
Abstract
The purpose of this study was to investigate if ibuprofen intake can influence mammary uptake of the proliferation-seeking radiotracer technetium 99m–pentavalent dimercaptosuccinic acid (99mTc-(V)DMSA) in women with severe epithelial and atypical epithelial breast hyperplasia. Eight patients with histologically confirmed severe epithelial breast hyperplasia with (n = 4) and without atypia (n = 4) were submitted prospectively to 99mTc-(V)DMSA scintimammography before and after a 4-week course of 400 mg ibuprofen daily oral intake. Lesion to background ratios 60 minutes postinjection were calculated and compared (t-test) before and after ibuprofen administration. Prior to ibuprofen, the patients with severe epithelial hyperplasia displayed a significantly higher 99mTc-(V)DMSA uptake ratio compared to those with atypical epithelial hyperplasia (2.40 ± 0.32 vs 1.67 ± 0.09, respectively; p = .003). They also exhibited a more substantial percent decline in tracer uptake postibuprofen compared to women with atypical epithelial hyperplasia (62.0 ± 7.1 vs 15.0 ± 0.2, respectively; p = .001). Ibuprofen induces significant uptake reduction of the proliferation-seeking radiotracer 99mTc-(V)DMSA in severe epithelial breast hyperplasia without atypia. This agent could therefore constitute a potential imaging tool for monitoring chemoprophylaxis effectiveness in women at the early stages of malignant transformation.
Technetium 99m–labeled pentavalent dimercaptosuccinic acid (99mTc-(V)DMSA) is a tumor-seeking radiotracer. Its relationship to focal adhesion kinase (FAK) activation and cellular proliferating activity has been described not only for invasive but also for preinvasive and benign proliferating breast lesions.5–9 This pilot study aimed to investigate whether ibuprofen exhibits an in vivo inhibitory effect on the uptake of the radiotracer 99mTc-(V)DMSA in cases with severe epithelial hyperplasia with (AEH) and without atypia (EH).
Materials and Methods
We prospectively enrolled eight females previously submitted to open surgical breast biopsy owing to suspicious mammographic findings in whom histology had confirmed severe epithelial hyperplasia, with (n = 4, age: 56 ± 3.4 years old) and without atypia (n = 4, age: 46 ± 2.3 years old). Baseline 99mTc-(V)DMSA scintimammography was performed not less than 3 months after surgery and a second (follow-up) study after a 4-week course of 400 mg ibuprofen daily oral intake. After intravenous administration of 925 MBq tracer activity, lateral prone and anterior supine planar images were acquired at 60 minutes postinjection. Breast 99mTc-(V)DMSA uptake was first assessed visually. Semiquantitative assessment in both the baseline and follow-up studies was performed by drawing regions of interest over the breast sites of greatest tracer uptake and over the normal breast parenchyma and then calculating the lesion to background (L/B) ratios. L/B ratios were compared (t-test) between the same (corresponding) breast areas in the two scintigraphic studies. The percent change in 99mTc-(V)DMSA uptake after the ibuprofen course was calculated as the mean percent change of all patients and was compared between the two groups. The level of significance was set at 5% (α = 0.05). All numerical data are expressed as mean value ± SD.
All patients gave their informed consent for ibuprofen intake and for both baseline and follow-up scintimammograms. The study was approved by the Ethics Committee of our hospital and was in accordance with the principles of the Declaration of Helsinki.
Results
On the baseline scan (prior to ibuprofen intake), the patients with severe EH displayed a significantly higher 99mTc-(V)DMSA uptake ratio compared to those with AEH (2.40 ± 0.32 vs 1.67 ± 0.09, respectively; p = .003). The L/B ratios in each group before and after ibuprofen are summarized in Table 1 and Figure 1. It is evident that ibuprofen administration was followed by a decline in tracer uptake in both histologic groups; however, this was statistically significant only in the population with severe EH. The percentage of tracer uptake reduction postibuprofen was more profound in the cases of severe EH than in those with AEH (62.0 ± 7.1 vs 15.0 ± 0.2, respectively; p = .001). Scintigraphic studies of two cases, one within each group, are presented in Figure 2.
