
Abstract
The purpose of this study was to standardize therapy monitoring of hepatic metastases from gastroenteropancreatic neuroendocrine tumors (GEP-NETs) during the course of somatostatin receptor radionuclide therapy (SRRT). In 21 consecutive patients with nonresectable hepatic metastases of GEP-NETs, chromogranin A (CgA) and 68Ga-DOTATOC PET/CT were compared before and after the last SRRT. On 68Ga-DOTATOC PET/CT, the maximum standard uptake values (SUVmax) of normal liver and hepatic metastases were calculated. In addition, the volumes of hepatic metastases (volume of interest [VOI]) were measured using four cut-offs to separate normal liver tissue from metastases (SUVmax of the normal liver plus 10% [VOIliver+10%], 20% [VOIliver+20%], 30% [VOIliver+30%] and SUV = 10 [VOI10SUV]). The SUVmaxof the normal liver was below 10 (7.2 ± 1.3) in all patients and without significant changes. Overall therapy changes (Δ) per patient (mean [95% CI]) were statistically significant with p < .01 for ΔCgA = −43 (−69 to −17), ΔSUVmax = −22 (−29 to −14), and ΔVOI10SUV = −53 (−68 to −38)% and significant with p < .05 for ΔVOIliver+10% = −29 (−55 to −3)%, ΔVOIliver+20% = −32 (−62 to −2) and ΔVOIliver+30% = −37 (−66 to −8). Correlations were found only between ΔCgA and ΔVOI10SUV (r = .595; p < .01), ΔSUVmax and ΔVOI10SUV (0.629, p < .01), and SUVmax and ΔSUVmax (r = .446; p < .05). 68Ga-DOTATOC PET/CT allows volumetric therapy monitoring via an SUV-based cut-off separating hepatic metastases from normal liver tissue (10 SUV recommended).
The purpose of this study was to standardize therapy monitoring of hepatic metastases from GEP-NETs by somatostatin receptor positron emission tomography/computed tomography (PET/CT).
Patients and Methods
Patients
Twenty-one consecutive patients (12 males, 9 females) aged 25 to 87 years (mean ± SD 61 ± 13 years) who underwent 52 SRRTs in nonresectable hepatic metastases owing to GEP-NETs were included in this retrospective study performed at the University Hospital of Dresden. The trial was approved by the local ethics committee.
PET/CT and Laboratory Values
On the same day, 68Ga-DOTATOC PET/CT was performed and laboratory values, including plasma chromogranin A (CgA), creatinine, hemoglobin, and thrombocyte count, were obtained within 1 month before and 3 months after SRRT.
PET/CT was performed on a 16-slice PET/CT scanner (Biograph 16, Siemens Medical Solutions, Forchheim, Germany) 50 ± 12 minutes after injection of 136 ± 36 MBq 68Ga-DOTATOC. The radiopeptide was produced in-house using a 68Ge/68Ga generator and 14 nmol (20 μg) DOTATOC (BACHEM, Switzerland, Bubendorf). The labeling and purification method is described elsewhere. 21
Imaging included low-dose (< 1 mSv) CT (10 mAs, 120 kV, 16 × 1.5 mm collimation, 0.42 s tube rotation time, 86 mm/s table feed, 3 mm reconstruction increment) performed in shallow respiration for attenuation correction followed by a PET scan in three-dimensional mode with iteratively reconstructed slices of 3 mm.
Therapy
SRRT was performed using the radiopeptide yttrium 90 DOTATOC or lutetium 177 DOTA-TATE intravenously administered in a dosage of 4.3 ± 0.5 GBq (range 2.6–5.2 GBq).
For renal radiation protection, an infusion of 2,000 mL of an amino acid solution (lactated Ringer solution [Proteinsteril, B. Braun Medical AG, Sempach, Germany], HEPA 8%, Mg 5-Sulfate [B. Braun Medical AG]) was given to inhibit tubular reabsorption of the radiopeptide. Infusion started 30 minutes before and continued up until 4 hours after administration of the radiopeptide.
