). Both attenuation- and non-attenuation-corrected images were reviewed to ensure that areas of higher density lung were not accounting for increases in the PET standardized uptake value (SUV). 20 Using an automated 5 mm region of interest manually moved throughout the lung parenchyma, the maximum standardized uptake value (SUVmax) was recorded (Figure 1).
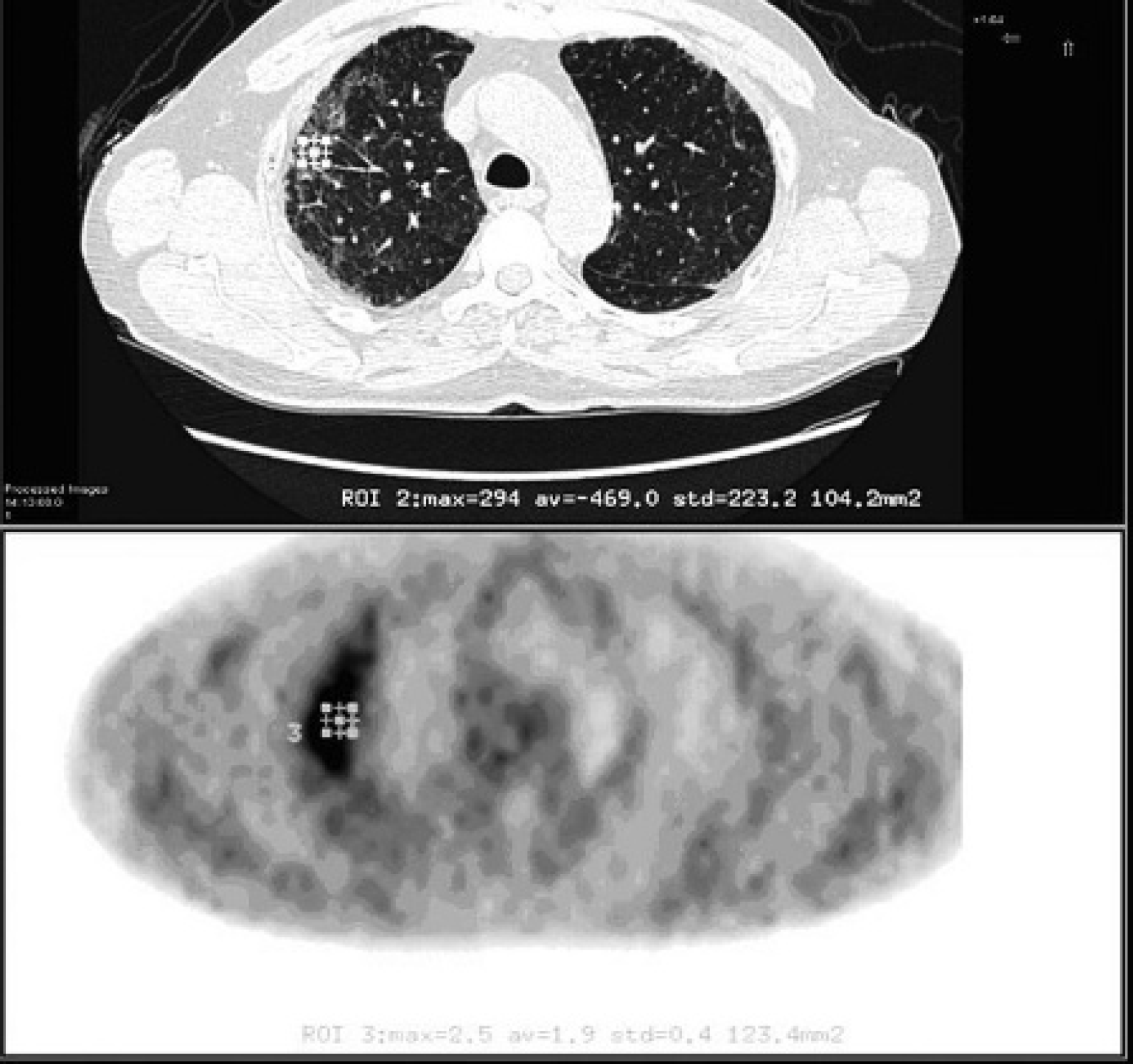
A 68-year-old male patient with known idiopathic pulmonary fibrosis. The lower image from a 18F-FDG-PET study demonstrates a region of interest (ROI) measuring the pulmonary SUVmax at 2.5. The upper image is the coregistered axial CT scan.