L/B Ratios in EH and AEH before and after Ibuprofen Intake and Comparisons
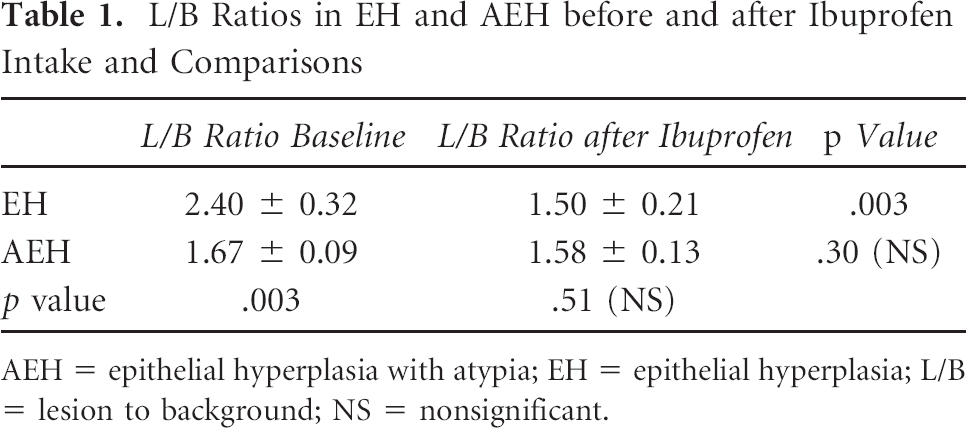
AEH = epithelial hyperplasia with atypia; EH = epithelial hyperplasia; L/B = lesion to background; NS = nonsignificant.
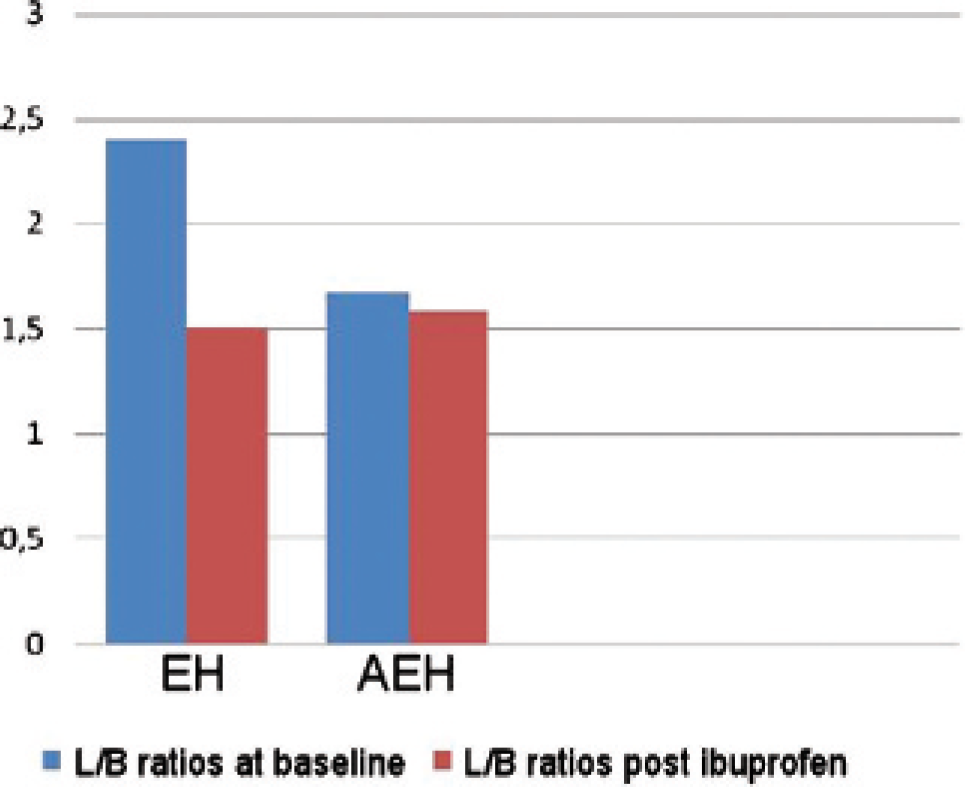
Lesion to background (L/B) ratios in epithelial hyperplasia (EH) and epithelial hyperplasia with atypia (AEH) before and after ibuprofen intake.