Most patients underwent several SRRTs, as follows: 6, 3, 9, 1, and 2 patients underwent 1, 2, 3, 4, and 5 SRRTs, respectively. The interval between therapies averaged 5 ± 2 months.
Measurements on PET/CT Images
On PET/CT, maximum standardized uptake values (SUVmax) for both the normal liver tissue and the hepatic tumor burden (hepatic metastases) were measured. In addition, on PET, the total PET-avid (functional) hepatic tumor volume was measured in relation to an SUV threshold that determines which volumetric pixel (voxel) counts as “malignant.” For this purpose, on CT images, the liver was extracted (segmented) by manually drawing polygons around the liver, which were copied and adjusted slice by slice. Within the CT-defined liver volume, the total PET volume of hepatic metastases was calculated by adding hepatic PET voxels with an SUVmax above a threshold that was supposed to separate normal liver tissue from metastases. As referent threshold, the constant (SUV = 10) threshold and the liver-dependent thresholds (SUVmax of the normal liver plus 10%, 20%, and 30%) were used. Thereby, four volumes of interest (VOI) were defined: VOI10SUV, VOIliver+10%, VOIliver+20%, and VOIliver+30%.
Statistical Analysis
Baseline values and their changes (Δ = [post-pre]/pre%) for CgA, PET values, and nephro- and myelotoxicity monitoring were correlated using the Pearson and Spearman coefficients for normal and nonnormal distributed variables, respectively. Using the one-sample-t-test, we determined if the relative changes (Δ) were significantly different from no change (Δ = 0%). A level of p = .05 was used to indicate statistical significance.
Results
The changes per patient are displayed in Table 1 and summarized in Table 2. CgA was elevated in all patients (range 33–5,510 U/L) (see Table 2). The SUVmax for normal liver was relatively constant and in all cases was under the cut-off of 10 SUV, rendering it optimal for separating metastases (SUVmax = 25.0 ± 12.2) from normal liver tissue (SUVmax = 7.2 ± 1.3). There was no correlation between baseline CgA and all tested PET values.
Indices for Therapy Monitoring

CgA = chromogranin A; SUVmax = maximum standard uptake value; PET = positron emission tomographic; VOI = PET volume of hepatic tumor burden in relation to the threshold of the confining isocontour (10 SUV, maximum liver SUV plus 10%, 20%, and 30%).
Accumulative dose.
Baseline Values and Their Changes

Δ = (post-pre)/pre).
Volume of interest (PET volume of hepatic tumor burden) confined by an isocontour defined by the threshold 10 SUV (VOI10SUV) and the liver-dependent thresholds: SUVmax of normal liver tissue plus 10% (VOIliver+10%), 20% (VOIliver+ 20%), and 30% (VOIliver+30%).
Fourteen of 21 patients showed a reduction after one therapy (Figure 1 and Figure 2). But changes were more significant, considering all therapies and comparing the last PET with the baseline PET (Figure 3 and Figure 4). Changes were significant (p < .01) for ΔCgA, ΔSUVmax, ΔVOI10SUV, Δhemoglobin, and Δthrombocyte count and not significant (p > .01) for ΔVOIliver+10%, ΔVOIliver+20%, ΔVOIliver+30%, and Δcreatinine (see Table 2).
