
Abstract
The field of biomedical optics has matured rapidly over the last decade and is poised to make a significant impact on patient care. In particular, wide-field (typically > 5 cm), planar, near-infrared (NIR) fluorescence imaging has the potential to revolutionize human surgery by providing real-time image guidance to surgeons for tissue that needs to be resected, such as tumors, and tissue that needs to be avoided, such as blood vessels and nerves. However, to become a clinical reality, optimized imaging systems and NIR fluorescent contrast agents will be needed. In this review, we introduce the principles of NIR fluorescence imaging, analyze existing NIR fluorescence imaging systems, and discuss the key parameters that guide contrast agent development. We also introduce the complexities surrounding clinical translation using our experience with the Fluorescence-Assisted Resection and Exploration (FLARE™) imaging system as an example. Finally, we introduce state-of-the-art optical imaging techniques that might someday improve image-guided surgery even further.
The unmet clinical need in surgery stems from the fact that visible light cannot penetrate into blood and tissue more than a few hundred microns owing to high photon attenuation from absorbance and scatter. Thus, when a surgeon looks at the surgical field, he or she only sees surface features. The implications of this are significant because over 40 million surgical procedures are performed in the United States each year, and even small improvements in outcome, or reductions in morbidity, will affect large patient populations. For example, with modern surgical techniques, 20 to 25% of breast cancers are still resected incompletely,2,3 and local recurrence remains unacceptably high at 12 to 28%. 4 Moreover, nerve damage during many types of surgery, resulting in postsurgical neuralgia and loss of function, occurs in 20,000 to 600,000 patients per year in the United States alone. 5 Being able to see structures that need to be resected, such as malignant cells, and structures that need to be avoided, such as blood vessels and nerves, is a profound unmet clinical need.
One relatively new technology that has the potential to guide surgeons in real time is the use of invisible near-infrared (NIR) fluorescent light within the “NIR window” of 700 to 900 nm. 6 Within this NIR window, the absorption of most biomolecules (ie, deoxyhemoglobin, oxyhemoglobin, water, and lipid) reaches local minima, scattering is relatively low, and tissue autofluorescence is relatively low. Thus, photon penetration into and out of tissue is relatively high (on the order of several millimeters), and the addition of exogenous NIR fluorophores produces “bright stars on a black background” or, more formally, a high signal to background ratio (SBR). Given that NIR fluorescent light is essentially invisible to the human eye, special imaging systems are required to excite the NIR fluorophore(s) within the surgical field and to collect emitted photons. Well-designed NIR fluorophores are needed to highlight the specific structures desired by the surgeon. Finally, training tools are needed to train surgeons how to use the technology. This latter issue has been addressed elsewhere and is not discussed further. 7
Recognizing the potential of optical imaging in general and NIR fluorescent light in particular to improve human surgery, the Cancer Imaging Program of the National Cancer Institute, the National Institute of Biomedical Imaging and Bioengineering, and the National Science Foundation have invested heavily in these technologies over the last decade. As described in this review, the return on this investment has been rather rapid preclinical validation, first-in-human clinical trials, and now commercial availability of NIR fluorescence imaging systems for image-guided surgery. NIR fluorophore development is proceeding at a slower pace but is also on target for clinical translation in the near future. This review details the key issues surrounding the development and clinical translation of continuous wave (CW), reflectance NIR fluorescence image-guided surgery systems and their associated NIR fluorophores in the hope of establishing a strong foundation on which the field can build the next generation of advances.
NIR Imaging Systems
Principles of Operation
NIR diffuse optical imaging takes advantage of the deep photon penetration of NIR light into living tissue to provide fast, quantitative, relatively inexpensive imaging of endogenous and/or exogenous contrast at depths < 1 cm.8,9 Within this field, NIR fluorescence imaging focuses on the detection of exogenous contrast agents that emit fluorescence between 700 and 900 nm. The typical fluorescence imaging system has been described in detail in various publications.10–15 Briefly, it consists of a spectrally resolved light source (filtered broadband source, light-emitting diode [LED], or laser diode) exciting a fluorophore within a turbid medium. The light emitted from this fluorophore is then imaged onto a charge-coupled device (CCD) camera, with special care taken to filter out the powerful excitation light.
Key Design Parameters
Although conceptually simple, virtually every design parameter will impact system performance and thus SBR.
Field of View
An adjustable field of view (FOV) is mandatory for surgical imaging and can be accomplished using either zoom or fixed magnification lensing (see below). In general, maximum FOV should be at least 10 cm (≈4 inches) in diameter and preferably 20 cm (≈8 inches) in diameter to accommodate various surgical applications. For resection of small tumors or avoidance of thin nerves, a minimum FOV should also be defined, preferably in the range of 1 to 2 cm. The major tradeoffs with FOV are excitation fluence rate, collection optics, and final resolution. The larger the maximum FOV, the more total power will be required by the light source, the higher the magnification will be needed to achieve the desired minimum FOV, and the lower the final resolution will be because the CCD camera(s) will have a finite number of pixels.
Fluorescence Excitation Light Source
Three major technologies are capable of producing light for excitation of NIR fluorophores: filtered broadband sources, LEDs, and laser diodes. The choice is not straightforward because each has advantages and disadvantages, as follows.
Filtered Broadband Sources. The overriding problem is efficiency. Most of the photons produced by the source are discarded to filter excitation light to a narrow enough band, and in most cases, excessive heat is produced that must be dissipated. These sources also have a relatively large solid angle, meaning that only a small fraction of the optical power propagates toward the surgical field. 10 Concentrating optical power inside light guides using mirrors and lenses is also difficult. Because of these issues, there are few applications in image-guided surgery where broadband sources would be optimal.
Light-Emitting Diodes. LEDs provide a good compromise between power (tens of mW each), spectral confinement (typical full-width at half maximum [FWHM] < 50 nm), efficiency, and cost. Moreover, their use in consumer markets has resulted in steady improvements in performance and reductions in package size. Working with LEDs for surgical imaging, however, can be challenging, and an in-depth discussion was recently published. 16 The key points are that heat dissipation is a major challenge for dense arrays, an excitation filter must be used to reduce the spectral FWHM, collimators must be used on each LED to restrict solid angle to the acceptance angle of the excitation filter (if needed), and lensing (either inherent to epoxy LEDs or external) must be used to concentrate optical power within the FOV.
Laser Diodes. Laser diodes are the most confined, spatially and spectrally, but can be difficult to integrate, are expensive at high power, and can trigger safety concerns related to maximal permitted exposure (MPE) and the need for personal protective equipment such as laser goggles. Laser diodes also require precise control in current and in temperature (using a proportional-integral-derivative feedback control loop) as temperature variations induce changes in wavelength and high temperatures reduce the lifetime of the diode. Recently, NIR diodes in the 1 to 2 W range have become available, although not every wavelength is available in high-power packages. In some situations, a major problem with coherent sources such as laser diodes is speckle, which may have to be removed prior to illuminating the surgical field by either rotating a diffuser or vibrating a fiber at frequencies much higher (typically 10 times) than the camera frame rate.