The HRCT images were reconstructed using soft tissue and high spatial frequency reconstruction algorithms. The images were then loaded into a proprietary workstation and reviewed by a thoracic radiologist with a specialist interest in HRCT (more than 13 years' experience) without detailed knowledge of the PET images. The radiologist had access to the full HRCT data set but was only given PET/CT images of the sites of interest identified by the PET reporters (see above). The lung parenchyma in the region of the maximal pulmonary 18F-FDG uptake (see above and below) was examined for the presence of ground-glass opacity, reticulation, honeycombing, and architectural distortion/traction bronchiectasis; thus, the predominant pattern was determined, that is, ground-glass predominant21,22 or reticulation/honeycombing predominant.23,24
Statistical Analysis
All statistical tests were performed using software from GraphPad (San Diego, CA). Normality was assessed using Kolmogorov-Smirnov testing. Comparisons between 68Ga somatostatin analogue and 18F-FDG uptake were made using unpaired t-tests. Comparison of findings between tracer pulmonary uptake of IPF and other DPLD patients and between SUV in honeycombing and ground-glass HRCT patterns was made using unpaired t-tests. Correlations between pulmonary tracer uptake and PFTs were made using linear regression. Statistical significance was set at p ≤ .05.
Results
See Table 1, Figure 2, and Figure 3.
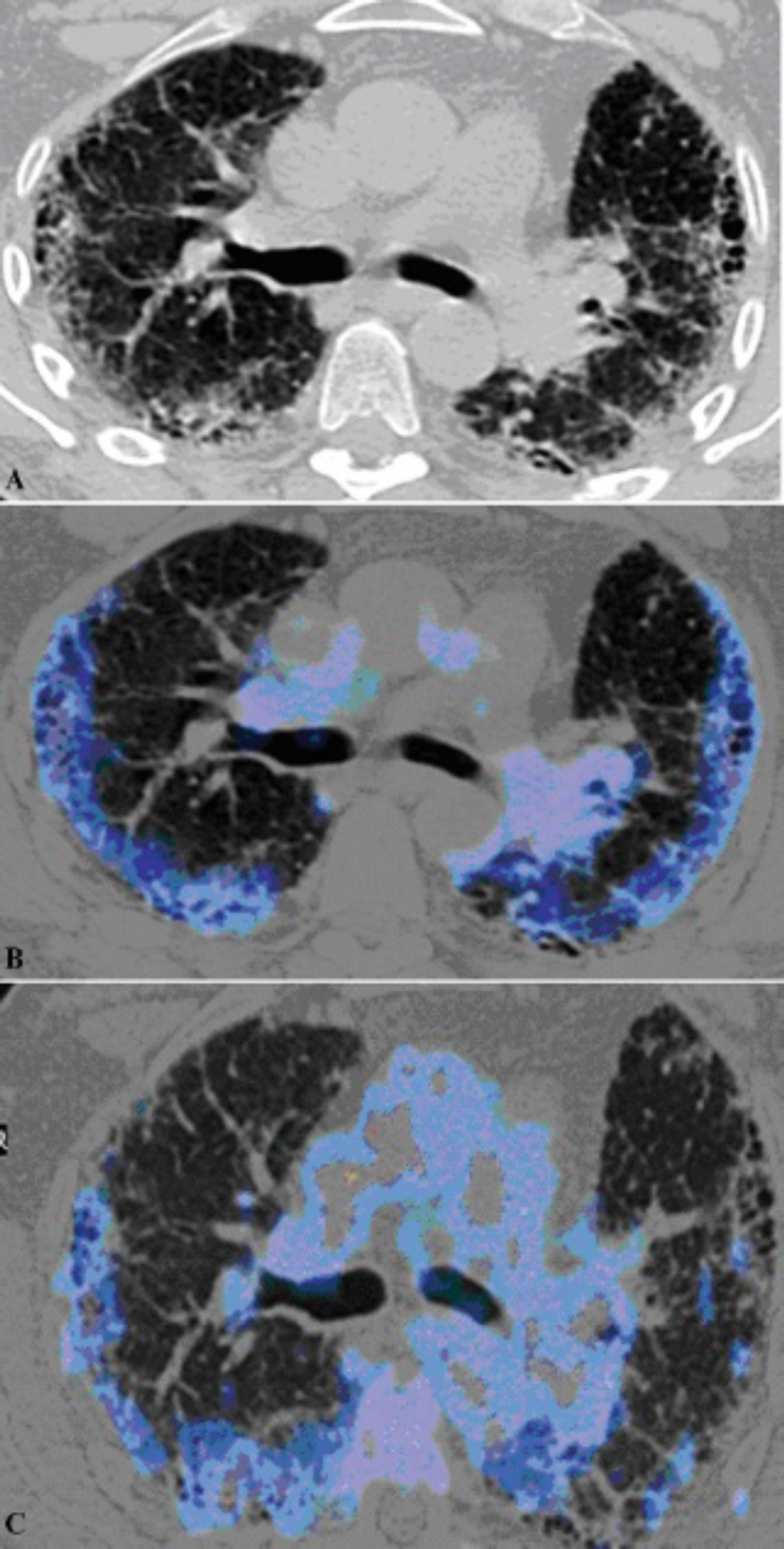