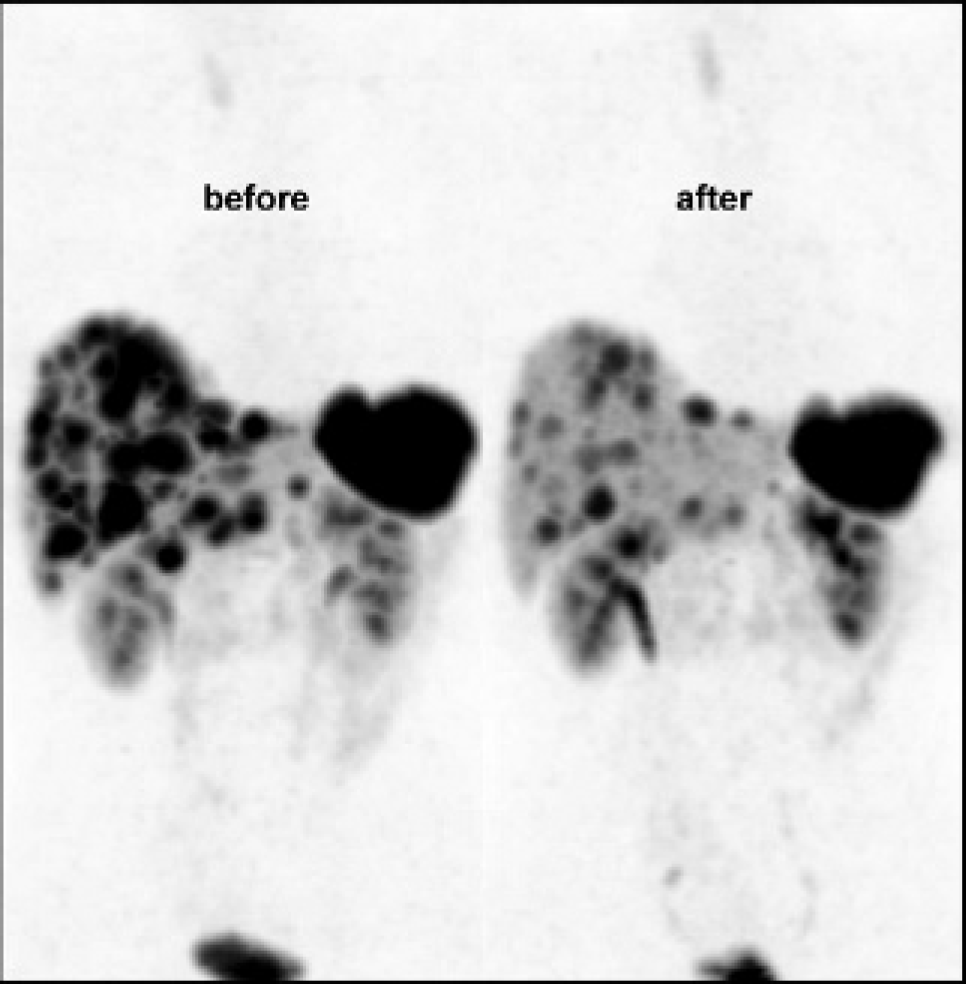
PET monitoring of somatostatin receptor radionuclide therapy in a 38-year-old patient with a resected pancreatic neuroendocrine tumor. Response after one therapy: ΔCgA = −6%, ΔSUVmax = −31%, ΔVOI10SUV = −87%, ΔVOIliver+10% = −88%, ΔVOIliver+20% = −90%, ΔVOIliver+30% = −90%.
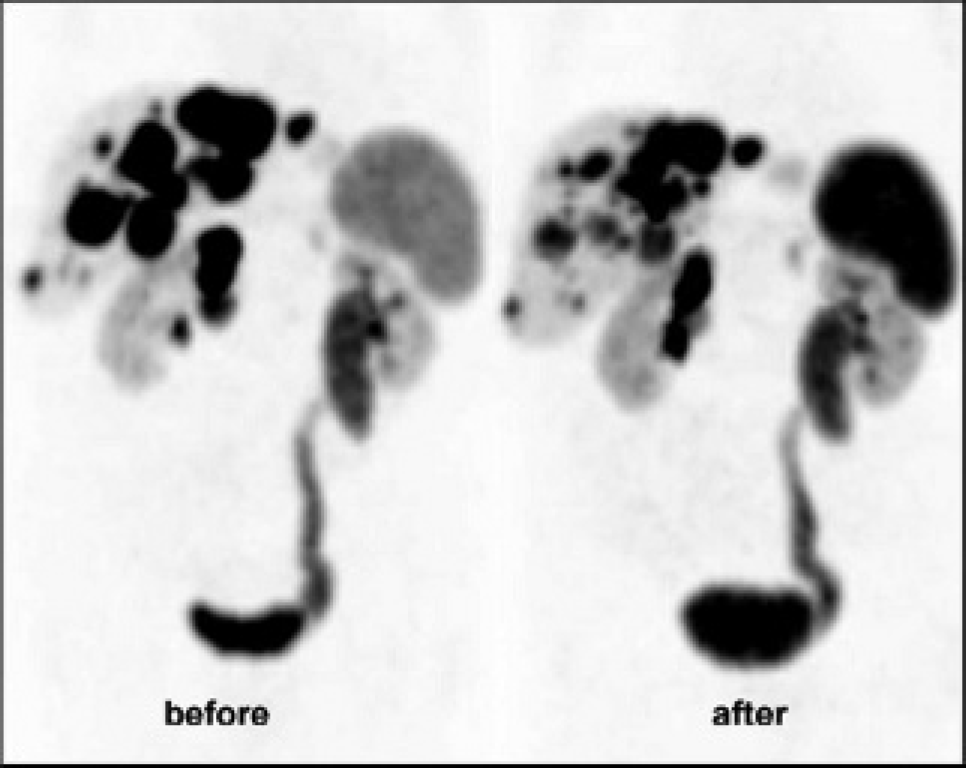
PET monitoring of somatostatin receptor radionuclide therapy in a 74-year-old patient with a pancreatic neuroendocrine