The two strategies for illuminating a surgical field with a light source are local and remote. Local lighting is placed immediately above the patient and can be achieved with all three sources. However, this requires high-power consumption in the imaging head, power loss in transmission lines, and introduction of potential radiofrequency noise from light source controllers. LEDs can be an excellent choice for local lighting. 16 Remote lighting employs a light guide to illuminate the field using a remote source. At the present time, laser diodes are the only reasonable solution for remote lighting because of the large solid angle of broadband and LED sources, resulting in poor light guide coupling efficiency and difficulty in achieving high fluence rates over large FOVs. With respect to light guides, fiber-based guides can offer high transmissivity over long distances and small bending radii compared to liquid light guides, and the latter also have a relatively high numerical aperture (typically > 0.5) and are sensitive to heat and mechanical manipulation.
NIR Excitation Fluence Rate (Irradiance)
As discussed below, small-molecule organic fluorophores typically undergo irreversible photobleaching when the excitation fluence rate is > 50 mW/cm2.17,18 Higher fluence rates also run the risk of heating tissue and causing thermal damage. An “adequate” fluence rate for a particular application depends on whether the fluorophore is embedded deep in tissue (highest fluence rate possible required), the f-number (f/#) of the collection optics, and the sensitivity of the CCD camera. The lowest possible fluence rate necessary to achieve NIR fluorescence emission in the middle range of the CCD camera, at its maximal frame rate, should be employed. Although this value will also depend on the concentration of the NIR fluorophore, in general, the fluence rate should be adjustable to accommodate all possible clinical scenarios. In all cases, care must be taken to limit MPE to the skin and the eyes to values defined in the International Electrotechnical Commission (IEC) standard #60825. For NIR wavelengths closer to the visible range, for example, 670 nm excitation, a maximally permitted fluence rate will also be limited by the changes induced in the color rendering index of the white light.
White Light Source
For simultaneous imaging of color video and NIR fluorescence emission using the Fluorescence-Assisted Resection and Exploration (FLARE™, contact Dr. Frangioni for availability) imaging system,15,16 it is important to filter “white” light to 400 to 650 nm. This produces effective isolation of the color video channel from the two NIR fluorescence channels. This is an important point because most surgical luminaries emit significant amounts of light above 650 nm. Two regulatory guidelines from the IEC standard #60601 then come into play. The first is that the minimum central luminance of the surgical field must be at least 40,000 lux at the typical working distance (WD). The second is that the color temperature must be between 3,000 and 6,700 K with a color rendering index ⩾ 85. The latter ensures that the surgical field is not preferentially “tinged” with one or more visible colors. Most filtered broadband and LED white light sources can be used for providing white light to the surgical field using local approaches. Supercontinuum laser sources, which are currently cost prohibitive and relatively low power, may someday be a robust solution for remote illumination.
Collection Optics
One of the most important components of the optical system is the lensing that relays white and NIR fluorescent emission light to the camera(s). There are multiple, complex tradeoffs among f/# (ie, amount of light transmitted by the system), depth of field, WD, and FOV that are beyond the scope of this review. In general, one can choose to employ macrozoom optics, optimized for a fixed WD, or fixed magnification optics, where the FOV decreases, but the excitation fluence rate increases as the imaging system is moved closer to the patient. Each choice has advantages and disadvantages, but both require special attention to chromatic aberration correction from 400 to 900 nm, minimization of distortion and vignetting, and parfocality is preferred to ensure that color video and NIR fluorescence images are in focus at all magnifications. It should also be noted that final system resolution may be diffraction limited or camera limited depending on f/# and lensing choices. For NIR fluorescent objects embedded below living tissue, the blur caused by scatter will far outweigh small deficiencies in system optics; however, resolution should always be as high as the data storage system can accommodate.
Cameras
Silicon-based CCD cameras are most commonly used for image-guided surgery but are not ideal. They suffer from low quantum efficiency (QE; typically ⩽ 25%) at 800 nm and relatively slow readout times (typically ≈15–30 fps) but do have low readout noise (⩽ 10 e− rms) when cooled and high resolution (512–1,324 pixels per dimension). An alternative is complementary metal oxide semiconductor (CMOS) sensors, which reduce size and power consumption and increase frame rate (⩾ 25 fps) but also have low QE and high readout noise. The newly introduced scientific CMOS (sCMOS) sensors appear to have all desired features, with readout noise < 3 e− and QE ≈33% at 800 nm, but remain expensive. Although not needed for qualitative imaging, pixel bit depths should be 10 to 12 bits for quantitative NIR fluorescence imaging. In general, noncooled silicon CCDs can achieve 10 bits and Peltier-cooled CCDs can achieve 12 bits. Finally, form factor is a concern in multicamera imaging systems, with cooled CCDs adding considerable size and weight.
Light Intensification
In some clinical scenarios, where NIR fluorescence emission collection is photon limited, light amplification using an image intensifier tube (IIT) might be needed. The most commonly used IIT is also used in military night vision systems and consists of a photocathode (PC), which converts photons into electrons, a single- or multistage microchannel plate (MCP), which accelerates electrons, and a phosphor screen (PS). Although currents are low (in the nA range), voltages are on the order of ≈–900 V for the PC to MCP input (ground), ≈1,000 V from MCP input to MCP output, and ≈4000 V from MCP output to PS. IITs add considerable cost to a system, tend to lower resolution, and if not cooled will add significant dark noise. If cooled, they are subject to condensation unless hermetically sealed.
Dichroic Mirrors and Filters
High-quality filters are essential for both excitation and emission light paths. Although absorption-type filters are inexpensive to make, they have poor out-of-band rejection and low transition slopes. The alternative is interference filters, with the state of the art being sputtered manufacturing techniques. A modern sputtered filter can achieve up to 98% transmission, extremely high blocking power (OD ⩾ 6), and high transition slopes. The main problems with sputtered interference filters are cost and some limitations with respect to extended spectral blocking ranges. Additionally, spectral characteristics vary greatly with incidence angle, and light should always strike the filter at normal incidence or be constrained to within a specified acceptance angle.
Data Display
A ⩾ 20-inch digital display monitor is typically used to provide the surgeon with real-time images, and screen resolution should be chosen to accommodate native camera(s) resolution. The FLARE™ imaging system actually has three monitors, two facing the technologist (one control, one image display) and one (image display) facing the surgeon. 15 Leakage current is the main concern with any monitor in the operating room, but using an isolation transformer can mitigate risk.