A 68–year-old male patient with idiopathic pulmonary fibrosis. The axial CT scan (A) shows the pulmonary parenchymal pattern of reticular and honeycombing. These areas correspond to increased uptake of 68Ga-DOTATATE (blue) on the fused PET/CT image (B). A similar lung parenchymal pattern of tracer uptake is identified on the 18F-FDG fused image (C). There is, however, more mediastinal uptake of tracer compared to the 68Ga-DOTATATE.

A 63-year-old male patient, one of eight with idiopathic pulmonary fibrosis in the study cohort. The coronal CT scan (A) shows the pulmonary parenchymal pattern of honeycombing, which corresponds to increased uptake of 68Ga-DOTATATE (blue) on the fused PET/CT image (B). The infradiaphragmatic uptake (yellow) is physiologic hepatic activity.
Somatostatin Imaging
The labeling yield and radiochemical purity of 68Ga-DOTATATE were > 97% at a specific activity of 17 to 34 GBq/μmol.
The mean lung 68Ga-DOTATATE SUVmax was 2.2 ± 0.7 compared to the quoted mean 68Ga-DOTATATE SUVmax of normal lung of 1.3. 25 The mean background lung 68Ga-DOTATATE was 0.4 ± 0.2 (normal lung confirmed on HRCT). The mean pulmonary somatostatin analogue target to background (lung) ratio (TBR) was 5.3 ± 2.3. The mean mediastinal node SUVmax was 1.8 ± 0.6. The areas of increased somatostatin analogue uptake corresponded to the distribution of lung parenchymal abnormality on coregistered CT. The mean 68Ga-DOTATATE SUVmax in patients with IPF was 2.5 ± 0.9, whereas in other forms of DPLD, it was 2.1 ± 0.7 (p = .253). The correlation between SUVmax and gas transfer (transfer factor of lung for carbon monoxide [TLCO]) was −0.34 (p = .127).