tumor. Response after one therapy: ΔCgA = −9%, ΔSUVmax = −39%, ΔVOI10SUV = −36%, ΔVOIliver+10% = −47%, ΔVOIliver+20% = −49%, ΔVOIliver+30% = −50%.
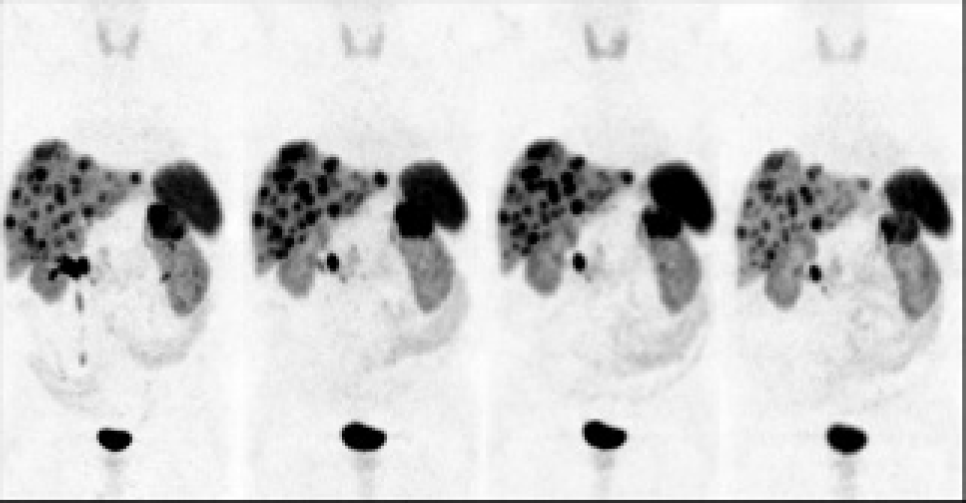
PET monitoring of somatostatin receptor radionuclide therapy in a 62-year-old patient with a resected pancreatic neuroendocrine tumor. Response after three therapies: ΔCgA = −54%, ΔSUVmax = −15%, ΔVOI10SUV = −41%, ΔVOIliver+10% = −30%, ΔVOIliver+20% = −24%, ΔVOIliver+30% = −21%.