Software
Imaging system software should be written in a compiled language (eg, C++ or C#) for robustness. The data archiving structure should provide lossless compression. In most circumstances, metadata, for example, excitation fluence rates and camera exposure time, should be saved along with the image. In multicamera imaging systems, seamless camera streaming is a significant challenge and often requires the use of multicore processors and/or a graphical processing unit. Calibration sequences should be employed prior to the start of each surgery and can help correct for illumination inhomogeneities and lens distortion if present. Recent work by Themelis and colleagues also provides real-time light absorption correction. 14
Electrical Constraints
The entire imaging system must be compliant with relevant electronics standards, which in the United States is defined in IEC #60601, as well as institutional standards. The main considerations with respect to safety are redundant grounding, maintenance of total leakage current < 300 μA, and a maximum power consumption compatible with a standard 15A, 120 V plug.
Ergonomics
Ergonomics is a key to clinical acceptance. In general, operating room staff prefer small devices with great flexibility in positioning and multiple degrees of freedom of the imaging head. To ensure safety, cart-based imaging systems must also comply with minimum tilt standards.
Sterility
Because of the delicate nature of CCD cameras and electronics, it is typically not possible to sterilize the entire imaging head. As an alternative, a sterilized shield/drape combination15,16 can be attached to the imaging head under sterile conditions and used to cover the entire apparatus to within 18 inches of the floor.
Existing Intraoperative NIR Fluorescence Imaging Systems
Several complete intraoperative NIR fluorescence imaging systems are now available for preclinical and clinical studies (Table 1). The Novadaq SPY system (Mississauga, ON) (<http://www.novadaq.com>) is already approved by the Food and Drug Administration (FDA) for use during a variety of surgical procedures, including coronary artery bypass grafting, plastic and reconstructive surgeries, and organ transplantation, and is available in narrow [n] or wide [w] FOV models. Fluoptics' (Grenoble, France) (<http://www.fluoptics.com>) Fluobeam, Hamamatsu's (Hamamatsu City, Japan) (<http://www.hamamatsu.com>) Photodynamic Eye (PDE), and the Frangioni Laboratory's (Boston, MA) (<http://www.frangionilab.org>) FLARE™ imaging systems are presently available for experimental use and are also eligible for 510(k) approval based on Novadaq's predicate device.
All of these imaging systems use either laser diodes or LEDs at fluence rates usually in the range of 1 to 10 mW/cm2. Systems use 12-bit dynamic range CCD cameras (FLARE™, Mini-FLARE™, and Fluobeam) or 8-bit cameras (SPY and PDE). WDs and FOVs vary. The FLARE™15,16 and Mini-FLARE™ 19 systems (Figure 1) provide simultaneous color video and two independent channels (700 and 800 nm) of NIR fluorescence imaging.
Not listed in Table 1 are surgical microscopes equipped with NIR fluorescence modules, such as the Zeiss INFRARED 800 (Oberkochen, Germany) and Leica FL800 (Heerbrugg, Swizterland). Although widely used in neurosurgical applications, these systems are not optimized for deep tissue imaging owing to the use of broadband sources, which result in a relatively low excitation fluence rate at large WDs or large FOV. Nevertheless, the Zeiss Pentero microscope with the INFRARED 800 module is in compliance with the requirements of the European Medical Device directive 93/42/EEC. The Leica M720 microscope with the FL800 module has received FDA 510(k) clearance for heart, plastic, and neurosurgery.
Near-Infrared Fluorescence Imaging Systems Available for Preclinical and Clinical Studies

FDA = Food and Drug Administration; FOV = field of view; LED = light-emitting diode; [n] = narrow FOV model; [w] = wide FOV model.
Contact Dr. Frangioni for availability.

FLARE™ and Mini-FLARE™ Image-Guided Surgery Systems. The FLARE™ imaging system is composed of a cart containing control electronics, a cooling unit, and a computer; an articulating arm providing 6 degrees of freedom, 127 cm lateral reach, and 178 cm vertical reach; and an imaging head containing a custom high-power LED light source, two NIR and one color camera, and custom optics. 15 The Mini-FLARE™ imaging system 19 represents a significant reduction in size and improvement in flexibility.
NIR Fluorescent Contrast Agents
Now that a variety of intraoperative NIR fluorescence imaging systems are available or are about to be available commercially, the development of effective NIR fluorescent contrast agents becomes of paramount importance. A general difficulty in effecting NIR absorption and emission in small molecules is the required number of double bonds. In general, 7 to 10 double bonds are required to reach wavelengths of ≈700 nm, and 9 to 12 doubles bonds are required to reach ≈800 nm, with the range dependent on the influence of nearby chemical substituents. Not only does each double bond increase molecular weight, but it also increases the hydrophobicity of the fluorophore. Thus, a core chemical structure that absorbs and emits in the NIR (Figure 2A) is necessarily relatively large and hydrophobic, which presents special problems for in vivo imaging (discussed below), including poor aqueous solubility, nonspecific uptake in normal tissues and organs, and exclusion by the blood-nerve-barrier (BNB) and blood-brain-barrier (BBB).
In addition to small molecules, various nanoparticle (NP) systems that generate NIR absorption and emission, including dendrimers, molecular dots, and quantum dots, have been described. Because the preclinical development and clinical translation of NIR fluorescent NPs are extremely complex, our group has recently reviewed this topic elsewhere. 20

Contrast agents for NIR fluorescence-guided surgery. A, General structure of the heptamethine indocyanine class of NIR fluorophores. B, Chemical structures and key optical properties (in serum) of the clinically available NIR fluorophores methylene blue and indocyanine green.
In the following section, we discuss the physicochemical, optical, targeting, and in vivo properties of NIR fluorescent contrast agents, which are either used clinically now or have the potential for clinical translation in the near future. The physicochemical and optical properties of commonly used NIR fluorescent small-molecule NPs are detailed in Table 2. The reader is also encouraged to read excellent recent reviews on this subject.21–24
Physicochemical and Optical Properties
Chemical Structure and Molecular Weight
Even though a relatively large number of double bonds are required to reach the NIR, some compact chemical structures have been described in the literature, including methylene blue (MB), which can reach ≈700 nm emission with a molecular weight of only 320 Da (Figure 2B), and styryl pyridinium (FM) fluorophores, which can reach ≈800 nm emission with a molecular weight of only 612 Da. 25 The compact nature of the NIR fluorophore is important for keeping the final molecular weight after targeting ligand conjugation as low as possible. Compactness is also important for nerve targeting, where the molecular weight should be ⩽ 500 Da for efficient BNB and BBB penetration.26,27
The most widely used chemical structure for achieving NIR absorption and emission is the polymethine backbone, composed of either a pentamethine ≈700 nm emission) or a heptamethine ≈800 nm emission; see Figure 2A) core. The heptamethine core, in particular, is remarkably versatile. Simply altering the linkage in R 17 position with oxo-, amino-, or sulfur- will shift peak emission to ≈800 nm, 760 nm, or 840 nm, respectively.28–30 Peak absorption for each of these R 17 linkages is not proportional to emission, however, which can be exploited to produce NIR fluorophores with extremely large Stokes shifts. 30
Peak Absorbance Wavelength and Extinction Coefficient
To preserve “white light” (400–650 nm) for color video imaging of the surgical field and efficient separation of fluorescence channels when using the FLARE™ imaging system, peak absorbance wavelength for the ≈700 nm NIR fluorophore is typically in the range of 670 to 680 nm and for the ≈800 nm fluorophore is typically in the range of 750 to 770 nm. When exploiting the FLARE™ imaging system's two independent NIR channels, it is usually preferable to keep the Stokes shift of the ≈700 nm fluorophore relatively low (20–30 nm) so that peak emission will fall below excitation for the <800 nm fluorophore (Figure 3).