Correlative Imaging with HRCT and 18F-FDG PET
Two of the above patients did not have 18F-FDG PET studies; one had a biopsy before the 18F-FDG study could be performed, and the other withdrew from the study following the 68Ga-DOTATATE PET examination. The mean interval between 68Ga-DOTATATE and 18F-FDG PET/CT studies was 2.2 months. In all patients, the areas of increased somatostatin analogue uptake corresponded to the distribution of lung parenchymal abnormality on coregistered CT. The uptake of DOTATATE had an SUVmax of 1.9 ± 0.7 in ground-glass-predominant HRCT lung parenchyma pattern, whereas in reticular honeycomb lung parenchyma changes, it was 2.4 ± 0.7 (p = .12).
The mean 18F-FDG SUVmax was 2.8 ± 1.0 versus 68Ga-DOTATATE of 2.2 ± 0.7 (p = .018). The mean 18F-FDG background lung was 0.6 ± 0.2 versus 68Ga-DOTATATE of 0.4 ± 0.2 (p= .008). The mean 18F-FDG TBR was 5.2 ± 2.1 versus 68Ga-DOTATATE TBR of 5.3 ± 2.3 (p = .832). The mean mediastinal node 18F-FDG SUVmax was 2.9 ± 1.0 compared to 68Ga-DOTATATE nodal uptake of 1.8 ± 0.6 (p < .001). The areas of increased 68Ga-DOTATATE uptake corresponded to the distribution of pulmonary 18F-FDG uptake at the site of lung parenchymal change on HRCT.
The 18F-FDG SUVmax parenchymal uptake in patients with typical IPF was 2.9 ± 1.2, whereas in those with other forms of DPLD, the uptake was 2.8 ± 0.9 (p = .743). The correlation between 18F-FDG SUVmax and TLCO was −0.49 (p = .028).
Discussion
We present novel PET/CT data on the imaging of DPLD with the use of a labeled somatostatin analogue in combination with 18F-FDG. In all DPLD patients, a disease signal was identified on 68Ga-DOTATATE PET. This signal mirrored the distribution of lung parenchymal abnormality on HRCT and the pattern of tracer uptake on 18F-FDG studies.
In this study, there was a moderate negative correlation between pulmonary 68Ga-DOTATATE uptake and gas transfer, in keeping with our previous observation using 18F-FDG. 6 However, the relationship between transfer factor and 18F-FDG uptake was stronger than with 68Ga-DOTATATE. In keeping with 18F-FDG PET DPLD studies,6,8 we found no significant difference in 68Ga-DOTATATE uptake between patients with IPF and NSIP. In fact, we once again observed that honeycomb areas had a higher uptake than that of ground glass, although this did not reach statistical significance in this series. The lack of difference between IPF and NSIP and the association of 68Ga-DOTATATE uptake with TLCO are in contrast to very recent published data. 26 In that study, using the less specific SSTR analogue 68Ga-DOTANOC, NSIP was shown to have higher pulmonary uptake than IPF. 26 An explanation for this discordance is needed highlighting the need for more investigation and data.
Preclinical studies with somatostatin analogue treatment in IPF have shown attenuation of pulmonary fibrosis. 16 Human studies have now been performed, and some studies have even been completed, and the results are awaited. 27 Given that we showed that we can detect a PET signal with a somatostatin analogue, there could be genuine interest in using PET in disease characterization, and it would be important to investigate whether this technique could be used for monitoring in therapeutic trials.
Given that the PET signal from both somatostatin analogue and 18F-FDG showed a similar distribution pattern at the corresponding sites of parenchymal abnormality on the coregistered HRCT, it would be important to reveal the exact source of the PET signal in our patients. It could be argued that the increased 18F-FDG PET signal in areas of pulmonary fibrosis could be attributed to neutrophils in infected dilated airways in DPLD patients. The apparent lack of SSTR expression in human neutrophils argues against this hypothesis accounting for the 68Ga-DOTATATE signal.