Discussion
The findings of this study indicate that breast EH is associated with diffusely increased 99mTc-(V)DMSA uptake, which is more profound in severe hyperplasia than in atypical hyperplasia. The extended time interval (3 months at the least) between open biopsy and baseline scanning practically excluded the possibility that baseline tracer uptake could have been attributable to a postbiopsy inflammatory tissue reaction or healing process rather than to hyperplasia itself. The fact that hyperplasia was the source of increased tracer uptake is further supported by the findings of another recent study of ours on two female groups, one without EH and the other with usual ductal breast hyperplasia and a nonincreased cellular proliferation rate (Ki-67 ⩽ 3%). Both groups displayed negligible 99mTc-(V)DMSA uptake (60-minute L/B ratios between 1.07 and 1.31 [mean 1.15] and between 0.77 and 1.62 [mean 1.2], respectively). 5
We recently reported an ibuprofen-mediated reduction of 99mTc-(V)DMSA uptake in vivo in a patient with severe breast EH. 10 Other recent studies have shown that COX-2 inhibitors may reduce the risk of breast cancer. A retrospective study of nearly 1,000 women showed that celecoxib, a selective COX-2 inhibitor, at an oral dose of 200 mg/d for at least 2 years reduced the risk of breast cancer by 83%, whereas rofecoxib at 25 mg/d reduced the risk by 64%. 1 The nonselective COX inhibitors aspirin and ibuprofen or naproxen gave a reduced odds ratio (0.49 and 0.37, respectively, with 95% confidence intervals) for the incidence of breast cancer compared to nonuse. Similarly, the odds ratio for breast cancer by dose and frequency was 0.28 for ibuprofen at a dose of 200 mg more than three times weekly. In this context, other investigators have suggested that inflammation mediated through COX-2 pathways may play a role in the progression of benign breast disease to carcinoma and that aspirin may reduce this risk in women with benign breast disease. 2

99mTc-(V)DMSA scintimammography in a case of epithelial hyperplasia with atypia at baseline (A) and after ibuprofen (B). The same in a case of severe epithelial hyperplasia without atypia (C and D, respectively) (EH). Following ibuprofen, tracer uptake was markedly decreased only in the case of severe EH. Regions of interest for lesion to background ratio calculation can be seen on scans A, B, and D.
It has been demonstrated that 99mTc-(V)DMSA is linked to FAK activation and cell proliferation rate in both in vitro and in vivo studies.5–9 The exact mechanism of 99mTc-(V)DMSA accumulation in benign proliferating disease is not yet clear.5,7 The present pilot study included only benign proliferative lesions; therefore, it was not truly an established increased cellular proliferation rate but most likely FAK activation that triggered increased 99mTc-(V)DMSA uptake. The inhibitory result of ibuprofen on mammary 99mTc-(V)DMSA uptake was exerted after a relatively short period of administration (4 weeks), which supports the hypothesis that its effect is most likely due to a possible “switch-off” mechanism on FAK activation rather than a diminishing effect in an already established proliferative activity. Pai and colleagues demonstrated that both nonselective and COX-2-selective inhibitors decreased FAK phosphorylation activation in a wounded gastric epithelial cell monolayer model. 11 Lahlou and colleagues reported that specific disruption of FAK function in the mammary epithelium blocks the transition of premalignant hyperplasias to carcinomas and their subsequent metastases. 12
It can therefore be postulated that the ibuprofen-mediated reduction of 99mTc-(V)DMSA in severe EH in our study could have been mediated through FAK inhibition. On the other hand, ibuprofen did not seem to have an equally significant inhibitory effect on AEH, a lesion in which cancer-related genes are dysregulated, as in ductal carcinoma in situ (DCIS), and this supports the hypothesis that both of these premalignant lesions (AEH and DCIS) are irreversible.
These findings derive from a limited number of cases and should therefore be regarded as preliminary evidence requiring further verification on a larger scale. This is our intention, with further research on this topic already under way. Nonetheless, to the best of our knowledge, this pilot study is the first report to depict in vivo—through the proliferation-seeking tracer 99mTc-(V)DMSA—the antiproliferative effect of ibuprofen on severe breast EH. Our imaging results support the hypothesis that ibuprofen may exert a potential antiproliferative chemoprophylactic role against the transition from severe EH to breast cancer.
In conclusion, ibuprofen induced the most significant reduction of 99mTc-(V)DMSA uptake in severe breast EH. As long as these lesions can be imaged with this radiotracer, it would be of great clinical interest if we could estimate the effectiveness of various chemoprophylactic agents (eg, NSAIDs, antiestrogens) by quantifying their inhibitory effect on 99mTc-(V)DMSA uptake. This diagnostic modality could constitute a substantial imaging tool in the optimal monitoring of women at the early stages of malignant transformation. Further research to support these initial observations is of particular interest.
Footnotes
Acknowledgment
Financial disclosure of authors and reporters: None reported.