Key Physicochemical and Optical Properties in Serum for Near-Infrared Fluorescent Contrast Agents Useful for Preclinical and Clinical Imaging

Abs = absorbance; CA = carboxylic acid; CW800 = IRDye™ 800CW; Em = emission; Ext Coeff = extinction coefficient; HD = hydrodynamic diameter; ICG = indocyanine green; MB = methylene blue; MW = molecular weight; NA = not applicable; NIR = near-infrared; QY = quantum yield; RES = reticuloendothelial system; UV = ultraviolet, ZW-1 (zwitterionic heptamethine indocyanine 38 ).
Wavelengths at which absorbance was matched for QY measurements: 655 nm for MB and Cy5.5-CA; 770 nm for Cy7-CA, ZW-1, CW800-CA, and ICG. QY standards included Oxazine 725 in ethylene glycol (QY = 19% 31 ) for 700 nm fluorophores and ICG in dimethyl sulfoxide (QY = 13% 32 ) for 800 nm fluorophores.
For small nanoparticles, the thickness of the organic coating and the number of surface-bound targeting ligands significantly affect final HD.
In a well-designed NIR fluorophore, the extinction coefficient at peak emission should be ⩾ 150,000 M−1cm−1 in serum, pH 7.4. As a frame of reference, the visible fluorophore fluorescein has an extinction coefficient of ≈88,000 M−1cm−1 at peak absorption. Given that fluorescence photon yield is proportional to the extinction coefficient, it is desirable to achieve the largest possible value in serum. It should be noted, however, that many NIR fluorophores, such as MB and indocyanine green (ICG), tend to have a wide absorption curve, which extends toward the blue (see Figure 3). This can cause undesired excitation of the ≈800 nm NIR fluorophore by the ≈700 nm fluorophore's excitation light if not careful.
Peak Emission Wavelength and FWHM
If only one channel of NIR fluorescence is desired, such as when using the SPY, Fluobeam, or PDE system, the emission wavelength simply has to be 20 to 30 nm higher than peak absorption. When using the FLARE™ imaging system, an 80 to 100 nm separation in the peak emission of the two NIR fluorophores is desirable to maximize spectral separation. Moreover, the FWHM of the 700 nm NIR fluorophore emission should be narrow enough to not extend into the emission band of the 800 nm fluorophore. There is less constraint on FWHM emission from the ≈800 nm fluorophore, and the wider the emission filter the better because the sensitivity of silicon cameras falls off rapidly above 800 nm.

FLARE™ imaging system optical channels in the context of clinically available NIR fluorophores. The color video, 700 nm NIR fluorescence, and 800 nm NIR fluorescence optical channels of the FLARE™ imaging system are shown, along with the absorbance (left axis) and fluorescence (right axis) of 5 μM methylene blue (MB) and 2.5 μM indocyanine green (ICG) in 100% serum, pH 7.4.
Quantum Yield
The quantum yield (QY) of small-molecule NIR fluorophores is highly dependent on the chemical environment. In general, a QY of ≈10 to 20% in serum, pH 7.4, is typical for heptamethine indocyanines, with higher QYs being rare. The measurement of absolute QY can be difficult, and most reports use comparison to published standards under conditions of matched absorbance at single-wavelength (ie, laser) excitation. Our laboratory typically uses Oxazine 725 in ethylene glycol (QY = 19% 31 ) for QY measurements of 700 nm fluorophores and ICG in dimethyl sulfoxide (QY = 13% 32 ) for measurements of 800 nm fluorophores.
Fluorescence Lifetime
In general, the fluorescence lifetime of heptamethine indocyanines in serum is in the range of 0.5 to 1.1 ns, 33 with lifetime being strongly influenced by chemical environment. A relatively unexplored, but potentially fruitful, area of investigation is how binding of a fluorophore to a target (ie, cell or protein) changes its lifetime. 34 If the change in lifetime on binding is large enough, it might be possible to discriminate target-bound NIR fluorophore from background NIR fluorophore. Then, again, the use of “modular” ligands, which have an isolating linker between the NIR fluorophore and the targeting ligand, 35 may preclude sensing of such binding events. At the very least, measurement of fluorescence lifetime permits separation of NIR fluorophore from tissue autofluorescence. 36
Photobleaching Threshold
Fluorescent NPs, such as quantum dots, tend to exhibit extreme photostability at CW excitation fluence rates as high as 600 mW/cm2, 17 that is, high enough to heat water. On the contrary, heptamethine indocyanines typically undergo irreversible photobleaching at fluence rates > 50 mW/cm2.17,18 This is an important point because it sets an upper limit to the excitation fluence rate that is needed (or desired) for image-guided surgery. On the FLARE™ imaging system, the excitation fluence rate for the 700 nm emission channel is kept to ⩽ 5 mW/cm2 so as not to move color temperature outside (ie, too “red”) IEC #60601 guidelines for a surgical luminary; the excitation fluence rate for the 800 nm channel is kept to ⩽ 50 mW/cm2 to avoid photobleaching.
Concentration-Dependent Quenching
All fluorophores will exhibit fluorescence quenching if their concentration is too high, and NIR fluorophores are no exception. Previously, we reported that the quenching threshold for heptamethine indocyanines was ≈10 μM. 37 Recently, we discovered that quenching threshold is a strong function of the geometry of the excitation and emission light paths used for the measurement. As shown in Figure 4, when measured using a traditional 90°, three-sided cuvette geometry, both MB and ICG in serum display quenching thresholds ≈10 μM. However, when measured using 0° geometry, as would occur during image-guided surgery, the quenching threshold shifts to ≈50 μM, with a much slower rate of decline as concentration is increased further. We believe that this phenomenon is due to differences in the photon path length. The path length in the 90° geometry is longer than in the 0° geometry and fixed, leading to greater reabsorption of emitted photons. This is a potentially important observation because it suggests that much higher concentrations can be used than previously thought and much higher signal can be attained, without significant quenching.