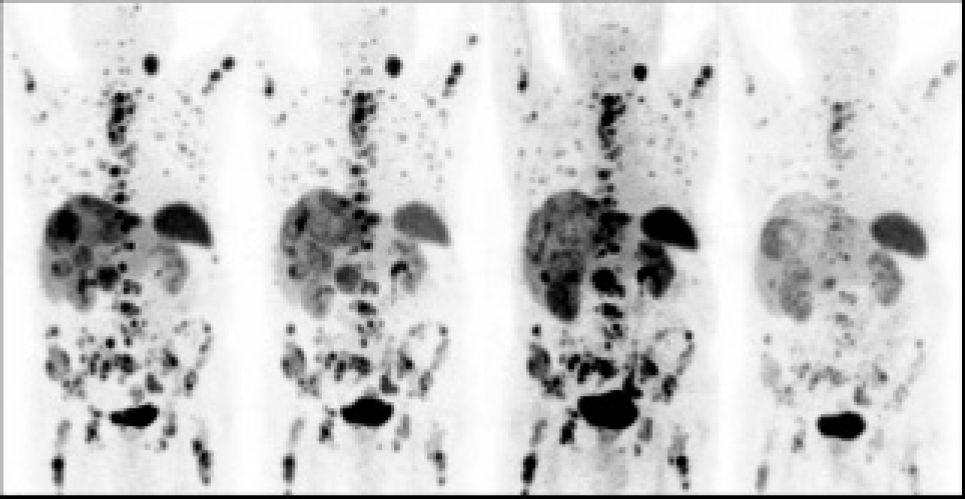
PET monitoring of somatostatin receptor radionuclide therapy in an 87-year-old patient with liver, lymph node, and bone metastases of a neuroendocrine tumor of unknown origin. Response after three therapies: ΔCgA = −81%, Δ|SUVmax = −58%, ΔVOI10SUV = −97%, ΔVOIliver+10% = −87%, ΔVOIliver+20% = −88%, ΔVOIliver+30% = −91%.
Correlations were found only between ΔCgA and ΔVOI10SUV (r = .595; p < .01), ΔSUVmax and ΔVOI10SUV (r = .629; p < .01), Δhemoglobin and Δthrombocyte counts (r = .468; p < .05), and SUVmax and ΔSUVmax (r = −.446; p < .05).
Discussion
GEP-NET is a rare and heterogeneous disease whose prognosis and therapy response are variable. 5 Thus, therapy monitoring and follow-up are necessary, especially in cases where therapies can provoke potential side effects.
Monitoring of Therapy Response
Currently, the assessment of therapy response is based on a unidimensional measurement (diameter) scoring procedure according to which therapy results are classified in four categories: progressive disease, stable disease, partial response, and complete response (Response Evaluation Criteria in Solid Tumors [RECIST] criteria). 22 Often, the classification of the unidimensional measurements cannot match the categorization according to the RECIST criteria, resulting in a loss of information. Therefore, a three-dimensional (volumetric) measurement is more desirable, enabling a reproducible and continuous quantification of the response. With 68Ga-DOTATOC PET/CT, the nature, tumor burden, and therapy response of GEP-NETs can be evaluated in vivo based on the expression of somatostatin receptors (SUVmax) and their volume (eg, VOI10SUV). In addition, the dynamics of the receptor expression and volume can be reliably and precisely measured, providing information on growth rates—similar to prostate specific antigen velocity. SUV is standardized, and volumetric PET measurements can be automated owing to the high contrast between normal liver tissue and metastases (see Figures 1 to 4). The PET volumetry is based on the addition of “malignant” voxels with an SUVmax above a cut-off. The precision of the measurement is given by the voxel resolution (field of view [FOV]/matrix size [512] × FOV/ matrix size [512] × CT reconstruction increment), which is 0.8 × 0.8 × 3 mm for 40 cm patient diameter (FOV) and 3 mm reconstruction increment. In CT, the liver to metastases contrast is too low and too noisy for a voxel-based segmentation (volumetry) and for standardization and too dependent on the timing of the individual contrast phase.
However, despite the high PET contrast between normal tissue and GEP-NET metastases, there is no PET definition for quantifying therapy response. 23 Currently, SUVmax is usually used as a follow-up parameter—possibly because it mostly correlates with the degree of malignancy. 24 Furthermore, it is easily measurable and reproducible and does not need any threshold for separating normal liver tissue from metastases. In 18F-FDG PET/CT, the SUVmax reflects the most metabolically active part of the tumor. This part is most “biologically” relevant and possibly also more predictive of outcome than the volume. But in contrast to 18F-FDG PET/CT, the SUVmax in 68Ga-DOTATOC PET/CT exclusively reflects the maximum receptor overexpression, yielding no information on metabolism, volume, or growth rate.