The best way to identify the cellular target of the 68Ga-DOTATATE PET/CT is to perform SSTR protein analysis in vitro on corresponding tissue samples, preferably with receptor autoradiography. Indeed, previous studies have shown an excellent correlation between in vitro and in vivo receptor data in SSTR-positive tumors. 28 The problem with DPLD, in comparison with tumors, is twofold: (1) poor availability of adequate fresh tissue for analysis; in the present study, fresh tissue was available from only 1 of the 26 cases; (2) histologically, the tissue in DPLD is made up of several different cell types, in contrast to tumors in which one cell type dominates. This makes it harder to identify the cell type responsible for the signal in DPLD. SSTR autoradiography 29 was performed in a single DPLD case in this investigation (data not shown) but did not reveal measurable SSTR levels, and SSTR immunohistochemistry with two different antibodies was also negative. 30 However, this sample was characterized by very few inflammatory cells, extensive fibrosis, and very few small vessels (despite numerous large vessels). As such, it may not have been a representative sample; therefore, it is impossible to draw a definitive conclusion.
SSTR2 expression has been found in both murine fibroblasts following bleomycin-induced pulmonary fibrosis and fibroblasts from patients with IPF. 16 Lebtahi and colleagues found some binding of labeled octreotide to lung fibroblasts from a patient with IPF compared to normal controls, but it was actually the blood vessels that contributed most to the autoradiographic signal. 17 Their results point to an intriguing possibility: SSTR2 and SSTR5 are preferentially expressed in proliferating human endothelium, 31 and perhaps the positive signal is coming from neovascularization around the fibrotic areas, and there is increased vascular density at the edges of the fibrotic regions. 32 In fact, the signal may be related to nonspecific factors such as increased vascular pool per se.
When performing radionuclide imaging of DPLD, it is possible to use the conventional gamma camera studies with the somatostatin analogue 111In octreotide. 28 However, the spatial resolution and sensitivity are inferior to those of PET; thus, quantification of disease response would be poor. 33 Imaging with 68Ga-DOTATATE PET has specific advantages over 18F-FDG PET; these include significant reduction in the radiation exposure, 34 no requirement either for pre-examination fasting or immobilization of the patient during the uptake period, and no dependency of a cyclotron as 68Ga is a generator product. 68Ga-DOTATATE PET shows clinical potential given that even with small numbers, there was a moderate relationship between pulmonary tracer uptake and TLCO, although the relationship was weaker than with 18F-FDG.
Study limitations include the heterogeneity of the study population; however, this enabled us to obtain PET data for more than one HRCT pulmonary parenchyma pattern. However, the two main groups (IPF and NSIP) had population sizes too small to perform routine statistical analysis. There are many PET/CT technical considerations, such as correcting for density and respiratory motion, which have been covered elsewhere. 9 It may have been ideal to have lung biopsies in all patients, but in keeping with guidelines, these were performed only when indicated. 2 Nonetheless, a tissue diagnosis was available in some patients.
This prospective study presents novel PET/CT data in patients with DPLD with a somatostatin analogue in comparison with the uptake to that of 18F-FDG. In all DPLD patients, a disease signal was identified on PET. This signal mirrored the distribution of lung parenchymal abnormality, which had a pattern of tracer uptake similar to that on the 18F-FDG studies. We provide noninvasive in vivo evidence in humans showing that SSTRs may be detected in the lungs of patients with DPLD. Further studies are needed to characterize the cells and pathways in DPLD that are responsible for this signal.
Footnotes
Acknowledgment
Financial disclosure of authors: This work was undertaken at University College London Hospital/University College London, which received a proportion of the funding from the United Kingdom's Department of Health's National Institute for Health Research Biomedical Research Centers funding scheme. A proportion of the funding was received from the Royal College of Radiologists (UK).
Financial disclosure of reviewers: None reported.