Charge and Charge Distribution
Because of the hydrophobicity of polymethine indocyanine cores, solubilizing groups are always required to render the molecules compatible with aqueous solvents and serum. The most commonly used solubilizing group to date is sulfonic acid, imparting a net negative charge to most polymethines. Although aqueous solubility is proportional to the number of solubilizing groups, the distribution of charge around the bulky core is equally important. ICG, for example, which has only two sulfonates, has two distinctly different characters. The “top half” of the molecule is extremely hydrophobic, whereas the “bottom half” is hydrophilic. The former likely contributes to the rapid extraction of ICG by the liver (half-life in blood ⩽ 1 minute).
Recently, we discovered that relatively equal spacing of solubilizing groups around a heptamethine indocyanine and alternation of anion and cation charges to create a zwitterionic (net neutral) molecule impart special properties to the NIR fluorophore, especially ultra-low nonspecific binding to serum proteins, normal tissues, and organs. 38
In Vivo Properties
Injected Dose
It is important to consider the “typical” injected dose of a NIR fluorophore in the context of other imaging modalities (Table 3). In most image-guided surgery applications, the NIR fluorophore dose will be ≈10 mg. This dose is 60 times lower than the bioavailable dose resulting from ingesting two acetaminophen (eg, Tylenol®) tablets, 700 times lower than MRI contrast agents, and 5,600 times lower than CT contrast agents. The administration of such low doses, in an infrequent fashion, might help reduce some of the burdens associated with regulatory approval (discussed below).

Concentration-dependent quenching of methylene blue (MB) and indocyanine green (ICG) using different optical geometries. NIR excitation and emission geometries were either 0° or 90° as indicated (top). Shown at the bottom is the concentration-dependent quenching of MB and ICG in 100% fetal bovine serum supplemented with 50 mM HEPES, pH 7.4, under conditions of 0° (open circles) or 90° (closed squares) excitation/emission geometries.
Typical Doses of Intravenously Administered Diagnostic Agents and Radiotracers from High (CT) to Low (PET)
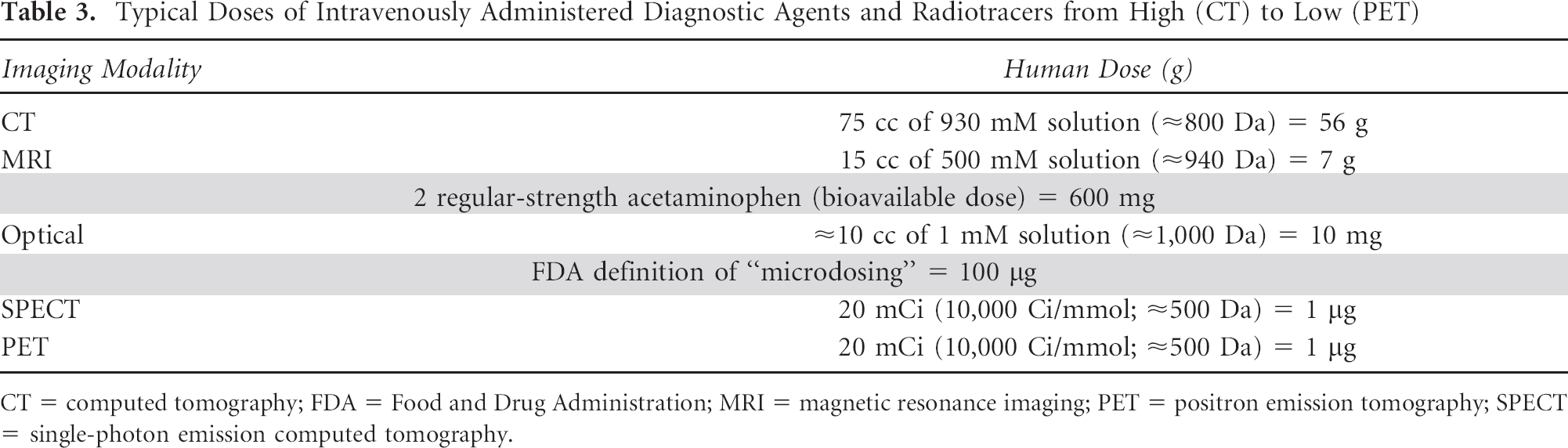
CT = computed tomography; FDA = Food and Drug Administration; MRI = magnetic resonance imaging; PET = positron emission tomography; SPECT = single-photon emission computed tomography.
Biodistribution
The molecular weight, charge, and dispersion of charge of a NIR fluorophore will determine its biodistribution after intravenous injection. In general, NIR fluorophores without any solubilizing groups are lipophilic cations, which readily cross the plasma membrane and are concentrated in mitochondria and/or endoplasmic reticulum. 18 When injected into the bloodstream, they act as perfusion tracers, with retention in certain tissues and organs providing “free” targeting without the need for a separate ligand. MB, for example, exhibits preferential retention in cardiomyocytes 39 and insulinoma 40 after a single intravenous injection. Interestingly, subtle changes to NIR fluorophore chemical structure can result in profound alterations in tissue and organ uptake. Newly synthesized pentamethine indocyanines, for example, provide endocrine gland- and endocrine tumor–specific targeting. 38
In the presence of two or more solubilizing groups, NIR fluorophores no longer cross the plasma membrane and remain extracellular after intravenous injection. In general, disulfonated heptamethine indocyanines exhibit short half-life (as short as 1 minute) in blood owing to rapid extraction by the liver, and tetrasulfonated molecules exhibit longer half-lives (on the order of 10 to 30 minutes). Recent data from our laboratory suggest that polyanionic NIR fluorophores exhibit high nonspecific uptake in normal tissues and organs despite high serum solubility. 38
Clearance
The clearance, or elimination, of NIR fluorophores from the body after intravenous injection occurs through the liver (ie, excretion into bile then feces), the kidney (ie, excretion into urine), or both. In general, disulfonated molecules, which retain both a strongly hydrophobic and a strongly hydrophilic character, are cleared into bile. Tetrasulfonated NIR fluorophores and molecules such as MB are excreted roughly equally by the liver and kidney. These natural clearance routes can be exploited to provide high-sensitivity identification of the ureters41,42 and bile ducts.43,44 Zwitterionic NIR fluorophores, on the other hand, are cleared exclusively by the kidney. 38 The route of clearance and clearance rate are critically important for targeted NIR fluorophores because they control blood half-life, and therefore contact time, with the target of interest, as well as influence background signal. Tetrasulfonated NIR fluorophores, for example, will always have difficulty in imaging gastrointestinal lesions because excretion into bile increases background in the gut, whereas zwitterionic NIR fluorophores can be used for image-guided surgery of any tissue or organ in the body with the exception of kidneys, ureters, and bladder.