Based on the above, volumetric PET values could show therapy response, whereas SUVmax remains constant, thereby underestimating therapy response. In our work, therapy response was found to be underestimated when using the SUVmax parameter for therapy monitoring instead of CgA or volumetric PET values (see Figures 1, 3, and 4).
Another method to monitor therapy response in a digital format is the measurement of specific or nonspecific biochemical markers of GEP-NETs. Among the nonspecific markers (serotonin, neuron-specific enolase, carcinoembryonic antigen, and urinary 5-hydroxyindole-3-acetic acid), CgA is considered the most reliable biomarker reflecting the clinical evolution of NETs. 25 CgA levels were found to correlate with tumor burden26,27 and recommended as more specific in the follow-up of such tumors. 28 In our study, no correlation between baseline CgA and volumetric PET values could be observed, suggesting that the CgA value might not reflect a tumor burden. In the detection of GEP-NETs, 111In octreoscan was shown to be superior to CgA.29–31 It has been reported that 68Ga-DOTATOC PET/CT might be more sensitive than 111In octreoscan32,33 and accordingly leading to the suggestion that CgA levels show less suitability for therapy monitoring compared to 68Ga-DOTATOC PET/CT in the detection of GEP-NETs. Thus, the less sensitive CgA also appears to be less suitable for therapy monitoring than 68Ga-DOTATOC PET/CT (see Figure 1). To our knowledge, there are no studies comparing CgA and 68Ga-DOTATOC PET/CT for therapy monitoring of GEP-NETs. However, follow-up 68Ga-DOTATOC PET/CT is required if it needs to be decided if the receptor density is sufficient to continue somatostatin receptor-mediated therapies.
The continuously quantified change in volume is summarized in Table 2. For VOI10SUV, the mean decrease (95% CI) in volume was 53 ± 33 (38–68). Using World Health Organization (WHO) categories, this translates to a response (ΔVOI10SUV > 50%) in 13 of 21 patients (62%). These results are similar to those of transarterial chemoembolization (TACE) 9 and SRRT. 17 Although Roche and colleagues reported a response rate of 74% with TACE (12% higher than SRRT in these studies), 9 a comparison between them cannot be done because of different parameters used for therapy monitoring.
Owing to the accumulative effect of radiation and chemotherapy, the time point for response assessment is crucial. However, the continuous character of a volumetric index enables normalization, for example, to the baseline volume, time (change/per time = velocity), dosage, or number of interventions, thereby facilitating the comparison between therapies, for example between intravenous and intra-arterial SRRT or between SRRT and SIRT. The volumetric character of the entire hepatic tumor burden is naturally more precise for assessing therapy response than the sum of diameters (RECIST) or the sum of the products of perpendicular diameters (WHO) of selected indicator lesions.
The WHO's response classification does not allow for normalizing responses to depict therapy efficacy more precisely. Also, for dynamic studies, the volumetric index of the tumor burden is naturally more precise than a unidimensional diameter of selected indicator lesions. Thus, 68Ga-DOTATOC PET/CT should be used for volumentric therapy monitoring.
In a diffuse infiltrated liver, it is difficult to determine the SUVmax of normal liver tissue. Thus, it is easier to use an absolute cut-off, which is independent of the individual SUVmax in a normal liver, for separating metastases from normal liver tissue. In addition, only the liver-independent volumetric changes were as significant as the changes in CgA and SUVmax (see Table 2).
Predictive Criteria for Therapy Response
Generally, the malignant potential of GEP-NETs and their response to therapy are difficult to predict. Negative prognostic factors include intact primary tumor, pancreatic site of origin, extensive liver metastases, bone metastases, a poor degree of tumor cell differentiation, and a high Ki-67 proliferative index.34,35 However, most authors agree that the most common cause of death in patients with GEP-NETs is hepatic failure from tumor progression and that extra hepatic metastatic disease has no significant effect on the outcome.