Metabolism
Few data have been published about the metabolic fate of NIR fluorophores after intravenous injection. Some tetrasulfonated molecules appear to be relatively stable, appearing in bile and urine unchanged after intravenous injection.42,44 However, clinical translation of these molecules will ultimately require a comprehensive understanding of the rate, location, and by-products of metabolism.45–48
Affinity and Targeting
As mentioned above, some lipophilic NIR fluorophores are capable of being extracted and/or retained by cells in the body and provide targeting by virtue of their inherent chemical structure.18,38 Hydrophilic NIR fluorophores, however, require covalent conjugation of a targeting ligand specific for an extracellular epitope. When using small-molecule and peptide ligands, the NIR fluorophore itself can often dominate in vivo behavior. Care must be taken, therefore, to select a NIR fluorophore whose biodistribution, clearance, and nonspecific uptake are compatible with the target of interest. The absolute affinity of the targeting ligand necessary for effective image-guided surgery is a key variable that is only now being defined precisely. In general, final NIR fluorescent contrast agent affinity in the picomolar to low nanomolar range is required to generate a SBR adequate for image-guided surgery.
SBR is also a strong function of BMax, that is, the number of receptors or epitopes per cell. Consider, for example, that most cell surface receptors occur at a frequency of only 103 to 104 per cell and that an average cell volume is ≈1 pL. Thus, the highest achievable concentration of NIR fluorophore bound to a collection of cells would be 2 to 20 nM. Endocytosis can “amplify” this signal two- to fivefold; however, under most circumstances, NIR fluorophore concentration is limiting. This fact serves to highlight why imaging system optimization and rejection of tissue autofluorescence are so important for image-guided surgery.
Clinically Available NIR Fluorophores
With so many groups around the world developing novel NIR fluorophores and targeted NIR fluorophores, the future of image-guided surgery looks bright. Nevertheless, the reality is that first-in-human testing of a new chemical entity (discussed below) has a minimum lag of ≈2 years and the commercial availability of a new chemical entity has a minimum lag of 2 to 5 years. For the foreseeable future, only two NIR fluorophores are approved for other indications by the FDA and thus clinically available for study: MB and ICG. Interestingly, both of these molecules have been used for the last 50+ years as visible dyes (blue for MB and green for ICG). Thus, there is an unprecedented body of clinical data regarding their safety when used at millimolar concentrations.
MB (see Figure 2B) is a hydrophilic phenothiazine derivative that emits ≈700 nm and is compatible with the first NIR channel of the FLARE™ imaging system (see Figure 3). Its performance as an NIR fluorophore is only fair, exhibiting an extinction coefficient and QY far below those of the indocyanines (see Table 2). Even so, after a single intravenous injection, MB provides contrast for many important surgical procedures, including identification of the ureters, 41 identification of extrahepatic bile ducts, 43 assessment of cardiac perfusion, 39 and, importantly, detection of neuroendocrine tumors, such as insulinoma. 40
ICG (see Figure 2B) is a disulfonated heptamethine indocyanine with moderate optical properties (see Table 2) that emits ≈800 nm. Like MB, there are many clever uses for ICG during image-guided surgery. After intravenous injection, it can be used for NIR angiography of blood vessels,10,39,49 identification of the extrahepatic bile ducts, 43 and identification of liver metastases. 50 After subcutaneous injection, ICG or ICG adsorbed to human serum albumin (ICG:HSA 36 ) can be used for sentinel lymph node (SLN) mapping15,51–55 and assessing lymphatic function. 56
Although it is the general consensus that MB and ICG are not ideal NIR fluorophores, they are presently the best the field has to offer. Clearly, new and better-suited fluorophores are needed to provide the best clinical options for both patients and surgeons.
Surgical Procedures that Could Benefit from Real-Time NIR Fluorescence Guidance
Unmet Clinical Needs
NIR fluorescence imaging has the potential to address a variety of unmet clinical needs related to finding structures that need to be resected, such as SLNs, malignant cells, and luminal calcifications, and avoiding other structures that could cause acute or chronic morbidity, such as nerves, blood vessels, ducts, lymphatics, and normal glands. We now highlight only a few examples from the literature where proof of principle has been established in preclinical or clinical studies.
SLN Mapping
Visible blue dyes exhibit poor contrast, have a risk of anaphylaxis, and stain the surgical field blue, and radioactive lymphatic tracers expose patients and caregivers to ionizing radiation, increase the cost of the procedure, and complicate logistics. Because of these challenges, many groups around the world have explored the use of NIR fluorescence imaging for SLN mapping.15,57–59 The ideal NIR fluorescent SLN tracer has yet to be identified, but until such an agent receives regulatory approval, our group has suggested that simple adsorption of ICG to HSA (ie, ICG: HSA), 37 which occurs naturally after injection into the body, albeit with slow kinetics, is effective for SLN mapping in breast cancer (Figure 5A). 15

Clinical imaging using the FLARE™ imaging system. A, Sentinel lymph node (arrow) mapping in the axilla of a woman with breast cancer after peritumoral injection of ICG:HSA as described in Troyan and colleagues. 15 NIR fluorescence = 800 nm channel; 67 ms exposure time. The NIR fluorescence image was pseudocolored in lime green and superimposed on the color video image to produce color-NIR merge. B, Perforator flap NIR fluorescence angiography after intravenous injection of indocyanine green. Dominant perforator artery (dashed circle) identified during dynamic imaging. 80 NIR fluorescence = 800 nm channel; 67 ms exposure time. The NIR fluorescence image was pseudocolored in lime green and superimposed on the color video image to produce color-NIR merge.
Identification of the Ureters and Urinary Calcifications
The natural clearance of some NIR fluorophores into urine can be exploited to identify the ureters and to assess intraluminal contents (ie, the presence of stones) and luminal integrity.41,42 One such agent with immediate clinical relevance is MB. 41 Additionally, NIR fluorophores that bind the hydroxyapatite calcium salt, such as Pam800, 60 can be used to identify microcalcifications within the urinary tract. 61
Identification of the Extrahepatic Bile Ducts
Natural clearance of some NIR fluorophores into bile can be exploited to identify the extrahepatic bile ducts and to assess luminal contents and integrity.43,44,62,63 Once again, MB is useful in this regard but is by no means ideal owing to its modest optical properties. 43
Identification of Tissue and Breast Cancer Calcifications
The same hydroxyapatite-specific NIR fluorophore that is capable of imaging urinary calcifications can be used to image microcalcifications in breast cancer.64–67 This could be useful in optical tomography to help identify malignant calcifications or during surgery to help ensure complete resection of breast tumors.