Given that 68Ga-DOTATOC PET/CT visualizes the density and anatomic distribution of somatostatin receptors, it can be simultaneously used to pretest if the expression of somatostatin receptors is sufficient for receptor-mediated radiation therapy. So far, parameters or cut-offs remain undefined for triggering the SRRT procedure. However, in our study, it was shown that the maximum baseline density of receptors reflected by the SUVmax correlates with the change in SUVmax (r = –.446; p < .05) rendering SUVmax as the only prediction index for response to SRRT.
Besides the maximum receptor density (SUVmax), the high vascularity of hepatic metastases is associated with a better prognosis and response to therapy.36,37 This suggests that local (selective) application increases the therapeutic efficacy and should be preferred over systemic application as recommended by McStay and colleagues and Limouris and colleagues.16,17 In the study by McStay and colleagues, the subgroup of patients (n = 9) who underwent concurrent polyvinyl alcohol particle embolization at the same time as 90Y-DOTA-lanreotide administration had a better tumor response rate than the patients (n = 14) who underwent 90Y-DOTA-lanreotide only. 16 Thus, the selective application—in combination with the cessation of the blood supply through embolization—might explain the success of selective TACE.10,36,38 Therefore, TACE has been recommended as first-line and, eventually, exclusive treatment. 9 Owing to the lack of contrast administration, we could not investigate the influence of the blood supply and vascularity of the hepatic metastases on the therapy response. However, this study shows that systemic SRRT is effective. When intravenously administered, about 30% of the injected activity is lost in the urine within the first few hours and does not contribute to the therapy. Thus, increased efficacy can be increased if the SRRT is directly delivered to the hepatic metastases through intra-arterial infusions, as seen in octeotride16,17 and MIBG therapies. 12
Side Effects
If SRRT is intravenously administered, a substantial proportion of the dose dissipates within the systemic circulation, reducing the amount of agent that reaches the target and increasing radiation exposure to kidneys and bone marrow. Radiation-mediated nephrotoxicity and myelosuppression can also be an issue,16,39 depending on the radioisotope applied. De Jong and colleagues reported the development of a myelodysplastic syndrome in 7.5% of patients with different types of somatostatin receptor-positive tumors. 40 A minor increase in creatinine of 10 ± 40% was observed, but a more significant decrease in hemoglobin (14 ± 9 [10–19]%) and thrombocyte counts (26 ± 23 [15–38]%) (see Table 1). There was no correlation between the changes in hemoglobin and creatinine, so damage to the kidney with consecutive reduction in the release of erythropoietin cannot explain the anemia observed. No correlation was depicted between hemoglobin or thrombocyte counts and volumetric PET values—neither for the baseline values nor for the changes. This makes a tumor volume-associated (paraneoplastic) anemia unlikely. Given that the changes in hemoglobin parallel the changes in thrombocyte count, this might suggest a myelotoxic effect. Therefore, a selective intra-arterial administration of SRRT should be preferred to increase efficiency and decrease side effects.16,17
Limitations
We could not correlate the changes in PET with the survival rate because all patients were still alive at the end of the study. Owing to the diffuse character of the hepatic metastases and lack of contrast media in CT, we could not determine a diameter (RECIST criteria, nonmeasurable disease). We could not correlate PET changes and morphologic changes according to the WHO criteria.
Conclusion
The monitoring of an in vivo GEP-NET therapy response is achieved using 68Ga-DOTATOC PET/CT, based on the nature and tumor burden and assessed by means of the expression of somatostatin receptors (SUVmax) and their volume (VOI10SUV). SUV can be standardized and volumetric PET measurements can be done owing to the high contrast between normal liver tissue and metastases. Furthermore, the dynamics of the receptor expression and volume can be reliably and precisely measured, providing valuable information on growth rates.
68Ga-DOTATOC PET/CT allows volumetric therapy monitoring via a recommended 10 SUV based cut-off, separating hepatic metastases from normal liver tissue.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.
The PET/CT scanner in Dresden was financed by the German Federal Ministry of Education and Research (BMBF).