Tumor Margin Detection
Without question, real-time tumor margin detection will someday be the primary application for NIR fluorescence–guided surgery. Even without clinical availability of ideal tumor-specific NIR fluorescent contrast agents, recent reports suggest that the uptake of MB in insulinoma permits highly sensitive, real-time identification and resection of submillimeter metastases, 40 and uptake of ICG helps identify tumors in the liver.68,69 Newer agents have greatly improved optical and tumor-targeting properties for this application. 38 The literature also suggests that tumor-specific agents will be available for many cancers within the next decade, with prostate cancer agents70,71 and integrin-specific agents72,73 probably being the furthest in their development.
Breast Reconstructive Surgery after Mastectomy
Several preclinical49,74–77 and clinical78–80 (see Figure 5B) studies have demonstrated the utility of NIR fluorescence angiography for perforator artery mapping and assessment of tissue perfusion before, during, and after flap preparation. Ongoing studies are identifying the intraoperative predictive nature of NIR fluorescence imaging toward long-term outcome.
Cardiovascular and Vascular Imaging
NIR fluorescence imaging has several potential uses in cardiovascular surgery, including simple angiography,10,11,81 cardioplegia delivery,82,83 and numerous other procedures.84–97 The use of hydroxyapatite-specific NIR fluorophores also permits the noninvasive identification of vascular calcifications. 98 Recently, our group has shown that autologous platelets can be made NIR fluorescent without loss of bioactivity and can be combined with the FLARE™ imaging system to identify intravascular thrombi and vessel patency, noninvasively and in real time.39,99 Fluorescence angiography is also widely employed in neurosurgery by using modified surgical microscopes.100–102
Nerves and Intervertebral Disks
Useful image guidance during spine surgery includes identification of the intervertebral disks and identification of nerves. A recent study demonstrated uptake of NIR-compatible fluorophores by the annulus fibrosus of the intervertebral disks in three species. 25 Another described the development of myelinated nerve-specific agents that are approaching NIR emission. 103
Clinical Translation
The typical sequence of events for moving a new imaging system or contrast agent from “bench to bedside” in the United States includes preclinical validation, manufacture under current Good Manufacturing Practices (cGMP), first-in-human clinical trials, clinical trials to support regulatory approval, regulatory approval, marketing, and postmarketing surveillance. In addition, each country has its own set of guidelines that regulate each part of this process. Because most investigators are familiar with regulations surrounding preclinical studies and regulatory approval is a complex subject that is beyond the scope of this review, we focus on the impact academic investigators can make on the field by performing first-in-human studies with new technology.
Imaging Systems
The details surrounding clinical translation of a new optical imaging system were recently reviewed by our group. 104 Briefly, the key to starting the process is determination of risk status: nonsignificant risk (NSR) or significant risk (SR). NSR devices do not necessarily require approval of an Investigational Device Exemption (IDE) application, but SR devices do. Preparation of an IDE is a labor-intensive and costly exercise that should be performed only when required.
The local Institutional Review Board (IRB) has the authority to make the risk status determination. The problem is that once an IRB has determined the level of risk for an NSR device, the labor-intensive portion of the application has already been completed. The need to backtrack adds delay, cost, and unneeded work to the process. Yet the IRB is under no obligation to make this binding decision until a full IRB application is submitted to them, that is, the “risk conundrum.” 104 For this reason, we recommend informal (nonbinding) discussions with the IRB prior to beginning the translation process. In general, pilot trials of imaging systems for which (1) there is no contact with the patient, (2) an NIR fluorescent contrast agent is being used in a way that is consistent with its indication, and (3) the imaging is not used to diagnose or treat the patient will be classifiable as NSR.
During clinical translation of the FLARE™ and Mini-FLARE™ image-guided surgery systems, we were careful to design the trials such that all patients received the standard of care, and the NIR fluorescence imaging as performed did not alter or interfere with the standard of care. Moreover, because such optical imaging systems have a long WD (ie, no patient contact) and the NIR fluorophores were used at low dose and consistent with previously approved indications, our IRB determined that these instruments were NSR. This permitted six-patient pilot trials of each device to be performed in a relatively short period of time, with feedback from surgeons helping our group develop the next-generation FLARE™ imaging system.
Contrast Agents
Until recently, the model for clinical translation of contrast agents and other drugs was for an academic institution to license the agent to a for-profit company, which would then invest the significant resources necessary for clinical translation. In NIR fluorescence image-guided surgery, however, there is no well-defined market, and most companies view clinical translation as both costly and risky. This leaves academic investigators with the burden of introducing new agents into the medical field, thereby minimizing the risks of commercialization by weeding out underperforming agents and identifying potentially successful agents.
In January 2006, the FDA issued a very important document titled “Guidance for Industry, Investigators, and Reviewers: Exploratory IND Studies.” 105 This guidance document creates the exploratory Investigational New Drug (eIND) application and reduces the cost and complexity of preclinical testing by replacing formal lethal-dose studies with no observed adverse event level (NOAEL) testing. There are two common misconceptions about the eIND mechanism. The first is that it can only be used for microdosing (< 100 μg) studies. This is incorrect; Example 2 in the guidance document is consistent with a NIR fluorophore to be used during image-guided surgery. The second is that preclinical animal studies must be expensive and complicated. This is exactly the opposite intent of the eIND, and NOAEL testing can be performed cost-effectively. Two recent articles help clarify these points.106,107
Nevertheless, the process of clinical translation is still complex and costly and requires careful forethought. The key steps in the process are (1) synthesis of the compound under cGMP conditions and preparation of the batch record and quality assurance/quality control documentation (≈$100,000–200,000, depending on the compound); (2) rodent NOAEL testing and second-species (typically dog) NOAEL confirmatory testing (≈$20,000 to $75,000 depending on resource availability); (3) additional toxicology tests (if needed, could add an additional $10,000 to $20,000): (4) submission of an eIND application to the FDA; (5) submission of an institutional IRB application after the eIND is approved by the FDA; and (6) conduction of the first-in-human trial. If the pilot clinical trial is designed correctly, it will have enormous value by not only evaluating safety (the primary role of the trial) but also by providing imaging data that will guide future trials.
Prior to embarking on first-in-human testing of a novel diagnostic agent, one must consult with an experienced regulatory specialist. Depending on the agent, the device it is used with, and the indication, the FDA has the right to label the proposed technology a “combination,” which under Title 21 of the Code of Federal Regulations (CFR) Part 3.2, Subpart (e) (ie, 21 CFR 3.2(e)), will require both an IDE and an eIND.
Future Imaging System Improvements
An important, yet unanswered, question is whether reflectance-based, CW fluorescence imaging is “good enough” for most image-guided surgery. The advantages of CW fluorescence imaging include real-time acquisition and display, no requirement for data postprocessing, relatively simple and inexpensive hardware and software, and an ergonomic footprint in the operating room. The disadvantages of CW fluorescence imaging include an inability to quantify the tissue optical properties or subsurface depth of NIR fluorophores or to distinguish between multiple fluorophores of the same peak emission wavelength. There is also a general trend in the field of surgery to replace “open” procedures with minimally invasive, fiberoptic-based procedures.
Minimally Invasive Imaging Systems
Endoscopy and laparoscopy are widely used surgical procedures that could benefit from NIR fluorescence imaging. Although all of the principles discussed in this review apply equally to fiberoscopy, certain engineering challenges unique to fiberoscopy are outside the scope of this review. Nevertheless, commercial fiberoscopy systems capable of simultaneous color video and NIR fluorescence are beginning to become available.
Fluorescence Lifetime Imaging
Fluorescence lifetime imaging (FLIM) measures the time-dependent fluorescence intensity decay of a NIR fluorophore and has been widely studied in biomedical optics and microscopy.33,108–111 FLIM consists of modulating, in time, the fluorescence excitation light and extracting the time-dependent decay by means of time-gated fluorescence intensity detection. It can be performed either in the temporal domain or the temporal frequency domain, with the performance of each dependent on the instrumentation used. Given that lifetime is dependent on chemical environment (eg, hydrophobicity, pH) and even NIR fluorophores with the same peak emission can be discriminated, FLIM has the potential to impact many surgical procedures. Some studies have demonstrated FLIM over large fields of view, under clinically realistic conditions.112–115
Depth-Sensitive Imaging
It has been known for some time that temporal or spatial modulation of a light source could provide depth-sensitive measurement of endogenous and exogenous optical contrast.116–119 However, it is only recently that developments in spatial frequency domain imaging have permitted in vivo imaging over large fields of view.120–123 Tomographic absorption measurements have been demonstrated121,124 and adapted to fluorescence imaging. 125 The technique not only provides depth-sensitive fluorescence detection but also contributes to improving lateral resolution of fluorescent targets within a diffusing medium. Depth-sensitive imaging might help identify critical structures, such as nerves, which are hidden under structures being resected, such as SLNs. Also contributing to the success of these techniques are recent advances in motion gating hardware, which can help isolate optical images from the effects of cardiac, respiratory, and involuntary motions. 126
Endogenous Properties and Chromophore Imaging
As just mentioned, temporal or spatial modulation of light permits extraction of tissue optical properties (ie, scattering and absorption). By making spectroscopic measurements, that is, at various wavelengths, a modified Beer Lambert's law can also be employed to separate the contributions of oxyhemoglobin, deoxyhemoglobin, water, and lipids.127–129 This technology should someday permit near-real-time assessment of tissue oxygenation during surgery, thus permitting the surgeon to assess tissue ischemia noninvasively, over wide FOVs, without the need for exogenous contrast agents.
Future NIR Fluorophore Improvements
Although few molecules have yet to reach the clinic, the level of innovation in the field of NIR fluorophore chemistry remains high. Particularly exciting are new classes of molecules that could lower fluorescence background by orders of magnitude. The first are “upconverting” fluorophores, which, through a two-photon process, absorb light of long wavelength and emit light of a shorter wavelength. 130 The second are “smart” NIR fluorophores, which become fluorescent only after encountering a particular external stimulus. 131
There is also continual innovation in the structure of NIR fluorophores. A carbon-carbon bond at the R 17 position of the polymethine backbone (see Figure 2A), introduced using Suzuki-Miyaura coupling, 132 improves stability and permits direct conjugation to targeting ligands. Zwitterionic NIR fluorophores 38 provide ultra-low nonspecific uptake and renal-only clearance, which are ideal for tumor-targeting applications. NIR fluorophores with varying fluorescence lifetimes could improve rejection of background caused by tissue autofluorescence. 33 Particularly exciting are voltage-sensitive NIR fluorophores, which could be used with the ratiometric capabilities of the FLARE™ imaging system to perform real-time imaging of electrical activity in the heart and brain.133–135 Ultimately, the discovery of disease-specific small-molecule targeting ligands will eventually find their way into NIR fluorescent contrast agents for image-guided surgery.
Conclusion
Objectively speaking, the impact of NIR fluorescence imaging on patient care is still unknown. Nevertheless, it is easy to forget that just 5 years ago, not a single NIR fluorescence-based image-guided surgery system was available commercially. Now several are available, with more options likely in the near future. The availability of imaging systems has finally broken the “chicken and the egg” problem in the field. The challenge, now, is to develop high-performance NIR fluorescence contrast agents that provide surgeons with the guidance they desire and to translate these agents to the clinic for patient care.
One of the main motivators for this review was to define the state of the art so that academic investigators could build on it and help develop the next generation of imaging systems and contrast agents for image-guided surgery. The key to future success will be first-in-human trials of new technology, which in turn requires a comprehensive understanding of those design parameters that are important and those that are not.
If one reviews the history of the other imaging modalities now used in clinical medicine (plain films, CT, MRI, US, SPECT, and PET), one finds that the time between first-in-human studies and routine use of the technology in patient care has a mean and a median of 23 and 22 years, respectively. The first description of intravenously injected ICG (aside, as an absorber rather than a fluorophore) for NIR tomographic optical imaging of the breast was in the year 2000. 136 If this is chosen as the start of the field, then 10 years have passed, and we are on target for clinical acceptance and widespread use in patient care around the beginning of the next decade. The next 10 years will likely see the explosion or the demise of image-guided surgery using invisible NIR light.
Footnotes
Acknowledgments
We thank Susan Troyan, MD, Bernard Lee, MD, Joshua Winer, MD, Mireille Rosenberg, PhD, Barbara L. Clough, MA, Summer Gibbs-Strauss, PhD, Alan Stockdale, BS, Rafiou Oketokoun, MS, Vida Kianzad, PhD, Razvan Ciocan, PhD, Sunil Gupta, BS, and Merlijn Hutteman, MSc, for their contribution to the FLARE™ and Mini-FLARE™ imaging systems design and clinical trials; Lucjan Strekowski, PhD, Gabor Patonay, PhD, and Maged Henary, PhD, for many helpful discussions on NIR fluorophores; Lorissa A. Moffitt, MS, for editing the manuscript; and Eugenia Trabucchi for administrative support.
Financial disclosure of authors: All intellectual property surrounding FLARE™ imaging technology is owned by the Beth Israel Deaconess Medical Center, a teaching hospital of Harvard Medical School. As inventor, Dr. Frangioni may someday receive royalties if products are ever commercialized. The work presented in this review was funded by NIH Bioengineering Research Partnership grants R01-CA-115296 and R01-EB-0005805 and a Quick Trials for Imaging grant R21-CA-130297 to J.V.F.
Financial disclosure of reviewers: None reported.